



PRETERM BIRTH RATES –BOLIVIA
Rank: 111 –Rate: 9% Estimated # of preterm births per 100 live births (USA – 12 %, Global Average: 11.1%)
Bolivia, officially the Plurinational State of Bolivia, is a landlocked country located in western-central South America. The constitutional capital is Sucre, while the seat of government and executive capital is La Paz. The largest city and principal industrial center is Santa Cruz de la Sierra, located on the Llanos Orientales (tropical lowlands), a mostly flat region in the east of the country.
The country’s population, estimated at 11 million, is multiethnic, including Amerindians, Mestizos, Europeans, Asians, and Africans. Spanish is the official and predominant language, although 36 indigenous languages also have official status, of which the most commonly spoken are Guarani, Aymara, and Quechua languages.
Modern Bolivia is a charter member of the UN, IMF, NAM, OAS, ACTO, Bank of the South, ALBA, and USAN. Bolivia remains the second poorest country in South America, though it has slashed poverty rates and has the fastest growing economy in South America (in terms of GDP). It is a developing country, with a high ranking in the Human Development Index. Its main economic activities include agriculture, forestry, fishing, mining, and manufacturing goods such as textiles, clothing, refined metals, and refined petroleum. Bolivia is very rich in minerals, including tin, silver, lithium, and copper.
Health
Between 2006 and 2016, extreme poverty in Bolivia fell from 38.2% to 16.8%. Chronic malnutrition in children under five years of age also went down by 14% and the child mortality rate was reduced by more than 50%, according to World Health Organization. In 2019 the Bolivian government created a universal healthcare system which has been cited as a model for all by the World Health Organization.
Source: https://en.wikipedia.org/wiki/Bolivia

COMMUNITY
Wishing the very best to our Global Neonatal Womb Community from our home in Seattle, WA. USA. In many ways the pandemic has provided and even demanded expansion of and collaboration towards our increased potential to access healthcare. At the same time, the gaps that exist in our global access to healthcare became more visible to the masses. Our hope is that the exposure to broadened community perspectives will continue to promote collaborative efforts to create, sustain and grow universal healthcare access, replenish/build a supported, vibrant, and empowered healthcare provider community, and decrease preterm birth and maternal and child mortality worldwide. We have a lot of work to do with pandemics, increasing climate change challenges and serious socio-economic barriers to address. Our preterm birth survivors need research, diagnostic/treatment options and provider development to address survivor needs. So, let’s get to it. We have what it takes.

This revolutionary Bolivian hospital is changing how women give birth

Javier Sauras/Narratively

July 14, 2016 – Michele Felix Javier and Bertelli Lill Sauras
Under the dim hospital light, a midwife, a doctor, a pregnant woman, and her mother silently ponder what they should do with a baby that fiercely resists coming out of the womb. The longer the labor, the more dangerous it gets, and it has been almost a full day since the woman arrived here at the hospital. In Bolivia, which has the second-highest maternal mortality rate in South America, such a delay is a mortal threat. But here, in the high Andean plateau, hours from any major hospital, the mother is in very good hands.
The pregnant woman never wanted to go to the hospital. The night before, her mother called Doña Leonarda, the midwife, or partera, to attend the delivery according to traditional Aymara customs. Doña Leonarda was working at the hospital today, so the woman reluctantly came here. Lying on her back, eyes wide open, the mother looks terrified. A young nurse turns to the physician, Dr. Henry Flores, and asks whether she should call the ambulance and take the woman to La Paz for a C-section.
“That would be unwise,” Flores answers in a smooth, low-pitch tone.
It would take more than two hours to get to the capital city and that could be too risky, too late for her. Her pain is increasing and she is already dilated. The doctor measures her contractions and tells the nurse to give the woman an IV solution. “It’s only vitamins,” Doña Leonarda says. But she knows better: they are dripping a painkiller into a plastic bag hanging from a pole — one of the few traces of modernity in this small chamber of the rural hospital. Three deep breaths later Dr. Flores makes a decision.
“Should we try the traditional way?” he asks the partera. “She is weak but she can do it,” Doña Leonarda answers.
Mother, partera, doctor, and nurse place a green mat on the floor of the hospital and gently move the woman over it. She is on her knees, her head on her mother’s hands; Doña Leonarda rolls up the woman’s skirt. It’s going to be a vertical delivery, virtually unheard of in Bolivian hospitals but the traditional method in the Andean region. It’s the way this pregnant woman was born herself, thirty years ago, just like her mother before her, and her grandmother, and so on. Dr. Flores learned the delivery method from the indigenous healers of El Altiplano — Bolivia’s Andean plateau — and he is one of the few doctors in the country who is confident enough to try it.
Here on the Bolivian side of El Altiplano, a vast plateau 13,000 feet above sea level, the difference between life and death wears a bowler hat and a rainbow skirt. Far from medical facilities, lacking academic training and marginalized by the public healthcare system, parteras provide the only help that most women get during childbirth. But their efforts are not enough. Hundreds of people die every year during labor, a curse that haunts one of the most vulnerable groups on Earth: rural, poor, indigenous women. Bolivia trails behind almost every other place in the Americas with 206 deaths per 100,000 live births. (The rate in the United States is just 14 deaths per 100,000.) This revolutionary hospital might be showing the way to put an end to this ongoing tragedy.
Dr. Flores, who runs the local hospital in Patacamaya, approached Leonarda Quispe 10 years ago to recruit her for the outpost, even though she had never set foot in medical school and she barely speaks Spanish. Born in a small indigenous Aymara community, Doña Leonarda, as people know her, has been delivering babies since she was 12. Nobody has ever died under her care, she says “neither a woman nor a newborn,” which might be a record for someone who has attended more than 10,000 childbirths. Seven years ago, Dr. Flores realized the partera was getting more calls than any of his obstetricians and came up with a surprisingly straightforward and inexpensive idea. His plan was to develop a new healthcare system that would attract the local population to the hospital by combining traditional indigenous practices and modern academic knowledge. Should it prove to be successful, it might be adapted and applied everywhere — not just in Bolivia, but around the globe.
In Dr. Flores’ hospital, parteras are welcomed and traditional indigenous doctors have their own offices, alongside skilled surgeons and trained specialists. Doña Leonarda and her husband, Don Vitaliano, are part of the staff; medical doctors like Flores often consult with them. Delivery rooms in Patacamaya’s hospital look like little rural houses: There are kitchens, windows with thick curtains, walls painted in warm colors, wooden furniture, and flurry blankets. Nothing is white or shiny. By the pale red cribs, a banner reads “Ususiñ Uta” (birthing chamber), although in the hospital everybody knows these spaces as “intercultural delivery rooms.”
Nearby, in the two-story brick house where Leonarda and Vitaliano live and run their own private practice, there are two bedrooms, plus an examination room filled with jars, syrups, ointments, a couple of tables, some notebooks, and a stretcher. As modest as the facility might look, Doña Leonarda and Don Vitaliano attract patients from as far as Chile, Brazil, Argentina, Peru, and even Spain.
Hidden in Leonarda’s pollera, a large cotton skirt typical of the Altiplano, a small cellphone insistently buzzes. “Another patient,” she says in Spanish while excusing herself with a gentle gesture of her hand before leaving the room. Wearing a pink sweater and a colorful skirt under a blue apron, she takes her bowler hat off for a second, revealing all of her braided black hair, almost three feet long. Don Vitaliano, a large man with gelled hair, the arms of a builder, and the smile of a high school student, stays behind. Ten years younger than his wife, he is her voice, her aide, and her driver. A Honda off-road motorcycle, the engine still warm, waits outside the house. They have just returned from the hospital, where they attended a delivery in the middle of the night.
It’s now seven in the morning. The previous night a woman called from La Paz to ask Doña Leonarda to attend her delivery. Leonarda told her to come here, to her private office in Patacamaya. But when the woman and her mother arrived in the early hours, Don Vitaliano had to convince them to meet his wife at the hospital, where she was still working, rather than at their place. It was a difficult task: They traveled three hours at night to give birth in a traditional environment, with a partera, far from medical doctors and their scary bright-white delivery rooms.
Convincing an indigenous woman to set foot in a hospital is like inviting her to take her life into her hands. “There are some diseases here, in the Altiplano, that urban doctors don’t want to treat,” Don Vitaliano says. Projecting his voice like a Roman orator, he explains the condition of sobreparto, a commonly reported postpartum condition among the Aymaras. Everybody in the rural area has heard about sobreparto and can describe its symptoms: headaches, swelling, fever, fatigue, and inability to perform complex tasks. But this malady is not recognized by modern medicine.
Therefore, it has no treatment. Indigenous women, however, are extremely scared of it. It attacks them when the rooms are frigid with tiles and metals and when nurses wash them with cold water. “Some mothers prefer to stay at home because they are afraid of getting cold,” Vitaliano says.
“When they go to hospitals they are not taken care of properly and, then, they get sick. Sometimes they don’t even speak the same language and doctors yell at them; they cannot talk to anyone and they are terrified.”
Narratively is a digital publication and creative studio focused on ordinary people with extraordinary stories.

