Laos, officially the Lao People’s Democratic Republic (LPDR), is a country in Mainland Southeast Asia, and the only landlocked country in Southeast Asia. It is bordered by Myanmar and China to the northwest, Vietnam to the east, Cambodia to the southeast, and Thailand to the west and southwest. Laos has a population of more than 6 million, and its capital and most populous city is Vientiane.
Health in Laos refers to the health of the population of Laos. Life expectancy in Laos was estimated at 67.78 years in 2021. Malnutrition, especially in children, is most prevalent in rural areas and among ethnic minorities. Poor sanitation, and tropical diseases including malaria are strains on the population’s health.
Lao health has improved in the period since Laos joined the World Health Organization in 1950: in addition to life expectancy increases, malaria deaths and tuberculosis prevalence have decreased and the maternal mortality ratio (MMR) has declined by 75%.
Healthcare in Laos is provided by both the private and public sectors.
Source:https://en.wikipedia.org/wiki/Health_in_Laos
- GLOBAL PRETERM BIRTH RATES – Loas
- Estimated # of preterm births: 10.4 per 100 live births
- (Global Average: 10.6)
- Source- https://worldpopulationreview.com/country-rankings/preterm-birth-rates-by-country

COMMUNITY
Public hospitals in Laos are working to achieve autonomy in a bid to improve service standards, reduce the number of people paying for medical services in other countries, and encourage VIP and private patients to make use of state-run facilities.
Minister of Health Ms Baikham Khattiya chaired a high-level meeting on February 13 with directors general from the ministry, directors of five central hospitals, and leading health officials from 10 provinces taking part in a pilot programme.
Mrs Baikham gave guidance on the reform process and spelled out three key goals: improving services for all patients, using resources more efficiently, and winning back VIP and private patients who typically seek treatment at private hospitals or overseas clinics.
Hospital autonomy allows management teams to make faster decisions on day-to-day operations and to allocate resources more effectively for diagnosis and treatment, so that hospitals can respond better to patient needs.
Starting in 2022, Mahosot, Mittaphab and Setthathirath hospitals have piloted the use of autonomy, while the Mother and Newborn Hospital, the Children’s Hospital and 10 provincial hospitals joined the programme last year.
The provincial hospitals taking part are in Bokeo, Oudomxay, Xayabouly, Xiengkhouang, Luang Prabang, Vientiane, Bolikhamxay, Khammuan, Savannakhet and Champasak.
The health minister urged hospital heads to lead staff in a patient-centred and quality-focused way, and to build trust among medical staff and patients.
Those in charge must be accountable role models and motivate their teams so that staff are inspired to improve services, she said.
Director General of the Department of Healthcare and Rehabilitation, Dr Khampasong Theppanya, reported on progress to date and outlined plans to further develop the legal framework around hospital autonomy.
Director General of the Department of Organisation and Personnel, Dr Bounserth Keopraseuth, said motivated personnel are essential and that hospital culture must shift towards greater self-responsibility.
Director General of the Department of Planning and Finance, Dr Viengmany Bounkham, highlighted the need for professional financial management and strong accountability and transparency.
A management expert with the Swiss Lao Hospital Project, Dr Alphons Schnyder, said public hospitals in Laos need to improve service standards so they are better placed to compete with private hospitals.
Skills in leadership, management, marketing, financial management, human resources management and change management must be strengthened to improve patient care, he added.
The Swiss Lao Hospital Project has supported the design and development of hospital autonomy since 2019, providing leadership and management training for hospital directors and key staff, and helping hospitals develop action plans.



Introduction: The design of Neonatal Intensive Care Units (NICUs) has significant implications for infant outcomes, parental well-being, and the delivery of family-centered care. Increasing evidence demonstrates that the physical environment of the NICU influences parental presence, participation in care, stress levels, and the development of parent–infant bonding (1-3). As such, NICU design should be understood not merely as an architectural or operational endeavor, but as a critical component of equitable, family-centered healthcare delivery. Centering family voices throughout the design process is essential to ensuring that NICU environments align with the lived realities, needs, and values of the families they serve.
