


Turkey, officially the Republic of Turkey, is a country straddling Western Asia and Southeast Europe. It shares borders with Greece and Bulgaria to the northwest; the Black Sea to the north; Georgia to the northeast; Armenia, Azerbaijan, and Iran to the east; Iraq to the southeast; Syria and the Mediterranean Sea to the south; and the Aegean Sea to the west. Istanbul, the largest city, is the financial centre, and Ankara is the capital. Turks form the vast majority of the nation’s population, and Kurds are the largest minority.
Turkey is a regional power and a newly industrialized country, with a geopolitically strategic location. Its economy, which is classified among the emerging and growth-leading economies, is the twentieth-largest in the world by nominal GDP, and the eleventh-largest by PPP. It is a charter member of the United Nations, an early member of NATO, the IMF, and the World Bank, and a founding member of the OECD, OSCE, BSEC, OIC, and G20. After becoming one of the early members of the Council of Europe in 1950, Turkey became an associate member of the EEC in 1963, joined the EU Customs Union in 1995, and started accession negotiations with the European Union in 2005.
Healthcare in Turkey consists of a mix of public and private health services. Turkey introduced universal health care in 2003. Known as Universal Health Insurance Genel Sağlık Sigortası, it is funded by a tax surcharge on employers, currently at 5%. Public-sector funding covers approximately 75.2% of health expenditures. Despite the universal health care, total expenditure on health as a share of GDP is the lowest among OECD countries at 6.3% of GDP, much lower than the OECD average of 9.3%. Average life expectancy is 78.6 years, compared with the EU average of 81 years. Turkey has one of the highest rates of obesity in the world, with nearly one third (29.5%) of its adult population obese.
Source: https://en.wikipedia.org/wiki/Turkey
PRETERM BIRTH RATES –TURKEY
Rank: 56 –Rate: 12% Estimated # of preterm births per 100 live births (USA – 12 %, Global Average: 11.1%)
COMMUNITY

Effects of a home follow-up program in Turkey for urban mothers of premature babies

Nebahat Bora Güneş MSc, PhD, Hicran Çavuşoğlu MSc, PhD
First published: 23 October 2019https://doi.org/10.1111/phn.12671
Abstract
Objective
To examine the effects of a home follow-up program in Turkey on care problems, anxiety, and depression levels of mothers after the birth of a premature baby.
Methods
A semi-experimental study with a pretest–posttest control group design. Eighty premature newborns and their mothers were included in the study. Nursing care was given to mothers and babies in the study group through a total of four home visits on weeks 1, 2, 3, and days 40–42 in Kırıkkale, Turkey guided by the Nursing Diagnosis System and Nursing Interventions Classification (NIC) system of the North American Nursing Diagnosis Association (NANDA). Data were collected from a sociodemographics form, home care needs evaluation form, Edinburgh Postpartum Depression Scale, and State Anxiety Inventory.
Results
There were no significant differences between groups for nursing diagnoses at baseline, while the study group resulted in significantly fewer problems on days 40–42, compared to the control group. Mothers had a comparatively lower depression and state anxiety risk in the study group compared to the control group.
Conclusions
Providing home-based nursing care for preterm mothers and babies during the first 40–42 days has the potential to decrease postnatal care problems, including maternal depression and state anxiety levels.
FULL TEXT –> https://onlinelibrary.wiley.com/doi/abs/10.1111/phn.12671
We appreciate both the simplicity and comprehensive picture of a neonatal therapist scope of practice this article provides for parents/families and healthcare providers/organizations. Please review the full article (links below) for access to the complete study, valuable charts and reference information.

Risk-adjusted/neuroprotective care services in the NICU: the elemental role of the neonatal therapist (OT, PT, SLP)
Jenene W. Craig & Catherine R. Smith Journal of Perinatology volume 40, pages549–559 (2020)
Abstract
Infants admitted to neonatal intensive care units (NICU) require carefully designed risk-adjusted management encompassing a broad spectrum of neonatal subgroups. Key components of an optimal neuroprotective healing NICU environment are presented to support consistent quality of care delivery across NICU settings and levels of care. This article presents a perspective on the role of neonatal therapists—occupational therapists, physical therapists, and speech–language pathologists—in the provision of elemental risk-adjusted neuroprotective care services. In alignment with professional organization competency recommendations from these disciplines, a broad overview of neonatal therapy services is described. Recognizing the staffing budget as one of the more difficult challenges hospital department leaders face, the authors present a formula-based approach to address staff allocations for neonatal therapists working in NICU settings. The article has been reviewed and endorsed by the National Association of Neonatal Therapists, National Association of Neonatal Nurses, and the National Perinatal Association.
Introduction
Infants requiring neonatal intensive care are a particularly vulnerable population secondary to prematurity and/or significant medical conditions. Risk-adjusted care considers the broad spectrum of medical, neurologic, developmental, and psychosocial outcomes experienced by neonatal subgroups [1]. The effectiveness of providing the highest level of care to support family-centered, holistic developmental care services to improve short- and long-term outcomes for preterm and medically fragile neonates is well documented in the literature [2,3,4,5,6,7,8,9]. This has resulted in a standard of care for implementation of developmental care procedures in patient management practices in many neonatal intensive care units (NICUs) in the United States and around the world. However, the elemental components needed to create an optimal neuroprotective healing environment for infants in the NICU lack the requisite standardization recommendations to ensure consistent quality of care delivery across NICU settings and NICU levels of care. A 2017 joint position statement from the Canadian Association of Neonatal Nurses, Canadian Association of Perinatal and Women’s Health Nurses, National Association of Neonatal Nurses (NANN), and Council of International Neonatal Nurses addressed this concern by detailing guidelines for the institutional implementation of developmental neuroprotective care in the NICU [10, 11]. Inclusion of neonatal therapists (NTs) as essential components of a comprehensive preventive model of developmental care in the joint position statement acknowledged the critical contribution of the therapy disciplines to developmental care service design and delivery in the NICU [11, p. 65]. Relatedly, the current article presents a perspective on the role of NTs—occupational therapists (OT), physical therapists (PT), and speech–language pathologists (SLP)—in the provision of elemental risk-adjusted, neuroprotective care services in the NICU.
Background
Neonatal therapy encompasses the art and science of integrating typical development of the infant and family into the environment of the NICU [12,13,14,15,16]. Incorporating theories and scopes of practice from the respective disciplines of occupational therapy, physical therapy, and speech-language pathology, neonatal therapy requires advanced knowledge of the diagnoses and medical interventions inherent to the NICU setting in order to provide safe and effective assessment, planning, and treatment [17]. While the provision of developmental neuroprotective care is a fundamental neonatal nursing responsibility, the five core measures included in the 2011 NANN guidelines serve as imperatives that an optimal neuroprotective environment requires the coordination of care with disciplines of medicine and nursing, including the scope of practice of NTs [18,19,20,21,22,23]. Skilled neonatal therapy competencies support preventative intervention from birth to enhance physiologic function and neurostructural development of the infant with benefits extending to all stakeholders including the infant, family, healthcare community, and provider networks [11, 24,25,26,27,28,29,30,31,32,33,34,35,36].
The Universe of Developmental Care (UDC) Model provides a useful framework to underscore the value of including neonatal therapy as an elemental component of quality service delivery in the NICU [37]. Recognizing the foundational interdependence of a shared surface interface when defining developmental care, the UDC model represents the impact of all body systems and the environment on brain development. Serving as an extension of the Synactive Theory proposed originally by Dr Heidelise Als, UDC purports that “all interactions begin at the organism–environment interface,” with the interface between the infant’s body and the environment serving as the tangible link between the person and all elements of the micro- and macroenvironment [38, 39, p. 146]. Accurate identification of both antecedents and consequences of consistent neuroprotective care formulates the basis to better understand the impact of the organism–environment interface as crucial to the delivery of quality care in the NICU. NTs are integral to the creation of a sensitive transactional interface through their understanding of sensory and environmental factors impacting critical elements of development.
Elemental roles of the neonatal therapist
Defining the necessary components required to provide risk-adjusted age-appropriate neonatal care for complex and critically ill infants will facilitate implementation of standardized care practices consistent with the central tenets of developmental care philosophy and the demonstrable effect on perinatal outcomes. The American Occupational Therapy Association (AOTA), American Physical Therapy Association (APTA), American Speech–Language–Hearing Association (ASHA) define the NICU as a specialized practice setting due to the medical and developmental fragility of the infants, the vulnerable emotional status of the families, and the intricacy of medical, cultural, and social factors that impact the family-infant unit [20,21,22,23, 40]. NTs apply knowledge of neonatal medical conditions, intensive care equipment, preterm infant development and necessary handling precautions, and family system dynamics to contribute to the development of a collaborative management plan that promotes age-appropriate infant neurobehavioral organization and interactions. Interventions provided by NTs optimize long-term development, prevent adverse sequelae, nurture the infant-family dyad, and support education needs of the family and NICU team [12].
Summary/conclusions
A rapidly expanding body of evidence supports the improved scope of outcomes for all involved stakeholders when a comprehensive neuroprotective developmental care model is applied in the NICU setting. Recommendations include neonatal therapy expertize as essential for optimal delivery of an integrated family-centered neuroprotective care model. Provision of therapy services in the NICU is an advanced area of practice for OT, PT, and SLP that requires specialized knowledge and experience to function independently as an expert NT in the NICU. Recommended preparation resources are available to assist licensed professionals to acquire the discipline-specific expertize needed to meet practice standards in this acute medical practice setting. It is incumbent on the individual therapist to work collaboratively within a transdisciplinary service delivery model to maximize the effectiveness of services of all care providers while simultaneously working to gain the requisite discipline-specific advanced training needed to fulfill the unique contributions the respective disciplines offer in this complex acute care setting.
FULL ARTICLE AND CHARTS:
https://www.nature.com/articles/s41372-020-0597-1

