


Cape Verde, also referred to in English by its Portuguese name Cabo Verde, and known officially as the Republic of Cabo Verde (Portuguese: República de Cabo Verde), is an archipelagic country in the central Atlantic Ocean off the coast of West Africa. It consists of ten volcanic islands with a combined land area of about 4,033 square kilometres (1,557 sq mi). These islands lie between 600 and 850 kilometres (370 and 530 miles) west of Cap-Vert (i.e., Dakar), the westernmost point of continental Africa, after which they are named. Cape Verde forms part of the Macaronesia ecoregion, along with the Azores, the Canary Islands, Madeira and the Savage Isles.
Cape Verde became independent in 1975. Since the early 1990s, it has been a stable representative democracy and has remained one of the most developed and democratic countries in Africa. Lacking natural resources, its developing economy is mostly service-oriented, with a growing focus on tourism and foreign investment. With a population of around 530,000 (as of 2026), Cape Verde is among the least populous countries in Africa. With a population of around 530,000 (as of 2026), Cape Verde is among the least populous countries in Africa.
Healthcare in Cape Verde Starting from July 2012, a telemedicine program, funded by the Republic of Slovenia through ITF Enhancing Human Security and implemented by the US-based NGO, the International Virtual e-Hospital, is building a hospital-based telemedicine network for the whole country. As of January 2014, all the inhabited islands of the country are connected through an integrated telemedicine network representing the first case in Africa of such an approach to telemedicine.
Source:https://en.wikipedia.org/wiki/Cape_Verde
STATS
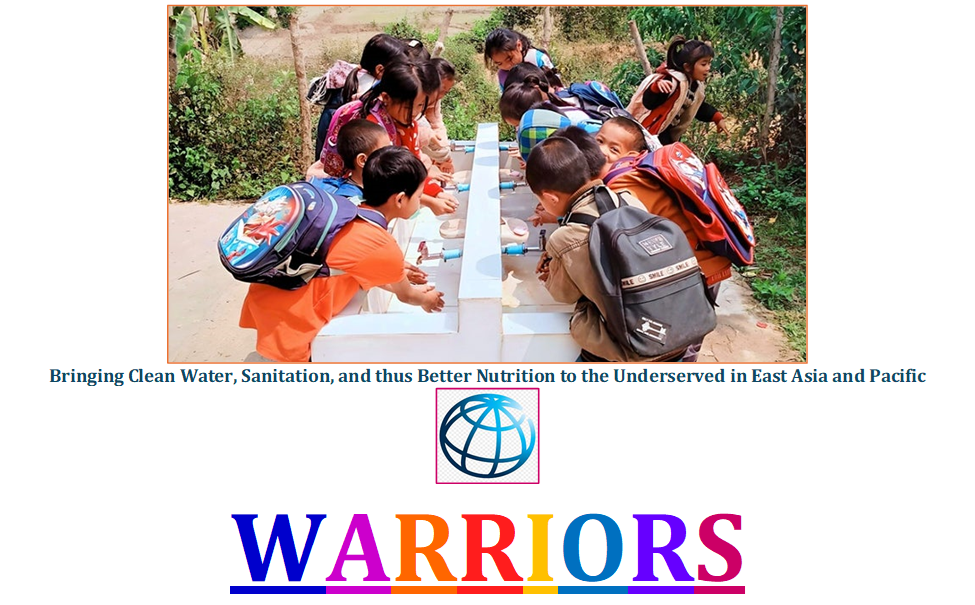
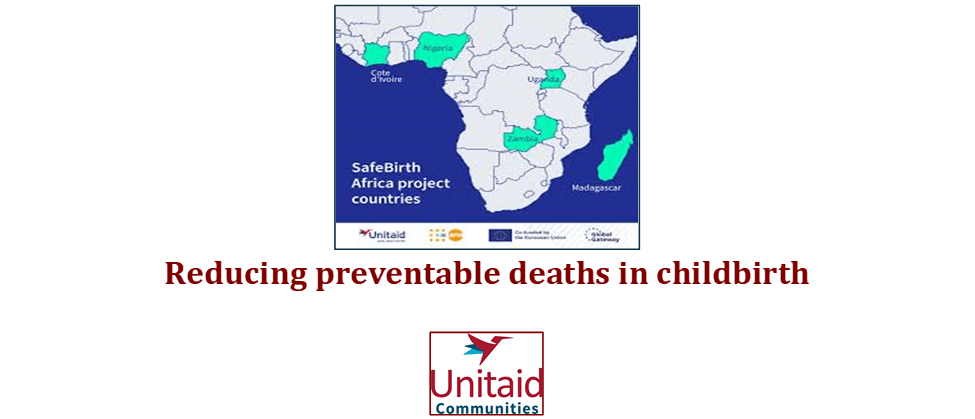
- GLOBAL PRETERM BIRTH RATES – Loas
- Estimated # of preterm births: 6 per 100 live births
- (Global Average: 10.6)
- Source- https://worldpopulationreview.com/country-rankings/preterm-birth-rates-by-country
It’s tempting to think of telemedicine as a pandemic-era invention, something born out of necessity in 2020. In reality, the idea of treating patients across a distance is more than a century old, and its evolution says as much about politics, insurance systems, and geography as it does about technology.
The seeds were planted long before video calls existed. In the 18th century, Claude Chappe’s optical telegraph laid the groundwork for transmitting information across distance, and by the late 1800s the United Kingdom had become the first country to link communication technology to the actual practice of medicine, a relationship that deepened from 1864 through 1945. In 1905, physiologist Willem Einthoven inventor of the electrocardiograph transmitted heart sounds by telephone from a hospital to his laboratory, and by 1910, American cardiologists in New York had published the first U.S. review describing electrocardiograms successfully sent by cable from hospital wards to the ECG room].
Radio Waves Over the Outback
If there’s a single moment that captures telemedicine’s founding spirit using whatever technology exists to reach people who’d otherwise have no care at all, it’s Australia in 1928. That year, Reverend John Flynn founded the Aerial Medical Service, combining telegraph, radio, and airplanes to bring diagnosis and treatment to some of the most remote communities on Earth. Doctors would consult by radio, then fly a health professional out to the patient. It’s widely regarded as the first organized effort anywhere to solve geographic isolation from healthcare using telecommunications.
Norway was moving in parallel. Haukeland Hospital began using two-way radio in 1920 to connect physicians with sailors at sea, and other countries soon followed with similar radio-based systems of their own.
Norway Turns Innovation Into Policy
Technology is one thing; making it a permanent part of a healthcare *system* is another. This is where Norway pulled ahead of the rest of the world. Through the 1980s and 1990s, Norway systematically built out telemedicine infrastructure starting with videoconferencing for medical purposes in 1986, followed by a national electronic patient record system for general practitioners in 1992, and a dedicated national telemedicine competence center in 1993 that handled everything from ultrasound transmission to teleradiology.