Fatal police violence may be linked to preterm births in neighborhoods nearby

April 16, 2021 Author Dana Goin Postdoctoral Scholar, University of California, San Francisco
Building on generations of work by activists and organizers, there is currently a national reckoning with the impacts of police violence on Black communities underway in the United States. It’s well established that killings, injuries and intense surveillance by police can traumatize not only the direct victims, but their communities. But little research has been done to assess whether police violence has spillover effects on other facets of human health.
I am an epidemiologist who studies how the social and physical environment shapes maternal and infant health, and my research team and I wanted to investigate whether witnessing the police killing someone – or even living nearby or hearing about it afterward – could affect the outcome of a healthy pregnancy. Our latest research suggests the answer is yes.
Our new study, published in March in the journal Paediatric and Perinatal Epidemiology, found that Californians who were pregnant when fatal police violence occurred in their neighborhoods saw increases in preterm birth. For Black mothers, the associations were particularly high: When police killed a Black person in the neighborhood, the hazard of delivering early increased by 35% or 81%, depending on the data source.
Previous studies show stressful or traumatic events of any kind during pregnancy can be linked to increased risk for preterm birth. Because Black people are disproportionately victimized by police violence, and because there are stark racial and ethnic inequities in preterm births, we anticipated that exposure to fatal police violence during pregnancy might also influence preterm birth risk.
Examining the data
Our study used California birth records to estimate pregnancy duration for the almost 4 million births statewide from 2007 to 2015. We then looked at anyone who was pregnant when a police killing occurred in their neighborhood, and compared them to their neighbors who were not exposed during their pregnancies. There is no single comprehensive source of data on police killings. We therefore used two sources of information about fatal police violence: California death records and the Fatal Encounters database, a compilation of Americans killed during police interactions.
We observed that when people were exposed to fatal police violence sometime during their pregnancies, there was a small increase in the hazard of delivering prematurely. Using the California death records, there was a 5% increased hazard of the baby being born between 34 and 36 weeks of gestation. There was a 3% increased hazard using the Fatal Encounters database. We didn’t observe associations between exposures to police violence and delivery even earlier, between 20 and 33 weeks of gestation.
Among Black women, we found that exposure to fatal police violence, especially when the victim was also Black, had an even stronger impact. When police killed a Black person in her own neighborhood, a Black mother’s hazard of delivering her child between weeks 32 and 33 increased 81% with the California death records. With the Fatal Encounters data, the hazard increased by 35%.
These findings are critical for a number of reasons. Preterm birth is the leading cause of infant death and may also carry implications for a child’s short- and long-term health. Mothers of preterm children may experience adverse mental health outcomes like increased anxiety and fatigue and use postnatal services less.
The cost of preterm birth is staggering, an estimated US$25.2 billion per year – about $65,000 per birth – with a substantial portion of that paid by Medicaid. For families, preterm birth can present additional financial hardships, including increased transportation costs for additional medical appointments and delayed return to work or missed work for employed parents.
The American Public Health Association provides detailed guidance on addressing police violence to improve health and health equity. This policy statement from public health researchers builds on work from community organizers and indicates what’s needed most is a shift in how government resources are allocated. It suggests that moving those resources away from criminalizing and policing marginalized communities to investing in their health, safety and well-being – through housing, food security, and quality health care and education systems – is the route to real change.
A little LOVE from Bolivian artist Bonny Lovy and Serkiel (Argentina)
Bonny Lovy Feat. Serkiel Amor Amor • 613,037 views • Bolivia & Argentina
Culture & Healthcare
Assault during pregnancy boosts risk of poor infant health
Author Beth Duff-Brown Published on September 17, 2020
Babies born to women who experienced an assault in their homes during pregnancy are more likely to be born prematurely and have a very low birth weight — which could lead to a lifetime of poor health and economic well-being, Stanford Health Policy research has found.
Health economist Maya Rossin-Slater, PhD, examined the effects of prenatal exposure to violent crime on infant health, using New York City crime records that are linked to birth records data. She and her colleagues found that in-utero assault significantly increases the incidence of adverse birth outcomes.
The findings were released in a NBER working paper last year; an updated version has since been accepted by the Review of Economics and Statistics.
In their analysis, the researchers found that assault during pregnancy leads to increases in the rates of very low birth weight (less than 3.3 lbs.) and low Apgar scores, a widely used metric for evaluating newborn health.
“Our results imply that interventions that reduce violence against pregnant women can have meaningful consequences not just for the women — and their partners — but also for the next generation and society as a whole,” Rossin-Slater said.
Findings timely due to COVID-19-related jump in domestic violence
Their research was conducted before the COVID-19 pandemic disrupted virtually every American household in a myriad of ways, including through an increase in domestic abuse. Rossin-Slater notes several studies have identified an association between stay-at-home orders and an increase in 911 domestic-violence calls and incidents in which police have been called to the scene. And there are likely many more cases that are not captured in the data.
That makes understanding the ramifications of domestic violence even more important, researchers believe.
“Lower-income pregnant women are more likely to be domestic violence victims than their more advantaged counterparts, and COVID-19 likely amplifies this disparity through the shelter-in-place orders,” said Rossin-Slater. “And then, the children of women who experience this violence are as a result also at a disadvantage — and this disadvantage may affect them throughout their life and even into their own children’s life.”
The research team also calculated the collateral economic damage of assaults on pregnant women.
They estimated that the annual social cost of violence during pregnancy in the United States is $3.8 billion to $8.8 billion. Those costs result from the increased rate of adverse birth outcomes, which in turn lead to a higher rate of infant mortality, increased medical costs at and immediately following birth, increased costs associated with childhood and adult disability, decreases in adult income, and reductions in life expectancy.
“Measuring the social cost of crime — and especially violent crime — is crucial for policy debates about the judicial system and programs that impact criminal behavior more broadly,” the authors concluded.
Source: https://www.sciencedaily.com/releases/2021/04/210428192712.htm

Risk of developmental difficulties remains high among children born early
Preterm birth continues to pose a large burden for families, healthcare, and educational systems, say researchers
Date: April 28, 2021 Source: BMJ