Family Partnership Councils as Decision-Making Bodies: The formation of a NICU-specific Family Partnership Council (FPC) provides a structured mechanism for embedding family perspectives into NICU quality improvement and processes, including design governance. Such councils should include parents and family members who have experienced a NICU stay and who represent diverse backgrounds and lived experiences. They should reflect variation in race, ethnicity, language, socioeconomic status, family structure, and infant diagnoses and outcomes.
Importantly, Family Partners should participate directly in design meetings and decision-making processes, rather than serving solely in advisory or consultative roles. Equitable participation requires intentional preparation, inclusive meeting practices, and recognition of family expertise as complementary to clinical and technical knowledge. When families are positioned as equal stakeholders, design outcomes are more likely to reflect authentic family needs and promote shared ownership of the resulting space. This looks like adopting a framework like the NEC Society’s All In Meeting Guidelines, which aims to dismantle the hierarchy in healthcare and empower everyone to stakeholders, design outcomes are more likely to reflect authentic family needs and promote shared ownership of the resulting space. This looks like adopting a framework like the NEC Society’s All In Meeting Guidelines, which aims to dismantle the hierarchy in healthcare and empower everyone to contribute, by providing meeting materials in advance so Family Partners can adequately prepare and decode acronyms and other medical jargon contribute, by providing meeting materials in advance so Family Partners can adequately prepare and decode acronyms and other medical jargon.
Early and Continuous Family Engagement: Family engagement in NICU design should occur early and be sustained throughout the planning and implementation phases. Traditionally, families are consulted during late-stage feedback or evaluation periods, limiting their meaningful influence on core design decisions. Early involvement enables families to contribute to the establishment of guiding principles, identify priorities, and highlight unmet needs that may not be apparent to clinicians, administrators, or design professionals.
Ongoing engagement throughout the design process allows for iterative refinement and ensures that family perspectives remain integrated as budgets, timelines, and priorities evolve. This continuous approach positions families as partners rather than passive stakeholders, thereby strengthening alignment between design intent and real-world use.
Accessibility, Inclusivity, and Equity Considerations: Centering family voices in NICU design necessitates intentional inclusion of families from historically marginalized or underrepresented groups, including non-English language preference (NELP) families and parents with disabilities. Without deliberate outreach and accommodation, design processes risk privileging a narrow subset of experiences. Inclusive NICU environments should incorporate multilingual communication tools, universally accessible layouts, and design features that accommodate a range of physical, sensory, and cognitive needs. Soliciting feedback from parents navigating linguistic or cultural barriers and those with disabilities ensures that design decisions promote equity and reduce structural obstacles to participation in care.
Co-Design Through Participatory Methods:
Participatory co-design methods offer a practical way to translate family input into actionable design solutions. Focus groups, mock room walkthroughs, and simulated environments allow Family Partners to interact with proposed layouts and provide experiential feedback prior to construction.
These methods enable assessment of factors such as room configuration, lighting quality, acoustic conditions, ventilation, and the clarity of wayfinding and signage. Families often identify usability challenges that may not be evident in architectural plans, particularly under conditions of stress or fatigue. They may also identify accessibility challenges as it relates to recovery from childbirth, including considerations for parents recovering from traumatic births and/or cesarean sections. Incorporating iterative feedback through co-design processes enhances usability, reduces the likelihood of costly post-construction modifications, and promotes environments that better support family well-being.
Designing for the Daily Realities of NICU Families:
Family-centered NICU design must be grounded in an understanding of families’ daily lived experiences during prolonged hospitalizations. Parents in the NICU frequently assume caregiving responsibilities while managing physical exhaustion, emotional stress, and logistical challenges. Design strategies should therefore prioritize functionality, comfort, and proximity. Key design considerations include the availability of spaces that support parental rest, layouts that facilitate continuous proximity to the infant, and infrastructure that enables sustained participation in feeding and pumping. Attention to these elements acknowledges parents as integral members of the care team and supports their capacity to remain present and engaged.