Then, on August 1, 1996, Norway became the first country in the world to implement a **nationwide telemedicine reimbursement schedule**, a fixed, government-backed payment structure for specialist and radiology consultations delivered remotely. This is arguably the moment telemedicine stopped being an experiment and became infrastructure.
The Global Picture: What the World Health Organization Found
Because telemedicine adoption happens unevenly, country by country, specialty by specialty, the clearest snapshots come from the World Health Organization’s Global Observatory for eHealth, which has surveyed member states periodically since 2005.
In its **2009 survey**, 114 countries (59% of WHO member states) completed the telemedicine module.
In its 2015 survey, the most recent global survey of its kind, 125 member states responded, the highest participation to date. Teleradiology was the most widespread service, used in 77% of responding countries, while telepathology, remote patient monitoring, and teledermatology were each in use in nearly half. Yet despite that growth, only 22% of countries reported having an explicit *national* telemedicine policy meaning most countries using telemedicine were still doing so without a formal regulatory framework behind it .
No comparable global census exists specifically for 2019, the WHO’s next major telehealth-focused work shifted to regional surveys, such as a 2022 European digital health survey. So while adoption clearly continued climbing through the late 2010s, there isn’t a single authoritative “X countries were using telemedicine in 2019” figure to point to.
The United States: Early Innovator, Late Policymaker
Here’s the twist in the story: the U.S. was never behind on the *science*. American researchers were transmitting ECGs by cable in 1910 , and NASA later pioneered remote physiological monitoring of astronauts during the Space Race. Where the U.S. genuinely lagged by decades was in turning that technology into a “system” patients could actually access.
Milestone – Country -Year
*First nationwide telemedicine reimbursement policy – Norway – 1996
*First (limited) Medicare telehealth reimbursement – United States – 1997
*Modest expansion, still geographically restricted – United States – 2001
* Interstate licensure barriers finally waived – United States – 2020
* Geographic/site restrictions lifted, payment parity achieved – United States – 2020
The U.S. didn’t begin reimbursing telehealth through Medicare until the **Balanced Budget Act of 1997, ” one year after Norway’s nationwide policy, and even then, coverage was narrowly restricted to rural areas, specific clinical settings, and a limited menu of services. The Medicare, Medicaid and SCHIP Benefits Improvement and Protection Act of 2000, effective in 2001, expanded the list of covered services to include office visits, psychotherapy, and pharmacologic management, but coverage remained locked to rural health professional shortage areas and non-metropolitan counties.
That framework barely changed for the next two decades. The Affordable Care Act in 2010 encouraged pilot programs and value-based care experiments, but didn’t overhaul telehealth reimbursement itself . Meanwhile, the single biggest practical barrier, a requirement that providers hold a medical license in whatever state the patient physically sat in, meant that true interstate telemedicine was, for most purposes, not legally possible.
It took the declaration of the COVID-19 public health emergency in 2020 to finally break the logjam. Almost overnight, the federal government waived interstate licensure requirements, extended reimbursement to home-based visits, expanded which providers could bill for telehealth, and critically achieved payment parity between virtual and in-person visits.
**So how late was the U.S.?** Measured from Norway’s 1996 nationwide reimbursement policy to the point the U.S. removed its major structural barriers, the gap is roughly 24 years. And even now, the picture isn’t fully settled: many of the pandemic-era flexibilities were temporary, and Congress has had to repeatedly extend Medicare telehealth waivers piecemeal, including a widely discussed “telehealth policy cliff” debate around October 2025, rather than making the changes permanent. Compared to countries with an established, stable national telemedicine framework, the U.S. arguably still hasn’t reached the same institutional footing that Norway achieved in the mid-1990s.
The Takeaway
Telemedicine’s story isn’t really about invention; the tools existed for over a century. It’s about the slower, harder work of building policy, reimbursement, and legal frameworks around technology that already worked. Norway got there first. The rest of the world, including the country that helped invent much of the underlying medical technology, is still catching up.
References
[1] National Library of Medicine. (n.d.). *The history of telemedicine* [Digital collection]. U.S. National Library of Medicine. https://collections.nlm.nih.gov/catalog/nlm:nlmuid-101520679-vid
[2] Curogram. (2022, February 8). *History of telemedicine*. Curogram Blog. https://curogram.com/blog/history-of-telemedicine
[3] Sigmund Software. (2023, July 28). *The history of telehealth: Telemedicine through the years*. Sigmund Software Blog. https://www.sigmundsoftware.com/blog/history-of-telehealth/
[4] UniNet. (n.d.). *History of telemedicine*. Conganat International Virtual Congress. https://www.uninet.edu/conganat/ICVHAP/conferencias/017/history.htm
[5] World Health Organization Global Observatory for eHealth. (2010). *Telemedicine: Opportunities and developments in Member States — Report on the second global survey on eHealth* (Global Observatory for eHealth Series, Vol. 2). World Health Organization. https://pmc.ncbi.nlm.nih.gov/articles/PMC3402558/
[6] World Health Organization. (2016, December). *WHO third global eHealth survey: Atlas of country profiles*. WHO Regional Office for the Eastern Mediterranean. https://www.emro.who.int/ehealth/ehealth-news/who-third-global-ehealth-survey-atlas-of-country-profiles.html
[7] World Health Organization. (2016). *Global diffusion of eHealth: Making universal health coverage achievable — Report of the third global survey on eHealth*. World Health Organization. https://www.who.int/publications/i/item/9789241511780
[8] Avanesova, A. A., & Shamliyan, T. A. (2019). Worldwide implementation of telemedicine programs in association with research performance and health policy. *Health Policy and Technology, 8*(2), 179–191. https://www.sciencedirect.com/science/article/abs/pii/S2211883718302636%5B9%5D Gullslett, M. K., Ronchi, E., Lundberg, L., Larbi, D., Lind, K. F., Tayefi, M., Ngo, P. D., Sy, T. R., Adib, K., & Hamilton, C. (2024).
[9] Telehealth development in the WHO European region: Results from a quantitative survey and insights from Norway. *International Journal of Medical Informatics, 191*, 105558. https://www.sciencedirect.com/science/article/pii/S1386505624002211
[10] ChartRequest. (2024, November 26). *The origins of telehealth*. ChartRequest Blog. https://www.chartrequest.com/articles/telehealth-origins
[11] Accessible Telehealth. (2026, February 11). *The history of telehealth: A brief history of remote care in the United States*. Accessible Telehealth Blog. https://accessibletelehealth.com/2026/02/10/the-history-of-telehealth-a-brief-history-of-remote-care-in-the-united-states/
[12] Center for Connected Health Policy. (2024, April 8). *Federal telehealth laws*. CCHP. https://www.cchpca.org/federal/
[13] HGA. (2024, July 19). *The history of telehealth*. HGA. https://hga.com/the-history-of-telehealth/
[14] Ivanova, J., Cummins, M. R., Ong, T., Soni, H., Barrera, J., Wilczewski, H., Welch, B., & Bunnell, B. (2025). Regulation and compliance in telemedicine: Viewpoint. *Journal of Medical Internet Research, 27*, e53558. https://doi.org/10.2196/53558
[15] National Consortium of Telehealth Resource Centers. (2025, September 26). *The telehealth policy cliff: Preparing for October 1, 2025*. https://telehealthresourcecenter.org/resources/the-telehealth-policy-cliff-preparing-for-october-1-2025/
Anthropic. (2026). *Claude Sonnet 5* [Large language model]. https://claude.ai

HEALTHCARE PARTNERS

Abstract
Each year, nearly 15 million infants are born prematurely worldwide. These infants are exposed to pain, noise and separation during the first weeks of life. The high exposure to pediatric medical traumatic stress places infants and their caregivers at risk for mental health challenges that can persist into adulthood. To advance understanding, early stressors have been studied and linked to the development of later psychopathology. Recognizing these stressors creates a valuable opportunity for prevention through Trauma-Informed Developmental Care (TIDC) and Emotional Revival Therapy (ERT). These approaches equip Infant Mental Health Professionals with effective tools to support premature families and keeping hope up during the NICU journey. These early interventions at NICU help prevent manifest regulatory and attachment disorders in infants as well as perinatal psychiatric disorders in parents.