Children born preterm (before 37 weeks of pregnancy) remain at high risk of developmental difficulties that can affect their behaviour and ability to learn, finds a study published by The BMJ today.
These difficulties were found not only in children born extremely preterm (22-26 weeks) but also in those born very and moderately preterm (between 27 and 34 weeks), say researchers.
Survival of preterm babies has increased worldwide. Children born early often have developmental issues, but studies have mainly focused on those born extremely preterm (22-26 weeks’ gestation) and less is known about children born very and moderately preterm (27-34 weeks’ gestation).
Given how important it is to identify children most at risk of developmental difficulties, researchers in France set out to describe neurodevelopment among children born before 35 weeks compared with children born at full term.
Their findings are based on 3,083 French children aged 5½ born after 24-26, 27-31, and 32-34 weeks gestation who were taking part in the EPIPAGE-2 study (designed to investigate outcomes of preterm children over the past 15 years) and a comparison group of 600 children born at full term.
Neurodevelopmental outcomes such as cerebral palsy, sensory impairments (blindness and deafness), and brain function (cognition), as well as behavioural difficulties and movement disorders, were assessed using recognised tests.
To further assess the family and social burden of prematurity, measures such as the need for extra support at school, visits to a psychiatrist, speech therapist or physiotherapist, and parental concerns about development, were also recorded.
After adjusting for other potentially influential factors, the researchers found that rates of neurodevelopmental disabilities increased as gestational age decreased.
For example, among the 3,083 children assessed, rates of severe to moderate neurodevelopmental disabilities were 28%, 19% and 12% and rates of mild disabilities were 39%, 36%, and 34% among children born at 24-26, 27-31 and 32-34 weeks, respectively.
Assistance at school was used by 27%, 14% and 7% of children born at 24-26, 27-31, and 32-34 weeks, respectively. And about half of children born at 24-26 weeks received at least one developmental intervention which fell to 26% for those born at 32-34 weeks.
Behaviour was the concern most commonly reported by parents.
Rates of neurodevelopmental disabilities were also higher in families with low socioeconomic status.
This is an observational study, so can’t establish cause, and the researchers point to some limitations that may have affected their results. However, by assessing a wide range of developmental and behavioural issues, they were better able to reflect the complexity of difficulties faced by these children and their families.
As such, they say their findings indicate that preterm birth “continues to pose a large burden for families, healthcare, and educational systems.”
Although rates of severe to moderate neurodevelopmental disabilities decreased with increasing gestational age, they point out that around 35% of the moderately to extremely preterm born children had mild disabilities requiring special care or educational services.
And a considerable proportion of parents had concerns about their child’s development, particularly about behaviour, which warrant attention, they add.
“Difficulties faced by these groups of children and their families should not be underestimated,” they conclude.
Source: https://www.sciencedaily.com/releases/2021/04/210428192712.htm

PREEMIE FAMILY PARTNERS

Exercise aids the cognitive development of children born preterm
Date: May 6, 2021 Source: University of Basel
Summary: A premature start in life can cause problems even into teenage years. A study indicates that training motor skills in these children helps even when they are older.
A premature start in life can cause problems even into teenage years. A study by the University of Basel and the University Children’s Hospital Basel (UKBB) indicates that training motor skills in these children helps even when they are older.
Children that are born before the 37th week of pregnancy remain under close medical supervision while they are young. Any cognitive limitations often disappear after a few years. However, children who come into the world even before the 32nd week of gestation still exhibit differences even into their teenage years. In a new study, researchers led by Dr. Sebastian Ludyga and Professor Uwe Pühse have demonstrated that these children have weaker impulse control compared with children born at term (after the 37th week of pregnancy). This can, for example, have disadvantages in school performance and is linked to behavioral problems and a higher susceptibility to addiction.
As the research team reports in the journal Developmental Cognitive Neuroscience, these differences in impulse control can be fully explained by the children’s motor skills. “In other words, premature children who had very well-developed motor skills were practically equal to children born at term when it came to impulse control,” explains Ludyga.
In their study, the researchers compared a group of 54 very preterm children aged 9 to 13 years with a control group of children of the same age who had been born at term. To test impulse control, the sports scientists conducted a “go/no go” test with the children. When given a signal, the young study participants had to push a button as quickly as possible. When given a different signal, they were not allowed to push the button — in other words, they had to suppress their impulse to move.
During the experiment, the researchers monitored certain brain activity parameters using an EEG (electroencephalogram) to determine how the children processed the stimulus. A comparison of the two groups showed that on average, the premature children found it more difficult to suppress the impulse to move due to impaired attention processes.
In further experiments, the researchers tested gross and fine motor skills, as well as ball handling. They found that the greater the deficit in motor skills, the more limited the impulse control in the children born very preterm.
“We conclude from these findings that targeted motor skills training could also reduce cognitive limitations,” explains Ludyga. The researchers now want to test this in a follow-up study.
Ludyga says that there are few support options for very premature children as they grow into teenagers unless they come under scrutiny for a different reason, such as ADHD or another illness: “Limited impulse control at this age, even if it sorts itself out later, can have negative consequences and restrict these children’s educational opportunities.”
In younger children in particular, the development of motor and cognitive skills are closely linked. The time window from 9 to 13 years is therefore a promising period in which to reduce cognitive deficits in children born very preterm.
University of Basel. “Exercise aids the cognitive development of children born preterm.” ScienceDaily. ScienceDaily, 6 May 2021. <www.sciencedaily.com/releases/2021/05/210506105422.htm>.
Source: https://www.sciencedaily.com/releases/2021/05/210506105422.htm
What Parents Want to Know after Preterm Birth