Pumping spaces, in particular, should be intentionally designed to support frequent, sustained milk expression by locating them in proximity to the infant’s bedside whenever feasible. Proximity reduces physical and psychological barriers to pumping, minimizes time away from the infant, and supports parental presence and engagement in care. These spaces should provide visual and acoustic privacy, adequate and secure storage for personal belongings and expressed human milk, and immediate access to hygienic cleaning and handwashing facilities. Integrating pumping infrastructure inside patient rooms acknowledges lactation as a core component of neonatal care rather than an ancillary activity, and reinforces the role of parents as active participants in their infant’s treatment and development.
Transparency and Accountability in the Design Process: Transparent communication is essential to sustaining trust and meaningful engagement with Family Partners. Families who contribute to NICU design efforts should receive regular updates regarding design decisions and clear explanations of how their feedback has influenced outcomes.
When constraints limit the feasibility of certain recommendations, openly communicating the rationale for these decisions reinforces accountability and respect. Transparency transforms family engagement from a symbolic exercise into a substantive partnership and supports long-term collaboration beyond the design phase.
Northern European Approaches to Family-Centered NICU Design: Exploring design and care models implemented in other countries, particularly in Northern Europe, can further expand the possibilities for family-centered NICU environments. Many Northern European NICUs have long prioritized continuous parental presence, integrated caregiving roles, and physical designs that support parents as primary caregivers rather than visitors.
Examining these international approaches can help illuminate alternative spatial configurations, workflows, and cultural norms that may not be readily apparent within U.S.-based systems. Limitations are often assumed to be fixed when, in fact, they are products of historical design choices and institutional culture. Without intentional efforts to look beyond familiar models, stakeholders may envision only incremental improvements rather than transformative change. Incorporating international case studies and comparative learning into the design process encourages stakeholders to question entrenched assumptions, broaden their conceptual frameworks, and reimagine NICU environments from principles grounded in family needs rather than legacy constraints.
Conclusion: Centering family voices in NICU design represents a critical strategy for advancing family-centered, equitable neonatal care. Through early and continuous engagement, the establishment of Family Partnership Councils, participatory co-design methods, attention to daily lived realities, inclusive practices, transparent communication, and examination of international approaches, NICU environments can be intentionally aligned with the needs of families. Ultimately, NICU design that is informed by family expertise contributes not only to improved physical spaces but also to a broader culture of partnership, respect, and shared responsibility in neonatal care.
Source: https://neonatologytoday.net/newsletters/nt-may26.pdf



HEALTHCARE PARTNERS
Innovation in neonatal care often stalls in the “Valley of Death,” the treacherous gap between laboratory discovery and clinical application. Dr. Bernard Thébaud explains that while amphibians possess a “blastema” to regrow limbs, humans rely on mesenchymal stromal cells (MSCs) to orchestrate healing. Research indicates that umbilical cord derived MSCs and their extracellular vesicles (EVs) offer significant lung and neuroprotective benefits in animal models. To overcome the 30 year drought of new neonatal medications, Thébaud introduced “The Incubator,” a clinical accelerator strategy that integrates parent perspectives and animated educational tools to improve trial enrollment. Using single cell RNA sequencing, his team can now barcode individual cells to distinguish between therapeutic progenitors and ineffective fibroblasts, aiming to transform cell therapy into a precise, high tech biotechnology.



PREEMIE FAMILY PARTNERS





INNOVATIONS
Japan has long set the global standard for neonatal survival: between 80–90% of infants born at 22–24 weeks’ gestation survive to discharge, with an overall NEC rate below 2% in very low birth weight (VLBW) infants. (1) Yet survival is only the beginning. Japanese clinicians recognized that, even with this impressive clinical success, neurodevelopmental outcomes could be improved with better early growth. Achieving that required solving a nutritional dilemma in Japan.