Abbreviations
ELS: Early-life stress
ERT: Emotional Revival Therapy
TIDC: Trauma-Informed Developmental Care
PMTS: Pediatric Medical Traumatic Stress
Introduction
Each year, close to 15 million infants are born prematurely worldwide, thrusting families into a world of uncertainty and intense medical intervention (World Health Organization, 2025). The physical and mental development of these vulnerable newborns has long been a central concern in neonatal care. Pioneering research in infant mental health shaped care strategies, emphasizing stress reduction and emotional regulation (Field, 1977; Als, 1982). The positive effects of these interventions have been extensively documented (Givrad et al., 2021). Despite these advances, preterm infants remain at heightened risk for psychiatric disorders from birth into adulthood (Johnson & Marlow, 2011). Johnson and Marlow (2011) describe the “preterm behavioral phenotype” which represents typical psychiatric manifestations of premature born adults characterized by inattention, anxiety, and social difficulties. Early-life stress (ELS), superimposed on immature neural pathways, deranges the developmental trajectory of prematurely born individuals contributing to the emergence of the preterm behavioral phenotype (Schmuecker et al., 2005).
Pediatric Medical Traumatic Stress (PMTS) is a term used to describe the responses of children and their families to trauma within a medical setting (Price, et al., 2016). The suffering during and after intensive care for both baby and parent underscores the importance of Trauma-Informed Developmental Care (TIDC) and Emotional Revival Therapy (ERT) throughout the hospital experience and beyond discharge to reduce the impact of PMTS. These interventions can mitigate the risks of mental health complications, to both baby and family that arise during the NICU stay and span the continuum from early childhood into adulthood. Ideally, these early interventions at NICU and beyond help prevent manifest regulatory disorders in infants, perinatal psychiatric disorders in parents, and disorders within the parent-infant relationship.
The NICU as a Dual Landscape of Healing and Trauma
The NICU is both a sanctuary of survival and a crucible of stress. For the infant, the soundscape of alarms and ventilators, the glare of fluorescent lights, and the invasive touch of medical procedures replace the gentle rhythms of the womb (Wolke, 1991). These sensory intrusions disrupt critical neural and emotion regulatory networks. In the womb, the baby’s sense of self is entirely relational, tied to the mother through a seamless co-regulatory bond that provides both physical and emotional sustenance. Suddenly, that bond is severed, leaving the baby exposed to bright lights and a cacophony of unfamiliar sounds, with so many hands touching, poking, and sticking needles into them. Tubes are inserted down their throat, often without any comforting reassurances or soothing touch. The babies, with no point of reference to understand the life-threatening situation, is left in a state of utter bewilderment and terror.
A state of shock is a natural response to birth that requires life-sustaining medical interventions for baby and mother, which begins when the two are torn apart. This separation is the first in a cascade of events that disrupts the intuitive bond between mother and child and often positions the caregiver(s) as visitors of their baby within the NICU. Imagine yourself as the parent; you are standing outside your baby’s room, separated by a door you cannot open. You must ring the bell and wait for permission to enter before you are then required to disinfect your hands and walk a long corridor before reaching your child. Even then, the natural response to gather your child into your arms and hold them in your loving embrace often depends upon the availability, and the permission of someone else to assist you. The power dynamic in these situations casts a long shadow over the caregiver’s experience. Parents often describe feeling like intruders in their child’s care, rather than being essential to their baby’s survival. Parents who are unable to participate in their child’s care often struggle with feelings of inadequacy and guilt, which can linger long after the NICU experience has ended.
TIDC seeks to mitigate these stressors, reframing the NICU as a place of healing (Coughlin, 2021). Within the context of earlier viability thresholds, TIDC faces new demands to address the heightened vulnerabilities of extremely preterm infants and their families. For parents, family-integrated care models, informed by trauma-informed paradigms, help to rebuild confidence and foster connection that is quintessential to healing. These person-centered paradigms transform the NICU from an alienating environment to one of shared caregiving. By integrating targeted developmental and relational strategies, TIDC aims to mitigate the compounded effects of early adversity.
Pediatric Medical Traumatic Stress: Defining the Experience
The experience of the infant in NICU typifies PMTS, with life threatening conditions, the suffocation associated with pulmonary immaturity, repeated painful procedures and prolonged caregiver separation. Unlike older children, newborns in the NICU lack established routines and memories, making it difficult to distinguish the infant’s baseline behavior profile from their lived experience of trauma. However, common key stressors associated with NICU hospitalization, that include respiratory distress, procedural pain, and separation from caregivers, are known risk factors for psychopathology (Pierrehumbert et al., 2013). Sleep fragmentation and noxious touch experiences, in conjunction with invasive procedures, further exacerbate the infant’s distress. Understanding how these stressors contribute to short and long-term developmental outcomes is essential for creating effective interventions.
Stressors in the NICU Environment
Pulmonary Immaturity: Respiratory distress syndrome is often a preterm infant’s first experience outside the womb, characterized by shallow breathing and grunting. It is a breathing pattern not exclusive to pulmonary immaturity but typical for a state of panic and a pretext to a traumatic development. To ensure the survival of the premature infant mechanical ventilation may follow the respiratory distress which alters physical recovery but also the neural pathways that regulate stress and basal affects. Often the infant experiences mechanical ventilation in a state of drug induced dissociation. Once the infant no longer needs external respiratory support, the pattern of dissociation may have become part of the infant’s neural networks and self-identity (Schore, 2012). Chronic lung conditions as well as early dissociation limits the individual’s quality of life, restricting their physical activities and potentially affecting their capacity for social participation (Lærum et al., 2019). The emotional cost of witnessing an infant’s struggle with respiratory distress weighs heavily on parents and caregivers, adding to their sense of helplessness and potentially influencing their capacity to provide attuned caregiving.