EDITORIALS| VOLUME 200, P10-11, SEPTEMBER 01, 2018 Edward F. Bell, MD Matthew A. Rysavy, MD, PhD Published: May 08, 2018
When faced with the birth of a child born very preterm, most parents’ first question is, “Will our baby live?” Then, “If so, how will she be?” or “What will his life be like?” And finally, “What will our lives look like now?” Generally, parents do not ask, “Will our child have neurodevelopmental impairment?” or “Will our child have a Bayley cognitive composite score less than 85?”
So why has “neurodevelopmental impairment” become the standard measure for neonatal studies? Why has it become central to the way we counsel patients’ families and discuss prognoses with them? Do our answers address the real concerns and needs of parents of infants born preterm?
The focus on certain aspects of neurological development as the primary outcome after preterm birth may be, in part, an accident of history. The largest and most rigorous study of infant outcomes in the 1960s, the same decade that the term neonatologist first came into use, was the Collaborative Perinatal Study, organized by the then National Institute of Neurological Diseases and Blindness. This study informed the methods for conducting follow-up assessments and provided a benchmark for subsequent outcome studies.
The term neurodevelopmental impairment, now in common use, came to incorporate the outcomes of such studies, including motor and sensory development, cerebral palsy, deafness, and blindness.
Is it possible that we present parents with information about neurodevelopmental impairment because it is what we measure? What outcomes are actually most important to parents?
In this volume of The Journal, Jaworski et al report the results of an analysis comparing parents’ reports of their prematurely born children’s well-being at 18- to 22-month follow-up with the categorization of neurodevelopmental impairment based on research definitions of the Canadian Neonatal Follow-Up Network.
The investigators evaluated 190 children born very preterm. They also asked the children’s parents an open-ended question, “What concerns you most about your child?” and asked the parents to “Please describe the best things about your child.”
The main result was that there was no association between the themes used by the parents in describing their children, which were predominantly positive, and the presence or degree of neurodevelopmental impairment. The rates of positive aspects and physical health concerns were similar among all groups, but the reporting of developmental concerns was most frequent among parents of children with mild or moderate impairment; two-thirds of parents of children in this group reported concerns about their children’s development. Parents of children with no impairment or severe impairment were less likely to report concerns—approximately one-half in each group. The result for the severely impaired children must be viewed with caution, as there were only 15 children in this group. Other limitations include the lack of data from the parents of 41% of the survivors eligible for follow-up and the absence of information about how parents of healthy children born at term would respond to the same questions.
The authors observed that parents’ concerns often were not included in the standard definition of neurodevelopmental impairment. Although development was of concern to many parents, many also worried about behavior, such as hyperactivity and aggression. Parents also worried about feeding issues and growth.
The overwhelming message is that many parents of infants born very preterm view their children as having a good personality, being happy, and making developmental progress. Nevertheless, one-half or more of parents in all groups were concerned about their child’s health and development. And, perhaps most important, there was no correlation between the parents’ perception of their child’s status and the degree of neurodevelopmental impairment as graded by standard testing.
This leads to the questions, “What is a satisfactory outcome?” and “Who should decide?” To answer the second question first, it seems that only the individual born prematurely can determine whether her outcome is satisfactory, and until she is old enough to express this for herself, her parents must speak for her. We have heard repeatedly that children and adults born prematurely and their parents are, as a rule, happy with their lives, at least as happy as their counterparts born at term.
As healthcare providers, we should give up the idea that we are trying to protect families and children from unspeakable horrors when we warn them of the daunting risks of very preterm birth. This is not what they want to hear, and these dire forecasts do not give the whole picture.
We should state the risks compassionately and accurately and temper this worrisome news with the possibility of good outcomes as well as bad ones.
The study of Jaworski et al also raises questions about which long-term outcomes we should assess in neonatal studies. How can we conduct better research that addresses what parents and survivors of preterm birth find most important? Moreover, what is the best way to use this research to relay the results to those who can use them?
It is time to include in our research outcomes that are most important to parents. We have the rudiments of guidance in this task, but we could use more input from parents in defining outcomes that are of practical importance to them and their children. This may require developing new measurement tools.
This effort is not entirely new. A few of our pioneer follow-up investigators recognized this need and have addressed it well; yet, the opportunity remains for most of us to do much better. Jaworski et al contribute to a growing body of evidence that challenges the way we think about prognosis for infants born preterm. They remind us that we must ask parents, and whenever possible former patients, what outcomes are most important to them, and we must listen to their answers.
Source: https://www.jpeds.com/article/S0022-3476(18)30526-2/fulltext

When the Stress of the NICU Goes Away, Trauma May Last
April 13, 2021

Newborn babies who need intensive or specialized medical attention are often admitted to the Neonatal Intensive Care Unit until they’re healthy enough to go home, but research has found that even after a baby comes home from the NICU, many parents find themselves dealing with their own long-lasting effects.
According to statistics kept by the March of Dimes, in 2019 there were 3,744 preterm births in Dallas County — or 10 percent of all live births. In Tarrant County, there were 2,874 preterm births, or 10.6 percent of all live births. About one in 10 babies is born prematurely each year in the United States, the March of Dimes says.
A preterm birth is a birth that occurs prior to 37 weeks of gestation. While preterm and premature are often used interchangeably, the World Health Organization says there are three levels of premature births—late preterm, or born after 32 weeks but before 37 weeks; very preterm, or born between 28 weeks and 32 weeks; and extremely preterm, or born before 28 weeks.
Even if their baby spends little time in the NICU, a parent can find themselves reacting to similar situations, smells or even sounds months after. Studies have found that post-traumatic stress disorder (PTSD) and/or acute stress disorder are not uncommon among parents of children who spent time in the NICU.
In a study published in Europe’s Journal of Psychology, researchers surveyed 21 Italian parent couples of preterm infants and 29 couples of full-term babies. All parents filled out the same questionnaires designed to measure how they were reacting to the stressors they were experiencing.
The study found that mothers and fathers of preterm infants reported more tension, depression, anger and fatigue than parents with full-term babies.
“Our findings suggest that parents of premature babies, in particular mothers, since the birth of their babies, are at risk of developing higher levels of anxiety, depression, anger and stress,” the article says. “Furthermore, the preterm infants’ external characteristics and signals associated with immaturity and severity of medical status could be a further stressor especially for mothers.”
A similar study in Poland also found that parents of premature babies were at higher risk for PTSD.
Everything that can happen in a NICU—the health of the tiny infants, the noises, the uncertainty—can certainly provide the circumstances for developing PTSD, says Donald Hafer Jr., Ph.D., director of the Texas Health Behavioral Health Service Line, especially when you also consider the potential traumatic surroundings of the birth that brought the baby to the NICU to begin with.
PTSD, Hafer explains, is diagnosed after someone has been having symptoms for more than 30 days. “Acute Stress Disorder can be diagnosed from day one to day 30, and the criteria are pretty much the same,” he says.
“It always has to be tied to some event; it could be something that actually occurred to you, that you saw happen, or even that you heard about,” Hafer says. “You can develop this vicariously.
“And PTSD can show up later—it doesn’t always, but it could come even years later.”
There are four main ways PTSD symptoms may manifest:
- Reliving the event (nightmares, flashbacks or something that triggers a memory of a traumatic time);
- Avoiding situations that trigger memories of the traumatic event, or even avoiding discussing the event;
- Negative beliefs and feelings (anxiety about the future, difficulty in having positive or loving feelings toward people);
- Hyperarousal (feeling like you must be on the lookout for danger, trouble sleeping, trouble concentrating)But not everyone who spends time watching over their infant in the NICU will experience PTSD, Hafer says.
But not everyone who spends time watching over their infant in the NICU will experience PTSD, Hafer says.
“You can be there, seeing this traumatic experience, and for some people there’s trauma, and for some people there’s not,” he explains. “If you’re there and there’s a big code on a baby, whether it’s yours or not, that can be a traumatic experience.
“It really all depends,” he continues. “Not everyone with a NICU stay has the same experience. For some, it is a relatively short stay with minimal medical complications and for others, it turns into months of one crisis followed by another.”
Whether that trauma continues to affect someone can often depend on what a parent has dealt with in the past.
“Trauma for one person is not the same as for another, based on their past life experiences,” Hafer explains. “Seeing your child in NICU, or vicariously seeing another child go through a code may become a trauma trigger.”
Hafer says that treatment for PTSD can take many forms. For some, knowing their triggers and avoiding the ones they can is helpful. “You may or may not be able to avoid them,” he says.
Sometimes medication is helpful, especially if there is underlying depression or anxiety tied to the PTSD, Hafer says. Others find a more psychoanalytical route helpful.
“There are also effective strategies that are symptom-based—things like breathing training, cognitive therapy, and relaxation training—that help you cope with the symptoms,” he says. “Sometimes it’s a matter of self-talk, asking if you’re saying things to yourself that could be exacerbating your anxiety.”
And sometimes seeking out people that have been in the same boat is helpful, too. One study published in the Canadian Medical Association Journal found that 16 weeks after preterm birth, mothers who were matched with parents who had lived through the NICU experience already had less anxiety and depression and felt they had more social support.
But if a parent does feel that they are experiencing PTSD, help is available.
“You need to visit with a mental health professional who is familiar with treating PTSD,” Hafer says. “You can start by talking to your MD about a referral, or you can call Texas Health Behavioral Health and schedule a free hour-long screening at any of our 20 locations within 24 hours.”
Source: https://areyouawellbeing.texashealth.org/stress-nicu-goes-away-trauma-may-last/
Other Resources: MARCH OF DIMES: https://www.marchofdimes.org/nicufamilysupport/index.aspx
INNOVATIONS