Prior to a recent landmark regulatory decision, human milk-based fortifiers (HMBF) were not approved for use in Japan; only cow milk-based fortifiers (CMBF) were available. Concerns over the risks of CMBF in the smallest and most vulnerable infants led clinicians to routinely delay or avoid fortification, leaving those infants without adequate nutritional support during the most critical window of brain development. Now, for the first time anywhere in the world, HMBF has been designated as a prescription drug with Japan’s Ministry of Health, Labour and Welfare approving Prolacta Bioscience’s fortifiers for use in VLBW and post-surgical infants. It is a decision that has the potential to transform not just Japanese neonatal care but the global standard.
The Neurodevelopmental Stakes: The third trimester is the most dynamic period of neurological development in the entire human lifespan, one in which brain mass increases measurably week by week and approximately 250,000 neurons are formed every minute. For the very preterm infant, this extraordinary period of growth is happening outside the womb in the neonatal intensive care unit (NICU) with care teams managing the nutritional support that fuels it.
The consequences of nutritional deficits during this window extend far beyond the NICU. Inadequate early nutrition reduces brain cells, myelin production, and synaptic connections, and has been associated with lasting cognitive impairment. What we feed these infants in their first days and weeks of life can shape their long-term neurodevelopmental trajectory in ways that no intervention later in childhood can fully reverse.
Why Japan’s Fortification Practice Needed to Change:
Despite its exceptional survival rates, Japan’s standard nutritional approach carried a critical limitation. The prevailing practice often relied on withholding or delaying CMBF and formulas, known to carry risks of complications in premature infants. The recently published study on the Japan-led JASMINE trial describes the clinical reality plainly:
Notably, Japan is a world leader in survival rates of extremely preterm infants, with 80–90% of infants 22–24 weeks surviving to discharge in 2022, and an overall NEC rate of 2% in VLBW infants. Despite these excellent outcomes, there is not yet wide availability of human donor milk (DM) and a great hesitancy to feed and fortify infants with cow milk-based products early, often leading to poor growth outcomes in Japanese infants. The result was inadequate nutrition and growth during the precise developmental window when the brain needs it the most. Japanese neonatologists were, in effect, winning on one metric while potentially compromising on another.
The JASMINE Trial: A Phase III Answer:
The JASMINE trial, Growth and Safety Evaluation in Very Low Birth Weight Infants Receiving an Exclusive Human Milk Diet: A Phase III Randomized Control Trial in Japan, was conducted across 11 Japanese NICUs and randomized very low birth weight infants to either an exclusive human milk diet (EHMD) with human milk-based fortifiers added to mother’s own milk or donor milk, or the Standard Diet where CMBF or formula was delayed or avoided completely. Baseline characteristics were similar between groups, with a mean birth weight of 908.1 g in the EHMD group and 947.6 g in the standard diet group, and a mean gestational age of 27.05 weeks and 27.63 weeks, respectively. For clarity, findings are summarized from the per-protocol set (PPS; n=135), which included infants who remained on protocol through 34 weeks’ gestational age (EHMD n=66; standard diet n=69) without a major protocol violation.
The EHMD comprised three Prolacta products in the trial: Prolact+6 and Prolact+8, human milk-based fortifiers, and Prolact CR, a human milk-derived fat module added to mother’s own milk or donor human milk. Prolact CR played a central role in the protocol; approximately 95% of infants in the EHMD arm received it, providing concentrated nutrition without substantially increasing feeding volumes.
