El Salvador, officially the Republic of El Salvador, is a country in Central America. It is bordered on the northeast by Honduras, on the northwest by Guatemala, and on the south by the Pacific Ocean. El Salvador’s capital and largest city is San Salvador. El Salvador’s population in 2024 was estimated to be 6 million.
The economy of El Salvador has historically been dominated by agriculture, beginning with the Spanish taking control of the indigenous cacao crop in the 16th century, with production centred in Izalco, along with balsam from the ranges of La Libertad and Ahuachapán. This was followed by a boom in use of the indigo plant in the 19th century, mainly for its use as a dye. Thereafter the focus shifted to coffee, which by the early 20th century accounted for 90% of export earnings. El Salvador has since reduced its dependence on coffee and embarked on diversifying its economy by opening up trade and financial links and expanding the manufacturing sector. The colón, the currency of El Salvador since 1892, was replaced by the United States dollar in 2001. As of 2019, Salvadoran economics gifted them the lowest level of income inequality out of nearby countries. Among 77 countries included in a 2021 study, El Salvador had one of the least complex economies for doing business.
The Human Rights Measurement Initiativefinds that El Salvador is fulfilling 89.6% of what it should be fulfilling for the right to health based on its level of income. When looking at the right to health with respect to children, El Salvador achieves 98.3% of what is expected based on its current income. In regards to the right to health amongst the adult population, the country achieves only 82.9% of what is expected based on the nation’s level of income. El Salvador falls into the “fair” category when evaluating the right to reproductive health because the nation is fulfilling 87.6% of what the nation is expected to achieve based on the resources (income) it has available.
There are now 30 public hospitals in El Salvador, plus various primary care facilities and 27 basic health care systems. Before 2009 a “voluntary” donation was demanded to access a public hospital or clinic. Clinics staffed by Community Health Teams have been established in the rural areas. Although services are supposed to be a free, a shortage of funds means that people may have to pay for supplies Emergency services are very basic. The private health sector offers care in medical facilities concentrated in urban areas.
Leadership by the head nurse/unit manager in facilitating the implementation of Infant and Family Centered Care (IFCDC) is often unrecognized. The key role of the head nurse/unit manager in promoting IFCDC and creating a NIDCAP Training Center within the neonatal intensive care unit at the University Hospital of Ghent, Belgium, serves as an example of significant practice change. Instead of taking a theoretical model of change as a starting point, concrete personal experiences and roles that are incorporated into daily practice are described. The aim is to provide insight into how leadership, entrepreneurship, and connection significantly contribute to successful implementation, and to inspire managers facing similar processes.
A description of the evolution of the role of the head nurse from clinical expert to an inspiring, facilitating, and strategic manager includes grounding in clinical skills that lead to an understanding of the necessity of implementing IFCDC. Expansion of the leadership role includes believing in one’s own team, actively giving employees opportunities to build and share expertise, and developing a culture of shared leadership and evidence-based working. The use of care consultants, working groups, and internal study days strengthened both expertise and team solidarity.
A focus on the importance of the head nurse’s entrepreneurial leadership complements clinical expertise and team leadership. Despite budgetary pressure, gaining insight into financial flows, using workload measurement tools, and developing an appropriate financing model enabled continued investment in training and innovation. Strategic alignment with the hospital’s mission, vision, and quality models increased support among senior management.
The head nurse’s role in connecting and communicating is highlighted as crucial for sustainable change management. Transparent communication, multidisciplinary involvement, and attention to pitfalls and concerns proved essential to embed IFCDC and NIDCAP principles into daily healthcare practice and create a shared sense of ownership and pride.
Background When preparing and developing a large project, such as a startup, any practice change involving developmentally supportive, family-centered care can be framed with objectives, project plans drawn, and theoretical frameworks developed from the literature. However, the role of the head nurse/unit manager does not include managing theoretical change processes; rather, it involves using concrete examples to demonstrate how implementation can work in a particular NICU. The theory can be used, often post hoc, to get insight into why a project is or is not implemented in practice.
The intent of the description of the head nurse’s/unit manager’s development and resulting role is to provide a narrative of what worked. The descriptions and strategies included are intended as inspiration for those facing similar implementation projects.
Knowledge background of the nurse manager
In the past, the ‘better nurses’ often rose to managerial positions. The person who was the most handy and who had the most clinical knowledge was often appointed as head nurse. However, it has become increasingly clear that the role has expanded to include many other competencies.
Inspirational role of a nurse manager
As a head nurse, it is first and foremost important to believe in the strength of your own team. Your own employees should be given maximum opportunities to develop their expertise, and in turn, they should share it within the team. A manager primarily facilitates nurses’ growth, embraces the knowledge they develop, and ensures it is shared with colleagues.
In the Ghent NICU, work is conducted across many domains (ventilation, breastfeeding, pain, transport, skin and wound care, resuscitation, developmental care, vascular topics, etc.). The head nurse/unit manager, recognizing the importance of work groups that address clinical care, grants a part-time exemption for a nursing consultant in each care domain. Their role is to follow and document the work group processes and provide training to colleagues, intra- and extramural. The resulting work on the specific care domains is supported not only by the nursing consultant but also by several team ambassadors. In this way, multiple contact persons for various topics are created, and opportunities are offered to different team members. Recognition of evidence-based, high-performance care then spreads within the broader organization.
Every two years, a symposium for nurses and midwives is developed and offered with significant support from the head nurse/unit manager. These educational programs provide a connection and collaboration towards a common goal within the various care domains of neonatal care. It is a moment to ‘shine’ as a team and to share the evidence we have acquired with others. This ‘study day’ can be seen as an example of the department’s dynamic culture, which pursues clinical excellence.
As a unit manager, inspiring is essential to education. For example, looking for relevant topics together and cross-pollinating ideas with each work group is an example of how to provide inspiration. Additionally, providing inspiration is essential for stimulating employee growth on your team. It is an opportunity both to optimize care quality and for nurses individually to grow and rise above themselves. If a manager is not afraid to step outside of their comfort zone, it can lower the threshold for employees to do the same.
Entrepreneurial and innovative role of the nurse manager
Inspiring and facilitating staff are important, but achieving financial freedom and earning the trust of senior management are necessary. In a context where resources are increasingly scarce and priorities are increasingly focused on direct business results, the role of a head nurse/unit manager as an entrepreneur and innovator is not an obvious choice. However, it is essential to the success of any initiative.
Financing as an entrepreneurial skill.
Financial autonomy to generate and control income is a key component of the entrepreneurial role of the head nurse/unit manager. To realize this new cultural shift in how a head nurse/unit manager’s role is perceived, an individualized, well-thought-out financial plan that generates income (e.g., by organizing symposia and offering training to external partners) is essential. In turn, generating income makes it possible, for example, to send colleagues to international conferences and training courses. It is therefore also the task of a head nurse, as the department’s budget holder, to identify, see, and take advantage of financial opportunities.
It is important to have insight into the NICU’s financial flows relative to the entire organization. Very often, people complain about deficiencies, which is nothing new and is probably a sore point in every organization. A head nurse/unit manager should try to get a handle on the income and expenses of their department. Demonstrating financial control often ensures that senior management has the confidence to start working with the NICU entrepreneurially. For example, the Ghent NICU, together with the other Flemish NICUs, successfully validated a neonatal measurement instrument and used it to document nurses’ workload on a daily basis (WANNNT). The outcome data, along with income from fees and historical hospitalization data for our service, enabled us to predict our unit’s budget. Working solely with post-factum data means the head nurse/unit manager is less able to respond quickly to a rapidly evolving context.
Innovation as an entrepreneurial skill.
An important aspect of the entrepreneurial role is innovation. Head nurses are expected to actively explore innovative solutions and consider opportunities to optimize patient care. Undoubtedly, these opportunities present themselves in every organization.
Neonatal care has undergone many developments in recent decades. NIDCAP and IFCDC are receiving increasing attention. It leads, among other things, to better neonatal outcomes, shorter length of stay, fewer complications, and less stress for parents. Sharing the most recent literature on this subject with the hospital’s management and higher management while also emphasizing the financial benefits to the hospital can help free up budgets more easily.
Implementing NIDCAP and IFCDC comes with a significant price tag. When hospitals are under financial pressure, they often quickly reduce non-primary assignments, including training. It is important to demonstrate that the investment in developmental care is profitable in the long term, not only through patient and family outcomes but also by showing the sustainability of quality of care and staff retention. In addition to having self-acquired resources to continue investing in your team’s education and training, it ensures a successful start to greater innovation in implementing NIDCAP training and IFCDC standards of care.
Policy implementation role of the nurse manager
Within the hospital, the mission and vision are periodically adjusted. The individual units and services are asked to align their departmental objectives with the hospital’s policy. Keywords of the Ghent University Hospital policy are excellent—daring, people oriented, and efficient. It does not take much imagination to see that the core IFCDC and NIDCAP values are reflected in these key words in hospital policies. The head nurse/unit manager of the NICU must translate the link between the hospital and the developmental care values using concrete examples from clinical practice and present it to the hospital’s higher management.
Each hospital also works around and with an international quality model. The NICU at University Hospital Ghent also strives to meet, as far as possible, the highest standards set by the European Standards of Neonatal Care. Working with 2 different models is not always efficient. As a service, embedding the Neonatal Standards of Care is done as much as possible within the various care domains with the hospital’s quality model as the goal. On the one hand, this ensures working on quality in a broad sense, as expected by the hospital, and avoiding ‘quality fatigue’ by working with parallel models. It is also an opportunity to demonstrate in practice how to translate the hospital’s keywords and the organization’s central vision into our daily policies.
Connecting the role of the nurse manager
The head nurse serves as a connector within change management, linking vision and practice. In a care context that is constantly evolving, the head nurse helps translate changes into reality for the nursing team. This translation is best made in collaboration with stakeholders from the developmental care team, in concrete terms. The multidisciplinary working group on development-oriented care includes NIDCAP professionals who serve as guides. In this way, a bottom-up culture of co-ownership for important projects is cultivated.
Clear and empathetic communication is essential here. A space for dialogue is created; active listening to questions and concerns is employed; and assurance is provided that employees feel heard and involved.
In this way, a team-oriented culture, in which cooperation and interprofessional respect are central, is promoted. In the past, NIDCAP and a developmental care emphasis were often seen as the work of a small number of passionate nurses. A multidisciplinary approach, in which doctors, psychologists and, for example, care consultants are closely involved, provides much more support for this process and increases the likelihood of success.
Finally, the head nurse/unit manager acts as a role model in the change process. By showing a willingness to change, flexibility, and a constructive attitude, you give the team direction and trust. In this way, the head nurse not only becomes an initiator of change but also a catalyst that connects and strengthens people to achieve these sustainable improvements together.
Communicative role of the nurse manager
The head nurse also plays a central role in communicating key changes. This role goes beyond merely passing on information; it includes actively connecting people, their expectations, and their goals. A head nurse is at the crossroads between the nursing team, the medical staff, and senior management, ensuring that those three worlds are anchored together.
Within the team, creating clarity and trust is a priority, and open communication is crucial. In addition, a culture of dialogue is emphasized in which team members, together, are encouraged to help shape the policy on developmental care. Congruence in thinking and acting is essential here. The manager must ensure that the team’s vision translates into daily operations in direct patient care: in other words, “make sure that you DO what you SAY”.
At the same time, the head nurse is an important communication partner with senior management. Frequent, open, and honest feedback to management about the current state of the change process creates a long-term atmosphere of trust between management and the team. In doing so, the possibility of identifying any additional needs (e.g., additional staff needs) is embedded. SAYING what you DO is therefore not an empty illusion here.
To achieve this, it is also an undeniable asset if senior management wants to delve into the content of the developmental and family centered care project to a certain extent. The presence of a board member during a feedback session with the Ghent NICU staff made it easier to continue the discussion. In this way, co-ownership of the change project is supported at the higher management level.
As in any organization, organizational change sometimes occurs at the senior management level. Every change and new situation should be proactively used to invite new board members to share the unit’s vision and to explain projects within the long-term vision of both the organization and the unit. This approach can ensure that a lot of additional context information is less necessary for specific and/or new questions related to the project.
Pitfalls
Does everything always go perfectly? Not at all. Not everyone is immediately open to change: why would anyone suddenly change something that they have been doing in a certain way for 20 years? Familiar questions are • “Is there sufficient evidence for changes to this protocol?” • “Do all those adjustments cost too much money?” • “Is that profitable?” communication is crucial. In addition, a culture of dialogue is emphasized in which team members, together, are encouraged to help shape the policy on developmental care. Congruence in thinking and acting is essential here. The manager must ensure that the team’s vision translates into daily operations in direct patient care: in other words, “make sure that you DO what you SAY”. At the same time, the head nurse is an important communication partner with senior management. Frequent, open, and honest feedback to management about the current state of the change process creates a long-term atmosphere of trust between management and the team. In doing so, the possibility of identifying any additional needs (e.g., additional staff needs) is embedded. SAYING what you DO is therefore not an empty illusion here. To achieve this, it is also an undeniable asset if senior management wants to delve into the content of the developmental and family centered care project to a certain extent. The presence of a board member during a feedback session with the Ghent NICU staff made it easier to continue the discussion. In this way, co-ownership of the change project is supported at the higher management level. As in any organization, organizational change sometimes occurs at the senior management level. Every change and new situation should be proactively used to invite new board members to share the unit’s vision and to explain projects within the long-term vision of both the organization and the unit. This approach can ensure that a lot of additional context information is less necessary for specific and/or new questions related to the project. Pitfalls Does everything always go perfectly? Not at all. Not everyone is immediately open to change: why would anyone suddenly change something that they have been doing in a certain way for 20 years? Familiar questions are • “Is there sufficient evidence for changes to this protocol?” • “Do all those adjustments cost too much money?” • “Is that profitable?” • “Is that really a priority now?” • “Are we not shifting the focus too much to education and training, to project work, which jeopardizes our clinical work in direct patient care?” • “As a care provider, will I still be able to take my holidays with all those different assignments?”
Thus, we can continue with similar questions for a while.
These are all recognizable concerns in departmental change processes—concerns that can and will come from both the team and senior management and concerns to which head nurses cannot always give an immediate, satisfactory answer. Nevertheless, it is important to stick to basic ideas and evidence, asking the question: “Why and for whom are we doing all this?” which will often help with forward movement. It will be important to stay transparent with the team—even during personal uncertainties— show vulnerability, and, above all, continue to ensure a safe climate in which employees can share their concerns. Working step by step so that the effort remains manageable for everyone and not forgetting to celebrate the team’s successes when reaching milestones are essential to avoiding missteps. In this way, it creates a joint sense of pride with the developmental and family-centered care implementation story, in which even the care for each other as care providers within the team must continue to receive necessary attention.
Summary
Successful implementation of a complex and intensive change process, such as the start-up of a NICU-wide infant- and family centered developmental care program and a NIDCAP Training Center, is not merely the result of a theoretically based project plan but above all of thoughtful and committed leadership in practice. The role of a head nurse/unit manager in this effort is multifaceted: entrepreneurial, innovative, inspiring, facilitating, strategic, connecting, and communicative.
By starting with trust in the team’s expertise and growth opportunities, a culture is created that centralizes shared leadership, multidisciplinary collaboration, and evidence-based care. Consciously investing in training, stimulating internal nursing consultancy, and making expertise visible within and outside the department not only strengthens the quality of care but also increases employee involvement and pride. Entrepreneurial leadership within a healthcare context that is increasingly under financial pressure appears to work. Insight into budgets, the use of financial opportunities, and the substantiation of investments with both clinical and economic arguments have proven necessary to make such a change process possible.
Sustainable change can only succeed if it is strategically embedded in the broader mission, vision, and quality structures of the organization. Alignment with hospital-wide policy objectives increased support and prevented fragmentation or ‘quality fatigue.’ Crucial here is the head nurse’s role as a link between the unit and the hospital’s management, where transparent communication strengthens trust on both sides.