Immediate “Kangaroo Mother Care” and Survival of Infants with Low Birth Weight
May 27, 2021 – WHO Immediate KMC Study Group

N Engl J Med 2021; 384:2028-2038
DOI: 10.1056/NEJMoa2026486
BACKGROUND
“Kangaroo mother care,” a type of newborn care involving skin-to-skin contact with the mother or other caregiver, reduces mortality in infants with low birth weight (<2.0 kg) when initiated after stabilization, but the majority of deaths occur before stabilization. The safety and efficacy of kangaroo mother care initiated soon after birth among infants with low birth weight are uncertain.
METHODS
We conducted a randomized, controlled trial in five hospitals in Ghana, India, Malawi, Nigeria, and Tanzania involving infants with a birth weight between 1.0 and 1.799 kg who were assigned to receive immediate kangaroo mother care (intervention) or conventional care in an incubator or a radiant warmer until their condition stabilized and kangaroo mother care thereafter (control). The primary outcomes were death in the neonatal period (the first 28 days of life) and in the first 72 hours of life.
RESULTS
A total of 3211 infants and their mothers were randomly assigned to the intervention group (1609 infants with their mothers) or the control group (1602 infants with their mothers). The median daily duration of skin-to-skin contact in the neonatal intensive care unit was 16.9 hours (interquartile range, 13.0 to 19.7) in the intervention group and 1.5 hours (interquartile range, 0.3 to 3.3) in the control group. Neonatal death occurred in the first 28 days in 191 infants in the intervention group (12.0%) and in 249 infants in the control group (15.7%) (relative risk of death, 0.75; 95% confidence interval [CI], 0.64 to 0.89; P=0.001); neonatal death in the first 72 hours of life occurred in 74 infants in the intervention group (4.6%) and in 92 infants in the control group (5.8%) (relative risk of death, 0.77; 95% CI, 0.58 to 1.04; P=0.09). The trial was stopped early on the recommendation of the data and safety monitoring board owing to the finding of reduced mortality among infants receiving immediate kangaroo mother care.
CONCLUSIONS
Among infants with a birth weight between 1.0 and 1.799 kg, those who received immediate kangaroo mother care had lower mortality at 28 days than those who received conventional care with kangaroo mother care initiated after stabilization; the between-group difference favoring immediate kangaroo mother care at 72 hours was not significant.
<a href=”http://BACKGROUND “Kangaroo mother care,” a type of newborn care involving skin-to-skin contact with the mother or other caregiver, reduces mortality in infants with low birth weight (Source:https://www.nejm.org/doi/full/10.1056/NEJMoa2026486

AAMC estimates 124K more physicians will be needed by 2034, with the largest gap among specialists
by Jacqueline Renfrow – Jun 15, 2021