Pain and Procedural Trauma
NICU infants endure numerous painful procedures daily, often without sufficient analgesia (Carbajal et al., 2008). Premature infants respond visibly to this pain with crying, hypertonus and increase of the heart rate (Pokela & Koivisto, 1994). Despite the aversive reaction of the infant, the painful procedures will go on for days to months, often under-managed. The infant’s attempts to withdrawal from the pain results in an enduring state of dissociation. This traumatic state impairs the physiological stability and emotional development of the infant, increasing the risk for developmental disorders (Lammertink et al,. 2022). The long term consequences of early-life exposure to unmanaged pain is associated with altered gene expression linked to greater socio-emotional stress sensitivity and behavioral challenges at school-age (Chau et al., 2014). Pain is a major risk factor for dissociation and a traumatic developmental trajectory, and may pose a risk for disorganized attachment patterns (Wolke et al., 2014).
Separation from Caregivers
Separation exacerbates the infant’s stress, depriving them of co-regulation by and safety with their primary caregivers. For infants, the absence of consistent caregiver presence disrupts the natural rhythms of attachment formation, leaving them in a state of affect dysregulation (Schore, 2012). When this absence occurs under the conditions of life-threatening circumstances and constant medical stress, the opportunity for co-regulation is significantly restricted for the baby and their parent. Private rooms within the NICU setting remain rare and are not a guarantee for 24-hour parental presence and so, newborns and their parents may not be able to physically be together for days at a time. The singularly most traumatic experience for a newborn across all mammalian species is maternal separation.
Research confirms the benefits of immediate skin-to-skin contact between baby and the birthing parent, while separation increase the experience of toxic stress and risk of disorganized attachment (Mehler et al., 2023). Skin-to-skin contact during the NICU stay has proven to promote autonomic and neurobehavioral brain maturation in preterm infants positively impact neurodevelopmental profiles and infant mental health outcomes (Feldman & Eidelman, 2003). Ensuring parental presence and empowering parental involvement, especially during stressful medical procedures, buffers the adverse effects of the NICU experience. Parental presence and participation in medical, parenting and caregiving activities in the NICU are protective factors against PMTS and compromised neurodevelopmental outcomes (Pineda et al., 2017).
Developmental Consequences of PMTS
Although the prevalence of PMTS in premature infants has not been systematically studied, developmental disorders, physical, neurological and mental health outcomes in this population have been researched for about 50 years (Johnson & Marlow, 2011). Specifically, infants born premature are at risk for disorganized attachment, even when their parents are sensitive caregivers (Wolke et., 2014). For many infants who experience the NICU, the overwhelming stress and absence of a consistent caregiver teaches them that the world cannot be trusted. This lack of trust is often expressed as reduced facial responsiveness to their caregiver’s positive emotions over the first year of life (Schmuecker et al., 2015). This interferes with activities of daily living such as feeding experiences. Infants who have experienced ‘feeding protocols’ in the NICU may learn to not trust the ‘feeding experience’ because of their lived experience of fear and pain in the setting of non-responsive/non-attuned ‘feeding’ interactions. Consequently, these children are at an increased risk for post-traumatic feeding disorder and feeding tube dependency (Wilken & Bartmann, 2014). Prolonged exposure to toxic stress impairs affect regulation, executive functioning, memory, and learning, creating challenges that extend well beyond infancy (Grunau et al., 2009). Preterm born adults who exhibit characteristics consistent with the ‘preterm behavioral phenotype’ have an increased risk for psychiatric disorders like anxiety disorders and depression (Lærum, et al., 2019). Research has shown that NICU-related stress corresponds with neural patterns akin to those observed in early-life trauma victims, highlighting the long-term impact of unaddressed stressors (Lammertink et al., 2022).
Early Intervention: Emotional Revival and Healing
Addressing PMTS requires early interventions that prioritize relational repair. In the NICU, TIDC serves as a prevention model, leveraging our understanding of the long-term effects of chronic toxic stress. By equipping caregivers with the knowledge and skills to mitigate these experiences, TIDC transforms the NICU into a space of healing and recovery for infants and families alike. Within a TIDC approach, interventions are designed to minimize stress, support neurodevelopment, and nurture resilience. This approach also deepens clinicians’ awareness of the infant’s lived experience, fostering greater attunement and responsiveness. However, even with the most effective TIDC practices, pain and separation cannot be entirely eliminated, as the infant remains in a critical medical situation. Despite the prevention intervention some premature infants will suffer from PMTS after discharge. ERT is a new need-based trauma treatement for infants with PMTS. Available since 2021 in Germany infants and parents will be seen bi-weekly in a home-based environment. During ERT the therapist creates synchronized rhythm with the child to re-establish a sense of safety in four phases (Wilken et al., 2023).
1: Create Contact
To establish a therapeutic alliance with infants in a state of traumatic withdrawal the therapist needs to gain the infants’ trust. To build trust the empathic therapist will track affective states of the infant and regulate traumatic dysregulation. Non-verbal contact through body language, mimicry, gesticulations and intonation activate the sense of self enabling the baby to experience a sense of self-coherence.
2: Create Emotional Response
In the initial phase of the ERT treatment, inner withdrawal will not allow the infant to communicate using their emotions. The window of affect tolerance is closed. The infant will primarily express dysregulated traumatized affects. With adaptive affect mirroring the therapist will slowly help the infant to transfer dysregulated affects into emotions. The window of affect tolerance will gradually open. Over the course of the ERT process emotions become more and more part of the infant’s communication repertoire.
3: Create Intersubjectivity
The revival of emotions marks the beginning of an emerging subjectivity. This subjectivity opens a window of opportunity for the infant and caregivers to foster their developing attachment. Attachment is under development until 24 months. The ERT therapist supports parents in recognizing and responding to their infant’s emotional cues, deepening the parent-infant bond. Infants and caregivers will then be able to re-introduce emotions into their communication toolkit.
4: Create Meaningful Relationships
Rebuilding trust through nurturing, predictable, well attuned and emotionally supportive interactions is essential to help the infant transition from a state of survival to a state of growth and development. With a deepened process of bonding, the basis for a meaningful and trusting relationship is revealed with a securre attachment organization. As the infant develops new capacities, needs and desires, conflicts may come up. In this phase of evolution, the ERT therapist will guide the caregiver to recognize and respond to their infant’s emotional cues, strengethening the parent-infant bond. In this process the parents will be given room to reflect on their own trauma and hurt experienced during the NICU stay. When infants and caregivers can communicate in a balanced partnership, the treatment process can be terminated.
Conclusions
Research over the last fifty years has shown that the lived experience of NICU hospitalization is a stressful and traumatic life event and may represent a major mental health risk factor for infants. Research has shown that early-life stress and trauma in infancy build pathways of dysfunctional physiological, neurological and mental growth (Schore, 2012). This paper gives an overview of how Pediatric Medical Traumatic Stress may contribute to significant short-term and long-term psychopathology in premature infants and their families. Therefore, prevention and treatment of PMTS in the NICU is paramount.