Finally, the change process is inevitably accompanied by uncertainties, resistance, and pitfalls. By leaving room for concerns, working step by step, and celebrating successes, a safe learning climate can be created in which change is not experienced as a threat but, hopefully, as joint growth. In this way, the head nurse not only becomes a manager of change but also a driving force behind sustainable, people-oriented care.
New parents Nicole and Joe welcomed identical twins Ava and Amelie, who were born premature at just 26 weeks at Birmingham Women’s Hospital, and were cared for on the Neonatal Intensive Care Unit (NICU) for over 11 weeks before they were well enough to go home.
Nicole, who lived in Lichfield at the time, was seen at the hospital’s Fetal Medicine Department when they noticed at her 16-week scan one of the twins was growing significantly smaller than the other.
She recalled: “It was my first pregnancy, and we found out we were having twins at six weeks and the pregnancy was going smoothly.
“They noticed at a scan one of the twins was growing significantly smaller, so we were referred to the Fetal Medicine team.”
The Fetal Medicine department discovered the twins had Selective Intrauterine Growth Restriction ( sIUGR ), a condition that can occur in identical twin pregnancies where one twin is growth restricted due to an absent or reversed flow from the umbilical cord.
Nicole added: “We’d never heard of the condition before, and it was really scary knowing something was potentially wrong.
“It was all due to where they’d ended up connecting to the placenta. The bigger twin was plugged in at a larger part so was getting plenty of nutrition, but the smaller twin was plugged into the tail end of the placenta, meaning she wasn’t getting enough nutrition and was so much smaller.
“We didn’t know what this would mean for them, but everyone was so kind and reassuring and explained things in a way we could understand.”
Nicole was scanned twice a week to closely monitor the smaller twin’s growth, until Nicole was 26 weeks pregnant and was admitted overnight for daily monitoring.
She said: “Her heart rate kept dropping low on the monitor, and we were starting to get concerned and thinking about having to deliver them early.
“It kept dropping and taking longer to come back up, and one of the consultants who looked after us said that it was time for them to come out now.
Ava and Amelie arrived prematurely at 26 weeks and 4 days, weighing just 2.2 and 1.9 pounds.
Nicole said: “I was able to see both girls after they were born before they went straight down to the NICU, where they were both intubated for 24 hours before progressing onto oxygen.
“Joe went down with them, and once I’d recovered, they took me to see them, and they looked so tiny and fragile.
“Amelie, the smaller twin, kept getting blood in her feeding tube, so had to be nil by mouth due to the risk of infection. She had a much harder ride to start with, but she kept fighting.”
Both twins started to get stronger with the help of oxygen and feeding tubes, however, when Ava was six weeks old, she developed Necrotising Enterocolitis (NEC) which, an infection which can affect premature babies and is a condition where the bowel becomes inflamed and damaged.
Nicole recalled: “Something hadn’t been quite right with her tummy the day before, but then we got a phone call at home to say she’d taken a turn for the worse.
“It was horrible hearing the phone ring in the middle of the night knowing it was probably about the girls, but knowing we weren’t with them.
“They were both so strong and were real fighters all the way throughout.”
During their stay at the NICU, Nicole and Joe visited every day, arriving first thing in the morning and staying until last thing at night. They also received counselling on the unit and were part of the family group that had been set up for parents to share their journey.
Nicole commented: “Nothing can prepare you for a stay on the NICU.
“While we were there, we lived in our own little bubble and we didn’t talk to family or friends much because it was hard to explain how it feels, and you don’t know what’s going to happen next.
“The team were really supportive, and they helped us be as hands-on as possible with their care, and the family group was really helpful too. It was nice to be able to talk to other parents who knew how it felt and were going through the exact same thing too.
“Walking away from your babies every night was just horrible, so to finally leave with them was a huge relief.
“When we went home, they both still had a feeding tube, but the team were brilliant in giving us training so we could do it ourselves at home. Both tubes ended up being removed the next day as they were doing so well breastfeeding.”
The twins are now over two years old and are thriving at home after their difficult start to life.
Nicole added: “They’ve got such different personalities now, but they’re both very cheeky little girls.
“Ava especially loves animals and trips to the farm, and they both love singing and dancing around the house.
“They both absolutely adore their younger sister and they’re so gentle and kind with her.
“We’re so thankful for everyone at the Women’s Hospital for looking after our girls, they’re both so strong and such fighters and we couldn’t be prouder of how far they’ve come already.
“Shireen Meher looked after us from our time in fetal medicine all the way to the delivery, and she was had such a positive impact on our journey.”
The neonatal intensive care unit (NICU) relies on a multidisciplinary team of advanced practice providers (APPs), including neonatal nurse practitioners (NNPs) and physician assistants. With the Accreditation Council for Graduate Medical Education residency rotation reductions taking effect in July 2025, the demand for NNPs to fill clinical coverage gaps will increase. Anticipated changes in federal reimbursement and Medicaid services and National Institutes of Health pose financial challenges for Children’s Hospitals.
Evidence Acquisition:
This review examines the current state of the NICU APP workforce with special emphasis on NNPs, including historical trends, educational requirements, and the impact of regulatory changes. Data were gathered from surveys completed by national professional organizations, published literature in PubMed, and expert communication.
Results:
Despite their critical role and increased demand, APPs including NNPs face challenges, such as burnout, staffing deficits, reimbursement, and a decline in the number of NNP graduates by 20% since 2022. Neonatal nurse practitioner recruitment is hindered by the lengthy onboarding process and high costs. The integration of physician assistants, hospitalists, and non-NNPs as possible solutions to fill the NNP shortage gap presents challenges, such as lack of training opportunities and managing patients outside their scope of practice.
Implications for Practice and Research:
Addressing workforce shortage requires strategies, including tuition-supported programs, recruiting registered nurses to become NNPs, developing mentorship programs, and increasing NNP preceptors. Further research is needed to evaluate the effectiveness of these strategies and to explore additional solutions for sustaining the NNP workforce.
Introducing Preemies Hub: A New Global Resource for Preemie Families, Built with You in Mind
For every preemie warrior and every parent who has stood beside an incubator, the journey into the NICU often begins without warning. It can feel overwhelming—filled with medical language, uncertainty, and the urgent need to make sense of what is happening to your baby. In those moments, access to clear, trustworthy, and relatable information is not just helpful—it is essential. That is why we are so excited to introduce Preemies Hub, an innovative new platform developed in partnership with Our Kids Health, designed to support families navigating the realities of premature birth.
Preemies Hub was created with a deep understanding that not all families experience the NICU in the same way. For many, challenges are compounded by language barriers, cultural differences, and limited access to reliable, evidence-based information. This platform addresses those gaps by providing translated, adapted, and culturally responsive health information specifically designed for parents across equity-deserving communities. Every piece of content has been developed with respect for different values, beliefs, and ways of communicating—ensuring that families can not only access information, but truly connect with it.
So why does this matter? Because caring for a premature baby is already one of the most emotionally and physically demanding experiences a family can face. Misconceptions about prematurity, lack of preparation for an unexpected early delivery, and difficulty navigating medical information can make that journey even harder. Preemies Hub helps change that. It empowers parents with knowledge they can trust, presented in a way that is clear, compassionate, and accessible—so families can feel more confident, informed, and supported in advocating for their child.
The platform offers a wide range of topics relevant to the NICU journey and beyond, along with resources available in multiple languages including Punjabi, Ukrainian, Tamil, Spanish, Mandarin, Inuktitut, Cantonese, Filipino, Arabic, and more. It also intentionally centers diverse communities, including Black families, ensuring that representation and inclusivity are not afterthoughts—but foundational to the resource itself. For providers, this means having a trusted tool to share with families. For parents, it means finally seeing information that reflects your language, your culture, and your experience.
At Neonatal Womb Warriors, we believe that every family deserves access to information that meets them where they are. Preemies Hub is more than just a resource—it is a step toward equity in neonatal care, a bridge between knowledge and community, and a reminder that no preemie journey should be navigated alone. 💙
The quality of health in Cambodia is rising along with its growing economy. The public health care system has a high priority from the Cambodian government and with international help and assistance, Cambodia has seen some major and continuous improvements in the health profile of its population since the 1980s, with a steadily rising life expectancy.
A health reform of Cambodia in the 1990s, successfully improved the health of the population in Cambodia, placing Cambodia on a track to achieve the Millennium Development Goal targets set forth by the United Nations. One such example is the Cambodian Health Equity Fund, largely financed by the country itself, created in 2000 to increase access to free health care to around 3 million poor people. The Fund, which pays for traveling expense and even daily allowance for anyone accompanying a patient, has resulted in increasing health care seeking among Cambodians who otherwise could not afford any kind of medical care. As a result of the reform, mortality rates significantly dropped. Similarly, life expectancy at birth in 2010 was 62.5 years, a 1.6 folds increase from 1980.
GLOBAL PRETERM BIRTH RATES – Cambodia
Estimated # of preterm births: 10.5 per 100 live births
Cambodia’s sustained progress in improving maternal, newborn and child health
20 February 2025
At the beginning of the 2000’s, Cambodia faced alarming maternal, newborn and child health indicators. The maternal mortality ratio stood at 437 per 100 000 live births, while newborn and child mortality rate accounted for 37 and 124 per 1000 live births respectively. Limited infrastructure, a shortage of skilled birth attendants and financial constraints hindered progress. To tackle these challenges, the Cambodian government, with support from WHO and key partners, embarked on a transformative journey to strengthen maternal and newborn health services and ensure equitable access to quality care.
Today, skilled birth attendance is near universal, with 98.7% of births attended by trained health professionals and 97.5% of women giving birth in a health facility. Between 2014 and 2021-2022, neonatal and under-five mortality rates declined by 54%, from 18 to 8 and from 35 to 16 per 1000 live births respectively, far exceeding the global average reduction of 14% during 2015-2022. Cambodia achieved its Sustainable Development Goal targets for reducing neonatal and under-five mortality eight years ahead of schedule.
Strengthening health systems
Cambodia’s investments in health systems and workforce capacity have been instrumental in driving progress. Midwifery training programmes have equipped health workers with essential skills to provide safe, high-quality care, including routine antenatal care, essential intrapartum care, postnatal care, and management of childbirth complications. Deployment strategies have ensured that even remote health centres are staffed with skilled birth attendants.
To incentivize facility-based deliveries, the government introduced a delivery incentive programme for health teams in 2007 and launched cash transfer programmes for pregnant women and infants from poor families in 2019, targeting the critical first 1000 days of life. These initiatives encourage families to seek comprehensive antenatal and postnatal care, ensuring access to a full package of essential health services. Financial mechanisms such as health equity funds, cash transfers and fee exemptions have alleviated economic barriers, making institutional care more accessible to vulnerable populations.
Improvements in water, sanitation and hygiene infrastructure have also contributed significantly to better health outcomes. An integrated routine primary health care delivery system has been established across provinces and districts, ensuring that essential services effectively reach communities. Health promotion and behaviour change campaigns have played a vital role in encouraging exclusive breastfeeding and antenatal care-seeking behaviours.
Strong leadership and strategic framework
A key milestone in Cambodia’s progress has been the strong leadership of the Ministry of Health, which has provided clear strategies for advancing maternal and newborn health. Two main coordination platforms — the Sub-Technical Working Group for Maternal and Child Health and the Early Essential Newborn Care (EENC) Coordination Committee — were established and have convened regularly to align efforts within the Ministry and with health partners.
With technical support from WHO and funding from the Korea Foundation for International Healthcare (KOFIH), the EENC Coordination Committee plays a crucial role in harmonizing national and sub-national efforts, monitoring progress through regular reviews, mobilizing resources to scale up EENC practices, and ensuring consistency in care delivery while addressing service gaps.
Recognizing the need for a strategic and systematic approach to newborn care, the committee led the development and adoption of the Five-Year Action Plan for Newborn Care (2016–2020). The plan emphasizes scaling up EENC and institutionalizing evidence-based practices, integrating key life-saving and cost-effective interventions — such as routine immediate care for all newborns under “The First Embrace” approach, as well as measures to prevent and care for small or sick newborns.
By 2023, EENC coaching was implemented in 89.4% of health facilities (1187 out of 1328), surpassing the 80% target. Kangaroo Mother Care for preterm and low birthweight infants has been scaled up to two national hospitals and ten provincial and district referral hospitals, while a national protocol for EENC in Caesarean sections, introduced in 2019, has standardized care nationwide.
“Maternal, newborn and child health are essential components of investing in human capital. Providing quality care for mothers and newborns brings immense benefits — not just for families, but for entire communities and economies. Cambodia’s coordinated approach to maternal and child health serves as an inspiring model for the region and globally. It demonstrates what can be achieved with strong national leadership, dedicated health workers and sustained partnerships,”stated Dr Marianna Trias, WHO Representative to Cambodia.
Remaining challenges
Despite significant achievements and high coverage of antenatal care and facility-based deliveries by trained health personnel, challenges persist. While maternal mortality has declined, it remains high at 154 deaths per 100 000 live births, primarily due to haemorrhage and pregnancy-induced hypertension — both preventable causes. Greater efforts are needed to get on track to achieve the 2030 target of 70 deaths per 100 000 live births. Similarly, child malnutrition continues to impact long-term productivity, with 22% of children under five stunted and 10% wasted for over a decade.
Disparities between urban and rural areas and gaps in facility capacity to provide quality essential services require targeted attention. Addressing unmet family planning needs and expanding adolescent-friendly services are crucial, particularly as rural adolescent girls aged 15–19 experience significantly higher birth rates than their urban peers.
The way forward
Moving forward, further reducing maternal and neonatal mortality requires a stronger focus on enhancing the quality of care. Building on significant improvements in coverage, efforts should prioritize improving the quality of basic routine care during antenatal and intrapartum periods, including emergency obstetric care, alongside establishing robust referral systems for cases requiring higher-level care. Achieving this will require both the strengthening of quality improvement mechanisms with enhanced monitoring and the implementation of targeted improvement actions.
The Fast-Track Initiative Roadmap for the Reduction of Maternal and Newborn Mortality (2025–2030) aims to accelerate progress by scaling up interventions, sustaining quality care and addressing service delivery gaps. To support its implementation, WHO will assist in developing a comprehensive country action plan and support the Coordination Committee for Strengthening Quality of Care and Wellbeing of Women, Maternal, Newborn and Child Health to ensure effective coordination and execution.
Bringing clean water to where life begins: a neonatologist’s story from Ukraine
12 June 2025
These are the words of Galina Dmytrova, a neonatologist at Chuhuiv Central Hospital in the Kharkiv region of Ukraine. To her patients, the support Galina and her colleagues provide make a difference between life and death.
“They are already under enormous stress because of the war and now we are facing water shortages again. Before the war, you’d turn on the tap and not think twice. But now, under daily shelling, the electricity goes out, and with it, the water too,” says Galina.
5 water stations set up across Kharkiv city and the wider region in Ukraine continue to allow hospitals to provide essential care despite the war. Among them is Chuhuiv Central Hospital. The stations were installed in 2025 by WHO with funding from the European Union and in partnership with Ukraine’s Ministry of Health.
For communities regularly affected by attacks that disrupt electricity and water supply, this support ensures access to clean, safe water for both patients and health workers, which is critical in maternity wards, where hygiene and continuity of care are vital.
“In our hospital, thanks to WHO and the European Commission, we now have a water treatment system. I’m deeply grateful. It’s hard to explain the importance – especially for mothers and their babies. Many people actually can’t believe women are still giving birth under such harsh conditions. But they are, and I truly admire them,” Galina adds.
Those are our babies
In 2024, some 179 children were born in the Chuhuiv Central Hospital in the Kharkiv region. This year, the birth rate is similar; in the first 3 months of 2025, hospital staff oversaw more than 45 births.