The U.S. is going to have a massive shortage of physicians in primary and specialty care by 2034, according to new estimates.
The Association of American Medical Colleges (AAMC) projects a shortage between 37,800 and 124,000 physicians, with the largest disparities being in the area of specialty doctors.
The seventh annual study by the life science division of IHS Markit was conducted in 2019, prior to the start of the COVID-19 pandemic, and looked at data such as physician work hours, retirement and other trends in the healthcare workforce.
“The COVID-19 pandemic has highlighted many of the deepest disparities in health and access to health care services and exposed vulnerabilities in the health care system,” AAMC President and CEO David Skorton, M.D., said in a statement. “The pandemic also has underscored the vital role that physicians and other healthcare providers play in our nation’s healthcare infrastructure and the need to ensure we have enough physicians to meet America’s needs.” One of the biggest concerns for the future of physicians is the rise in clinician burnout, which—intensified by the pandemic—has led workers to cut hours or accelerate retirement. Before the pandemic, in 2019, 40% of U.S. physicians felt burned out at least once a week. And according to the survey, more than two out of every five active physicians in the U.S. will reach the age of 65 or older within 10 years.
“We are taking a closer look at the well-being of healthcare workers,” Janis Orlowski, M.D., chief healthcare officer for the AAMC, told Fierce Healthcare. “We had a summit right before COVID with CEOs to discuss what we could do nationally to standardize metrics for credentials and licensing to take the burden of paperwork and overhead from physicians.”
Simultaneously, she said the industry needs to make sure teams are working together locally to improve well-being for all healthcare staff, and ultimately, patients.
Shortage or not, factors within the U.S. population are speeding up the need for more healthcare workers. For example, from 2019 to 2031, the population is projected to grow by 10.6%, with an increase of 42.4% of those aged 65 and above.
Looking at the data specifically, primary care shortages will range between 17,800 and 48,000 physicians. And within specialties, surgical shortages will be one of the highest, between 15,800 and 30,200 physicians.
Orlowski notes the number of medical schools and medical education enrollment are up, which is a positive step toward increasing the number of physicians in the U.S.
And at the end of 2020, Congress added 1,000 new Medicare-supported graduate medical education positions—200 per year for five years—targeted at underserved rural and urban communities. New bipartisan legislation called The Doctors of Community (DOC) Act, introduced in the House of Representatives Tuesday and expected to be released in the Senate next week, would permanently authorize the Teaching Health Center Graduate Medical Education program that aims to train primary care medical and dental doctors. The legislation would increase annual funding by more than $500 million per year from 2024 through 2033.
Finally, the pandemic has put a spotlight on disparities in health and access to care among underserved populations in the U.S. The estimates in the survey do not include the additional 180,400 physicians AAMC believes the country would need if there were fewer barriers to access for minority populations as well as if people living in rural communities and people without health insurance were included.
“The issue that I’m probably most worried about is equity,” said Orlowski. “As we take a look at equity throughout the U.S. and how different populations are affected by COVID, it strikingly points out the differences of access and utilization. If everyone had the same access to physicians as those who are living in an urban center, white, not low-income, we would still need more than 180,000 physicians to build equity. And that’s not 15 years from now, that’s today.”
Source:https://www.fiercehealthcare.com/practices/physician-shortage-continues-to-widen-now-estimated-at-124-000-by-2034

HEALTH CARE PARTNERS

Neonatal Intensive Care Unit Admission Temperatures of Infants 1500 g or More -The Cold Truth

ORIGINAL RESEARCH: Apanovitch, Audrey R. BS, RN; McGrath, Jacqueline M. PhD, RN, FNAP, FAAN; McGlothen-Bell, Kelly PhD, RN, IBCLC; Briere, Carrie-Ellen PhD, RN, CLC Advances in Neonatal Care: June 2021 – Volume 21 – Issue 3 – p 214-221 doi: 10.1097/ANC.0000000000000787
Abstract
Background:
Smaller preterm infants often receive extra attention with implementation of additional thermoregulation interventions in the delivery room. Yet, these bundles of interventions have largely remained understudied in larger infants.
Purpose:
The purpose of this study was to evaluate initial (or admission) temperatures of infants born weighing 1500 g or more with diagnoses requiring admission to the neonatal intensive care unit (NICU).
Methods:
Retrospective medical record review of 388 infants weighing 1500 g or more admitted to the NICU between January 2016 and June 2017.
Result:
In total, 42.5% of infants weighing 1500 g or more were admitted hypothermic (<36.5°C), 54.4% with a normothermic temperature, and 2.8% were hyperthermic. Of those infants admitted hypothermic, 30.4% had an admission temperature ranging from 36°C to 36.4°C and 12.1% had an admission temperature of less than 36°C. When compared with infants weighing less than 1500 g, who were born at the same institution and received extra thermal support interventions, there was a statistically significant difference (P < .001) between admission temperatures where infants less than 1500 g were slightly warmer (36.8°C vs 36.5°C).
Implications for Practice:
Ongoing admission temperature monitoring of all infants requiring NICU admission regardless of birth weight or admission diagnosis is important if we are going to provide the best support to decrease mortality and morbidity for this high-risk population.
Implications for Research:
While this study examined short-term outcomes, effects on long-term outcomes were not addressed. Findings could be used to design targeted interventions to support thermal regulation for all high-risk infants.
Conclusion:
Neonates admitted to the NICU weighing 1500 g or more are at high risk for developing hypothermia, similar to smaller preterm infants.

What Did Pre-COVID PTSD Look Like for Interns?
— Life-related risk factors played a key role, study found by Kara Grant, Enterprise & Investigative Writer, MedPage Today June 8, 2021

Symptoms of work-related post-traumatic stress disorder (PTSD) were three times higher for interns than the general population, according to a 2018 study.
There were 10.8% of intern physicians who screened positive for PTSD at the end of their first internship year compared with a 12-month prevalence of 3.6% in the general population, reported Mary Vance, MD, of the Uniformed Services University’s Center for the Study of Traumatic Stress in Bethesda, Maryland, and colleagues.
Among 1,134 resident physicians surveyed, 56.4% reported exposure to trauma in the workplace, and 19% of that group screened positive for PTSD by the end of their residency, the authors wrote in JAMA Network Open.
“Doctors with PTSD … in addition to being unwell, don’t necessarily function at the top of their ability,” commented Albert Wu, MD, of Johns Hopkins Bloomberg School of Public Health in Baltimore, who was not involved with the study. “This can diminish their ability to deliver the best quality care, and may increase incidents of medical errors,” he told MedPage Today.
Wu coined the term “second victim” over 2 decades ago to highlight the need for mental health services for doctors who were involved in a medical error. He explained that physicians-in-training are particularly susceptible to trauma exposure, as they are just beginning to adjust to the onslaught of new stressors from residency.
For the study, Vance and colleagues contacted interns from participating institutions across a wide array of specialties 2 months before the start of participants’ training. After this baseline assessment, there were four follow-up surveys sent via email at months 3, 6, and 12 of internship. The authors used the Primary Care PTSD Screen for DSM-5 to assess trauma exposure and PTSD symptoms.
The mean age of those surveyed was about 28; 58.6% were women and 61.6% were non-Hispanic white.
Multivariable logistic regression analyses found, not surprisingly, that those who reported working longer hours experienced higher rates of exposure to work-related trauma (OR 1.01, 95% CI 1.00-1.03, P=o.03). Early family environment and the presence of stressful life events at baseline were also significant risk factors (OR 1.03, 95% CI 1.01-1.05, P<0.001; OR 1.46, 95% CI 1.06-2.0, P=0.02, respectively) for trauma exposure, the researchers found.
There were associations between screening positive for PTSD and certain risk factors, such as being unmarried (OR 2.00, 95% CI 1.07-3.73, P=0.03) or experiencing stressful life events during internship (OR 1.43, 95% CI 1.14-1.81, P=0.002).
While there was no association between specialty and trauma exposure overall, the authors found surgery and psychiatry were “less associated” with PTSD following work exposure (OR 0.26, 95% CI 0.09-0.81, OR 0.15, 95% CI 0.03-0.77, respectively), but Vance’s group urged caution when interpreting these findings as they were only compared to internal medicine.
For interns and residents who reported depression during their last month of training, there was a significant association between depression and PTSD (OR 2.52, 95% CI 1.36-4.65, P=0.003). PTSD and reports of anxiety during the last month of residency were also significant (OR 2.14, 95% CI 1.13-4.04, P=0.02), the team reported.
Study limitations included the relatively low response rate to the survey (26% overall).
“More research is needed to determine the prevalence of trauma exposure and PTSD at different stages of a physician’s career,” the researchers concluded.
Wu agreed, noting that the interns who made it through the survey process may have wanted a platform to air out frustrations and grievances; he suggested that, as a result, the study’s rates of PTSD symptoms might be an overestimation.
He said that considering the physicians who started their journey into residency during a pandemic, COVID-19, and the high rates of work-related trauma that emerging doctors have experienced this year have made medicine more receptive to conversations around PTSD and funding future research.
“Interns experience tremendous stress during training,” he said. “I’d like to see every training program … take steps to make sure they have adequate support systems in place for … their most valuable asset — their health workers.”
JAMA Network Open
Source: https://www.medpagetoday.com/psychiatry/anxietystress/92994?vpass=1