TIDC represents a paradigm shift, reframing the NICU from a space solely focused on survival to one that fosters resilience and growth for infants and families alike. As a prevention model, TIDC seeks to mitigate the cumulative effects of chronic toxic stress by addressing its root causes and implementing evidence-based interventions that promote healthy development. One of the most transformative aspects of TIDC is its focus on empowering parents as essential members of the care team. This empowerment is critical for fostering a sense of hope and connection, which counteracts the pervasive helplessness often felt by parents navigating the NICU experience.
Transforming the NICU from a place exclusively focused on disease management and medical technology to an environment that acknowledges and responds to the multifaceted human and developmental needs of critically ill babies and their families is a long-term project. Sadly, pain, suffocation and separation will continue to impact babies and families experiencing NICU care around the globe. And Post-traumatic Stress Symptoms will likely be endured for generations to come. Therefore infants and caregivers should have access to early intervention like ERT or Psychoanalytic Parent-Infant Psychotherapy as preventive psychotherapy during NICU stay and in the following 1001 days. Research will show, if these interventions decrease the risk for feeding, sleeping or attachment disorders. With every incremental step toward more holistic care, we move closer to a future where the tiniest humans and their families are met with care that honors their humanity and potential. Together, we can create a world where no family feels alone, no infant’s needs to go unheard, and hope becomes the heart of every NICU journey.

PREEMIE FAMILY PARTNERS
When I share my story with new NICU parents, they are often astonished that all three of my children were in the NICU and that I made it through those challenging times. They may think I’m stronger than I am. Honestly, each time I got pregnant, I didn’t believe my baby would end up in the NICU. Each time, I was surprised. I’ve always believed there is a silver lining, but when it came to the health of my babies, it was hard to see one.
My oldest daughter is now a teenager, but I still remember the day she was born like it was yesterday. My pregnancy was full-term and relatively normal. However, during labor, the umbilical cord was wrapped around her neck, affecting her breathing. She didn’t make a sound when she was born, and I couldn’t hold her. I was overwhelmed with fear and worry, unprepared for the NICU experience. She spent almost three weeks in the NICU. Leaving the hospital without her was devastating, but after several consultations, we were assured she wouldn’t have any long-term effects. The NICU stay changed our lives, but I never thought we would go through it again.
For a while, my husband and I didn’t plan on having more children due to a massive fibroid that required surgery. In 2019, I had a myomectomy, and the doctors assured me I could still have children, though it would require a c-section. During the pandemic, I became pregnant again at 40, which made me high-risk. The isolation of the pandemic made the experience even harder. Despite a smooth pregnancy, my second daughter had low glucose levels at birth and needed to stay in the NICU. We were distraught and unprepared, facing the NICU once again for a different reason.
Six months later, I became pregnant with our third daughter. At four months, an ultrasound revealed a cyst in her abdominal area, indicating she would need to stay in the NICU. After she was born, she had to be transported to another hospital for surgery.
Juggling a newborn in the hospital, a toddler at home, and a teenager was incredibly stressful, but now I am able to look back and know that I made it through all of that. My NICU journeys were tough, but my support system helped me through it.
Throughout these three NICU experiences, I’ve learned some valuable lessons:
- Build a Support System Lean on family and friends when you can. Having people to talk to and share your worries with can make a significant difference. Hand to Hold’s support resources are built around the notion of talking to someone who’s been there. Find support groups, peer mentors, and more.
- Focus on Progress No matter how small the progress, focus on it. Keeping a gratitude journal helped me maintain a hopeful outlook.
- Advocate for Your Baby Don’t be afraid to ask questions and seek second opinions. Trust your instincts and ensure you understand your baby’s medical care.
- Take Care of Yourself Your baby needs you to be strong. Prioritize self-care, rest when you can, and seek support for your mental health if needed.
- Stay Informed: Educate yourself about the NICU process and your baby’s condition. Knowledge can empower you and reduce fear.
Being a NICU parent is a journey filled with unexpected challenges, but with support, hope, and advocacy, you can navigate through it. You are stronger than you think.
Source: https://handtohold.org/my-journey-as-a-three-time-nicu-mom/
For decades, the conversation surrounding perinatal mental health has centered—appropriately—on mothers. The recognition of postpartum depression, anxiety disorders, and birth-related trauma has transformed obstetric and pediatric practice. Universal screening recommendations, increased public awareness, expanded access to mental health services, and growing legislative support have all reflected an important truth: the emotional well-being of mothers profoundly influences the health and development of their children. However, amid this progress, one parent has remained largely absent from both clinical practice and public policy
Last June 2025, Neonatology Today published an NCfIH Column examining paternal mental health and the often overlooked psychological challenges experienced by fathers during the transition to parenthood. (1) That article highlighted an uncomfortable reality: while medicine increasingly recognizes the importance of supporting mothers, fathers frequently receive little acknowledgment of their own emotional vulnerabilities. Despite a growing body of evidence demonstrating that paternal mental health significantly affects infant development, maternal wellbeing, family functioning, and long-term childhood outcomes, routine assessment and treatment of fathers remain uncommon throughout obstetric, neonatal, and pediatric care. (1-7)
This omission represents more than a gap in clinical practice. It reflects a fundamental inconsistency in our commitment to family centered care. If family-centered care truly seeks to optimize outcomes for infants by supporting the entire family system, then paternal mental health can no longer remain an afterthought.
The Expanding Science of Paternal Mental Health
The traditional image of fatherhood has emphasized strength, emotional stability, and unwavering support for one’s family. While these qualities remain admirable, they have also contributed to a culture in which fathers often suppress emotional distress rather than acknowledge it. Modern neuroscience, psychology, and developmental medicine tell a far more complex story.
The transition to fatherhood represents one of the most profound psychosocial adjustments in adult life. New fathers experience dramatic changes in identity, family dynamics, financial responsibilities, sleep patterns, interpersonal relationships, and daily routines. Increasingly, research demonstrates that measurable biological alterations accompany these psychosocial changes. Investigators have documented reductions in circulating testosterone, changes in cortisol regulation, fluctuations in prolactin, oxytocin, and vasopressin levels, and alterations in neural pathways associated with attachment and caregiving. These neuroendocrine adaptations appear to facilitate paternal bonding and promote nurturing behaviors. However, they may also increase susceptibility to mood disorders in vulnerable individuals. (2-4)
These biological findings reinforce an important concept: paternal depression is neither a personal weakness nor simply a stress reaction. Rather, it represents a multifactorial medical condition arising from the interaction of biological, psychological, and social factors.
Current estimates suggest that approximately 8–10% of fathers experience postpartum depression during the first year following childbirth. The prevalence rises substantially when mothers are also experiencing postpartum depression and may exceed 20–25% among fathers whose infants require prolonged hospitalization in a neonatal intensive care unit (NICU). Fathers also demonstrate increased rates of generalized anxiety disorder, adjustment disorders, acute stress reactions, and post-traumatic stress disorder (PTSD), particularly following traumatic deliveries, neonatal surgery, congenital anomalies, or extreme prematurity. (2,3, 5-7) These numbers likely underestimate the true burden of disease because paternal mental health remains significantly underdiagnosed.