“That’s our maternity ward, our babies, around 15 every month – even while the war goes on,” Galina tells us.
The certainty and assurance that care is available, that there is a hospital nearby, gives people hope. A functioning hospital is a reminder that life goes on. The opposite is also true; when health facilities are damaged or attacked in conflict, it not only deprives communities of access to health care. It also deprives them of hope.
“When the war started, I was new to Chuhuiv. I didn’t know the area that well. One night, a woman in labour came very late and explained they’d been looking for a boat. The bridge to her village had been destroyed – so, to get here, they had to cross the river. But they did it, because they knew here was a hospital that could help,” says Galina.
Fortifying our commitment to pediatric academic medicine during turbulent times
Academic Medicine, with its tripartite mission to advance medical science, cultivate the next generation of healthcare professionals, and provide exceptional clinical care, offers unparalleled opportunities to shape the future of evidence-based healthcare delivery and inform health policy. Biomedical innovation developed through collaboration between academic medicine and public health can improve health at the individual and population health levels including mapping disease trends and improving treatment outcomes. According to the Association of American Medical Colleges (AAMC) economic impact report published in 2022, every one dollar spent by the AAMC member medical schools and teaching hospitals contributes $1.62 to the United States economy. Unfortunately, medical schools and teaching hospitals continue to face reductions in government funding for research and education support and have faced decades of under-reimbursement for publicly insured care, often delivered in these systems which also serve as safety net health care systems across the country.
The National Institutes of Health (NIH) revealed that the nation’s supply of physicians engaging in research continues to decline, with increased competition for decreasing available federal funding. Pediatric research is disproportionately impacted by gaps in funding, directly impacting the scientific innovation aimed at improving child health outcomes. As advanced technology such as artificial intelligence (AI) balanced with rapidly evolving scientific discoveries offer novel and dynamic clinical approaches to care, these persistent funding gaps often lead to pediatric care falling behind adult care delivery. With an estimated 646,000 researchers supported by federal grants, 48% of whom are students and trainees, the cross-cutting dependence and impact of federal funding on research and education is undeniable. Therefore, to mitigate further impact in pediatric academic medicine, continued promotion of NIH-funded pediatric research must leverage the understanding that return on the investment continues over the lifespan of the growing child to adult.
In the article by Arnaez and colleagues, Dr. Garcia-Alix is celebrated for his longitudinal contributions and global reach in academic medicine, specifically in field of Neonatal Neurology. By understanding that at least 30% of neonates admitted to Neonatal Intensive Care Units (NICUs) present with neurological pathology or other conditions impacting brain development, he recognized the importance of studying neuroprotective factors that impact these children’s morbidity. For Dr. Garcia-Alix, this area of interest sparked a career long passion. His dedication was evident, while advancing and supporting academic education and mentorship of his learners, generously investing time and role modeling for further generations. With the appreciation of the life-course model for his neuro-neonatal patients, Dr. Garcia-Alix, translated the overarching goal of improvement of functional outcomes by creating Brain-Aware Care, a family-centered, multidisciplinary approach targeting protecting an infant’s developing brain at the earliest stages. He recognized and appreciated that neuro-neonatal care delivery differs requires a comprehensive, multidisciplinary, family-centered approach tracking continuity of care as a baby grows, as is the continued research to understand how to develop appropriate care guidelines and protocols for developing, growing and thriving children. Dr. Garcia-Alix dedication and contributions as a physician scientist and educator with global impact on generations of patients in the field Neonatal Neurology is a testament of the longitudinal investment and support required to achieve the return on investment in child health outcomes in pediatric academic medicine.
Fiscal pressure on the future of pediatric academic medicine
The goal of pediatric academic medicine is to continue to develop and support clinician scientists like Dr. Garcia-Alix throughout their careers, who are committed to innovation, clinical care, and education. However, the fiscal pressure on pediatric academic medicine for the past several years, balancing under-reimbursed Medicaid clinical activity, rising labor costs, inadequate availability of pediatric extramural funding, and insufficient graduate medical education funding, is leaving teaching hospitals and partnered medical schools to find novel ways to advance this pediatric academic mission. Institutional-level investment in clinician scientists (e.g., 3 year contracts where early career faculty have time to successfully compete for a career development grant) are less feasible as financial pressure mount from funds flow models in Children’s Hospitals. Similarly, competition for institutional (e.g., KL2) and external (e.g., K23) grants are increasing as paylines are decreasing. With recent changes in administration policy, opportunities for first-generation scientists and those underrepresented in biomedical research (e.g., diversity supplements, MOSAIC award) are now unavailable. Protecting NIH funding, particularly money appropriated to child health research, is essential to promote the mission of pediatric academic medicine. Moreover, given diminishing availability of federal extramural funding, reviewing alternative, non-traditional academic sources of funding mechanisms for research including private industry, venture capital or foundation funding will be necessary to explore to uphold the tripartite mission of our pediatric academic mission.
In addition to research challenges, pediatric residency training programs are in jeopardy. Since the annual budget for graduate medical education is supported through the Congressional appropriations processes, strategic consideration of alternative platforms of support for retention, learner mentorship, and workforce pipelines are critical to ensure continued access to care for our pediatric population. Mentors can be instrumental at different stages of learners, from guiding students in explicit academic knowledge, to implicit knowledge of professionalism, ethics and the art of medicine.9 Retention of faculty is critical during times of economic stressors in academic medicine and leaning on mentorship and sponsorship as a key strategy, especially given pay inequity between pediatric and adult academic clinicians. Finally, evaluation of the economics of health professions education (HPE), is critical with ongoing cost-constrained academic medicine environments, especially with graduate medical education funding at risk.
Call to action for the health of our nation’s children
We need to reinforce and double-down on our commitment to the pediatric academic medicine mission-centered goal in improving the health and well-being our children and youth through investments in advancing science, cultivating our next generation of pediatric learners and improving clinical care for our pediatric patients. With several decades of Medicaid under-reimbursement, challenging degradation of federal pediatric extramural funding compared with adult funding, and even greater disparities in pediatric workforce shortages, families are facing a stark reality in worsening access to pediatric healthcare which will only grow in the upcoming years due to Medicaid cuts. We must continue to educate legislators and government officials that children require the same level of extramural funding (if not greater), in efforts to evolve even greater investment on return investment over the life-course trajectory. We must advocate for reimbursement parity greater than Medicare, especially understanding the discrepancy between Medicaid enrollment and Medicaid expenditure on children, being roughly 50% and 20%, respectively. Finally, we must educate that pediatric academic medicine, with its medical schools and teaching hospitals, contribute to the economy and health of the United States.
Call to action
Support the Bipartisan Legislation H.R. 3890 (Sewell, Fitpatrick)- Resident Physician Shortage Reduction Act of 2025- Educate your local legislators on the importance of Pediatric Education workforce pipeline and its’ impact on access to care, especially in rural communities
Continuing to unequivocally advocate for Children’s Hospitals Graduate Medical Education (CHGME), and budget appropriation within the annual Labor Health and Human Services Appropriations Process for the House and Senate Committees
Support NIH funding increases for Pediatric Research funding, which will increase and parity (and increase) for pediatric extramural funding for research to improve the evidence-based decision-making, and uphold trust with patients, families and society
Continue to educate our legislators about the life-course model in child health, and the return on investment, with the reality that for every $1 investing in early intervention, there is a return on investment from $1.26 to $17.07 for every child invested in the United States.
Finally, ensure that with the rapid advancing in technology, including artificial intelligence (AI), gaps do not arise regarding access to therapeutic tools between pediatric and adult populations in healthcare.
Background: Perinatal loss is a profoundly complex form of grief, often linked to heightened risk of prolonged bereavement and adverse mental health outcomes. Perinatal grief rooms-private, supportive spaces within healthcare settings-aim to help families process their loss, spend time with their baby, and create meaningful memories in a respectful environment. While bereavement care has received growing attention, the role of the physical environment in supporting grief remains underexplored.
Objective: To synthesize current evidence on how dedicated physical spaces can support individuals and families after perinatal loss, and to identify priorities for research, design standards, and interdisciplinary collaboration.
Methods: A narrative review was conducted in accordance with PRISMA-ScR guidelines. Literature searches were performed across PubMed, PsycINFO, Medline (OVID), Embase, ScienceDirect, SCOPUS, SciELO, and Google Scholar using terms, such as “perinatal grief rooms”, “bereavement rooms”, “angel suites”, “butterfly suites”, “snowdrop suites”, “cloud rooms”, “designated units for perinatal loss”, and “birthing + bereavement suites”. The review examined (1) the current role of physical spaces in the perinatal loss experience, and (2) how their availability and design may influence grief outcomes.
Results: Of the 17 articles meeting inclusion criteria, only 4 (24%) referenced bereavement rooms, and just 3 (18%) noted the need for formal protocols-without offering concrete examples. No studies evaluated implementation, design standards, or measurable impact on grief, mental health, or family well-being. This lack of empirical evidence and standardized guidance underscores a critical gap that limits integration of therapeutic environments into perinatal bereavement care.
Conclusion: Despite increasing recognition of the importance of bereavement care, dedicated grief rooms remain under-researched and inconsistently implemented. Advancing this field will require rigorously designed studies, development of design standards, and collaborative partnerships among healthcare providers, researchers, policymakers, and design experts to ensure equitable access to therapeutic spaces for grieving families.
Harnessing the power of a multidisciplinary team carries vast potential for effectiveness and problem-solving—while achieving high-performance with diversely skilled stakeholders requires adroit management.
The Center for Innovative Leadership (CIL) exists to support and accelerate the production of new research on leadership in today’s dynamic, complex organizations and bring research to life through engaging student experiences and powerful industry partnerships.
Summary: In healthcare it is common practice for multidisciplinary teams to be involved in efforts to improve the quality and safety of patient care. The perioperative period, which encompasses the time before, during, and after a surgical operation, is a prime target for multidisciplinary improvement efforts because of the diversity of professional roles and care delivery settings involved. Failure to achieve improvement targets in this context is often attributed to lack of resources or resistance to change.
A recent study counters this view, suggesting failure is more likely to be due to the way the multidisciplinary improvement team is led and how well it collaborates. Successful improvement projects depend on effective leadership—from designing the team, communicating a shared vision, planning the project, through to creating a collaborative approach to getting work done, and a structured training and feedback process.
A new study distils existing literature and gathers expert opinions on leadership and high-performing teams to offer practical guidance on those factors and behaviors relevant to the delivery of perioperative improvement projects, but also to leading multidisciplinary teams outside of healthcare.
High-performing healthcare services continually seek to improve patient experience and outcomes. One key area of focus for improved performance has been the perioperative period—the time leading up to, during, and after surgery. Unfortunately, perioperative improvement teams often fail to achieve their goals and when this happens the blame is often ascribed to resistance to change or lack of resources.
A recent study highlights that another important – yet overlooked – reason why t improvement projects fail is because of the way multidisciplinary improvement teams are designed, how they are led, and how the multidisciplinary teamwork is managed.
The study, from Christina Yuan and Michael Rosen, Faculty Affiliates at the Center for Innovative Leadership at Johns Hopkins Carey Business School, in collaboration with Tasnuva Liu, Benjamin Eidman, Della M. Lin, and Elizabeth Wick, contends that taking time to pre-plan and continually reflect on how team leadership behaviors are enacted is the best way to ensure team success—yet this is often overlooked.
The researchers surveyed a range of thought leaders and team leaders with deep-rooted experience in perioperative work to discover the leadership behaviors and practices considered to be most relevant to planning and implementing perioperative improvement initiatives.
Based on their findings the researchers recommend the following six key areas leaders should consider when designing and leading teams to deliver perioperative improvement projects—recommendations that carry implications for the management of multidisciplinary and cross-functional teams in a wider context too:
Design and Define
It is important to clearly define the aims of the mission, and to choose a team that includes all stakeholders and the right mix of skills and roles—allowing flexibility and ensuring that roles are not too rigidly defined. It is also wise to include those who are skeptical about improvements, as well as those who are more receptive, so as to understand the scope of the challenge ahead and ideally to bring skeptics on board.
Manage
Leaders should create an environment where collaboration is prioritized and fine-tuned. Through discussion, establish effective processes for getting work done and delegating tasks. With agreement leaders should identify challenging but realistic goals for the team. They should monitor and report on progress and help the team recover from any small set-backs.
Sustain
An environment of psychological safety should be created, where team members feel they have a voice and their opinions are acknowledged. Leaders should communicate regularly to everyone to show how the project is progressing and to build a collective understanding of what is being achieved and what more might be done. This should be framed as a positive way to learn from successes and failures as opposed to seeking compliance.
Train and Feedback
Listening, asking good questions, and soliciting feedback are essential leadership behaviors. In a multidisciplinary team it is important everyone participates and is heard, including less vocal team members. This interaction can be the basis for providing skills training and promoting continuous learning—appreciating that failures can be opportunities for learning.
Manage Team Boundaries
It is a leader’s role to clarify the boundaries between the core project team and other groups and departments, as well as to be a liaison with these entities. It is vital to obtain senior leadership buy-in at the outset of the project and to maintain this throughout with regular reporting on progress, successes, and any potential barriers. Messages should be brief and individualized to address each senior leader’s particular concerns.
Manage Organizational Context
Aligning the team’s efforts with organizational needs is key. Here an important factor is for senior leaders to ensure access to data the team needs to make decisions and do their work. Removing barriers to data sources and providing the team with opportunities to ask senior leaders questions and get information as needed is also the leader’s responsibility.
In a busy healthcare setting, where the delivery of a perioperative improvement project will be one of many priorities for the members of the assigned multidisciplinary team, above all team leadership must be clear and precise. It must ensure all members of the team understand their roles, feel free to participate fully, and are empowered to achieve to the best of their abilities. There are innumerable management theories and practices that might be suggested to accomplish this.
The value of Yuan and Rosen’s study is that it helps to distil the essence of what is really required for effective team leadership in this context.
Recent research provides new insights into significant brain and behavioral changes in the baby’s first six months after birth, laying a foundation for later physical, cognitive, and social development. Preparation in utero leads to infant behavioral responses that ensure survival, and the caregiving environment provides safety and protection during these early months. Brain development accelerates, and regulation of biophysiology is demonstrated in respiratory, cardiovascular, and gastrointestinal systems, as well as in behavior.
Newborns and young infants often exhibit behaviors that signal caregivers to provide protective and nurturing responses. Caregivers, usually the baby’s parents, typically respond to the baby’s signaling. Mutual reinforcement of behavior leads to the dyad becoming adapted and regulated in early infancy. Mismatches in the baby’s explicit behavioral signaling and/or challenges in the caregiver’s reading and/or responding to the baby’s behavior in these early formative months can affect later social, emotional, and cognitive development.
Signaling behavior:
Signaling behaviors such as crying, vocalizations, alertness, and face scanning prompt interaction with others. Crying signals distress and is likely to promote immediate caregiver response. Facial expressions, such as smiling, brow knitting, and pouting, often elicit an emotional response from the baby’s caregiver. The resulting dyadic exchanges promote ongoing social interaction. As brain development proceeds at a rapid pace, the transition from reflexive to volitional behaviors typically occurs around 2-4 months. These more intentional behaviors lead to more sophisticated behavioral repertoires and social bids.
The responsive caregiving environment and mutual interaction between caregivers and their baby during this time contribute to the development of increasingly regulated behavior. Caregivers of newborn and very young infants need support to understand babies’ available signaling behaviors, as these behaviors have a significant impact not only on early caregiving relationships but also on brain development.
Signaling behavior of hospitalized babies:
Early-born or sick newborns are at a disadvantage in the development of signaling behavior. Their experience as a fetus and during delivery can interfere with the development of or overwhelm effective behavioral communication. Early-born babies have not had experiences during the last weeks of their fetal life that contribute to more organized behavioral responses. Their reflexes may be weak or hard to elicit, arousal and visual regard may be limited, and physiologic instability may affect responsiveness. Necessary medical support may also overwhelm their meager energy and/or fail to recognize their efforts to signal.