Barriers to Kangaroo Care in the NICU A Qualitative Study Analyzing Parent Survey Responses
Saltzmann, April M. RN, MSN, NNP-BC; Sigurdson, Krista PhD; Scala, Melissa MD Editor(s): Dowling, Donna PhD, RN; ; Schierholz, Elizabeth PhD, MSN, NNP-BC; ; Parker, Leslie PhD, APRN, FAAN; Advances in Neonatal Care: May 27, 2021 – Volume Publish Ahead of Print – Issue – doi: 10.1097/ANC.0000000000000907
Abstract
Background:
Despite its benefits, parents in the neonatal intensive care unit (NICU) face significant barriers to kangaroo care (KC). Clinician-reported barriers to KC include staff education, environment, and equipment among others; however, parent-perceived barriers are underexplored.
Purpose:
To examine parental understanding of KC, parental perception of experiences with KC, and parental views on the key factors that help or hinder KC.
Methods:
This is an observational, mixed-methods study that used an author-developed survey to assess parental feelings, perceived importance, and barriers to KC. Likert scale responses were analyzed using descriptive statistics. Free-text responses were analyzed using thematic analysis. A comparison of results was made between parents receiving and not receiving infant mental health services.
Results:
Fifty (N = 50) parents completed surveys. Eighty percent of parents stated they wanted more information on KC. Common barriers to KC were reported by parents, such as issues with space/environment. The most frequently reported barrier when asked openly was fear of hurting their infant. Ninety-six percent of parents believed that KC helped their emotional well-being. Parents receiving mental health services reported more fear but results did not reach significance.
Implications for Practice and Research:
The frequency with which factors are reported as important to parents may allow a prioritization of barriers to KC, which may help focus quality improvement initiatives. The results of this study underscore the vital role nurses play in supporting KC. Additional attention needs to be given to the mental health of NICU parents and its impact on care practices.
© 2021 by The National Association of Neonatal Nurses
INNOVATIONS

Gravens by Design: Should Nurturing Stimuli be Limited to Times When a Preterm Baby is Awake?
For many years, the NICU was an undesirable place for a baby’s brain to develop. Lights were bright, the noise was pervasive, painful procedures plentiful, sleep disturbed frequently, and parental access severely restricted. There has been a gradual awakening to the adverse effects this can have on a premature infant who is in the “synaptic explosion” stage of brain growth and development, which, coupled with technological changes that allow us to monitor babies better and less invasively, has enabled us to minimize these noxious stimuli. The importance of infant sleep to brain development has also gained greater recognition so that timing necessary interventions to protect sleep is happening more often.
Concurrently, there has also been a move to introduce nurturing stimuli into the baby’s experience. Skin-to-skin care (1), music (2), reading (3,4), and circadian lighting (5) are examples of such stimuli that are much more commonly offered today than they were in the earlier days of NICU care.
Unfortunately, in many NICUs, the effort to reduce overstimulation and protect infant sleep has come into conflict with the desire to provide nurturing stimuli. It is hypothesized by some practitioners that there is danger in providing these stimuli when an infant is asleep on the grounds that it may cause overstimulation or interfere with the important sleep cycle itself. Thus, nurses and parents are often admonished to stop reading and providing music once their baby falls asleep and to keep the lights dim. Some also prescribe a maximum amount of time these stimuli should be provided in the course of a day, suggesting again that there is a risk of overstimulation. In fact, there is no data to support these beliefs; it is more likely an overly enthusiastic acceptance of the desire to protect babies that has led to this practice – good intentions can have unintended consequences. William Fifer demonstrated that newborns, unlike any other age group, learn while they are asleep (6,7). In utero, we know that infants learn to recognize their mother’s voice (8) and smell; we also know that the fetus sleeps most of the time, so these stimuli are likely presented and learned for many hours every day, much of that time while the fetus is asleep.
Unless new data demonstrate that presenting these nurturing stimuli to babies is harmful or that limits are necessary, then we should no longer proscribe their use once an infant falls asleep. Babies are likely to benefit and, in all likelihood, will not be harmed by continuing to provide them with auditory, vestibular, and circadian stimuli throughout the sleep cycle. Of course, these stimuli should be removed if the baby appears to react adversely, but it is much more common to see that babies continue to sleep peacefully even when the nurturing stimuli are continued. Incubators and private rooms are important tools for protecting babies from overstimulation, but they can also become isolation chambers if parents are absent and we do not enrich their sensory environment or do so only in small doses. The best environment for neurosensory development in the NICU is in the arms of a caregiver or when that is not feasible in the presence of nurturing stimuli. Certainly, we need more data to determine what that should look like exactly, but our default should not limit sensory input altogether in a well-meaning effort to protect infant sleep.
Source:https://www.neonatologytoday.net/newsletters/nt-may21.pdf
Fetal Surgery Boosts Survival for Babies With Severe Birth Defect
— Randomized trial confirms benefit of complex fetal procedure
by Amanda D’Ambrosio, Enterprise & Investigative Writer, MedPage Today June 8, 2021