TACKLING HEART DISEASE IN BOLIVIA WITH THE NIT OCCLUD DEVICE
September 03, 2020– Natalie Clark Photo: Flickr

Bolivia is the second poorest country in South America, performing poorly in education, life expectancy, economic strength and overall development. Most alarmingly, it lacks sufficient medical care due to a limited supply of adequate resources. Bolivia’s unique geography advances its tremendous healthcare challenges, causing children to be 10 times more likely to be born with congenital heart defects. These conditions are nearly impossible to treat without trained cardiologists and updated facilities, two things often inaccessible to most Bolivians. Thus, addressing heart disease in Bolivia is quite challenging as a result of these factors. However, Franz Freudenthal, inventor and cardiologist, is improving medical care with a simple technique that utilizes an indigenous hobby to heal holes in hearts.
What is PDA?
Patent Ductus Arteriosus (PDA) is a common congenital heart defect, particularly prevalent in certain parts of Bolivia. The defect is caused by an opening between two major blood vessels traveling away from the heart. The opening is crucial to a baby’s circulatory system before birth, but it should close almost immediately upon exiting the womb. PDA cases, however, present holes in the heart that remain open. Although the exact cause of congenital heart defects like PDA is typically unclear, decreased oxygen levels have a direct impact on fetal heart health. Because La Paz, Bolivia sits at 3,600 meters above sea level, where the atmosphere has lower oxygen levels than most parts of the world. Therefore, Bolivia’s altitude is the likely cause of irregular blood. Also, the mother’s inability to provide appropriate oxygen levels to her child can result in severe complications.
Breathlessness and failure to thrive are the most common symptoms in mild cases, but fatigue and failure to gain weight can also occur because harmed hearts must work three times harder to pump blood than healthy hearts. Children with severe cases of PDA are at a higher risk for pulmonary hypertension, arrhythmias, infective endocarditis, anticoagulation and congestive heart failure. However, each of these symptoms can be relieved by skilled women in the Andes Mountains’ high plains.
Ingenuity to Fight Heart Disease in Bolivia
Aymara women have been knitting clothes and blankets for centuries, but with help from Franz Freudenthal, they are now knitting heart-closure devices to mend PDA. The Nit Occlud is a hi-tech medical advancement modeled after an occluder, an industrially-produced device intended to block holes in babies’ hearts. Unlike a normal occluder, the Nit Occlud’s design cannot be mass-produced due to its intricate design. Therefore, Freudenthal had to search for an alternative production plan. The perfect method, he soon found, was the wonderful weaving skills of the Aymara women.
The Nit Occlud is composed of a super-elastic metal known as nitinol, a nickel-titanium alloy capable of memorizing its own shape. After a doctor inserts the device through the body’s natural channels, it travels through blood vessels, expands to its original shape, plugs the heart’s hole and permanently restores basic cardiac functionality.
Typical treatments for PDA include surgical procedures, cardiac catheterizations, or heart transplants, but these are not available Bolivia and are not welcomed by the Aymara people. Even though the Aymara people have recently adopted Catholicism, they still believe in the power of the Andes Mountains spirits and their effects on human souls. Keeping in mind that manipulating a heart – performing open-heart surgery or a transplant – is considered desecration according to the spirits, Freudenthal created a minimally invasive innovation to respect patient beliefs and to “make sure that no child is left behind.”
Making Impact
Although congenital heart defects remain the fourth leading cause of premature deaths in Bolivia, the rate has dropped 36% since 2007. Freudenthal’s Nit Occlud has saved more than 2,500 children in nearly 60 countries after experiencing immense success in Bolivia. The country is also succeeding in its fight against poverty. The number of Bolivians living on less than $3.20 a day is projected to decrease by 35% in the next 10 years. Additionally, more children are being vaccinated and more prenatal care opportunities are becoming available to mothers. With these advancements in healthcare and poverty reduction, the economy will soon flourish and rates of heart disease in Bolivia are sure to drop.
Source: https://borgenproject.org/heart-disease-in-bolivia/

Higher levels of nitrate in drinking water linked to preterm birth, Stanford study finds

Women exposed to higher levels of nitrate in drinking water were more likely to deliver very early, according to a study of 1.4 million California births
Pregnant women exposed to too much nitrate in their drinking water are at greater risk of giving birth prematurely, according to a Stanford University study of more than 1.4 million California births.
Agricultural runoff containing fertilizer and animal waste can greatly increase the nitrate level in groundwater, which naturally contains a low level of the chemical.
“We found that higher concentrations of nitrate in drinking water during pregnancy were associated with an increased risk of spontaneous preterm birth, even at nitrate concentrations below the federal regulatory limit,” said Allison Sherris, a graduate student in the Emmett Interdisciplinary Program in Environment and Resources at Stanford. “That was surprising.”
The study, which published online May 5 in Environmental Health Perspectives, is the largest ever to connect nitrate exposure and premature birth. Sherris is the lead author. The senior author is Gary Shaw, DrPH, professor of pediatrics.
The research found that the risk of early preterm birth, in which an infant is born at least nine weeks early, more than doubled among women whose tap water had nitrate levels that exceeded the federal limit of 10 milligrams per liter compared with those whose tap water nitrate levels were less than 5 milligrams per liter. The risk was elevated by about half among women exposed to a moderate level of 5-10 milligrams per liter of nitrate in their water. Later preterm births, in which an infant arrives three to eight weeks early, were also associated with elevated nitrate, but the connection was less pronounced.
Early preterm births are fairly rare, composing less than 1% of all births, but are medically severe for affected infants. These preemies typically require long hospitalizations and can experience short- and long-term complications with vision, hearing, digestive function and neurological development.
“If we can prevent even a fraction of these births, that would be enormously beneficial,” Sherris said.
The federal safety limit of nitrate in drinking water was set after it was discovered that newborns drinking formula mixed with high-nitrate water can develop “blue baby” syndrome, in which infants’ blood carries too little oxygen. Both fetuses and young infants have a special oxygen-carrying protein in their blood called fetal hemoglobin, which is especially susceptible to damage by nitrate.
“Our drinking water matters,” Shaw said. “Water is a very complicated thing to study, but it’s important to know if there are risks associated with what’s in our water.”
Analysis of sibling births
The study drew on records of more than 1.4 million births of sibling pairs who were born to about 650,000 women in California between 2000 and 2011. The siblings in the study were not twins or other multiples but had the same mother. Comparing siblings helped the researchers control for factors that might influence preterm birth independently of nitrate exposure, such as the mothers’ genetics, socioeconomic status and dietary habits.
“The within-mother approach gives us confidence in our findings,” Sherris said.
The researchers used public data on nitrate levels in local drinking water systems at the mothers’ homes to estimate their nitrate exposures during each pregnancy. Some women in the study had the same exposures for multiple pregnancies, whereas other women were exposed to different nitrate levels, either because the amount in their local drinking water changed, or because they moved between pregnancies.
Compared with women exposed to the lowest nitrate level of less than 5 milligrams per liter, the odds of spontaneous preterm birth occurring nine or more weeks early was 47% higher in women exposed to 5-10 milligrams per liter, and 252% higher in women exposed to more than 10 milligrams per liter in drinking water.
The link between preterm births that happen four to eight weeks early and nitrate exposure was not as strong. This was not surprising, as other research has suggested that early and later preterm births may be biologically distinct phenomena with different causes.
The strongest effects of nitrate on prematurity risk were seen in California’s agricultural regions, including the San Joaquin Valley and the Inland Empire, the study noted.
A higher proportion of births in these areas are to Hispanic women than in other regions of the state, said Sherris, adding, “This is one of many environmental justice issues facing women in rural California.”
Further research may help inform whether stricter regulations are needed for nitrate levels in drinking water, the researchers concluded.