In addition to early birth and/or medical concerns, the caregiving environment in intensive care is vastly different from the “expected” one for a more typically developing baby and can thus affect foundational brain and behavioral development. It is well known that long-term effects on brain development, social/emotional, and cognitive development in babies hospitalized at birth are recognized as less than optimal. Early birth, medical issues, and hospitalization can interfere not only with a baby’s ability to provide clear signals but also with caregivers’ ability to interpret them.
Intensive care professionals are typically trained in medical assessment and intervention, which until recently have not included behavioral assessment. Berry Brazelton was a pediatrician who took the lead in understanding the behavioral repertoire of newborn babies. Heidelise Als, one of his protégés, extended that understanding to babies born early. She developed the Newborn Individualized Developmental Care and Assessment Program (NIDCAP) and emphasized observing and interpreting babies’ behavior. Based on those assessments, caregiving recommendations are developed to help the baby achieve regulated behavior and thus achieve their own developmental goals. Since her early work, most NICUs now incorporate identification of at least some behavioral signals and implement strategies to support babies’ development.
IFCDC standards provide a foundation for supporting signaling behavior:
At the center of the IFCDC standards concept model is an emphasis on the baby as an interactor in their relationship with their primary caregiver, typically the mother. Woven into each of the other principles is the understanding that the baby influences how they are cared for both by family members and by intensive care professionals. The model implies that the baby’s individualized interaction with the environment of care influences their physical, social, emotional, and cognitive development.
Each of the six evidence-based areas of developmental care emphasizes the importance of understanding the baby’s behavioral communication to fashion an individualized approach to their caregiving experience. Additionally, each of the six areas includes an emphasis on supporting the baby’s primary caregivers, typically the parents, to observe, interpret, and respond to the baby’s behavioral signals. Early-born and medically fragile babies’ signals can be challenging to interpret. Professional staff must have a thorough understanding of the baby’s signaling behavior to provide individualized caregiving and support parents in knowing how best to care for their baby.
The continuum after discharge:
The continuum after discharge: Leaving intensive care marks a transition into early infancy and involves a multitude of brain and behavioral changes. During these foundational months, rapid brain development is reflected in significant behavioral changes. As noted above, reflexes become modified into volitional events, and signaling behaviors become dependent on the baby’s environment of care. As the medically fragile or early-born baby becomes more physiologically and behaviorally regulated, their signaling becomes more socially responsive.
The primary caregiver, on the other hand, may still be affected by the intensive care experience and be hesitant to interact with their previously fragile baby vigorously. It is postulated that as the baby becomes clearer in their communication, more intentional, and ready to interact, the parent can be less responsive to their bids.
Although targeted interventions for caregivers in their early relationships with their baby begin in the NICU, they must be continued after discharge, as behavioral changes in the first months are rapid, and it is often difficult to understand how best to respond.
Caregivers’ understanding of their baby’s signaling behavior as it changes over time must be supported and reinforced by knowledgeable professionals for at least the first six months of the baby’s corrected age, and sometimes longer, depending on the baby’s adaptation during this period. As brain and behavior, as well as parenting skills, are still developing, individualized dyadic care should be provided early and frequently after discharge and should continue for at least six months.
Conclusion:
The continuum of brain and behavior development from the fetal to the newborn to the early infancy period evolves in the context of the baby’s environment of care. The behavior the baby uses to signal their need for caregiving changes dramatically over the first six months, and caregiving responses that regulate the baby’s behavior lay the foundation for later physical, cognitive, and social emotional development. Babies born preterm or medically fragile are typically less effective in their signaling behavior. Due to the altered environment in which they develop and the myriad factors that influence their parents’ responsiveness to their behavior, they and their parents need supportive measures to assess, interpret, and provide support for early development. The current IFCDC standards incorporate supportive strategies into both the concept model and the evidence-based practice areas. Because brain and behavior are particularly vulnerable during the first six months, there is a need not only to understand and respond to their behavior in intensive care but also to continue this understanding and response after discharge for at least the first six months.
Breastfeeding a premature baby requires special care, patience, and close monitoring—especially during the transition from tube or bottle feeding to the breast. In this hospital-based guide, a healthcare professional demonstrates how to safely breastfeed a growing preterm infant while ensuring adequate milk intake.
This video explains how pre- and post-feeding weight checks are used to accurately measure how much milk a premature baby consumes. You’ll learn correct breastfeeding positions, how to maintain proper body alignment, and how to achieve a deep, effective latch. The guide also helps parents distinguish between nutritive sucking and comfort sucking, recognize early signs of fatigue or stress, and follow essential safety protocols such as monitoring breathing patterns and proper burping techniques.
Ideal for parents of premature babies and NICU families, this video supports confident, safe breastfeeding during a critical stage of infant development.
INNOVATIONS
“In the 1960s, when the first NICUs opened, premature infants had a 95% chance of dying. Today, they have a 95% chance of survival” – Dr. Rahul K. Parikh, a pediatrician from California, published in August 2012 in the New York Times . This incredible shift in survival can be considered a great example of the conquest of modern neonatal medicine. Among many technological advancements, the ability to continuously monitor vital signs such as heart rate and respiratory rate, was followed by closed loop body temperature (T) control, blood pressure assessment, and finally by continuous and non-invasive monitoring of oxygen saturation. Monitoring of these vital signs was paramount for the assessment of well-being and detection of pathophysiological states in tiny patients, allowing for adjustments or initiation of treatments or interventions that are lifesaving.
There is no question that neonatal technology has advanced tremendously over the last 60 years and parents have become very approving of this. In the book From Surviving to Thriving, Fabiana Bacchini, the mother of a twin baby boy born at 27 weeks, wrote: “I was able to watch in happiness and gratitude, all the technology that exists to keep these tiny beings alive.” Later, it also became clear that, despite the important role of technology, it can also cause fear and anxiety for parents. Fabiana mentioned that the first time she entered the NICU “I did not see a baby, I saw wires, monitors and a breathing machine” .
Indeed, current technology for vital signs monitoring uses several skin sensors connected to the bedside monitors by wires and cables. In most patients, raw signals, average values and trends of heart rate, respiratory rate, temperature, and oxygen saturation are continuously displayed. However, this system carries some challenges for patients, parents, and healthcare professionals (HCP) as the multiple wires can tangle around the infant body, restrict the patient’s movement, and cause discomfort or pressure sore. Hence, regular care involves frequent removal, reapplication, and readjustments of the sensors, which may harm the fragile neonatal skin, cause pain, and/or interrupt resting or sleeping. For parents, not much information is available on what are their perspectives on these vital signs monitoring systems. Some small surveys have reported that the presence of multiple wires and cables can cause intimidation and additional stress, acting as a barrier to skin-to-skin contact for fear of disconnecting the sensors or wires, or interfering with regular monitoring . This technology may also increase HCP’s workload as wires and cables may touch contaminated surfaces or become soiled with urine, blood or stools, increasing the risks of nosocomial infections. Consequently, nurses must constantly inspect, sanitize, reposition, or replace components of the system.
Is a Wireless NICU Possible?
Neonatal intensive care units manage a diversity of health problems with variable degrees of severity and patient maturation. To develop a wireless system that can be used during the first days of life in a 400 g extremely preterm infant born at 22–23 weeks of gestation and a 4-kilo term infant born with perinatal asphyxia is a real challenge. Furthermore, there are some more stable infants that are just feeding and growing, or infants with chronic problems that require prolonged hospitalizations. Noticeably, the needs of these populations are different, creating challenges for the development of new vital signs monitoring systems. As an example, an extremely preterm infant in the first days of life spends most of the time quiet, sleeping inside the incubator, and has very sensitive skin that can easily be damaged by skin adhesives and sensors. In these cases, non-contact technologies may play a very important role, at least for the monitoring of heart rate and respiratory rate. This is not the case with more stable and mature infants that are active, and where parents can constantly hold and promote kangaroo care (KC). Therefore, the adoption of new monitoring technologies needs to consider those different needs, be very familiar with the technology advantages and limitations, and develop protocols and proper training for all healthcare providers involved.
Is a Wireless NICU Desirable?
Although wired vital sign monitors are the standard, they are frequently cited as obstacles to key aspects of family-integrated care and routine clinical practice. Wireless vital sign monitoring technologies are increasingly being explored as a potential solution to these issues. However, there is limited research available which quantitatively or qualitatively examines how key NICU stakeholders such as parents and HCPs, perceive the current monitoring system and these wireless innovations.
The small number of existing studies have highlighted that the wires and sensors used in current systems interfere with skin-to-skin contact and KC, limit parents’ ability to hold or touch their infants, and contribute to a highly technical environment that many find overwhelming. Survey and interview studies consistently show that parents perceive the wires as intimidating and as contributing to their anxiety . HCPs also express widespread concerns with the current systems, especially regarding the physical clutter created by wires, challenges with positioning and handling of infants, risk of pressure sores from adhesives, and the frequency of false alarms .
These concerns have led to growing interest in wireless monitoring as a possible solution. While research on parent and HCP in this area is very limited, all existing studies show optimism toward the adoption of wireless technology. Parents have generally responded positively, citing benefits such as reduced anxiety, possible easier interaction with their infant, improved KC, and enhanced infant comfort. However, there are some apprehensions related to signal reliability, sensor size and appearance, battery duration, and potential risks such as radiation exposure . Similarly, HCPs have voiced strong support for wireless monitoring, highlighting its potential to reduce handling difficulties, decrease false alarms, and improve comfort for both infants and families . Importantly, they also emphasize areas of concern, including reliability, safety related to radiation, and costs . In particular, the absence of economic feasibility studies is a significant gap in the current literature.
Overall, the available evidence indicates that wireless monitoring is a promising advancement, with support from key stakeholder groups in the NICU. The shift away from wired systems could improve key aspects of neonatal care, particularly KC and parental engagement, while also addressing some of the frustrations voiced by HCPs. However, to address these challenges, and ensure new technologies will be adopted by NICU staff and parents, concerns around reliability, safety, and cost must be addressed through careful user-centered design, and rigorous research including clinical evaluation. Future research should prioritize that wireless systems not only meet regulatory and clinical standards but are also feasible and acceptable for daily use in the NICU.
What Wireless Technology for Neonatal Vital Signs Monitoring Is Available or Emerging?
Non-Contact
A large number of small studies have investigated the use of non-contact vital sign monitoring in the NICU. Most studies used a single-device system and monitored respiratory or heart rate using offline analysis. The following technologies have been tested: red, green, blue cameras, infrared cameras, monochrome cameras, depth cameras, and radar, primarily for respiratory rate and heart rate monitoring . Non-contact sensors are typically placed at the head or foot of the infant’s incubator or crib. In some cases, the sensor cannot collect data through the plexiglass and may require either an open incubator or a small opening to maintain a clear line of sight. Depending on the technology and algorithms used, a defined Region of Interest within the sensor’s visual field may be designated for vital sign extraction.
These studies generally featured small sample sizes and short recording durations of <1 h . Nearly all exclusively focused on accuracy by comparing novel non-contact methods to a reference measurement using the Bland-Altman method. Analyses of heart rate and respiratory rate using this method revealed low bias and moderately acceptable 95% limits of agreement. Feasibility outcomes were rarely explored and measured using metrics such as the amount of usable data or processing times. No studies explored outcomes related to safety, although this can be expected as these monitoring methods pose no threat to the fragile neonatal skin.
While these technologies show promising preliminary results, several concerns remain. First, feasibility concerns remain as most devices rely on an uninterrupted clear view of the infant. How it would perform in situations where the infant is moving, clothed, or receiving care needs to be better clarified. Additionally, a systematic review of non-contact technologies applied the QUADAS-2 assessment and revealed several areas of concerns regarding risk of bias and applicability due to lack of clear inclusion and exclusion criteria and small sample sizes . Furthermore, many studies lacked key basic descriptors of the population, such as age and weight, making it difficult to ensure a representative range of NICU patients such as those requiring respiratory support or in incubators were included in the research. Additionally, some studies provided incomplete descriptions of reference measurements, only naming them as “standard” or “routine” monitoring, limiting the ability to determine the risk of bias. Unfortunately, most non-contact studies lack a conflict-of interest statement.
Ultimately, non-contact technologies may represent an appealing monitoring solution for some of the most vulnerable infants in the NICU, such as extremely premature infants with extremely fragile skin. This research area is rapidly growing as non-contact studies often utilize commercially available cameras and present low research risks for patients. However, concerns regarding the ability to perform reliably for prolonged periods in a real NICU environment and across a range of patients require further exploration and validation.
Wireless Wearables
Studies focusing on wearable devices provide slightly more detailed information regarding participant selection criteria and larger sample sizes. Emerging classes of wireless sensors in the form of soft, flexible, skin-like (“epidermal”) platforms have the potential to redefine practices for monitoring in the NICU, with additional possibilities for use in the home. Recent work at Northwestern University shows that a pair of devices of this type, each of which gently and non-invasively adheres to the fragile skin of a premature neonate, is capable of capturing complete, clinical grade vital signs information without any wires or cables . These devices include distributed flexible electronic components with stretchable interconnects; all embedded in strategic layouts within medical-grade silicone encapsulating structures. The designs optimize for conformal interfaces to the skin at relevant anatomical locations. In pilot studies on patients in NICU settings, these technologies achieved high accuracy and fidelity similar to those of traditional wired monitors. Extensions enabled by additional sensors allow for precise measurements of body sounds, relevant to cardiac and respiratory monitoring, with additional capabilities in tracking gastrointestinal activity . Specifically, high-bandwidth microphones and accelerometers yield seismocardiograms, lung sounds, bowel motility, and even the spectral and temporal features of crying and other forms of vocalization. In this way, these advanced technologies can not only capture vital signs and physiological signals but also an array of important biophysical metrics of health status, beyond those addressed with conventional NICU hardware.
Commercial translation is also gaining momentum. As an example, Sibel Health (Sibel Health, USA) has secured successive FDA 510(k) clearances since 2021 for its ANNE® One sensor platform, a pair of chest and foot patches to continuously monitor heart rate, respiratory rate, skin and core temperatures, oxygen saturation and biomarkers. It is also noteworthy that ANNE One® is currently under investigation in NICU at Montreal Children’s Hospital with the aim of create a wireless NICU. Meanwhile, other emerging technologies, focusing on more specific modalities, include Bambi Belt (Bambi Medical, the Netherlands) and Boppli® (PyrAmes, USA) for monitoring ECG/EMG and blood pressure, respectively.
Collectively, efforts with wireless technologies signal a paradigm shift to transform neonatal care with fewer risks and burdens, and to improve clinical workflow and patient safety. With continued refinement and real-world validation, wireless multimodal sensors are poised to enhance monitoring precision, promote a patient-centric environment, and ultimately give our most vulnerable patients a gentler start to life . With that, a wireless NICU became a much closer to reality than just fiction.
Vaginal cervical cerclage and progesterone are established treatments for prevention of pregnancy loss and prematurity. There is limited data to assess the effect of these treatments in combination. The objective of this study was to investigate the association between progesterone and no progesterone treatment on pregnancy outcomes in women at high risk of preterm birth who had received a vaginal cervical cerclage.