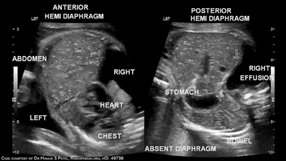
Fetoscopic endoluminal tracheal occlusion (FETO) resulted in higher survival rates among babies with severe diaphragmatic hernia on the left side, according to a randomized trial.
Fetuses with severe left diaphragmatic hernia, a condition that disrupts normal airway and pulmonary vascular development, had more than double the chances of surviving to discharge from the NICU after they underwent FETO between 27 and 29 weeks’ gestation, compared to fetuses that received expectant care (RR 2.67, 95% CI 1.22-6.11), reported Jan Deprest, MD, PhD, of University Hospitals Leuven in Belgium, and colleagues.
Fetoscopic endoluminal tracheal occlusion (FETO) resulted in higher survival rates among babies with severe diaphragmatic hernia on the left side, according to a randomized trial.
Fetuses with severe left diaphragmatic hernia, a condition that disrupts normal airway and pulmonary vascular development, had more than double the chances of surviving to discharge from the NICU after they underwent FETO between 27 and 29 weeks’ gestation, compared to fetuses that received expectant care (RR 2.67, 95% CI 1.22-6.11), reported Jan Deprest, MD, PhD, of University Hospitals Leuven in Belgium, and colleagues.
Infant survival rates in the FETO group were identical up to 6 months after the procedure, the researchers wrote in an early edition of the New England Journal of Medicine.
The prevalence of severe diaphragmatic hernia is 1 in 4,000 infants, with around 85% of the defects occurring on the left side. Deprest and colleagues stated that the condition is associated with high rates of neonatal death from respiratory failure or pulmonary hypertension, as the hernia blocks a fetus’s airway and can disrupt lung growth.
Fetal lung growth can be stimulated by tracheal obstruction, the researchers noted. During FETO, clinicians prenatally insert a small, inflatable balloon into a fetus’s trachea, which can be done while the mother is under local anesthesia. A few weeks after insertion, the balloon is removed.
Deprest said that observational data previously indicated that FETO may increase survival rates among fetuses with congenital diaphragmatic hernia, but this randomized trial was able to confirm that benefit. Now, he said, researchers are looking into ways to optimize timing of diagnosis.
“To have choices, parents need to have a prenatal diagnosis, and it is better to have that by end of the second or beginning of the third trimester,” he told MedPage Today.
Deprest’s group did find some adverse effects. FETO was associated with a higher risk of preterm, pre-labor rupture of membranes (RR 4.51, 95% CI 1.83-11.9), and preterm birth (RR 2.59, 95% CI 1.59-4.52).
Additionally, the researchers conducted another study published in the New England Journal of Medicine evaluating the effect of the procedure on fetuses with moderate congenital diaphragmatic hernia on the left side. The group found no benefit of FETO when performed between 30 and 32 weeks (RR 1.27, 95% CI 0.99-1.63, P=0.06).
“To me, it was surprising that there was a difference in the effect,” Deprest said. “But in retrospect, this probably has to do with the fact that we did the operation later,” he added, noting that in fetuses with a severe condition, the procedure was likely to be performed at least a week earlier than those with moderate illness.
In an accompanying editorial, Francis Sessions Cole, MD, of the Washington University School of Medicine in St. Louis, said that the data from this trial increase our understanding of FETO and may help inform counseling for parents. However, Cole stated that this trial is limited in that it only followed infants 6 months after the procedure, and did not perform prospective genetic screening.
Cole added that the trial raises technical questions about the procedure, including the frequency of spontaneous balloon deflation prior to removal, as well as the increased risk of pre-labor rupture of membranes and preterm birth.
“The current reports serve as a critical basis for future studies to improve outcomes in pregnancies complicated by fetal congenital diaphragmatic hernia and in infants,” Cole wrote.
Study Details
Deprest and colleagues designed the Tracheal Occlusion to Accelerate Lung Growth (TOTAL) trial, to assess postnatal survival rates after FETO in infants with severe pulmonary hypoplasia from a diaphragmatic hernia on the left side. They conducted the open-label, randomized trial in 10 FETO centers and 26 neonatal care centers in several countries, including Belgium, Japan, the U.S., and others.
Women were included in the study if they were older than age 18, had a singleton pregnancy, were at a gestational age less than 30 weeks, had congenital diaphragmatic hernia on the left side and severe pulmonary hypoplasia. Mothers were excluded if they had conditions that would make fetal surgery risky or an elevated risk of preterm birth.
Starting in February 2011, researchers conducted preliminary assessments on more than 1,300 mothers carrying fetuses with congenital diaphragmatic hernia. The trial was stopped in March 2020 for efficacy at the third interim analysis, and 80 women were ultimately included. Of these, 40 were randomized to FETO surgery and 40 to expectant care. There were no differences in baseline characteristics between groups.
A total of 40% of infants in the FETO group and 15% in the expectant care group survived to discharge from the NICU. Survival at 6 months was identical to survival at discharge from the NICU.
In 38% of patients, delivery occurred within 24 hours after balloon removal. Preterm, pre-labor rupture of membranes occurred in 47% of mothers in the FETO group, while it occurred in only 11% in the expectant care group. Preterm birth was observed in 75% of women in the FETO cohort, compared to 29% in the expectant care group.
Among the FETO procedures, there were five spontaneous balloon deflations. Additionally, there was one case of placental laceration from fetoscopic balloon removal that led to neonatal death, and another neonatal death from failed balloon removal.
Deprest and colleagues noted that their results were limited by the long duration of the trial, as protocols for postnatal care of congenital diaphragmatic hernia may have changed. The group also acknowledged that this study only provides information on short-term outcomes, and that future studies are needed to assess the long-term effects of FETO. Finally, as the trial involved experienced fetal surgery units, the researchers said that results should not be generalized to centers that do not have experience in fetoscopy or FETO.
Deprest stated that future research will evaluate optimal timing of diagnosis, and medications that could improve the success of the procedure. “But there is hope now, for these patients,” he said.
Source:https://www.medpagetoday.com/obgyn/pregnancy/92984
This subject is very close to my heart and intellect. I also want to shout out to Bruce Lipton PhD, a global leader in the science of epigenetics, whose work I have followed for decades. Treatment for preverbal PTSD, which many preemies may experience, is critically lacking. Expertise towards developing therapies to treat preterm birth survivors who experience preverbal PTSD is not developed or available. A key component in the neonate development to consider beyond unique NICU stimulus is the lack of human touch. I believe that an essential component in developing treatment for the effects (physical, cognitive, neurological, psychological, developmental) of preterm birth experience is to avoid assuming that symptom-similar psychological/cognitive behaviors imply similar interventions are effective and adequate. It is critical to look at the preterm birth development process as a unique human developmental experience that justifies focused research and specifically related medical, physical, behavioral, educational, cognitive and psychological treatment options.