Why Fathers Go Unrecognized
One of the greatest barriers to addressing paternal mental health is that men often experience depression differently from women. Rather than expressing persistent sadness or tearfulness, fathers may present with irritability, emotional numbing, anger, increased conflict within relationships, substance misuse, compulsive work behaviors, social withdrawal, sleep disturbances, diminished concentration, or risk-taking behaviors. These manifestations are frequently interpreted as personality changes, occupational stress, or relationship difficulties rather than symptoms of an underlying depressive disorder.
Cultural expectations further compound the problem. Traditional masculine norms encourage emotional self-reliance and discourage help-seeking behavior. Many fathers perceive acknowledgment of emotional distress as evidence of personal failure or inadequate parenting. Others believe that their own emotional needs are secondary to those of their partner and infant.
Healthcare systems unintentionally reinforce these beliefs. Throughout pregnancy, childbirth, and postpartum care, fathers often occupy the role of supporter rather than recipient of care. Obstetric providers appropriately focus on maternal health, while pediatric providers concentrate on infant well-being. Consequently, fathers may accompany dozens of medical encounters without anyone directly asking about their own mental health. Ironically, they may be among the individuals most in need of support.
The NICU: A Perfect Storm for Psychological Distress
Although every transition to parenthood presents challenges, few experiences equal the psychological burden associated with neonatal intensive care hospitalization. Parents of critically ill newborns experience repeated exposure to uncertainty, invasive procedures, life-threatening complications, alarms, unfamiliar technology, and prolonged separation from the infant they anticipated bringing home shortly after birth.
While considerable research has documented maternal psychological distress during NICU hospitalization, fathers often shoulder multiple simultaneous responsibilities. They may balance full-time employment with daily hospital visits, care for siblings at home, provide emotional support to their partner, communicate with extended family, navigate insurance and financial concerns, and participate in complex medical decision-making.
Many fathers describe feeling obligated to remain emotionally composed for everyone else, leaving little opportunity to process their own fears or grief. Not surprisingly, studies demonstrate significantly elevated rates of anxiety, depression, and PTSD among NICU fathers. These symptoms frequently persist long after hospital discharge, influencing parenting behaviors, family relationships, and future reproductive decisions.
Ignoring paternal mental health, therefore, represents a missed opportunity to improve both immediate and long-term family outcomes.
The Impact on Infant Development
The importance of paternal mental health extends well beyond the father himself. Contemporary developmental science increasingly recognizes fathers as critical contributors to early childhood development. Positive paternal engagement promotes language acquisition, executive functioning, emotional regulation, social competence, and cognitive development.
Conversely, untreated paternal depression has been associated with reduced parent-infant bonding, diminished responsiveness to infant cues, decreased participation in reading and play, increased behavioral difficulties during childhood, and higher rates of anxiety and depression among offspring. The effects are often indirect but profound.
A father experiencing depression may struggle to provide emotional support to his partner, increasing maternal stress and impairing co-parenting relationships. Household conflict may rise. Communication deteriorates. Family resilience diminishes precisely when it is needed most. From a systems perspective, paternal mental health should therefore be understood not as an isolated psychiatric concern but as an essential determinant of family health.
Family-Centered Care Must Include Fathers
Family-centered care has become a foundational principle within neonatal medicine. Its core philosophy recognizes parents as essential partners in their infant’s care and emphasizes collaboration, respect, education, and shared decision-making.
However, meaningful family-centered care requires more than inviting parents to participate in bedside rounds.
If healthcare systems genuinely recognize families as integral members of the care team, they must also recognize that the psychological well-being of every caregiver directly influences infant outcomes. Supporting fathers should become an expected component of comprehensive neonatal and pediatric practice rather than an optional service available only at selected centers. This begins with acknowledgment.
Simple screening instruments for paternal depression and anxiety already exist and can be incorporated into NICU follow-up clinics, pediatric well-child visits, and postpartum care with relatively little additional burden. Education on paternal mental health should be incorporated into prenatal counseling, childbirth education, NICU orientation, and discharge planning.
Equally important is ensuring that screening leads to meaningful intervention through referral pathways that include behavioral health professionals, peer support groups, cognitive behavioral therapy, psychiatric evaluation when appropriate, and community resources designed specifically for fathers.
A Policy Imperative Clinical care alone cannot address paternal mental health. Public policy must evolve alongside scientific evidence. Paid parental leave remains inconsistent across the United States despite substantial evidence demonstrating benefits for parent-infant bonding, maternal recovery, breastfeeding success, and paternal involvement. Expanding paid paternity leave may also reduce psychological distress by allowing fathers a greater opportunity to adjust to new parenting responsibilities while participating actively in infant care.
Similarly, insurance coverage should facilitate access to behavioral health services for fathers during the perinatal period. Funding agencies should prioritize research examining paternal depression, anxiety, PTSD, and effective interventions, particularly among families experiencing NICU hospitalization or medically complex births.
Professional organizations—including the American Academy of Pediatrics, the American College of Obstetricians and Gynecologists, the National Perinatal Association, the National Coalition for Infant Health, and neonatal nursing organizations— have an opportunity to develop evidence-based guidance to support routine paternal mental health assessment and referral. Such recommendations would acknowledge what decades of developmental science have already demonstrated: supporting fathers ultimately supports children.
Changing the Narrative
Perhaps the greatest challenge lies not within medicine but within society. We must replace the outdated expectation that fathers endure emotional suffering silently with a more accurate understanding of paternal resilience. Seeking help is not evidence of weakness. It is evidence of insight, responsibility, and commitment to one’s family.
The feature NCfIH published in Neonatology Today last June represented an important step toward bringing paternal mental health into mainstream neonatal discourse. (1) That conversation should not end with a single publication. Rather, it should catalyze sustained clinical innovation, multidisciplinary research, professional education, and policy reform. Medicine has successfully transformed maternal mental health from a neglected topic into a recognized public health priority. There is every reason to believe we can achieve the same progress for fathers.
Doing so requires us to broaden our definition of perinatal care. Caring for infants means caring for parents. Caring for parents means caring for both mothers and fathers. Until paternal mental health receives the same attention, resources, and scientific rigor as maternal mental health, our vision of family-centered care will remain incomplete. (1) The health of fathers matters—not only because they deserve compassionate, evidence-based care, but because the well-being of fathers profoundly shapes the health, resilience, and future of the families they love.
Source: https://neonatologytoday.net/newsletters/nt-jul26.pdf

INNOVATIONS
Bringing a child into the world can feel overwhelming for most new parents, but these feelings are heightened when the new baby must be admitted to the Neonatal Intensive Care Unit, or NICU, due to prematurity, a genetic condition or critical illness that requires around-the-clock care. About 10% of all newborns need this specialty treatment.
For Esther Kangethe, those feelings began in June 2024, when she was rushed to Oregon Health & Science University due to significant cramping and bleeding while 20 weeks pregnant with twins.