Methods and findings
This is a secondary post-hoc analysis of women recruited to the C-STICH randomised controlled trial, which recruited in 75 obstetric units in the UK between 2015 and 2021. In the C-STICH trial, women with a singleton pregnancy, receiving a vaginal cervical cerclage due to a history of pregnancy loss or premature birth, or if indicated by ultrasound, were randomised to cerclage with braided or monofilament suture, with a primary outcome of pregnancy loss, defined as miscarriage, stillbirth, or neonatal death in the first week of life. In this secondary analysis, the primary outcome was pregnancy loss, defined as miscarriage and perinatal mortality, including any stillbirth or neonatal death in the first week of life. Secondary maternal outcomes included miscarriage and previable neonatal death; stillbirth; gestational age at delivery; preterm pre labour rupture of membranes, and sepsis. Secondary neonatal outcomes included early/late neonatal death and sepsis. For each outcome, regression models were fitted adjusting for prespecified prognostic variables.
From the 2,048 women recruited to C-STICH, 1943 (95%) women had a vaginal cerclage placed and available progesterone data. Of these, 834 (43%) women received progesterone and 1,109 (57%) did not receive progesterone. In women with primary outcome data available, in our predefined analysis pregnancy loss occurred in 49 (5.9%) of 832 women who received progesterone and 91 (8.3%) of 1,103 women who did not receive progesterone (adjusted* risk ratio 0.70 (95% confidence interval (CI) [0.50, 0.99]); adjusted risk difference −0.02 (95% CI [−0.04, −0.001], *adjusted for indication, obstetric history, surgical technique, and maternal age). Further exploratory analysis excluding women who had termination of pregnancy for foetal anomaly demonstrated a nonsignificant reduction in the risk of pregnancy loss. Key limitations of this study include a non-randomized trial design and unknown confounding relating to variation in progesterone use.
Conclusion
In women with a vaginal cervical cerclage and concomitant progesterone there appears to be an association with a reduced risk of pregnancy loss. This combination therapy may be an important opportunity to further reduce the risk of pregnancy loss in this high-risk cohort.
Stronger Together: Building Friendship, Community, and Courage as Neonatal Womb Warriors
Building friendships is one of the most powerful ways we grow as Neonatal Womb Warriors. As preemie survivors, we begin life in a world of uncertainty, strength, and resilience that most people never experience. That journey can sometimes feel isolating—but it doesn’t have to be. When we build friendships with peers, colleagues, and our broader community, we create spaces where our stories are understood, our challenges are validated, and our victories are celebrated. These connections remind us that we are not alone—we are part of a network of survivors, supporters, and advocates who stand together.
Friendship also teaches us how to trust again—trust in others, and trust in ourselves. Many preemie survivors grow up navigating medical complexities, transitions, and moments of vulnerability. Through friendships, we learn how to communicate our needs, listen to others, and build mutual support systems. Whether it’s a colleague who understands the importance of flexibility, a friend who encourages us during a difficult moment, or a mentor who helps us see our potential, these relationships become pillars of strength. They help transform survival into thriving.
Stepping outside of our comfort zone is often where the most meaningful connections begin. It can feel intimidating to introduce yourself, to join a new group, or to share your story—but courage lives in those small steps. For Neonatal Womb Warriors, getting out of our comfort zone is not just about social growth; it’s about reclaiming our voice and our place in the world. Each time we reach out, collaborate, or say yes to a new opportunity, we expand what is possible for ourselves and for others who may be watching and learning from our example.
At its heart, friendship is teamwork. It is showing up for one another, lifting each other up, and building something stronger together than we could alone. As a community of preemie survivors, families, clinicians, and advocates, we are all part of a shared mission: to help every warrior survive, grow, and thrive. When we lean into friendship and community, we build not only support systems, but movements of compassion, advocacy, and hope. And that is the true strength of a Neonatal Womb Warrior.
Belize’s abundance of terrestrial and marine plants and animals and its diversity of ecosystems, including extensive coral reefs, give it a key place in the globally significant Mesoamerican Biological Corridor. It is considered a Central American and Caribbean nation with strong ties to both the American and Caribbean regions.
It has an area of 22,970 square kilometres (8,867 sq mi) and a population of 397,483 (2022). Its mainland is about 290 km (180 mi) long and 110 km (68 mi) wide. It is the least populated and least densely populated country in Central America. Its population growth rate of 1.87% per year (2018 estimate) is the second-highest in the region and one of the highest in the Western Hemisphere. Its capital is Belmopan, and its largest city is the namesake city of Belize City. The country has a diverse society composed of various cultures and languages. It is the only Central American country where English is the official language. Belizean Creole and Spanish are widely spoken, followed by the Mayan languages and Garifuna. Over half the population is multilingual due to the diverse linguistic backgrounds of the population. It is known for its September Celebrations and punta music.
Healthcare in Belize is provided through both public and private healthcare systems. The Ministry of Health (MoH) is the government agency responsible for overseeing the entire health sector and is also the largest provider of public health services in Belize. The MoH offers affordable care to a majority of Belizeans with a strong focus on providing quality healthcare through a range of public programs and institutions.
In contrast to the public health sector, the private health sector provides care to a smaller portion of the population. However, similar to the public sector, private health services are offered at a relatively low cost with a shared emphasis on quality of care and quality improvement.
The Human Rights Measurement Initiative[3] finds that Belize is fulfilling 83.0% of what it should be fulfilling for the right to health based on its level of income. When looking at the right to health with respect to children, Belize achieves 99.1% of what is expected based on its current income. In regards to the right to health amongst the adult population, the country achieves only 86.6% of what is expected based on the nation’s level of income. Belize falls into the “very bad” category when evaluating the right to reproductive health because the nation is fulfilling only 63.2% of what the nation is expected to achieve based on the resources (income) it has available.
Longest continuously running study on preterm birth that has followed research participants for more than 35 years published in JAMAURI College of Nursing Professor Amy D’Agata’s study shows that the effects of preterm birth can linger throughout an individual’s lifetime, necessitating the inclusion of birth history in adult health records.
KINGSTON, R.I. — August 4, 2025 — The stress preterm infants experience at birth can carry on throughout a lifetime and cause negative health impacts later in life, necessitating the routine inclusion of birth history in medical records and the development of clinical guidelines for adults born preterm, the longest continuously running study of individuals born preterm in the United States has shown.
University of Rhode Island College of Nursing Professor Amy D’Agata is continuing the work that began in the 1980s with a group of babies born preterm at Women & Infants Hospital. Involving 215 people born 35 years ago—including a control group of full-term babies, and preterm babies born at 22 to 36 weeks—the study tracks the successes and difficulties preterm babies continue to face into adulthood, and compares them to the group of participants born full term. The project has so far garnered more than $10 million in research grant funding.
D’Agata, who took over as principal researcher after the retirement of Professor Emeritus Mary Sullivan, has published the most recent results in the Journal of the American Medical Association. The published paper focuses physiological and psychological health outcomes that D’Agata and her team of researchers have identified as the study participants approach 40 years old. Those born preterm have shown a higher risk of high blood pressure, high cholesterol, increased abdominal fat, and low bone density. Psychologically, the group tends to internalize problems, often resulting in increased levels of depression and anxiety.
“Preterm birth is not just a neonatal issue. It, in fact, is a lifelong condition,” D’Agata said the study shows. “For individuals who have medical complications early in life, we are now seeing an increased risk of different chronic health issues later in life. We are now realizing that there is a very strong link between what happens to you early in life and later health outcomes.”
The study offers important takeaways for health-care clinicians, who are not always aware a patient was born preterm because birth history is not commonly included in adult medical records. D’Agata’s study is showing the need to include the information, and to develop adult screening guidelines for individuals who have a history of preterm birth. The work is also helping people who have been impacted by preterm birth understand that their birth history should be included in their medical records and should be considered in the context of their overall health.
“In this country, millions of people born preterm have grown into adulthood and are now seeing clinicians across primary care and various specialties, yet providers rarely ask about birth history,” D’Agata said. “We are urging that birth history be included as a standard question on every adult intake form. Health cannot be fully optimized if we overlook such a critical assessment piece.
Understanding an individual’s birth history, alongside growing research identifying increased health risks for those born preterm and the development of targeted clinical guidelines, will advance health equity for survivors of early birth. We believe a paradigm shift is needed in health care that recognizes preterm birth as a chronic condition requiring lifelong monitoring and support.”
While the study’s most recent results were just published in JAMA Network Open in July, D’Agata is already looking toward the next set of findings. Continuing to work with fellow URI professor Justin Parent, D’Agata is examining epigenetic age acceleration among individuals born preterm. Understanding any differences in epigenetic aging that may exist between preterm and full-term born adults may be another approach to understanding long-term health.
In the heart of the Cuban capital, the Dr. Cosme Ordoñez Carceller Teaching Polyclinic stands as a testament to the nation’s unique approach to healthcare: universal, free of charge, accessible, regionalized, community-centered, and deeply rooted in preventive medicine. Unlike the profit-driven models that dominate much of the world, Cuba’s system prioritizes equitable access, public health education, and early intervention.
At the core of this approach is a commitment to health promotion through education, disease prevention through habit management, and the integration of medical care and rehabilitation. By emphasizing proactive healthcare rather than reactive treatment, the system ensures that communities receive continuous, comprehensive support to maintain overall well-being.
During a recent visit to the Dr. Cosme Ordoñez Carceller Teaching Polyclinic in Havana, the staff detailed how the system was developed and how it ensures that no Cuban, regardless of income, is left without medical care.
The structure of Cuba’s healthcare system
Cuba’s National Health System operates as a hierarchical, state-run model designed to ensure seamless coordination of care. At the top, the National Assembly oversees the Ministry of Public Health, which sets national policies and directs specialized health institutes that tackle broader public health concerns.
Below the Ministry, provincial governments, answering directly to the Assembly, oversee provincial health departments, which manage larger hospitals and specialized medical facilities. These provincial bodies, in turn, delegate responsibilities to municipal governments, which run the municipal health departments and smaller hospitals that serve local populations. At the community level, municipal health departments manage Cuba’s extensive polyclinic network, the cornerstone of the country’s healthcare system. These polyclinics not only provide specialized care, diagnostics, and emergency services, but they also coordinate closely with family doctor-and-nurse teams, who serve as the first point of contact for Cuban citizens.
These frontline providers play a crucial role beyond immediate treatment, emphasizing preventive care, home visits, and alternative therapies such as nutrition counseling, acupuncture, and plant-based medicine. Despite supply shortages exacerbated by US sanctions, this integrated, top-down approach ensures that resources are distributed efficiently, maintaining consistent healthcare access nationwide.
Founded in 1974, the Dr. Ordoñez Carceller Polyclinic serves approximately 13,000 residents, offering care in medical specialties such as cardiology, orthopedics, fertility consultations, and genetic testing. The clinic is named after Dr. Cosme Ordoñez Carceller (1927–2019), an epidemiologist and pioneer of Community Medicine, who championed the polyclinic model that emerged in the 1960s and 1970s. He played a key role in training young physicians in comprehensive general medicine and launched innovative programs like the Grandparents’ Circles, a senior care initiative so effective that it was replicated nationwide.
Cuba’s system prioritizes equitable access, public health education, and early intervention. The country’s healthcare approach is rooted in promoting health through education, preventing disease by managing habits, and ensuring comprehensive medical care and rehabilitation. Unlike the fragmented, for-profit US healthcare model, Cuba’s integrated, community-based approach ensures better health outcomes and higher patient satisfaction. At polyclinics like Ordoñez Carceller, primary care is not just about treating illness but about education, prevention, and holistic well-being. This commitment to accessible, people-centered medicine reflects Cuba’s broader philosophy: that healthcare is not a privilege, but a fundamental human right.
Cuba’s healthcare achievements: A global leader in public health
Despite enduring over six decades of economic embargo, Cuba has achieved remarkable public health milestones. The following list highlights key accomplishments of both the Ordoñez Carceller Polyclinic and the Cuban healthcare system as a whole:
AIDS: Cuba identified HIV in 1983 and quickly set up a system to track and treat it. By 2014, it eliminated mother-to-child transmission of HIV and syphilis, a milestone the US has yet to reach.
COVID: Cuba developed two COVID vaccines, kept infections low, and even sent vaccines abroad.
Diabetes: The nation has developed an effective medication that treats diabetic ulcers (skin wounds that result from poor blood sugar control)
Alzheimer’s research: Cuba developed a drug that may help reverse Alzheimer’s effects
Maternal-fetal medicine: 99% of Cuban children are vaccinated, and the country has a lower infant mortality rate than the US
Nutrition: While obesity is not an issue in Cuba, malnutrition is an increasing concern due to shortages caused by the US embargo
Home health Doctors make house calls to care for the elderly and new mothers.
Profit vs. public health: How medical education and healthcare delivery differ in Cuba and the US
The paths to becoming a doctor in Cuba and the United States could not be more different. In the US, medical students take on crippling debt, often exceeding USD 200,000, before ever treating a patient. The pressure to repay loans steers many toward high-paying specialties, leaving primary care and rural communities underserved. The system is structured around financial incentives rather than public need, reinforcing the idea that medicine is a business first, a service second.
Cuba takes the opposite approach. Medical education is fully state-funded, allowing students to focus on patient care instead of profit. Training begins immediately after secondary school, with students placed in community clinics early in their careers. By the time they specialize, they have already served in primary care settings, ensuring that the system produces physicians committed to public health, not private wealth.
A focus on prevention, not just treatment
Cuba’s prevention-first model stands in stark contrast to the reactive nature of US healthcare. While American medicine often prioritizes treatment over lifestyle interventions, Cuban doctors routinely incorporate nutrition, exercise, and disease prevention strategies into care plans. The country’s polyclinic system ensures patients receive consistent, community-based healthcare rather than navigating a fragmented, for-profit system that often leaves them behind.
The US blockade: An unjust barrier to health
The US embargo continues to hinder Cuba’s healthcare system by restricting access to essential medicines, medical equipment, and scientific research. Pharmaceutical and shipping companies, fearing US penalties, avoid business with Cuba—leading to severe shortages of everything from aspirin to cancer treatments.
Even medical journals and online resources are blocked due to US restrictions, forcing Cuban researchers to work under constraints that most Western physicians never encounter.
Yet, rather than succumbing to these barriers, Cuba has turned to self-sufficiency, investing in biotechnology, vaccine development, and herbal medicine research to compensate for limited imports. If freed from economic sanctions, Cuba’s contributions to global healthcare innovation could expand exponentially.
For decades, Cuba has exported medical expertise worldwide, sending doctors to disaster-stricken and underserved regions. These global medical brigades have provided care to millions, particularly in Latin America, Africa, and the Caribbean. Yet, rather than supporting these humanitarian efforts, Washington has sought to dismantle them. In February 2025, the US expanded sanctions on Cuba’s international medical program, further restricting its ability to send doctors abroad. The move reflects a deeper failure to understand Cuba’s model of solidarity-driven healthcare, a stark contrast to the US system, where medicine is often dictated by profit rather than public service.
It is within this profit-driven framework that Cuba’s medical missions are misunderstood, labeled as “forced labor” by those who cannot imagine doctors choosing service over salary. The very idea of healthcare as a human right, rather than a commodity, challenges the US worldview, leading to efforts to discredit and sanction those who practice it differently.
What could be if the embargo were lifted
Cuba’s healthcare system is a model of resilience and innovation, but its full potential remains hindered by decades of US sanctions. If given access to global resources and technology, Cuban researchers could expand medical advancements in infectious diseases, chronic illness treatment, and disaster response. For now, Cuban doctors continue their work—undaunted by external pressures, committed to the principle that healthcare is a right, not a privilege.
People’s Health Dispatch is a fortnightly bulletin published by the People’s Health Movement and Peoples Dispatch. Renée L. Quarterman, MD, FACS, is a surgical breast specialist. She is the director of Delaware Breast Care, a part of US Oncology.
Quality improvement (QI) initiatives have become essential to advancing patient outcomes in the neonatal intensive care unit (NICU), where high acuity and complex care are the norms. NICU nurses are uniquely positioned to find inefficiencies, propose practical solutions, and drive meaningful change. However, despite the growing emphasis on QI in nursing practice, well-intentioned projects fall short due to avoidable missteps in the planning and execution phases.