Epigenetics Explains the Imperative for Extended, Intimate Human Contact in Every Newborn, Especially Those at the Highest Risk
“Developmental Care,” a term often used to encompass both sensory protection and targeted sensory stimulation in high-risk newborns, has faced two serious challenges since its inception:
• It has been difficult to prove its value.
• It has not been easy to incorporate into a NICU culture.
The primary tenets of developmental care – that newborns should be protected from noxious stimuli and provided with age-appropriate nurturing stimuli by their parents whenever possible – were established in extensive studies decades ago. In the 1950s, John Bowlby (in humans) and Harry Harlow (in monkeys) showed that separating newborns from their mothers led to immediate and lasting psychological changes. Even so, this separation continued to be practiced in newborn nurseries until it was successfully challenged by Marshall Klaus and John Kennell in the 1970s. Their work led to a radical change in maternity services in the newborn nursery but a much lesser degree in the NICU.
As parents continued to be excluded from the NICU or, at best, allowed to “visit” their infants, efforts to enrich the sensory environment in the absence of parental caregiving were introduced, of which the Newborn Individualized Developmental Care and Assessment Program (NIDCAP) is the most notable example. A highly structured, labor-intensive, specialist-based program, NIDCAP became well-established in some NICUs, supported by several trials that suggested efficacy (1), but has not been adopted by a large majority of NICUs because of its cost, complexity, and absence of evidence of a compelling benefit(2). However, several other developmental care-based programs have been introduced, some of which, such as the SENSE program, are actively being studied (3).
Concurrent with these efforts, families have been granted increased access to their infants as both structural and operational barriers are removed. The importance of family participation is emphasized in NIDCAP, SENSE, and similar programs, but the value of simple skin-to-skin care, even without a structured developmental care program, has also been demonstrated. While numerous trials suggest efficacy, meta-analysis has yet to confirm the benefit of skin-to-skin care in high-risk premature infants except in resource-limited settings (4).
Perhaps the chief challenge with these efforts has been that neuronal development in the premature infant is still largely a “black box.” The impact of a ventilator change, a dose of surfactant, or most other NICU interventions can be easily demonstrated – if not immediately, then at least within a short time and almost always by the time an infant is discharged. However, there is no such obvious positive response to developmental care that a clinician can appreciate by making rounds. A NIDCAP therapist can detect responses to interventions, as can a nurse when an infant is being held skin-to-skin, but these do not show up on the datasheets or outcome measures that drive decision-making in the NICU. It may well be that more long-term brain deficits are secondary to inadequate developmental care in the NICU than to intraventricular hemorrhage, but we have no real-time markers available to us to study this.
Developmental Care Has Not Been Easy to Incorporate into a NICU’s Culture:
Providing the optimal sensory environment for high-risk newborns throughout their NICU stay is challenging for multiple reasons:
• Parental interaction is often restricted by operational rules or by parental absence.
• Nursing provision of developmental support is seen as secondary and optional in many NICUs. Nurses obtain vital signs, provide feedings, and change diapers in even the most stable infants; they understand there will be consequences if they do not do this. But all these tasks can be accomplished without providing any nurturing stimuli and neglecting this aspect of care rarely brings any consequences to the provider.
• Developmental specialists are costly in that their services generally do not generate revenue
If developmental care provided immediate evidence of its value or generated revenue, it would be much easier to incorporate into the fabric of NICU care.
Is There a Way Forward?
It is unlikely that strong data to support developmental care or skin-to-skin care in high-risk infants will appear in the near future, given that large, multi-center trials are not currently in progress and are unlikely to be launched due to their cost and complexity.
Fortunately, in an ironic twist that Harry Harlow would best appreciate, we have been able to return to studies in primates to find compelling evidence of the lifelong impact of sensory deprivation caused by the separation of babies from their mothers at birth, expressed in a language that modern-day scientists understand: DNA methylation. In a fascinating TED talk (5), Moshe Szyf describes how early life experience, especially maternal-infant interaction, influences the long-term expression of many genes. Monkey newborns who are separated from their mothers appear healthy, but an examination of DNA methylation of their genome reveals dramatic differences from siblings who remained with the mother. As in Harlow’s studies, the monkeys who provided surrogate care suffered long-term psychological and physical differences that could not be explained by genetic differences or health in infancy. Instead, the lack of normal sensory input early in life led to a permanent change in gene expression that persisted into adulthood. These trials provide evidence that cannot ethically be obtained in humans but is certainly relevant to the NICU environment of care. It requires little imagination to draw a line connecting these findings to the continued high burden of neuropsychological disability seen in NICU graduates.
Epigenetics, then, explains how early life experiences influence the expression of the genetic code, even for neurons yet to form. Changes in DNA methylation that occur early in infancy can have a lifelong impact on health and behavior. Neuronal growth, synaptic formation, and DNA methylation are not put “on hold” while the infant is in the NICU; therefore, developmentally supportive care, centered around parents whenever possible, is an essential component of state-of-the-art NICU care.
Source:http://www.neonatologytoday.net/newsletters/nt-jun21.pdf

How Early Life Experience is Written into DNA
Moshe Szyf is a pioneer in the field of epigenetics, the study of how living things reprogram their genome in response to social factors like stress and lack of food. His research suggests that biochemical signals passed from mothers to offspring tell the child what kind of world they’re going to live in, changing the expression of genes. “DNA isn’t just a sequence of letters; it’s not just a script.” Szyf says. “DNA is a dynamic movie in which our experiences are being written.”
This talk was presented to a local audience at TEDxBratislava, an independent event. TED’s editors chose to feature it for you.

PREEMIE FAMILY PARTNERS

Miracle baby clutches onto life in central Turkey
KONYA, Turkey

Zehra Melek Cat |08.01.2021
Baby girl born 520 grams in 23rd week of pregnancy discharges from hospital following 142 days of treatment.
A miracle baby girl born 520 grams (1.1 pounds) in the 23rd week of pregnancy in central Turkey clutched onto the life following the 142 days of treatment.
Dilber Nisa Varis, the third child in the family, was born early by cesarean section in the central Konya province.
Emete Varis, 30, the mother of the miracle baby, who gave birth at the Selcuk University Faculty of Medicine Hospital, experienced the happiness of holding her baby in her arms after five months of treatment in an incubator.
The baby, who reached a weight of 1,800 grams (nearly 4 pounds), was discharged with the applause of the hospital staff, and reunited with her two elder sisters and parents at home.
“My other kids were [born] normal. My pregnancy [this time] was problematic. We filled 23 weeks with treatment under constant doctor control,” Varis told Anadolu Agency.
Noting that doctors warned her during the pregnancy about the possible outcomes, Varis said she is very happy that her baby overcame the difficulties.
“Thank God we reached these days. We have been in a mother-baby adaptation program for three weeks. Before I was coming occasionally [to the hospital] and leaving breast milk for the baby,” the mother said, adding that she had some worries because the baby is still very small.
Hanifi Soylu, a pediatrics professor and head of the neonatal division at Selcuk University, emphasized that there are generally some health problems observed in premature babies, adding that the miracle baby also had problems related to nutrition and breathing.
“We are sending the baby home healthily without any bleeding in her head and without being dependent on oxygen [machine],” he said.
Soylu underlined that “saving a life of a baby is like saving the whole mankind.”
*Writing by Jeyhun Aliyev from Ankara
Source:https://www.aa.com.tr/en/life/miracle-baby-clutches-onto-life-in-central-turkey/2103040