The JASMINE results were compelling. In the per-protocol set (PPS), the EHMD group demonstrated significantly greater weight gain velocity than infants in the Standard Diet group (14.30 vs. 11.96 g/kg/day, p <0.001). Standard Diet (0.85 vs. 0.66 cm/week, p≤0.0016), and infants in the EHMD group achieved full feeding volumes faster. Notably, the EHMD group spent fewer days on antibiotics compared to the Standard Diet group, a meaningful indicator of infection resilience in a context where sepsis remains the leading acquired cause of neonatal death in Japan. Although not statistically significant, head circumference growth was numerically improved in the human milk arm. Critically, these growth gains came without compromising safety. There was a single NEC case in the EHMD group, consistent with Japan’s low baseline NEC rates. Although randomized, the EHMD group included a higher proportion of infants born at 22–23 weeks’ gestation than the Standard Diet group, making the superior growth outcomes even more meaningful.
Human Milk Fat and the Developing Brain: For the preterm infant, fat is not simply a source of calories. The fat in human milk is uniquely structured to nourish the developing brain in ways that cow milk-based products cannot match. Human milk fat globules (MFGs) comprise approximately 98% of the fat in human milk and deliver 191 bioactive proteins, as well as long-chain polyunsaturated fatty acids, including DHA, which is critical for brain development. Premature infants miss approximately 80% of the DHA that would normally accumulate in the brain and tissues during the third trimester. (15) Prolact CR is composed of approximately 25% human milk fat and has been shown to increase weight and length velocity in VLBW infants significantly. A randomized trial of infants 750–1,250 g showed that infants who received human milk-derived cream had superior weight gain (14.0 vs. 12.4 g/kg/day, p=0.03) and superior length gain (1.03 vs. 0.83 cm/week, p=0.02) compared to those who did not receive it. Cow milk-based products cannot replicate this bioactive profile, as intact MFGs are largely absent from CMBF. Prolacta’s vat pasteurization process preserves MFG integrity, maintaining the structural and functional properties of these bioactive components in their native state. By contrast, processing methods such as homogenization and ultra-high-temperature (UHT) sterilization disrupt MFG membranes and additionally degrade key bioactive proteins. Immunoglobulins are reduced to nearly undetectable levels under UHT, and vascular/endothelial growth factor (VEGF), critical to gut and vascular development, is reduced by more than 60%. The human milk-based products also preserve a wide spectrum of human milk oligosaccharides (HMOs), the third-most-abundant component in human milk, which guide the development of beneficial gut bacteria and, emerging research suggests, may directly influence neurodevelopmental processes in early brain development.
The Long View: Neurodevelopmental Outcomes Beyond the NICU: The JASMINE trial had a clear goal: to optimize early growth in the most vulnerable preterm infants to support better neurodevelopmental outcomes potentially. Evidence from EHMD use in other settings underscores the long-term benefits.
A 2025 multicenter study by Chou and colleagues across 13 Kaiser Permanente Southern California NICUs involving more than 1,000 infants found that an EHMD was associated with 26% lower odds of motor skill delays at age 3, compared with infants fed cow milk-based products, despite EHMD infants being born approximately three weeks earlier and weighing more than 300 g less at birth. Hair and colleagues reported that infants fed an EHMD had significantly higher cognitive scores and a trend toward improved language scores at 18–22 months corrected age compared to those fed cow milk-based diets.
A Landmark Decision with Global Implications:
Japan’s prescription drug designation for Prolacta’s human milk-based fortifiers is not simply a regulatory milestone; it is a clinical statement grounded in rigorous Phase III evidence that early fortification with an EHMD is achievable, beneficial, and safe for VLBW infants. For NICUs globally, this approval sets a powerful precedent that the evidence is strong enough and the safety profile clear enough that all NICUs should be using human milk-based products to fortify the enteral feeds of very preterm infants, not just to help premature infants survive but to help them thrive in the long term.