The following guide can be utilized by NICU nurses to navigate through common pitfalls in QI research and offers evidence-based strategies to overcome them. By focusing on foundational principles and real-world examples, this guide supports nurses in conducting impactful, sustainable QI work that enhances neonatal outcomes and team collaboration.
Common Pitfalls in QI Research
Lack of Clear Problem Definition
A common pitfall in QI efforts is the failure to define the problem thoroughly. Without a precise understanding of the issue, teams may invest critical time and resources into solutions that do not address the root cause.
For instance, a unit may notice an uptick in central line-associated bloodstream infections (CLABSIs) and immediately implement new sterile techniques without investigating the underlying variables. Was the increase related to staffing changes, procedural drift, or equipment issues? Without a clear problem definition, interventions risk being misaligned or ineffective.
Strategy: Use structured problem-identification tools—such as root cause analysis (like the Five Whys) or fishbone diagrams—to uncover deeper system issues. Frame the problem in a way that is specific, data-informed, and agreed upon by stakeholders. A clearly defined problem becomes the foundation for targeted and measurable interventions.
Neglecting Stakeholder Involvement
Successful QI initiatives require input and collaboration across disciplines. A common misstep occurs when projects are developed in isolation, often without input from those who will implement or be affected by the change. This can lead to resistance, logistical challenges, or unintended consequences.
For example, consider a QI team aiming to improve feeding initiation times by adjusting nursing workflows. If respiratory therapists or neonatal physicians are not consulted, the new protocol might inadvertently clash with intubation or stabilization practices, resulting in delays rather than improvements.
Strategy: Identify all stakeholders early in the project, including nurses, physicians, respiratory therapists, pharmacists, and families, when appropriate. Conduct stakeholder analyses and engage representatives in project design and testing phases. Inclusive collaboration fosters ownership, smoother implementation, and more sustainable outcomes (Institute for Healthcare Improvement, n.d.).
Poorly Defined Metrics
Without clearly defined, relevant, and measurable outcomes, a QI initiative’s impact is difficult to assess. Broad or vague goals such as “improve thermoregulation” fail to provide direction or an evaluation method.
Strategy: Use SMART goals—Specific, Measurable, Achievable, Relevant, and Time-bound—to guide metric development. For instance, instead of aiming to “reduce hypothermia,” a SMART goal might be: “Increase the percentage of newborns with normothermic admission temperatures (36.5°C–37.5°C) from 65% to 90% over six months.” Tools and resources are available to learn how to develop clear metrics, help track progress, guide adjustments, and communicate results to the team and leadership (Agency for Healthcare Research and Quality, 2020).
Inadequate Data Collection Planning
Even well-designed projects can falter without a strong plan for data collection. Inconsistent, incomplete, or biased data limit the ability to draw valid conclusions and make informed decisions.
Strategy: Design a standardized data collection process before the intervention begins. Identify what data are needed, who will collect data, how often, and how data will be stored and analyzed. Use validated tools where possible and use the electronic health record (EHR) system to reduce manual workload and increase reliability. Pilot test the data collection process to identify issues before scaling up.
Failure to Pilot Interventions
Another frequent misstep is implementing large-scale changes without first evaluating them in a controlled way. Skipping the pilot phase can lead to disruptions in care, staff confusion, or overlooked safety concerns.
Strategy: Use Plan-Do-Study-Act (PDSA) cycles to test changes on a small scale. For instance, a new bedside handoff tool can be trialed with one team for over a week before expanding unit wide. Piloting helps refine interventions, identify barriers early, and build staff confidence.
Lack of Sustainability Planning
Often, improvement is easier to achieve than sustain. QI initiatives can experience initial success but not maintain gains over time due to a lack of follow-up, ownership, or integration into routine practice.
Strategy: Plan for sustainability from the outset. Embed new practices into policies, electronic systems, and training programs. Assign champions to monitor compliance, provide feedback, and adapt as needed. Ongoing measurement and leadership support are critical to prevent regression.
Not Sharing or Publishing Results
When results are not shared beyond the unit, valuable insights and lessons are lost. This limits the potential for broader impact and professional growth.
Strategy: Disseminate findings through presentations, newsletters, or professional journals. Even small projects can inspire similar efforts elsewhere and contribute to the collective advancement of neonatal care. Sharing also strengthens the culture of learning and improvement.
Better QI Creates Lasting Change
Quality improvement is a powerful tool NICU nurses use to enhance care and outcomes. By avoiding common pitfalls—such as unclear problem definitions, poor metric planning, and lack of sustainability—nurses can lead effective and lasting change. Through structured planning, collaborative engagement, and thoughtful execution, every QI effort becomes an opportunity for growth and better care for our most vulnerable patients. (Institute for Healthcare Improvement, n.d.).
Ghosting is one of those terms that seem out of place in medicine, borrowed from social media and dating culture. However, the phenomenon itself is alive and well in our clinical ecosystems. In fact, medicine may be one of the most fertile environments for it. How else can someone remain deeply involved, wholly committed, ever-present in the work, yet increasingly pushed to the side, rendered peripheral to decisions they once shaped?
In the professional world, ghosting is less dramatic and more insidious. It is not someone vanishing; it is colleagues stepping around them. It is conversations that slip behind closed doors. It is the rise of intermediaries and buffers. It is the subtle but unmistakable shift from direct speech to third-person references. It is the choice to go around rather than through.
It is ostracizing, but with a veneer of civility. It is quiet exclusion disguised as efficiency.
And yes, it does not feel very good. For many, the experience intensifies with seniority. The more seasoned someone becomes, the more they know, the more institutional memory they carry, the more perspective they bring; the easier it becomes for others to rationalize keeping them out of the loop. People frame it as respect, as courtesy, as a desire not to “burden” them. Nevertheless, the line between courtesy and dismissal is thin and often crossed.
Technology, ironically, amplifies the problem. Zoom, Teams, and the creeping normalization of AI presence create new pathways for invisibility. What once required the discomfort of face-to-face avoidance now happens silently. Disengagement becomes frictionless. They can be physically present on a screen and still be utterly alone in the room. When they realize they are the only one who showed up in person, while everyone else has delegated their attendance to an AI proxy, they feel the ghostliness in full.
Ghosting rarely begins with an attack. It begins with a narrative.
“They’re too busy for this.”
“They have so much on their plate already.”
“They’re so senior; we shouldn’t bother them with this.”
“They don’t need feedback—they’re above the evaluators.”
What begins as deference quietly morphs into distance. And distance, unchecked, hardens into exclusion. Soon, the storyline shifts:
“They’re not involved.”
“They didn’t attend the last meeting.”
“They never weigh in anymore.”
What remains unsaid and often unnoticed is that no one invited them, no one asked for their opinion, and no one created space for them to be part of the process.
Decisions move forward. Processes evolve. Incentives and priorities shift. Meanwhile, the ghosted clinician continues to do their work, unaware that the landscape is changing around them in ways that diminish their role, complicate their tasks, or diminish their influence. When they finally recognize that something fundamental has shifted, it is often too late to re-enter the conversation.
What does this feel like? It feels exactly like being a ghost.
The film The Sixth Sense offers a powerful metaphor. (Spoiler Alert) Bruce Willis’s character, after suffering a fatal gunshot wound, continues living as though nothing has changed. He goes to work, he engages in therapy, and he attempts to connect with his wife. However, something is off. People drift away. His wife is distant. Rooms feel colder. It is only through his sessions with a child who can “see dead people” that he finally confronts the truth: he is no longer part of the living world, no longer part of the relationships he believes himself to be nurturing.
Professionally, the comparison is not perfect, but it is evocative. In medicine, the “ghosts” have not died. They walk our halls. They mentor trainees. They contribute to scholarship. They carry decades of clinical experience. They built the foundations upon which our teams now stand.
Nevertheless, they are treated as if they no longer inhabit the same professional world as everyone else.
Ghosting in medicine is not just a social slight; it is a cultural wound. It erodes respect. It weakens teams. It destroys continuity. It discards institutional memory. It creates unnecessary rifts between generations of clinicians. It deprives trainees of mentorship. It can turn accomplished physicians into isolated figures who continue to serve, but without the acknowledgment or inclusion that sustains service.
Most dangerously, ghosting perpetuates the illusion that this is normal. That it is natural. That it is simply the denouement of a career.
But it does not have to be.
In an era where burnout is widespread, where talent is scarce, and where the wisdom of experience is more valuable than ever, ghosting is a luxury medicine cannot afford. Inclusion is not just good manners: it is good practice. It strengthens teams, enhances decision-making, and honors the very people who paved the way.
So the next time you see a colleague who seems peripheral, someone once central, now slowly fading from the edges of the conversation—pause before stepping around them. Invite them in. Ask their opinion. Keep them part of the fabric of the work. The difference between belonging and ghosthood may hinge on the smallest acts of acknowledgment, the simplest acts of inclusion. Because the ghost you see before you today is not a relic to be ignored; they are a reflection, a warning, of what any one of us might become.
At well-baby visits, your baby’s provider checks your baby’s health and development and gives your baby vaccinations to protect them from diseases.
If your baby has a medical condition, they may need ongoing care from different healthcare providers.
If you think your baby is sick, call their provider. If you think it’s an emergency, call 911.
If your baby needs medicine or medical equipment at home, learn how to give or use it correctly before your baby leaves the NICU.
When does your baby need to see their healthcare provider?
Your baby will get several checkups (well-baby visits) with their provider during their first year. At each visit, talk to their provider to make sure your baby’s developing in a healthy way. Are they rolling over, sitting up, crawling, and walking when they should? These skills are called developmental milestones. You may need to remind the provider that your baby spent time in the neonatal intensive care unit (NICU), because this may affect when they reach the milestones.
Take your baby’s medical file to your first visit with your baby’s provider. This file includes their discharge summary and other information from the hospital. The provider needs to know what happened during and after your baby’s birth. Hospital staff may send the summary directly to the provider.
If your baby has a medical condition, such as a birth defect, they may need ongoing care from different healthcare providers. Find a way to keep track of your baby’s medical appointments. This may be on a calendar in your kitchen or on your phone with an alert to remind you. Decide if it’s easier to schedule a few appointments on the same day or spread them out over different days.
Ask your providers to keep your baby’s main provider up to date about all visits and treatments. This helps make sure that all members of your baby’s healthcare team have the same information.
Keep your own record of any checkups, tests, and treatments your baby has had. When your doctor makes a change to your baby’s care or medication, make sure this is also shared with your baby’s in-home nursing care agency and equipment company if you use these services.
What should you do if your baby gets sick?
All babies get sick from time to time. But babies who were in the NICU are more likely than other babies to get infections. Watch for signs that your baby may be sick so you can get medical help right away. You should call your baby’s healthcare provider if your baby:
Looks blue around the nose, lips, or on the skin, or is paler than usual
Refuses to eat or doesn’t eat enough
Throws up (which is more serious than spitting up or reflux)
Has less than five wet diapers in a 24-hour period, or has diarrhea for more than a day
Has a large or hard belly that they have not had before
Has a temperature higher than 100.4 F or lower than 97 F (using a rectal thermometer)
Has apnea or trouble breathing. Apnea is when the baby stops breathing for 15 seconds or more.
You know your baby best. If you think something is wrong, call their provider, call 911, or take your baby to the emergency room.
How do vaccinations help protect your baby?
All babies, including those who spend time in the NICU, need vaccinations to help protect them from serious diseases. Some babies start getting these shots while they’re in the NICU. Check with your baby’s provider about when they need their vaccinations. Keep a record of your baby’s vaccinations in your medical file for them.
If you have other children, they need their vaccinations, too. This helps keep them from passing infections to the baby. During flu season, everyone in the family, including parents, should get a flu shot. Any adult who may have contact with your baby also needs a Tdap vaccination. This vaccination helps protect against tetanus, diphtheria, and pertussis (whooping cough). If you didn’t receive your Tdap vaccine during pregnancy, you can get it after you’ve given birth. To create a safe space for your baby, it is important for everyone who will be in contact with your baby to receive their vaccinations.
How can you protect your baby from respiratory syncytial virus (RSV)?
RSV is a common virus. It affects almost all children before they reach age 2. Most of the time, it causes a slight cold. But for preterm babies (born before 37 weeks of pregnancy), this virus can be more serious. Babies born preterm or who have heart or lung problems may benefit from a medicine to keep them from getting RSV. Ask your baby’s healthcare provider if your baby got this medicine in the NICU or if they should get it now that they’re at home.
What do you need to know about giving your baby medicine?
Some babies go home from the NICU still taking medicines. Learn how to give your baby their medicine before they leave the hospital. Write down all the directions. If you have questions or are worried about giving your baby medicine, tell the nurse or other NICU staff. They can show you exactly what to do so you feel comfortable and confident about giving your baby medicine.
When giving your baby medicine, make sure you know:
Where you can get the prescription filled (at a grocery store, drug store, or pharmacy). A prescription is an order for medicine given by a healthcare provider.
How much medicine to give, how often to give it, and when to stop giving it
If you can give it before, during, or after feedings
If the medicine needs to be refrigerated, prepared, or mixed
What to do if you miss a dose
If your baby needs more than one medicine, if you can give them together at the same time
You also need to know:
What position your baby should be in to take the medicine
What to do if your baby spits up or vomits the medicine
If there are side effects from the medicine and what to do if your baby has them
To track your baby’s different medicines and when to give them, use a chart. Ask the nurse to help you make the chart.
How can you manage your baby’s medical equipment at home?
If your baby has medical equipment at home, this can feel like a lot to manage. Staying organized and planning ahead can help. Keep a list of your baby’s equipment and medical supplies, including order numbers, size, and quantity. The equipment company can give you a checklist. Be sure to re-order supplies with enough time, as shipments can sometimes be delayed. Always be prepared when you leave the house, make sure you have your baby’s supplies even when you’re just going to the park.
If the equipment uses electricity:
Share information about your baby’s medical condition with your local fire department and emergency or first responders so they know what to expect in case they’re called to your home for an emergency. Invite them to come to your home to meet you and your baby.
Contact your utility companies to let them know your baby’s healthcare needs. They may have a priority list for repairing power outages or plowing snow.
Make a plan for if the power goes out. Have back-up batteries and know how long they will last.
Anxiety is another word for feeling worried or scared. It’s normal for children and teens to feel anxious sometimes, like before a big test at school or talking in front of a group of people. But if your child’s anxiety gets in the way of normal activities, such as sleeping alone at night, playing outside or going to school, they may need extra support.
The good news is that there are things you can do to help prevent your child from feeling anxious and help them handle worries when they happen. Talk with your pediatrician to discuss strategies and tips that can help.
What are some common signs of anxiety in children?
If your child is feeling anxious, they may not be able to tell you. Your child may feel bad or sick without knowing why, or you may notice they seem restless or tired.
Feeling as if their heart is racing
Sweating or blushing
Shaking or feeling sick to their stomach
Feeling very cold or hot
Trouble paying attention or sitting still
Touching the crotch area (for young boys)
How can I help my child manage anxiety at home?
These tips are helpful for all children, but they can be especially helpful for children with anxiety. Parenting is a busy job, so use your judgment about which tips make the most sense for your family.
Connect with your child
Set aside one-on-one time every day without TV or other media. Even just 10 minutes each day can make a big difference. Try gardening or taking care of houseplants, drawing or going for a bike ride.
Praise your child and make them feel good about themselves. For example, “You did a great job on that homework assignment!” or “Thank you for helping me with the laundry. I’m so lucky to have your help.”
Find out what’s worrying your child, because stress can make them feel anxious. Things such as being bullied at school, divorce, or a death in the family can make a child feel anxious. Your child may need extra help to handle issues such as these.
Help your child learn to manage fears
When your child is calm, start a conversation about things they can do to manage fears and worries when they happen. For example, let them know that they can
Practice deep breathing and muscle relaxation.