Prevalences and predictive factors of maternal trauma through 18 months after premature birth: A longitudinal, observational and descriptive study

Citation: Brunson E, Thierry A, Ligier F, Vulliez-Coady L, Novo A, Rolland A-C, et al. (2021) Prevalences and predictive factors of maternal trauma through 18 months after premature birth: A longitudinal, observational and descriptive study. PLoS ONE 16(2): e0246758. https://doi.org/10.1371/journal.pone.0246758
Abstract
Posttraumatic reactions are common among mothers of preterm infants and can have a negative influence on their quality of life and lead to interactional difficulties with their baby. Given the possible trajectories of posttraumatic reactions, we hypothesized that prevalences of postpartum posttraumatic reactions at given times underestimate the real amount of mothers experiencing these symptoms within 18 months following delivery. Additionally, we examined whether sociodemographic and clinical characteristics of dyads influence the expression of posttraumatic symptoms among these mothers. A sample of 100 dyads was included in this longitudinal study led by 3 french university hospitals. Preterm infants born before 32 weeks of gestation and their mothers were followed-up over 18 months and attended 5 visits assessing the infants’ health conditions and the mothers’ psychological state with validated scales. Fifty dyads were retained through the 18 months of the study. The period prevalence of posttraumatic reactions was calculated and a group comparison was conducted to determine their predictive factors. Thirty-six percent of the mothers currently suffered from posttraumatic symptoms 18 months after their preterm delivery. The 18 months period prevalence was 60.4% among all the mothers who participated until the end of the follow-up. There was a statistical link between posttraumatic symptoms and a shorter gestational age at delivery, C-section, and the mother’s psychological state of mind at every assessment time. Only a small proportion of mothers were receiving psychological support at 18 months. Preterm mothers are a population at risk of developing a long-lasting postpartum posttraumatic disorder, therefore immediate and delayed systematic screenings for posttraumatic symptoms are strongly recommended to guide at-risk mothers towards appropriate psychological support.
Full Article –> https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0246758

Understanding Paternal Grief at the Loss of a Child

Barb Himes, IBCLC, Kelly D. Farley
June brings us Father’s Day, which can be a difficult time for fathers who have lost a child. First Candle’s bereavement support services have been there for fathers as well as mothers and other family members, and we have come to know Kelly D. Farley, the author of Grieving Dads: To the Brink and Back. Kelly and his wife Christine lost their daughter Katie in 2004 and their son Noah in 2006, both stillborn. It changed his life, leading him to seek help for his grief and become involved in helping other grieving fathers.
Today he provides individual and group counseling for fathers and continues to write extensively on facing and living with paternal grief. In honor of Father’s Day, we share some of his work, which may offer health care providers insights into this side of bereavement when an infant is lost to Sudden Unexpected Infant Death (SUID) or a child is lost due to other causes.
Father’s Day Void
I spent two years interviewing men that have experienced the death of a child. As you can imagine, I heard a lot of heartbreaking stories. All were different, and all were bad. I also learned a lot about my own pain and suffering caused by the aftermath of burying two children. Those interviews, and my own hard lessons, are captured in my book Grieving Dads: To the Brink and Back.
I have tried to become an advocate of sorts for grieving dads. My goal is to make sure these men feel like they have the permission to grieve, to feel the impact, and express their pain without society trying to hush them because the topic of a child’s death is uncomfortable for those who have not experienced it.
Because of my book and my advocacy, I receive a lot of requests to write Father’s Day articles about the dark side of the day from the perspective of the guys who have had to bury a child. Is the day harder than most? Yes, but to us grieving dads, it is not much different from the holidays, birthdays, and death anniversaries. They are all difficult to navigate, and each one stirs similar but different emotions.
There is not a day that goes by that we do not think about our absent child. Regardless of the circumstance of their deaths, we miss them deeply. However, there are days where we feel this pain more acutely than other days. Days like Father’s Day remind us that they are not here. We are keenly aware of their absence every single day, and on days like Father’s Day, the hole they left grows a little bigger.
We feel a sense of emptiness on Father’s Day because there is an obvious void that tends to suck the air out of the day, creating a difficult space that we do not know how to navigate. We try our best, but it is hard to explain our feelings to those that haven’t lost a child. It is not fair for us to expect you to understand; you’re one of the lucky ones that have never had to walk in these shoes.
Most of us will try to keep our minds occupied with other living children or by filling the day with busy, mindless tasks. It’s a defense mechanism that helps us to hide from the harsh reality that lurks in the darkness, seeking our whereabouts. It’s a constant battle that we often lose in the early years. Yes, I said years.
This isn’t something that goes away after a year. It’s a burden that weighs heavy on our souls for the rest of our lives. However, the weight lightens dramatically as time moves forward, and we continue to process our loss. The death of a child becomes who we are. It does not define us, but it certainly changes the course of our lives and destroys the naivety we once had.
Regardless of the day, most people will not bring up the fact that your child died because it is too awkward for them. They are not sure if they should acknowledge this day. Let me resolve this confusion: you should acknowledge Father’s Day.
It certainly isn’t a “Happy” Father’s Day. So, what should people say or do?
Try saying something like, “I know this must be a difficult day, but know I am thinking about you.” This statement, or a variation of it, goes a long way with the men that are on the receiving end of it. It might trigger a visible emotion, but know the emotion constantly lurks just below the surface regardless. Though you just don’t see it, it’s just waiting for an opportunity to escape. I wish all fellow grieving dads a peaceful Father’s Day. If you know a grieving dad, pay them a visit, or make that phone call to tell them that you are thinking about them and their child. – KDF
Source: https://firstcandle.org/