Source: https://neonatologytoday.net/newsletters/nt-jun26.pdf
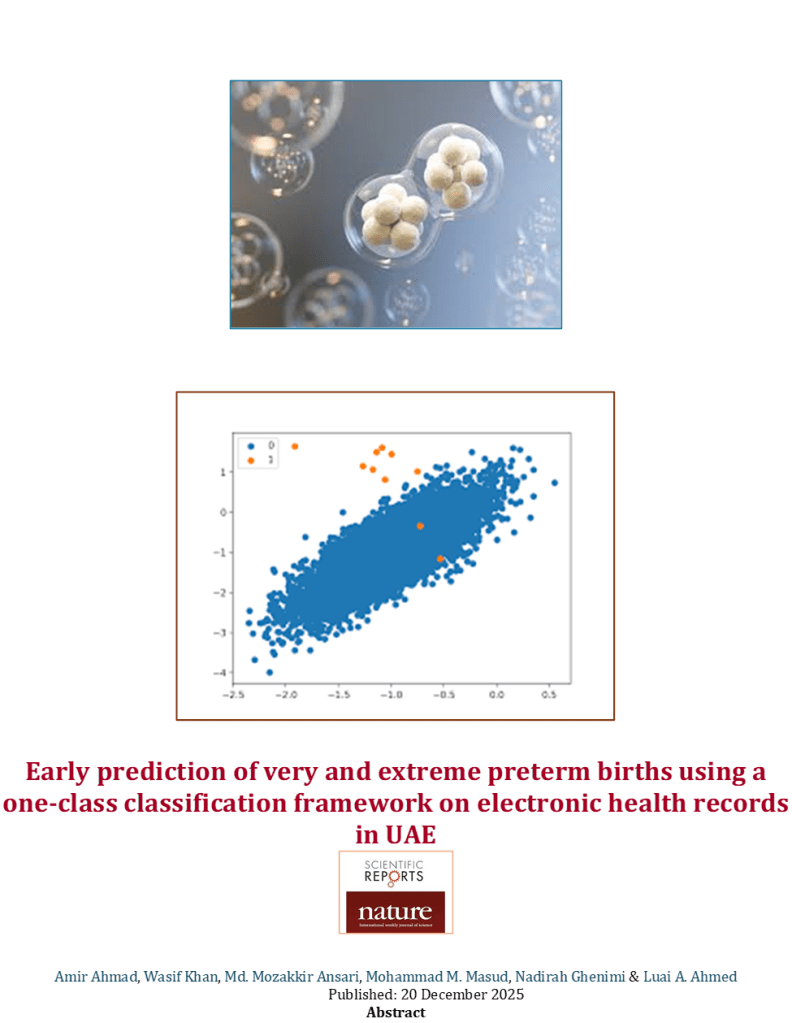
Very Preterm birth (vPTB) and extreme Preterm birth (xPTB) are the major concerns in maternal and child healthcare and are associated with increased morbidity and mortality. Machine learning methods have traditionally been used to predict preterm births (vPTB and xPTB). However, most medical datasets, including preterm births, are imbalanced in class distribution. Although data-balancing techniques can be employed, complications due to the limited sample size of the minority class are frequently encountered, leading to inconsistent results. This study adopted a novel approach by employing one-class classification (OCC) in conjunction with several strategies to predict instances of vPTB and xPTB within an Emirati pregnant population. We used a well-curated dataset acquired during the first trimester of pregnancy. We employed multiple OCC algorithms and their ensembles involving multiple aggregation strategies to predict vPTB and xPTB in both parous and nulliparous populations. Our approach effectively incorporated only majority class information during training. Our detailed experimental setup demonstrated that the proposed methodology achieved promising performance with a maximum AUC-ROC of 0.823 for the parous population without any explicit modeling of the minority class. Our approach demonstrated robustness and efficacy in identifying at-risk pregnancies within the Emirati population. Our results suggest that one-class classification framework which requires only normal data points for training can be used for early prediction of very preterm and extreme preterm births with reasonable accuracy. In this paper, we applied one-class classification framework only on the Emirati population. Generalizing the proposed approach in this domain requires experimentation on similar datasets from other countries.