Telehealth for Prenatal Care Gets Seal of Approval From Patients, Providers
Majority say that telemedicine should continue post-pandemic by Amanda D’Ambrosio, Enterprise & Investigative Writer, MedPage Today May 4, 2021
Patients and providers felt that prenatal care via telemedicine was safer, more accessible, and cost-effective during the COVID-19 pandemic, a survey found.
Three-quarters of patients stated that they felt safer using telehealth for their obstetrics care during the pandemic, with 18% responding that they would have forgone care if telehealth wasn’t available, reported Karampreet Kaur, a medical student at Vanderbilt University School of Medicine in Nashville.
More than 95% of healthcare providers also felt that providing prenatal care via telemedicine was safer than in-clinic for themselves, their patients, and their peers, she noted during a presentation at the American College of Obstetricians and Gynecologists (ACOG) virtual meeting.
“From our survey study, we found that overall both obstetrical patients and providers believe telehealth was a safe modality that improved access to obstetrics care during the COVID-19 pandemic,” Kaur said. “A majority believe that telehealth options should be considered for delivery of prenatal care independent of COVID-19.”
The survey results showed that telemedicine allowed patients to save money on transit and childcare, as well as reduce their missed wages. Future studies should include a more comprehensive cost analysis, to further understand savings associated with telehealth for both obstetrics patients and hospitals, she added.
Kaur’s group collected self-administered survey data from obstetrics patients and providers at Vanderbilt University Medical Center. They included clinicians, advanced practice providers, genetic counselors, social workers, and registered dietitians. The researchers received responses from patients from June 2020 to April 2021, but only collected answers from providers during the summer of 2020. All patients included in the survey had at least one prenatal appointment via telehealth.
The researchers obtained survey data from 167 patients, more than half of whom were ages 25 to 34. Around 70 providers responded to the survey, the majority being MDs or DOs.
Of all patients who responded to the survey, 44% last saw a generalist, 28% saw a maternal-fetal medicine specialist, 26% saw a genetics counselor, and just 1% saw a social worker. Approximately 84% of all telemedicine visits were conducted at home, while the remaining 16% were conducted at a clinic, most frequently after an in-person ultrasound appointment.
Around 75% of patients agreed that telehealth reduced their travel time, and almost half saved at least $35 in transportation, childcare, and missed wages. The researchers found that 95% of patients were satisfied with their telehealth obstetrics care, and 96% thought that the state of Tennessee should develop a permanent telehealth obstetrics program.
In their analysis of provider responses, Kaur’s group concluded that 94% of providers thought telehealth was an acceptable way to provide obstetrics services, 85% said that telehealth allowed for high-quality communication with their patients, and 96% agreed that telehealth improved patients’ access to obstetrics healthcare.
Nearly all providers who responded to the survey said that they’d be willing to use telehealth for obstetrics care outside of the pandemic, and that the Vanderbilt telehealth system was positive for the state of Tennessee.
Kaur acknowledged that this study was limited by both non-response bias and sampling bias. As the survey was administered electronically to patients on smartphones or computers, patients without access to these technologies may not have been able to respond.
Source: https://www.medpagetoday.com/meetingcoverage/acog/92409

Disparities in the follow-up of very preterm born children in Europe

With a letter issued in February 2021, a group of researchers presented an analysis of the cross-European disparities of routine follow-up services of children who were born very preterm (<32 weeks of gestational age (GA)). It was found that the mother’s sociodemographic characteristics and her perinatal situation were among the main factors regarding these disparities.
Aiming to describe the use of follow-up services in Europe, the research team collected data from obstetric and neonatal records from 19 regions across 11 European countries. A population-based analysis was conducted using standardised parental questionnaires. The goal was to evaluate the use of routine follow-up services on 3635 children born before 32 weeks of gestation and until their fifth birthday.
Despite the limitations concerning parental recall, the study presented interesting results, stating that 90.3% of the children had used follow-up services, and 27.3% continued with these until the age of five. A family’s lower socioeconomic status was associated with use of follow-up services. Mothers younger than 24 years and mothers born outside of Europe were two groups associated with never having used follow-up services. This underuse is concerning, as their children already belong to a vulnerable minority. Infants with perinatal risk factors such as low GA, small for GA or bronchopulmonary dysplasia (BPD), were among the group to continue follow-up services at older age. Interestingly, the group of male preterm babies used more follow-up services than the female group.
Given the importance of follow-up appointments in children born very preterm, and considering that the most affected groups shown in the study are already in a challenging life situation, the study highlights the need for standardisation in follow-up protocols and calls for action in this regard.
EFCNI was part of the SHIPS Research Group – one of the main data contributors and collaborators of this study.
Paper available to view at: British Medical Journal

HEALTHCARE PARTNERS
New device uses harmless light particles for real-time monitoring of newborn babies’ brains

An estimated 500,000 babies born around the world each year develop unnecessary brain damage that could be treated if caught in time – but monitoring these infants’ delicate brains is extremely difficult. However, spotting these underlying causes at a critical, early stage, a new photonics device currently in development aims to reduce unnecessary disabilities by improving the instant, real-time monitoring of newborn babies with harmless light particles.
No medical tools currently exist to create a harmless, real-time, continuously moving image inside newborn babies’ delicate brains.
MRI scans can provide an accurate picture inside adults but are highly unsuitable for newborn babies, given they require a patient to sit still while giving out harmful radiation.
Neurodevelopment disabilities like cognition or motor skill impairments that affect half a million infants globally every year – resulting from defective heart vessels – can be treated but are difficult to monitor and catch in time.
However, the ‘TinyBrains’ health consortium run in conjunction with ICFO – The Institute of Photonic Sciences in Barcelona is developing a new wearable device to help doctors see what is going on inside infants’ minds quicker than ever.
Putting near-infrared lasers and LEDs into a small, wearable cap that are combined with EEG electrodes, the scientists send harmless signals into the infant’s brain – working almost like an ultrasound scan, but using photonics (or light) to give much more information, a more detailed picture and an image of the underlying brain activity rather than the anatomy.
The signals can measure the cause of so many unnecessary neurodevelopment disabilities by keeping a close eye on any slight drops in critical oxygen levels to and from the brain instantaneously in real-time.
Heart defects and neurological complications
TinyBrains project coordinator, Professor Turgut Durduran, said: “A staggering 500,000 people suffer unnecessary disabilities that result from congenital heart defects (CHD) and other structural defects in the heart across the world, drastically affecting the life of the patient if they are not picked up soon after birth.
“At present, it is tough to monitor these at-risk populations both technically, because of the lack of appropriate tools, and also ethically because consent and risks have to be taken into consideration.”
Each year 3.4 million babies worldwide are born with a congenital disability, and of these, congenital heart defects (CHD) are the most frequent. About 40% of these infants need a cardiac surgical intervention during their first year of life with a subsequent stay in the intensive care unit.
Most of these babies survive to adulthood but risk suffering from deficits in their neurological development due to brain blood flow and perfusion alterations happening during the intervention. These alterations often result in learning disabilities, leading to low quality of life for these patients and their families, constituting a significant challenge to public health.
Scanning with light
The cap’s sensors connect to a portable unit and measure the cerebral metabolic rate of oxygen – or the oxygen saturation in the blood and the concentrations of oxy- and deoxy-hemoglobin – and build up a 3D color image in real-time.
“We are using high-density near-infrared spectroscopy (fNIRS) and diffuse correlation spectroscopy (DCS) to measure the oxygen saturation levels in the blood. By integrating both of them with an imaging device as the electroencephalography (EEG), the resulting 3D images have higher resolution, increase the brain specificity and penetration and for the first time, a spatial resolution to this class of measurements.” Turgut Durduran, Professor and Project coordinator, TinyBrains
By identifying brain function alterations during surgery and stays in intensive care units will allow doctors to analyze why brain disorders frequently occur in the postnatal period and to pinpoint the types of clinical interventions that can improve the neurological outcome of these infants and, ultimately, their quality of life, as infants, young persons and adults.
Calling themselves TinyBrains, the consortium took their inspiration from similar scope and technologies: a national project called PhotoDementia, a twenty-year collaboration with the Children’s Hospital of Philadelphia, and projects from the European Commission – BabyLux (which monitored cerebral oxygen metabolism and blood flow for Neonatology), and LUCA, a similar light-based technology to monitor thyroid nodule screening to improve thyroid cancer screening.
Although each technology is different, the underlying principles are the same: using photons, or harmless light, to make an instant, non-invasive scan deep within the body.
Concluding in 2024, the TinyBrains project will conduct future trials at the Children’s Hospital Sant Joan de Déu in Barcelona.