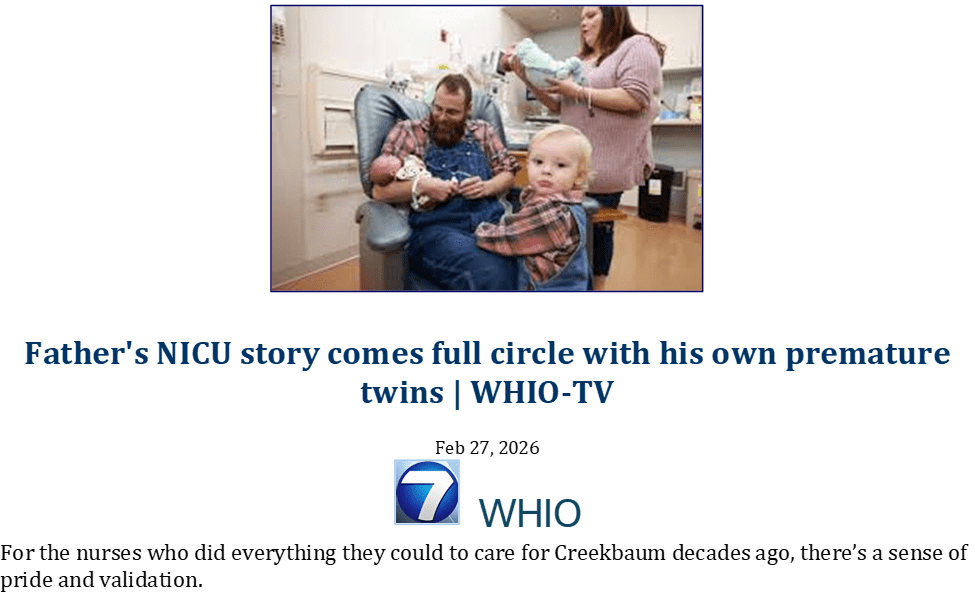
Tragically, Kangethe lost one of her twins that day. But she held onto hope as “Twin B” remained stable for the next few weeks. She gave birth to her son at 23 weeks; he weighed just over a pound. He was named Myles — a profound tribute to his health journey, representing the miles traveled between the different hospital units during their stay.
Although overjoyed that Myles was born safely, Kangethe understood there was a long road ahead to ensure he grew strong and healthy.
“Now the reality hit me that I had a baby in the NICU, and I was so scared,” she said. “It was something new I’d never experienced before.”
But Kangethe wasn’t alone for what would be five months in the NICU. Recognizing the need for both mental health and resource support through the traumatic experience of a NICU stay — particularly for families from racial and ethnic minority groups — OHSU Doernbecher health care teams have established culturally specific support groups designed specifically for Black and Latino families. The groups are open not only to OHSU patient families like Kangethe but all families who have had a child in a Portland NICU.
“It’s hard to explain what’s going on with your baby to someone who hasn’t had that experience. A lot of families are spending days and nights in the hospital, which can lead to a feeling of extreme isolation,” said Devlynne Sasha Ondusko, M.D., assistant professor of pediatrics in the OHSU School of Medicine who helped establish the support groups.
“Peer support groups provide the opportunity for families with similar lived experiences to come together, learn from and mentor one another, and find hope from those families who have come out the other side.”
Personalized support
Navigating a NICU stay is a challenging experience for any family, but can be especially so for racial and ethnic minority groups. An OHSU-led study published recently in the journal Pediatrics found that Black families continue to experience differential treatment in the NICU, including discrimination and poor communication, which reinforces the untrustworthiness of the health care system.
Improving care and the patient family experience requires more transparent communication, advocacy and mental health support, increasing engagement in patient families’ parental roles, and decreasing biased treatment and provision of resources, said Ondusko, corresponding author of the study.
“One thing that is apparent is that there is not nearly enough mental health support for parents who are going through the traumatic experience of a NICU stay,” she said. “Finding resources and staying connected to resources is very hard, especially during and after the transition of taking your baby home. We started to think about how we could better support families of color, who have told us they experience additional isolation in this setting.”
The OHSU support groups seek to address that issue. They are a safe, supportive space where families can come together, share a meal, learn about resources and, most importantly, find connection with others sharing a similar experience. The discussions are participant-led but guided by facilitators, who are qualified mental health professionals, and community organization leaders, including Healthy Birth Initiatives and Healthy Families.
Ondusko introduced Kangethe to the support group for Black families. Kangethe said the group is not only a safe place to speak about her emotional experiences, but also provides the opportunity to ask questions and better understand her baby’s care.
“I’ve been going to the meetings every month and have connected with the parents there who had similar situations to mine, and that has really given me hope,” she said. “These groups make you stronger and remind you that you’re not alone in this.”
Feeling supported by the care team was a crucial part of her overall experience, Kangethe said.
“The doctors in the OHSU NICU were really the best,” she said. “They understood the parents, were very good at explaining things, had empathy and were able to listen. They even offered regular one-on-one time with my doctor where I could ask any questions and write things down.”
Expanding access to support
Ondusko and colleagues are now conducting ongoing research, including in-depth interviews with patient families, to understand what is beneficial about the support groups and what could be improved, as well as how to expand access throughout the community and adapt the format to other groups.
“I’d love to see us make this more inclusive between all of the NICUs, and even alternate between sites to ensure all families can access this resource,” Ondusko said.
Ondusko also hopes to leverage lessons from these groups for the development of a program that could be shared and applied in other NICUs around the country.
For Kangethe, after five long months in the NICU and meeting with her support group, she received the ultimate holiday gift: Baby Myles was discharged just before Thanksgiving. At 8 months old, he’s now happy, healthy and thriving at home with his family.
Background
Telemedicine uses videoconferencing technology to enable real-time audio and visual communication, linking on-site healthcare providers with specialists at remote locations. Over the past decade, telemedicine has grown significantly within the field of neonatology. This study seeks to deepen the understanding of telemedicine applications for newborns and neonatal intensive care units (NICUs) through a detailed bibliometric analysis.
Methods
Publications on telemedicine in newborns and NICUs from January 1, 2004, to October 22, 2024, were retrieved from the Web of Science Core Collection. Using Microsoft Excel, CiteSpace, the R package “bibliometrix,” and VOSviewer, we analyzed the data to examine the number of publications, contributing countries/regions, institutions, authors, journals, references, and keywords.
Results
Since 2004, 1177 publications have been included, reflecting a rapid increase in research on telemedicine in newborns and NICUs over the past decade. These studies originated from 55 countries/regions and 139 institutions. The United States, the United Kingdom, and India were the primary contributors in terms of publication volume. Among the 405 authors analyzed, Jennifer L. Fang had the highest number of publications, while James P. Marcin received the most co-citations. BMC Pregnancy and Childbirth published the most articles, and Pediatrics had the highest citation count. The most frequently used keywords included “accuracy,” “depression,” “digital health,” “mobile health,” and “parents,” highlighting key research areas. Emerging research frontiers such as “palliative care,” “low-income populations,” “artificial intelligence,” and “parents with high-risk infants” indicate rapidly advancing topics in this field.