Use positive self-talk (for example, “I can try this” instead of “I can’t do this”).
Think of a safe place, such as their bedroom or favorite place outdoors.
Gradually facing fears. Consider gradually exposing your child to feared objects or activities.
Praise and reward brave behavior: the goal is to cope, not avoid.
Get active! Encourage your child to be active for at least an hour every day. This activity can include playing outside, joining a sports team or an activity at the YMCA, biking or walking to school, or dancing at home to favorite music.
Eat healthy. Eat healthy meals every day, including fruits and vegetables, whole grains, and protein foods. Remember to eat breakfast!
Get plenty of sleep. School-aged children need 9 to 12 hours of sleep every night, and teens need 8 to 10 hours.
Build a family media planto set healthy guidelines around entertainment screen time. Avoid scary or violent TV shows, video games, and movies.
Set up family routines. Follow a regular schedule for playtime, mealtime, and bedtime. Knowing what to expect can help your child feel safe and secure.
How can I help my child manage school anxiety?
Children may find it hard to focus on or even go to school when they’re feeling worried. If your child is having trouble in school, try these ways to help.
Gently but firmly tell your child why it’s important to go to school.
Talk with your child’s teachers and the guidance counselor about what to do if your child asks to go home from school early.
If you think your child may be upset by family stress or pressure to do well in school, let them know they are doing a good job and you’re proud of them.
Help your child set realistic goals for school. If they set goals that are too hard to meet, they may feel worse about themselves.
Remind your child that they can take steps to control their worries. For example, they can think about what to do ahead of time to handle a stressful situation.
Reward your child’s brave behaviors at school. Spending time doing fun activities with a parent is a very powerful reward.
Remember, you know your child best.
Whether it’s at school or the doctor’s office, you are your child’s biggest advocate. Don’t hesitate to speak up on behalf of your child.
When do I need to go back to the doctor?
If your child’s anxiety doesn’t go away or gets worse, get back in touch with the doctor. You and the doctor can make a plan to try new approaches or strategies with your child.
It’s especially important to talk with your child’s doctor if:
Your child starts to experience other behavior problems, such as shyness.
Something scary happens in your child’s life that may make their anxiety worse, such as an injury or death in the family.
You suspect your child’s anxiety is affecting another medical condition (for example, if your child’s asthma gets worse with anxiety).
The doctor can also help you decide whether visiting a specialist may help. For example, a type of therapy called cognitive behavioral therapy can be helpful for children with anxiety.
Make time to care for yourself, too.
Parenting can be stressful. If you’re feeling overwhelmed, don’t be afraid to ask for support from family, close friends, social services, or your faith community. Children pick up on the stress and worries of adults, so getting support for yourself can help your child too.
The neonatal intensive care unit (NICU) is a special unit in the hospital for babies born preterm, very early, or who have some other serious medical condition. Most babies born very early will need special care after birth. This is done by or under the supervision of a neonatologist, a doctor with special training in the care and problems of newborns.
This article discusses the consultants and support staff who may be involved in the care of your infant depending on your infant’s specific medical needs.
Information
AUDIOLOGIST
An audiologist is trained to test a baby’s hearing and provide follow-up care to those with hearing problems. Most newborns have their hearing screened before leaving the hospital. Your health care providers will determine which hearing test is best. Hearing tests may also be done after leaving the hospital.
CARDIOLOGIST
A cardiologist is a doctor that has special training in the diagnosis and treatment of heart and blood vessel disease. Pediatric cardiologists are trained to deal with newborn heart problems. The cardiologist may examine the baby, order tests, and read test results. Tests to diagnose heart conditions may include:
If the structure of the heart is not normal due to a birth defect, a cardiologist might work with a cardiovascular surgeon to perform surgery on the heart.
CARDIOVASCULAR SURGEON
A cardiovascular (heart) surgeon is a doctor who has special training in doing surgery to correct or treat defects of the heart. Pediatric cardiovascular surgeons are trained to deal with newborn heart problems.
Sometimes, surgery can correct a heart problem. Other times, complete correction is not possible and surgery is done just to make the heart work as well as possible. The surgeon will work closely with the cardiologist to care for the baby before and after surgery.
DERMATOLOGIST
A dermatologist is a doctor who has special training in diseases and conditions of the skin, hair, and nails. Such a doctor might be asked to look at a rash or skin lesion on a baby in the hospital. In some cases, the dermatologist might take a sample of the skin, called a biopsy. The dermatologist might also work with the pathologist to read the biopsy results.
DEVELOPMENTAL PEDIATRICIAN
A developmental pediatrician is a doctor who has been specially trained to diagnose and care for infants who have trouble doing what other children of their age can do. This type of doctor often evaluates babies who have already gone home from the NICU and will order or perform developmental tests. The doctor can also help you find resources near your home that provide therapies to help infants and children in meeting development milestones. Developmental pediatricians work closely with nurse practitioners, occupational therapists, physical therapists, and sometimes neurologists.
DIETITIAN
A dietitian has special training in nutritional support (feeding). This type of provider may also specialize in pediatric (children’s) nutritional care. Dietitians help determine if your baby is getting enough nutrients, and may recommend some choices of nutrition that can be given through the blood or a feeding tube.
ENDOCRINOLOGIST
A pediatric endocrinologist is a doctor with special training in the diagnosis and treatment of infants with hormone problems. Endocrinologists might be asked to see babies who have problems with the level of salt or sugar in the body, or who have problems with the development of certain glands and sexual organs.
GASTROENTEROLOGIST
A pediatric gastroenterologist is a doctor with special training in the diagnosis and treatment of infants with problems of the digestive system (stomach and intestines) and liver. This type of doctor might be asked to see a baby who has digestive or liver problems. Tests, such as x-rays, liver function tests, or abdominal ultrasounds, might be done.
GENETICIST
A geneticist is a doctor with special training in the diagnosis and treatment of infants with congenital (inherited) conditions, including chromosomal issues or syndromes. Tests, such as chromosome analysis, metabolic studies, and ultrasounds, may be done.
HEMATOLOGIST-ONCOLOGIST
A pediatric hematologist-oncologist is a doctor with special training in the diagnosis and treatment of children with blood disorders and types of cancer. This type of doctor might be asked to see a baby for bleeding problems due to low platelets or other clotting factors. Tests, such as a complete blood count (CBC) or clotting studies, might be ordered.
INFECTIOUS DISEASE SPECIALIST
An infectious disease specialist is a doctor with special training in the diagnosis and treatment of infections. They might be asked to see a baby that develops unusual or serious infections. Infections in babies can include blood infections or infections of the brain and spinal cord.
MATERNAL-FETAL MEDICINE SPECIALIST
A maternal-fetal medicine doctor (perinatologist) is an obstetrician with special training in the care of high-risk pregnant women. High-risk means there is an increased chance for problems. This type of doctor can care for women who have premature labor, multiple gestations (twins or more), high blood pressure, or diabetes.
NEONATAL NURSE PRACTITIONER (NNP)
Neonatal nurse practitioners (NNP) are advanced practice nurses with extra experience in the care of newborn infants in addition to completing master’s or doctoral level educational programs. The NNP works along with a neonatologist to diagnose and treat health problems in babies in the NICU. The NNP also performs procedures to help diagnose and manage certain conditions.
NEPHROLOGIST
A pediatric nephrologist is a doctor with special training in diagnosing and treating children who have problems with the kidneys and urinary system. This type of doctor might be asked to see a baby who has problems in the development of the kidneys or to help care for a baby whose kidneys do not work properly. If a baby needs kidney surgery, the nephrologist will work with a surgeon or urologist
.NEUROLOGIST
A pediatric neurologist is a doctor with special training in the diagnosis and treatment of children with disorders of the brain, nerves, and muscles. This type of doctor might be asked to see a baby who has seizures or bleeding in the brain. If the infant needs surgery for a problem in the brain or spinal cord, the neurologist might work with a neurosurgeon.
NEUROSURGEON
A pediatric neurosurgeon is a doctor trained as a surgeon who operates on children’s brains and spinal cords. This type of doctor might be asked to see a baby who has problems, such as spina bifida, skull fracture, or hydrocephalus.
OBSTETRICIAN
An obstetrician is a doctor with special training in taking care of pregnant women. This type of doctor might also assist women who are trying to get pregnant and follow women with medical conditions, such as diabetes or decreased fetal growth.
OPHTHALMOLOGIST
A pediatric ophthalmologist is a doctor with special training in diagnosing and treating eye problems in children. This type of doctor might be asked to see a baby who has birth defects of the eye.
An ophthalmologist will look at the inside of the baby’s eye to diagnose retinopathy of prematurity. In some cases, this type of doctor might perform laser or other corrective surgery on the eyes.
ORTHOPEDIC SURGEON
A pediatric orthopedic surgeon is a doctor with special training in the diagnosis and treatment of children who have conditions involving their bones. This type of doctor might be asked to see a baby who has birth defects of the arms or legs, hip dislocation (dysplasia), or fractures of the bones. To see the bones, orthopedic surgeons might order ultrasounds or x-rays. If needed, they can perform surgery or place casts.
OSTOMY NURSE
An ostomy nurse is a nurse with special training in the care of skin wounds and openings in the belly area through which the end of the intestine or the collecting system of the kidney stick out. Such an opening is called an ostomy. Ostomies are the result of surgery needed to treat many intestinal problems, such as necrotizing enterocolitis. In some cases, ostomy nurses are consulted to help care for complicated wounds.
OTOLARYNGOLOGIST/EAR NOSE THROAT (ENT) SPECIALIST
A pediatric otolaryngologist is also called a pediatric ear, nose, and throat (ENT) specialist. This is a doctor with special training in the diagnosis and treatment of children with problems with the ear, nose, throat, and airways. This type of doctor might be asked to see a baby who has problems with breathing or a blockage of the nose.
Occupational and physical therapists (OT/PT) are professionals with advanced training in working with infants with developmental needs. This work includes neurobehavioral assessments (postural tone, reflexes, movement patterns, and responses to handling). In addition, the OT/PT professionals will help determine a baby’s nipple-feeding readiness and oral-motor skills. Speech therapists will also help with feeding skills in some centers. These types of providers might also be asked to provide family education and support.
PATHOLOGIST
A pathologist is a doctor with special training in lab testing and examination of body tissues. They supervise the lab where many medical tests are performed. They also examine tissues under the microscope that are obtained during a surgery or an autopsy.
PEDIATRICIAN
A pediatrician is a doctor with special training in the care of infants and children. This type of doctor might be asked to see a baby in the NICU, but is usually the primary care provider for a healthy newborn. A pediatrician also provides primary care for most babies after they leave the NICU.
PHLEBOTOMIST
A phlebotomist is a specially trained professional who takes your blood. This type of provider may take the blood from a vein or a baby’s heel.
PULMONOLOGIST
A pediatric pulmonologist is a doctor with special training in diagnosing and treating children with respiratory (breathing) conditions. Even though the neonatologist cares for many infants with respiratory problems, the pulmonologist might be asked to see or to help care for babies who have unusual conditions of the lung.
RADIOLOGIST
A radiologist is a doctor with special training in obtaining and reading x-rays and other imaging tests, such as barium enemas and ultrasounds. Pediatric radiologists have extra training in imaging for children.
Social workers are professionals with special education and training to determine the psychosocial, emotional, and financial needs of families. They help families find and coordinate resources in the hospital and community that will help to meet their needs. Social workers also help with discharge planning.
UROLOGIST
A pediatric urologist is a doctor with special training in diagnosing and treating conditions involving the urinary system in children. This type of doctor might be asked to see a baby with conditions such as hydronephrosis or hypospadias. With some conditions, they will work closely with a nephrologist.
X-RAY TECHNICIAN
An x-ray technician is trained in taking x-rays. X-rays can be of the chest, stomach, or pelvis. Sometimes, solutions are used to make body parts easier to see, as with barium enemas. X-rays of bones are also commonly performed on babies for a variety of reasons.
Pediatric surgical conditions are a significant source of morbidity and mortality in low- and middle-income countries (LMICs), where children with surgically treatable conditions lack access to care owing to an insufficient number of pediatric surgeons, poor and limited training, and financial barriers. There is a growing shift from charitable missions to capacity-strengthening projects, which strengthen the skills and resources of communities. The objective of this study was to synthesize the literature to identify capacity-strengthening projects, their methods and outcomes, and their limitations and barriers.
METHODS
MEDLINE, EMBASE, Cochrane, and Web of Science were searched until May 5, 2023. Eligibility criteria were as follows: (1) inclusion of pediatric surgery patients; (2) designation as capacity-strengthening interventions; (3) outcomes of improved access defined through Lancet Commission on Global Surgery Indicators; and (4) designation as an LMIC defined by the World Bank. Two independent reviewers conducted screening and extraction.
RESULTS
A total of 80 studies met inclusion criteria. Interventions were implemented in 69 LMICs and used 19 different methods of capacity strengthening. Common capacity-strengthening methods included the following: international surgical visits, training programs, partnerships, mobile clinics and camps, infrastructure enhancements, and telemedicine. Common methods used included the following: training of local providers, continuous contact between both countries after the visit was completed, improved access for rural families, and economic support for low-income families. A total of 1 357 077 pediatric surgeries were performed through these interventions. Limitations included the fact that only peer-reviewed studies were included. Included studies were mainly case series or small observational studies with qualitative data.
CONCLUSIONS
This review identifies methods to implement capacity-strengthening interventions in LMICs, including their successes and barriers. Future research should report ethical concerns and quantitative outcomes to determine effectiveness.
Neonates and infants are commonly referred to as “therapeutic orphans” due to the overall scarcity of therapeutic interventions that have been developed and tailored to their needs and specific characteristics. This is well known by care providers and researchers active in this field, but is perhaps less on the radar of authorities, funding bodies or the broader public. There is significant health inequity when comparing newborns to other age populations in terms of specific drug and device development and therapeutics. In addition there are health inequities in the provision of neonatal care globally which require special attention in terms of improvement.
Bronchopulmonary dysplasia, neonatal seizures, poor growth, necrotizing enterocolitis (NEC) and short bowel, hypoxic-ischemic encephalopathy, retinopathy of prematurity (ROP), neonatal infections and sepsis hereby serve as a non-exhaustive list of “orphan conditions” in need of more equity, through adequately and urgently funded research and improvement.
The good news is that there have been increased efforts, in recent years, by researchers and regulatory bodies to focus on the provision of drugs, devices, and treatment modalities tailored for neonatal use, while further advocacy remains an obvious need . This brings perspective and explains the initiative taken to organize a focused research topic on what is on the horizon as well as recent advances.
Overview of the topics covered
We targeted emerging or new aspects related to monitoring, diagnostics and therapeutics in neonatal care for the current research topic. Fortunately, this research topic was perceived as very relevant by the research community, as 135 authors expressed their interest as contributors, resulting in 20 accepted papers. This serves as a signal of the importance to continue to work on this topic.
Post-hoc, and in a somewhat arbitrary way (because of overlap in these subcategories) these papers were subdivided by the editors into different subcategories, with focus on (1, 5 papers) perinatal biomarkers in blood and urine and how these relate to or predict outcomes, (2, 6 papers) adaptations of existing and newly emerging equipment in neonatal units, (3, 3 papers) needed advances in pharmacotherapy, (4, 3 papers) machine learning or deep learning applications in neonatal care, and finally, (5, 3 papers) underreported aspects of contemporary NICU care, with a focus on the holistic nature of care for the infant and the family.