Follow-up after very preterm birth in Europe

Follow-up programmes aim to detect neurodevelopmental and health problems and enable early interventions for children born very preterm (<32 weeks of gestational age (GA)). Although the importance of post discharge follow-up is widely acknowledged, recommendations differ regarding eligibility criteria, frequency, duration and content, especially for follow-up beyond early childhood. We used data from a European cohort of children born very preterm to describe the use of routine follow-up services until 5 years of age.
The data were collected for the Effective Perinatal Intensive care in Europe and Screening to Improve Health in Very Preterm Infants studies, which constituted and followed up an area-based cohort of children born very preterm in 2011/2012 in 19 regions across 11 European countries. Perinatal data were collected from obstetric and neonatal records, and parents completed questionnaires at 2 and 5 years of age. Out of 7900 live births, 6792 were discharged from neonatal care, of whom 6759 were alive at 5 years and 3635 (53.8%) participated in the study.
Based on a question on the use of routine follow-up services for children born very preterm in the 5-year parental questionnaire, we classified children as having never used follow-up, no longer using follow-up or still using follow-up services. We described associations with family sociodemographic characteristics and perinatal risks and estimated adjusted risks using multinomial regression models with robust variance estimators for clustered samples and inverse probability weights using baseline characteristics to account for study attrition bias.
Of all children, 90.3% had used follow-up services, and 27.3% (10.9 to 58.4% by country) were still doing so at 5 years of age. Never using follow-up services was associated with maternal sociodemographic characteristics (younger age, low educational level and being born outside Europe) and lower perinatal risk. Continued follow-up at 5 years of age was related to perinatal risk factors (low GA, small for GA, bronchopulmonary dysplasia and male sex). Children with mothers born outside of Europe were less likely to continue follow-up. Adjustments for social and perinatal characteristics failed to explain differences between countries.
This study provides novel data on use of routine follow-up services after preterm birth based on a population-based design and standardised questions on follow-up from diverse European regions. Limits are reliance on parental recall and study attrition.
Children from socially disadvantaged families were more likely to never use follow-up services, corroborating previous studies. This is concerning, as these children are more vulnerable to the adverse neurodevelopmental consequences of preterm birth, and may benefit most from interventions. Variation between European countries in the percentage of children continuing follow-up at five persisted after accounting for perinatal risk factors, such as lower GA and neonatal morbidities. While differences are expected, given the heterogeneity in follow-up policies and programmes, the magnitude of these cross-country disparities, in tandem with marked social inequalities at follow-up entry, underscore the need for better evidence on optimal follow-up organisation and duration.
Source: https://fn.bmj.com/content/early/2021/02/09/archdischild-2020-320823

Clinical Pearl: A Day in the Life: A Preemie Experience
Catherine Ney, MS, CCLS, Joseph R. Hageman, MD/ NEONATOLOGY TODAY Peer Reviewed Research, News and Information
Have you, as a clinician, wondered what it is really like to be a premature infant being admitted to the Neonatal Intensive Care Unit? Even after spending time as a patient in the intensive care unit after a cardiac arrest, intubated, then post-operatively following a four-vessel bypass as I did in 2013, I do not think I really know what it is like for a preemie.
Catherine Ney, my co-author, and colleagues in the Developmental Care Committee have organized an excellent simulation for NICU nurses, neonatal and pediatric nurse practitioners, residents, fellows, and faculty with help from the experts in our Simulation Unit at the University of Chicago. The simulation explores aspects of an admission experience includes admission procedures highlighting the effects of the sensory experience (i.e., sound, noise, taste, smell, light, and positioning). Additional components to effectively simulate the neonate’s experience included the sensation of a weighted positioner on your chest and movement restrictions due to an overly tight swaddle and poor positioning. One of the adults assumes the role of the patient as the providers complete admission tasks with a follow-up discussion regarding the effects on development, potential pathological effects, and how it must feel for the baby.
A comprehensive introduction, led by our Neonatal Nurse Practitioner Chris Elsen, highlights premature development through a developmental care lens that helps focus our participants before their breakout simulation sessions.
Pat Byrnes-Bowen, our physical therapist, explains the stages of development in utero and, as a consequence of preterm birth, what that infant will no longer have an opportunity to experience. As providers in this space, she discusses how we can use various tools and techniques to make the infant’s extrauterine life as physically supportive as possible. Pat explains how positioning needs change and how important proper positioning can be to aiding in a successful life as a young child and adult.
Moving through our additional stations, participants discuss taste and smell with Julie Sadowski, Speech-Language Pathologist, and myself (Dr. H). In this session, participants learn about the aspects of development in utero that prepare infants for feeding later and how exposure to noxious smells can interfere with bonding and deter patient’s from positive oral experiences. This simulation allows participants to smell common items used on or near these patients at a high concentration. They are encouraged to smell various containers and identify alcohol wipes, adhesive remover, and perfume. Even in the age of mask-wearing, these smells permeate without losing their potency.
As participants enter the sound and vision station, they often notice an iPad set up with a decibel reader that is left on throughout the discussion. Catherine walks them through the developmental components of life in utero and the fascinating way the evolution of pregnancy prepares infants for the outside world. For most of our patient population, this natural experience is stripped away as they are thrust into a space that assaults their immature sensory systems. As the discussion moves toward sound, graphs are highlighted with decibel level readings of physical spaces on our unit compared to the recommended level of 45dB’s. The discussion in the room spikes to the mid 70dB range with just one person talking . As the participants digest these thoughts, the lights are dimmed, and they are encouraged to get comfortable in their chairs with eyes closed as they are about to enter the world of a preemie for a few moments. Recorded sounds are played, starting with a heartbeat track that is layered with common noises on the unit. Participants appear visibly shocked as these noises begin and have thoughtful comments during our discussion.
Prior to the final discussion, all participants are gathered for a presentation on mindfulness. Working in the health care field and in an intensive care unit demands more than clinical competence. Compassionate care supports a family-centered model but can be hard to sustain amid the daily challenges on our unit, not to mention the global pandemic. Participants are encouraged to explore the use of G.R.A.C.E. to help support their cultivation of compassionate care toward their patients and families and find ways to support their capacity to do so. We also discuss what the clinicians can do to be more sensitive to the infant’s senses and developmental needs, optimize their NICU experience, and minimize the negative effects of this experience.
We have had several nurses, NNPs, fellows, and attending neonatologists experience this simulation, and the feedback has been really positive thus far. We have a debrief and ask them what can be done to improve the experience and have received a lot of helpful feedback to refine the simulation.
This is by no means a unique simulation as other NICUs have been doing this for a number of years (Phillips https://www.learningconnection.philips.com/en/course/preemie-day), and Catherine has spoken with clinicians from other units about their programs.
We will continue to refine this Day in the Life simulation and plan to do some follow-up surveys for those clinicians who have been through this to see if it has affected their practice in the NICU. An educational handout with summaries of development and the senses is also provided for the attendees.
A Day in the Life: A Preemie Experience Educational Handout is available through the link below