Let’s Get Physical! 20 Easy Exercise Ideas for Parents and Kids

Thursday, July 23, 2020
“Don’t look at it as exercise — instead, play games and have a ton of fun! The main thing is just to get outside every day and do something you think is fun. You can play sports like soccer, basketball, or badminton. You can play games like freeze tag or ride a bike or do running races with your friends or family. You can go on hikes with your family or go swimming or paddling. Do lots of different things, and again, focus on having fun, and doing it often.” – Leo Babauta
You’re a parent, so you don’t have time to exercise, right? I can relate. But moving our bodies is a basic part of self-care. We can’t nurture our kids with emotional generosity unless we nurture ourselves at the same time. And we aren’t fully nurturing ourselves unless we figure out a way to get physical.
We all feel a lot more energetic when we move and stretch. It actually changes the chemistry of our bodies so we’re happier, more relaxed, and our bodies are healthier. We not only look better, we feel better — and so we “act” better as parents. Exercise is the one of the most effective “treatments” for tendencies to anxiety and depression, after deep breathing and getting enough sleep. What more incentive do you need?
If you can motivate yourself to go out running, or do a yoga class online, and you can leave your kids with your partner, you’ve got it covered. But if you’re like the rest of us, you need to find fun ways to be active while you’re WITH your children. Luckily, you have children to be active with, so you have a head start!
Kids love it when you play physically with them. It’s a terrific way to add some connection and fun back into a relationship that too often deteriorates into constant correction and conflict. You don’t need to tell your kids this exercising is for you — they’ll assume it’s special family time! And if your child is spending too much time staring at screens, this is the best way to get her up and moving.
The secret is setting aside the time. Even ten minutes a day outside together is a great start during the week. On the weekend, you can plan an outing. Before you know it, you’ll have worked up to 20 minutes daily, with an hour on weekend days. Sure, you’ll skip some days. But if that’s more exercise than you’re getting now, read on.
- For Instance:
- Put on music and have a family dance party.
- Use your little one as a football; run her around the rest of the family into the end zone. Your will love it.
- Take a soccer ball outside and take turns chasing each other as you dribble the ball. Kids love the soccer practice.
- Play tag or frisbee with your children.
- Bring your wipes and hand sanitizer and join your kids on the monkey bars. Great upper body workout! Who cares what the other parents think?
- Roughhouse! Play “Take off each others’ socks,” wrestling, or chase games. Anything that gets your kids laughing. That’s a huge bonus, because you’re helping them evaporate any anxieties they’re carrying around.
- Let each person in the family take turns being the leader while the rest of the family follows,doing jumping jacks, sun salutations, sit-ups, or invented moves.
- Keep any bubble wrap that comes your way in a bag at the back of your closet. On a rainy day, pull it out for a Bubble-Wrap dance party!
- Find good work-out classes for kids online, and exercise with your kids.
- For outings:
- Load the kids and their bikes or scooters into the car and drive to the track at your local high school when it’s empty. Let the kids ride their trikes or bikes around the track, while you walk or jog.
- Online “Baby & Me” yoga classes will help you keep good form while you get your stretch on.
- Listen to your favorite podcasts while you walk briskly with your little one in a carrier or stroller.
- Take family pride in how far you can park from your destination and walk. (“Is this a two \block day? Let’s go for it!”)
- Let your exercise time double as social time by distance-walking with a friend and her child; the kids will entertain each other.
- Chasing your toddler all over the park? Instead of resenting it, get a pedometer, and work up to 10,000 steps a day.
- If your child is old enough, bike or roller blade together. One dad I know took up skate boarding with his 11 year old. Great for his body, great for their relationship as his son headed into the teen years.
- Want to get an older child or teen moving? Do a charity run together.
- When you’re working:
- Work standing whenever possible.
- Walk around while you’re on the phone. Use a pedometer and keep trying to increase your daily steps.
You won’t believe how much ten minutes of movement daily will lift your mood. And when we feel good, it has an almost magical effect on our children. We have a lighter touch, and a sense of humor. We don’t get triggered as easily. All of which makes our kids happier and more cooperative. So think of this as “we” time– bonding time with your family that gives you huge collateral benefits.
You’re also getting your child hooked on an active lifestyle, which is a great counter-balance to all that screen-time in our lives. Kids who are physically active into the preteen and teen years are 75% less likely to be overweight or feel they aren’t fit as adults.
If you do this every single day, you’ll all start looking forward to it. Way to nurture yourself and your child at the same time!
Source:https://www.ahaparenting.com/blog/15_Easy_Exercise_Ideas_Parents_Babies_Kids_Children#
Zumba Kids Class What Does the Fox Say Dance / Zumba® Fitness Choreography
Apr 11, 2014
Michelle Smith Apr 11, 2014
Zumba Kids Class What Does the Fox Say. We had a great time dressing up and doing this song. Please give us a like because the kids worked very hard practicing this routine to bring to you. I hope you enjoy.

The Hero In All of US
Gannon is our PTSD rescue cat. He has been healing our PTSD wounds for the past 4 ½ years, and it has been a mutual exchange.
A few weeks ago, when going out to grab some ice cream, Gannon, in his carrier, was stolen from my car. I was only gone for 7 minutes and parked directly outside of a local ice cream parlor. Following a frozen moment of gut-wrenching terror, I jumped into action, checking the surrounding area in hopes the culprit threw Gannon out of his carrier.
After a phone call to my mom and reporting the incident to local police, I asked some of the local community members in the Lake City homeless encampment across from the ice cream parlor if they had seen anyone in the area with a red carrier and a cat. They were fast to respond, exclaiming they had seen a man with Gannon and that they were already working together to try to get some of their friends to stop the man from attempting to sell Gannon to someone residing in a trailer park down the street. Within the span of 2 minutes, they located where Gannon was going, and two young men took off to bring Gannon back. Within 10 minutes they texted me photos of their rescue (shown above) and shortly thereafter they arrived safely back to the encampment with Gannon in his carrier.
My mom and I felt so devasted by the temporary loss and so overwhelmingly blessed by the actions of good people.
We often villainize, misunderstand, judge, misrepresent the homeless. The community of the Lake City homeless encampment represented to us a true “community” and characterized the Hero in all of us. At its best, community represents caring for and doing right with/beside others. Even in the face of great adversity the community members of the Lake City encampment demonstrated solid citizenship, neighborly love, good will, integrity and grit. The community went out of their way to help a stranger and rescue a precious life.
As a global neonatal community, we have all faced the challenge of adversity in times of uncertainty and we share a common thread that connects us all as a part of humanity. There is a Hero within each and all of us. I encourage us to reflect on community, compassion, love, and action employed from a sense of deep integrity and humanity. Together, through action, we can positively impact our own lives and the lives of others.
Sending a big shout out and endless gratitude to the Lake City homeless encampment!
To support this amazing Lake City (Seattle) community, check out the link below: https://lakecitypartners.org/
Thank you. Kat, Kathy and Gannon

Alanya Dalga Sörfü Eğitim Merkezi
Aug 8, 2016