Conclusions
This study is the first to perform a comprehensive bibliometric analysis of publications on telemedicine in newborns and NICUs. In the previous 20 years, global interest in teleneonatology research has significantly increased. Our bibliometric findings offer valuable insights for researchers, helping them understand essential information, recognize current research hotspots, identify potential collaborators, and explore future research frontiers in this field.
Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC12035156/

Background: Caregiver-child interactions, and specifically child-directed speech, play a central role in early language acquisition by scaffolding children’s attentional and lexical development. The features and developmental effects of child-directed speech may vary depending on the child’s developmental status and communicative needs, especially in clinical risk conditions such as preterm birth.
Aims: This study examined maternal child-directed speech in a semi-structured context, focusing on prosodic cues (mean pitch, pitch range, and speech rate) and structural features (lexical diversity, verbosity, and syntactic complexity) in preterm (PT) and full-term (FT) 18-month-old toddlers interacting with their mothers. We explored (a) differences in child-directed speech between PT and FT groups, (b) the modulation of prosody based on word familiarity, and (c) associations between child-directed speech characteristics, children’s attentional engagement (visual exploration of familiar/unfamiliar objects), and vocabulary skills.
Methods and procedures: Forty-three mother-child dyads (20 PT, 23 FT) participated in the study. Maternal speech was transcribed and analysed for linguistic features, while target word tokens were acoustically analysed with PRAAT for prosodic measures. Child visual exploration of objects was coded from video recordings, and vocabulary skills were assessed using validated measures.
Outcomes and results: All mothers modulated prosody to highlight novel words, using higher pitch, wider pitch range, and slower speech rate for unfamiliar versus familiar referents. Mothers of FT children produced more frequent and lexically diverse speech compared to PT counterparts, though verbosity did not differ between groups. In the FT group, slower maternal speech rate was associated with reduced visual exploration of objects, suggesting dynamic adaptations to children’s attention. No such association was found in PT dyads. In the PT group, receptive vocabulary index was positively correlated with maternal verbosity, lexical diversity and syntactic complexity.
Conclusions and implications: Findings highlight both shared and group-specific patterns in maternal child-directed speech effects. While prosodic adjustments to word familiarity are preserved in PT dyads, structural aspects of maternal input appear more closely linked to receptive vocabulary in PT children, possibly reflecting adaptive scaffolding strategies. These results underscore the importance of considering both prosodic and structural features of child-directed speech and child conditions in informing targeted early interventions.
What this paper adds: What is already known on this subject CDS is essential for early language acquisition by enhancing attention and vocabulary. However, CDS characteristics may vary with child developmental status, and little is known about differences in maternal speech between preterm and full-term toddlers in relation to word learning. What this paper adds to existing knowledge Both preterm and full-term mothers modulate prosody to mark unfamiliar words, yet full-term mothers use more frequent and lexically diverse speech. Structural aspects of maternal input correlate more strongly with receptive vocabulary in preterm children, indicating possible adaptive strategies. What are the potential or actual clinical implications of this work? These results support the need for early interventions tailored to preterm children that target both prosodic and structural features of maternal speech to optimise language development.
2025 Royal College of Speech and Language Therapists.: https://pubmed.ncbi.nlm.nih.gov/41456959/


The Music That Carries Our Preemie Community
For many of us, music has been part of our journey since the NICU. Our earliest soundscape may have included monitors, ventilators, alarms, and the quiet voices of parents and caregivers beside an incubator. Within that unfamiliar environment, a softly sung lullaby, gentle humming, or the familiar rhythm of a parent’s voice could create a moment of comfort and connection. Music therapy in the NICU can also offer families a meaningful way to participate in their baby’s care, nurture bonding, and bring warmth into a highly medicalized space.
As preemie survivors, NICU parents, siblings, caregivers, and advocates, we know that healing and development do not end when a baby leaves the hospital. Music can continue to support us throughout childhood and adulthood—as a source of expression, emotional release, confidence, memory, and joy. A familiar song may remind us of how far we have come, help us through difficult moments, or give us a way to celebrate the strength that has always existed within our community.
Music also connects our preemie community across cities, countries, cultures, languages, and generations. We may have different birth stories, medical experiences, traditions, and favorite styles of music, but we recognize many of the same emotions: uncertainty, hope, fear, gratitude, resilience, and love. Through lullabies, cultural songs, community performances, shared playlists, and family traditions, music reminds us that none of us is walking this journey alone.
Summer offers a beautiful opportunity for our community to enjoy that connection together. Music surrounds us at cookouts, picnics, neighborhood festivals, outdoor concerts, family reunions, city/town events, and relaxed evenings with the people we love. This season, we can create playlists that celebrate our journeys, share songs that helped our families through the NICU, dance with our children, attend accessible community concerts, or simply enjoy music together at home. Every beat can become a celebration of our survival, our families, our cultures, and the powerful community we continue to build.

Cabo Verde Song for Kids 🇨🇻 | Learn About Cabo Verde (Cape Verde) | Africa Island Geography Song
Learn about Cabo Verde (Cape Verde) with this fun and educational song for kids!Kids explore this African island nation, its geography, and culture through real-life footage and catchy music designed for young learners.


Zayn Malik Reads ‘Music Is In Everything’ | CBeebies Bedtime Stories
Zayn Malik joins us for a Bedtime Story. Listen as he reads ‘Music Is In Everything”, written by Ziggy Marley and illustrated by Ag Jatkowska. This story is a picture book celebrating the joy of music all around us. From the sound of sea waves to laughter and dancing in the family kitchen, music really is in everything!


Our Little Miracle – A Heartfelt Song from Parents to Their Newborn Baby
Our Little Miracle is a heartwarming song from parents to their newborn child — a tender celebration of life, love, and the first moments of parenthood. 💕
This song captures the magic of holding your baby for the first time — the warmth, the tears, and the unspoken promise of unconditional love. Whether you’re a new parent, expecting, or reminiscing about your baby’s first days, this lullaby will melt your heart.

In Santa Maria, a group of people from different corners of the world share what brings them together: a love for the ocean and a passion for learning.
This video, filmed in collaboration with Kite Verde, captures the essence of that energy: laughter, wind, learning, and the feeling of being exactly where you’re meant to be.




















































































































































































































{kind=link}