Source:https://www.nature.com/articles/s41598-025-29219-4
Abstract
Background
In the neonatal intensive care unit (NICU), premature neonates frequently endure painful procedures that can lead to long-lasting sequelae, underscoring the critical need for safe and effective pain management strategies. Auricular massage has demonstrated significant benefits for children, including anxiety and stress relief. Investigating its effectiveness in alleviating pain in neonates could introduce a valuable nonpharmacological approach to pain management, enhancing the overall care and comfort of these vulnerable infants.
Objective
This research is aimed at studying the effectiveness of a 3-min session of auricular massage in reducing pain caused by nasal and oral suctioning among premature neonates in the NICU in Jordan.
Methods
A randomized controlled trial employing a single-blind crossover design was conducted in a single hospital. Preterm neonates were randomly assigned to one of two conditions. In Condition I, neonates initially received auricular massage treatment after suctioning, followed, after 2 days, by no massage after suctioning. Conversely, in Condition II, neonates had the reversed sequence, starting with no massage and then receiving auricular massage treatment after 2 days. Pain levels in the neonates were assessed using the Premature Infant Pain Profile-Revised (PIPP-R) scale.
Results
Data from 60 preterm neonates were analyzed using the SPSS Version 28. Chi-square and independent t-tests revealed no significant differences between neonates in the study conditions based on gender (p = 0.43), gestational age (p = 0.41), and body weight (p = 0.35). Paired t-test results indicated a significant difference in pain scores when comparing periods of auricular massage to periods without massage. The mean pain score following auricular massage was 3.63 (SD = 2.36), whereas it was 10.23 (SD = 2.40) in the absence of massage.
Conclusion
Auricular massage for a 3-min duration is an effective nursing intervention that warrants consideration as a nonpharmacological method of pain relief for premature neonates during admission to the NICU.
Source:https://pmc.ncbi.nlm.nih.gov/articles/PMC12520807
Neonatal Womb Warriors for a Healthier World
To everyone reading this who started life early: this one is for you. For many of us, the beginning of our story was not only a medical event, but an environmental one. Research increasingly links extreme heat, wildfire smoke, and fine particulate air pollution with higher rates of preterm birth. For some families in this community, the air outside the hospital window may have helped shape what happened inside it. That truth is heavy, but it also gives neonatal womb warriors a powerful place in the fight for cleaner air, safer pregnancies, and healthier futures.
The NICU that saved so many of us is one of the greatest examples of human skill, science, technology, and love working together. Monitors, isolettes, tubing, ventilators, medications, and specialized teams ran day and night to give fragile, early life a chance. Because we know what that care means, we also know why the future of neonatal care matters. Green NICU initiatives are beginning to show how hospitals can reduce waste, conserve energy, and limit unnecessary plastic while protecting the lifesaving care that babies and families depend on.
The science keeps getting clearer: heat waves, air pollution, fine particulate matter, and ozone are associated with increased risks of early delivery, low birth weight, and other complications. Families living near heavy traffic, industry, wildfire smoke, or poor air quality often carry the highest burden. Climate and air quality are not side issues for the neonatal community. They shape pregnancy, birth, survival, and long-term health.
That is why neonatal womb warriors have such an important voice. Supporting clean air policy is preemie advocacy. Pushing for climate-resilient hospitals is preemie advocacy. Reducing unnecessary healthcare waste is preemie advocacy. Protecting pregnant people and newborns from environmental harm is preemie advocacy. This is the same fight, carried further upstream, toward a world where fewer babies have to begin life fighting so hard.
So let this be a small flag planted for every preemie survivor, NICU graduate, parent at the bedside, clinician in the unit, and tiny warrior who did not make it home. The world that shaped our beginning is worth protecting. Bring your reusable water bottle, support policies that clean the air, ask your hospital about sustainability, and talk about this connection with people who may never have considered it before. You were a warrior before you ever drew an unassisted breath, and now that strength can help build cleaner air, stronger hospitals, safer births, and a healthier world for the next generation of tiny fighters.