http://neonatologytoday.net/newsletters/nt-may21.pdf


Gotham Reads presents Jaimal Yogis, acclaimed writer, reading “Mop Rides the Waves of Life”. Going to school and navigating classmates can be hard—but all that goes away when little surfer Mop paddles out in the waves. With a few tips from his clever mom, Mop studies the wisdom of the water and learns to bring it into his life on land: taking deep breaths, letting the tough waves pass, and riding the good ones all the way. With newfound awareness and courage, Mop heads back to land—and school—to surf the waves of life. #GothamReads #JaimalYogis #MopRidesTheWavesOfLife
Kat’s Corner

How to Live Life to the Fullest and Enjoy Each Day


Have you ever felt like others don’t understand your pain when they seem to be living a happy life? You’re not alone in feeling this way, but the truth is that happiness takes work, and learning how to live life to the fullest takes dedication and practice.
People who smile in public have been through every bit as much as people who cry, frown, and scream. They just simply found the courage and strength to smile through it and enjoy life in the best way possible.
Life is short, and we only live once. Learning to live life to the fullest is an important step in making the most of every day. Here are 9 ways you can try.
1. Decide What’s Important to You
Whether it’s taking care of your children, working hard on your career, writing a new blog post each day, or baking up fabulous creations, you get to decide how you enjoy spending your time. Your parents, friends, community, and society in general all have their opinions, but at the end of the day, you’re the only person who will be around for every moment of your life.
Do what makes you happy, and everything else will fall into place. This may not mean finding your perfect job if you’re limited by education, location, or job openings. However, you can still do what you love by engaging in hobbies, volunteer work, or mentoring.
Want to discover what’s important for you? I recommend you make use of this 3-Step Guide To Break Free And Design the Life You Want. It’s a free guide to help you figure out what truly matters to you so you can align your everyday life with it and start to live the life you want. Grab your free guidebook here.
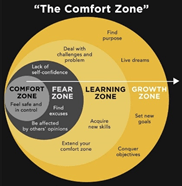
2. Take More Risks
Sometimes there’s danger involved in life, but every reward carries risk with it. If you never take risks, you’ll never get anywhere in life, and you certainly won’t learn how to live life to the fullest.
Staying in your comfort zone is the fastest way to become discontent[1]. Without stepping outside what you’re already comfortable with, you will cease to learn and stagnate in both your personal and professional life.
How Fulfilled Are You In Your Life?
While it may feel uncomfortable, taking a risk can be as simple as saying yes next time your friends want to go out instead of staying at home alone. It can mean going out on a blind date, buying plane tickets to a new city, or dragging out those paints that have been stuffed away for years.
When people look back on their lives, they regret the chances they didn’t take more than the ones they did, so find something new to try today and set goals beyond what you currently believe possible.
3. Show Your Love to People You Care About
Family and friends will always appreciate hearing that you love and appreciate them in everyday life. It will brighten a stranger’s day to hear a random compliment. If you like someone’s shirt, tell them. If you notice that they’re doing a great job not losing their temper while their kid screams in the supermarket, let them know.
If you have a romantic interest in someone, just go for it. There are a lot of ways it may end, and only one of them keeps them in your life forever. In the end, you may look back and wish you had asked them out.
4. Live in the Present Moment
Your past is important to learn from. Your future is important to work towards. At the end of the day, though, the only thing that exists outside of your head is the present.
In order to ground yourself in the now, you can practice mindfulness, which involves learning to live in the moment by noticing what’s around you, how you’re feeling, why you’re feeling that way, etc. Meditation can also help with this as it helps you get in touch with your thoughts and feelings.
Gratitude is another amazing tool for living in the present[2]. Each day, practice gratitude by writing down three to five things you’re grateful for. You’ll be amazed and how quickly this helps place you in the moment and start to live life to the fullest.
5. Ignore the Haters
No matter what you decide to do with your life, there will always be someone around to point out the many ways you’ll fail or what you’re doing wrong with each step you take.
Know that every winner loses, but not every loser wins. Successful people don’t start out successful. What makes them successful is that they keep pushing through failure.
Next time you run into a hater, work on placing boundaries and practice self-love to build your self confidence and make it impenetrable to the outside forces trying to break it down.
Take a look at these 10 Famous Failures to Success Stories That Will Inspire You to Carry On.
6. Don’t Compromise Your Values
If something doesn’t feel right, don’t do it. Don’t compromise on your internal code of ethics, as this will leave you feeling empty and full of regret.
Life doesn’t work like a movie. It’s filled with gray areas. Trust your instincts, and do whatever you want so long as you can look yourself in the mirror with appreciation and love.
7. Be Kind to Others
Every day, you’ll see someone who could use help. While you may not be at a place to help them financially, offering a smile or a kind word can do wonders to help someone feel better about where they’re at in life[3]. When others see you practicing kindness, they’ll also be more likely to do so, which can help everyone learn how to live life to the fullest.
You can also try these 29 Ways to Carry Out Random Acts of Kindness Every Day in order to live life to the fullest.
8. Keep Your Mind Open
Having an open mind is important for your growth. Just because you’re right about something doesn’t mean there aren’t other ways to look at it.
Listening to ideas you don’t agree with or understand keeps your brain active and healthy. You’ll continue to learn as long as you stay open to difficult conversations. Don’t assume you know everything about another person, as they always have more to teach you.
Here’re 5 Ways to Cultivate a Growth Mindset for Self Improvement.
9. Take Action for What Matters to You
You’ll hear people say, “I had that idea,” every time you see someone create something great. Everyone had the idea for Facebook first. The reason Mark Zuckerberg got rich off of it is because he went out and did it while everyone else was talking about it.
Ideas are useless if you don’t act on them. Less thinking, more doing.
The Bottom Line
Learning to live life to the fullest is a big step in discovering a path that will lead you to your greatest sense of happiness and accomplishment. We all need moments to rest and relish in a sense of contentment, but staying in one place too long will leave you feeling a lack in life. Discover what makes your life feel meaningful and go after it.
Source: https://www.lifehack.org/articles/communication/how-live-life-the-fullest.html

— THE ALTIPLANO PROJECT — Country: Bolivia Location: Uyuni, Potosi (The world´s largest salt flat located in the Altiplano region at a height of 3653 m with a surface of 10.582 km² Because we couldn´t find any information that somebody has ever tried to fly there with a paraglider without a motor, we started the Altiplano project. We developed a system to safely tow a paraglider behind a car into the air. The project started already in Germany where we did some tests. We used a 250 meter-long rope with a special strain. We had a breaking point on the paraglider and wipple trees on the car. The only problem was the big height. The Paraglider is really fast because of the thin air. After a few tests it was finally working. 🙂