Perinatal biomarkers in blood and urine and how these relate to or predict outcomes
Two papers focused on biomarkers related to gestational diabetes, with reflections and data on maternal and neonatal outcomes. Postnatal maternal levels of glycated albumin and hemoglobin A1c in mothers of large-for-gestational-age (LGA) informed us of the relevance of accurate diagnosis during pregnancy. This is because postpartum women without diagnosis during pregnancy had higher glycated albumin values, associated with LGA and associated complications (Železnik et al.). Interestingly and related to this paper, Yin et al. reported on a untargeted metabolomics study in women with gestational diabetes, with the recommendation of a maternal serum metabolite panel to forecast neonatal adverse outcomes (hypoglycemia and macrosomia) (Yin et al.).
Other papers focused on the use of vitamin D, acid-base and biomarkers associated with fetal growth restriction with impaired neurodevelopmental outcome. In a cohort of 217 preterm neonates, a multivariate regression analysis identified antenatal steroids as protective, and lower birth weight, duration of ventilation, sepsis and the serum 25-(OH)D vitamin as risk factors to develop ROP (Yin et al.). Musco et al. reported on a systematic review on blood biomarkers indicating risks of adverse neurodevelopmental outcome in fetal growth restricted infants (Musco et al.). While the authors retrieved some data on neuron specific enolase and S100B, the overall conclusions reflect a call for further research. Finally, an association between lactate levels in umbilical cord blood and cerebral oxygenation in preterm neonates was studied as a secondary outcome analysis (Dusleag et al.). In non-asphyxiated preterm neonates with respiratory support, lactate levels were negatively associated with cerebral and arterial oxygenation. In term neonates without respiratory support, no associations were observed.
Adaptations of existing and newly emerging equipment in our units
In a review on emerging innovations in neonatal monitoring, Krbec et al. concluded that there is an urgent, still unmet need to develop wireless, non- or minimal-contact, non-adhesive technology, capable to integrate multiple signals in a single platform, tailored to neonates (Krbec et al.). Related to this call of action, Svoboda et al. reported on their pilot experience with contactless assessment of heart rate, applying imaging photoplethysmography (Svoboda et al.). Rectal and axillary temperature monitoring on admission were compared in a cohort of preterm (n = 80, <32 weeks gestational age) by Halabi et al., reporting that rectal measurement was likely more reliable in the event of hypothermia (Halabi et al.). Ultrasound-guided measurement of anterior cerebral artery resistive index in the first week of life in 739 preterm neonates (<35 weeks) was not associated with subsequent co-morbidities on admission or during neonatal stay (asphyxia, sepsis, NEC) (Singh Gill et al.). A case series of neurally adjusted ventilatory assist to rescue pulmonary interstitial emphysema in 5 extremely low birth weight infants illustrated the potential value of this ventilatory equipment and strategy and need for further study (Chen et al.). Finally, van Rens et al. compared a conventional to a modified Seldinger technique (a dedicated micro-insertion kit) for peripherally inserted central catheter (PICC) placement, illustrating the relevance of developing “low risk, high benefit” type of medical devices, adapted to the specific needs of neonates (van Rens et al.).
Advances needed in pharmacotherapy
The currently available medicines and dosing regimens in neonatal care are limited and there is an urgent need for improvement in this domain. This was illustrated by articles on sepsis, septic shock and steroids. Inequity in provision of neonatal care across the globe ought to be a major focus of improvement. Gezahegn et al. described the outcome in neonates admitted with sepsis in Harar (Ethiopia). Low white blood cell count, desaturation, preterm birth, absence of prenatal maternal care, and chorioamnionitis were important risk factors for sepsis-related mortality (Gezahegn et al.). Addressing these prognostic factors hold the promise to act as levelers to improve outcomes. A pilot study compared noradrenaline and adrenaline as first line vasopressor for fluid-refractory sepsis shock (Garegrat et al.). Both interventions were comparable to resolve the septic shock, while the overall mortality (13/42, 30%) remained significant, highlighting the need for better diagnostic and therapeutic options. Finally, in a systematic review, outcome of postnatal systemic corticosteroids (hydrocortisone to dexamethasone) were compared as reported in randomized controlled trials (Boscarino et al.). The authors concluded that dexamethasone appeared to be somewhat more effective than hydrocortisone in improving respiratory outcomes, but with inconclusive but relevant concerns on the uncertainties on long-term neurodevelopmental outcome, again highlighting the need for better therapies for prevention and management of chronic lung disease of prematurity.
Machine learning or deep learning applications in neonatal care
Artificial intelligence is a rapidly advancing area with fast evolving clinical applications in healthcare, including in the NICU (6). It is no surprise that the current research topic also contains papers illustrating its relevance to improve our practices and outcomes. Two papers hereby focused on NEC, and a 3rd paper on prediction of significant patent ductus arteriosus (PDA). In a mini-review, Cuna et al. reports on the various pathophysiological processes underlying NEC endotypes, and how artificial intelligence holds the promise to influence further understanding and management (Cuna et al.). An approach to enhance surgical decision making in NEC is illustrated by Wu et al. Based on x-rays from 263 neonates diagnosed with NEC (94 surgical cases), a binary diagnostic tool was trained and validated, with Resnet18 as approach applied (Wu et al.). For PDA, an ultrasound-based assessment of ductus arteriosus intimal thickness in the first 24 h after birth was applied in 105 preterm neonates. A prediction model for closure on day 7 included birth weight, mechanical ventilation, left ventricular end-diastolic diameter, and PDA intimal thickness (Hu et al.). Such models can be considered to better target future study, integrated in a precision medicine approach. Use of AI and big data have the potential to significantly improve our understanding of neonatal conditions and also support neonatal researchers in asking better research questions.
Underreported aspects of contemporary NICU care, holistic care
As part of this research topic, we also accepted papers reporting on the use of music on pain management, on multisensory stimulation to improve maternal milk volume production, and parents’ experiences related to congenital cardiac surgery. All these 3 papers reflect the need for holistic care and to further integrate the perspectives of (former) patients and parents into neonatal practice.
In a systematic review, Ou et al. demonstrated that music is an effective intervention to relief procedural pain (e.g., Premature Infant Pain Profile score) in preterm neonates, as it reduced some markers of stress, and improved blood oxygen saturation (Ou et al.). Multisensory stimulation (audiovisual, or audiovisual + olfactory) compared to a control setting improved maternal milk volume production, with evidence of positive effects of both interventions, even more pronounced if both interventions are combined (Cuya et al.). Finally, a quantitative analysis of parent’s experiences with neonates admitted to NICU with a congenital heart disease reinformed us on the importance of actively focusing on parental experiences of care (Catapano et al.).
From advances in neonatal care to implementation In our opinion, this research topic nicely illustrates the diversity in ongoing clinical research activities, that all hold the promise to improve our clinical management practices, with the overarching aim to improve neonatal outcomes. There is an urgent need to focus on the current health inequities in the provision of care to neonates (3). The trend towards a “neuro” dedicated NICU care is an illustration on how relevant progress may occur. This progress is based on improved neuromonitoring techniques (7), improved management and precision medicine in the field of anti-epileptic drugs (8), and integrating families as partners in neonatal neuro-critical care and similar improvement programs (9). The good news is that we are already experiencing a shift in the right direction. The neonatal community and all other relevant stakeholders need to work better together to improve the pace and scale of this improvement.
Despite the widespread use of pain rating scales in neonatal care worldwide, a new Cochrane review shows that current tools for assessing pain in newborns are based on very low quality evidence. According to the review, none of the pain rating scales in use today are methodologically reliable enough to measure pain.
The Cochrane analysis, which included 79 studies involving over 7,000 infants across 26 countries, evaluated 27 different clinical rating scales. The findings reveal significant limitations in the reliability and clinical usefulness of all currently available tools, raising concerns about whether healthcare professionals can accurately measure pain in this extremely vulnerable population.
“We were truly hoping that one pain scale would be stronger than another, but instead we found that all of them are poorly developed. This is an issue that also affects Swedish clinical practice and research. For example, a recent publication out of KI found that 25 percent of Swedish infants were assessed without using a rating scale at all, which was already shocking, and now we can confirm that the remaining 75 percent of the infants were assessed with rating scales that are now known to not be methodologically sound enough to measure pain. So, this unfortunately means that medical professionals cannot be sure whether they are measuring pain at all.” says Emma Persad, Phd student at the Department of Women’s and Children’s Health, Karolinska Institutet.
Yet, from this uncertainty comes a call to action. The researchers hope these findings will spark a global collaborative effort, led by Swedish experts, to develop a new, robust, and evidence-based pain assessment scale for newborns. Such a tool could greatly improve neonatal care worldwide and further establish Sweden as a leader in the field of neonatology.
According to the article “this involves developing better rating scales or physiological techniques to measure pain”.
““This is precisely what we are hoping to do. Through convening the global community we hope these findings and the outcome become a global collaborative effort, driven by Swedish researchers, to finally develop a pain rating scale that is robust and evidence-informed (and will hopefully be properly adapted and translated for use worldwide). We hope that Sweden’s role in neonatology can further be solidified through this work,” says Emma Persad.
Dr. Michael Copass, M.D.—a Harborview Emergency Medicine physician instrumental in the early development and later leadership of the Medic One paramedic training program, helping expand it beyond cardiac care—worked alongside Dr. Leonard Cobb and Seattle Fire Chief Gordon Vickery to shape what would become one of the world’s most respected emergency medical systems. When the original grant funding for the Medic One program ended unexpectedly, the community rallied in extraordinary ways: bake sales, marathons, neighborhood drives, even children donating their birthday money. Their efforts raised nearly $200,000, inspiring the creation of the Medic One Foundation in 1974 to ensure this lifesaving work would never fade. Since that time, more than $35 million has been invested in Medica One’s training, equipment, and research, contributing to lifesaving outcomes on a daily basis.
Years later, that legacy still lives and breathes inside the halls of Harborview Medical Center. As a student assistant with the University of Washington School of Medicine and the UW surgical residency program, I had the privilege of witnessing something quite extraordinary. Each week, an Emeritus physician would return to the hospital—not for recognition or ceremony, but simply to sit down for lunch and vibrant conversation.
Those gatherings were never formal lectures. They were living, breathing exchanges of wisdom — stories from the early days of emergency medicine, thoughtful clinical reflections, and gentle reminders that compassion matters just as much as technical skill. Students, interns, residents, fellows, and senior attendings all pulled up chairs. Hierarchies faded. Curiosity filled the room. Medicine, in its truest form, felt like a shared calling.
It was in those moments that I truly understood the impact Emeritus physicians have on the medical community. They often carry history, perspective, humility — and they give it away freely. Their mentorship strengthens not just clinical practice, but the heart of healthcare itself. The legacy of Medic One isn’t only found in ambulances and survival rates — it is also found in conversations around cafeteria tables, where knowledge is passed from one generation to the next.
And as we continue to advocate for fragile newborns and medically complex children, that lesson stays with me: when compassion, community, courage, and teaching come together, the ripple effect is immeasurable — and hope continues forward.
Lebanon, officially the Republic of Lebanon, is a country in the Levant region of West Asia. Situated at the crossroads of the Mediterranean Basin and the Arabian Peninsula, it is bordered by Syria to the north and east, Israel to the south, and the Mediterranean Sea to the west; Cyprus lies a short distance from the coastline. Lebanon has a population of more than five million and an area of 10,452 square kilometres (4,036 sq mi). Beirut is the country’s capital and largest city.
Most of the Infant and Family Centered Developmental Care (IFCDC) Standards focus on evidence-based approaches to care of the baby and family while in intensive care. An ever expanding literature provides rationale for promoting the best care environments for the baby’s developing brain, as well as for parents’ physical and emotional adjustment as they transition to parenthood. As babies may spend days, weeks, and sometimes months during a critical time for brain and behavioral organization, an emphasis has been placed on neuroprotective caregiving strategies and environmental protection to enhance medical, developmental, and psychosocial outcomes.
Both neurodevelopmental and physiological research focus primarily on the age range of babies from birth to discharge, typically ending at 40 weeks post-conceptional age, or when the baby goes home. As babies may be discharged at earlier ages than in previous years—when medically stable, but before many neurodevelopmental tasks have been firmly established (e.g., coordinated eating, sleeping, and regulation)– it is important to extend the focus to the weeks and months after discharge when the baby is still in a developmental fast track.
Babies deemed medically stable enough to transition home need appropriate supports for discharge and preparation for life after hospitalization. A growing literature documents best practices for that preparation, assuring a smooth and uncomplicated transition to community services.
Post-discharge visits to the baby’s pediatrician typically focus on medical stability, as is appropriate. However, most follow-up clinic visits, which include developmental assessment and monitoring, may not occur until the baby is 3-6 months of age. Early intervention services in the United States provide developmental assessment and intervention, if appropriate, for those babies who are “categorically eligible” through Part C of the Individuals with Disabilities Education Act (IDEA). https://www.ed.gov/laws-andpolicy/individuals-disabilities/idea.
Each state determines the qualifications for eligibility, often including diagnoses of established conditions that demonstrate evidence of significant developmental delay (e.g., Down syndrome, chromosomal abnormalities, deafblind conditions, etc.). Often, low birthweight is either not included or restricted to birthweight under 1200 grams, which excludes those babies who have been identified as likely to have lingering developmental deficits (e.g., late preterm babies 34-36 weeks post-conceptual age). Part C assessment and follow-up are mandated to occur within a 45-day timeframe. However, many babies are not identified while they are in the hospital and may not be deemed eligible until obvious developmental concerns surface.
Rationale for assuring continuity of developmental and psychosocial supports from hospital to home.
Support for early brain organization during the neonatal period and throughout the first years of a baby’s life is critical for later development. The literature is replete with evidence regarding neurophysiological and behavioral development, as well as an emphasis on the need for appropriate relationship environments to promote optimal outcomes. Emerging evidence of specific brain development during the first few months of a baby’s life (often referred to as “the fourth trimester”) lends emphasis to the importance of not only understanding the enormity of brain development during this period, but also the potential opportunities for creating appropriate environments and caregiving.
The impact of early birth, medical complexities, and associated hospitalizations on brain development and organization indicates that short and long-term neurophysiologic, behavioral, and mental health outcomes are affected. These and many other outcome studies emphasize the need for early, appropriate environmental and developmental protections, as well as individualized care. Given the recent findings regarding the significant brain development and organization during the first three to six months (in addition to development during the last trimester), it becomes apparent that a significant focus should be on effective interventions both before and after discharge.
Brain and behavior development in parents
Brain changes also occur as parents are transitioning to becoming primary caregivers of their new baby. Emerging evidence of neuroendocrine, neurophysiologic, and behavioral changes during pregnancy, delivery, and postpartum indicates that the experience of becoming parents—for both mothers and fathers — has significant implications for later physical and mental health. Fewer studies indicative of brain changes in parents of early born and medically fragile babies are available; however, there are clear associations with parental mental and physical health challenges.
Punctuated events and recalibration
As babies transition from being fetuses to newborns, there is a significant impact on their brain and behavioral organization. The environment is significantly different, necessitating adaptation from uterine to a maternal caregiving environment. This dramatic change has been referred to as a “punctuated event,” which signifies a significant change in both physiology and behavior, resulting in a period of adaptation and recalibration of behavior.
As previously proposed, a similar punctuated event occurs when the baby transitions from the familiar hospital caregiving environment to the novel home/community environment. (39, 40) It is no wonder that the babies who transition home experience changes in physiology and behavior as a result. Often, medical issues arise, sleep states are disorganized, feeding challenges occur, and previously effective calming strategies seem to be ineffective. If the parent and baby have not had a chance to experience intimate and consistent caregiving in the hospital, which provides the continuity of a trusting relationship, there can be challenges in the process of recalibration.
Parents also experience significant life-changing events to which they must adapt and recalibrate. Pregnancy to delivery and delivery to parenting represent significant punctuated events that may cause other physiologic and/or mental health concerns to emerge. Most parents of term and medically stable babies have had opportunities to adapt to this change cognitively and psychologically. For parents who have a challenging pregnancy, a difficult delivery, and/or a baby at risk for medical challenges, these punctuated events can raise physiological and psychological challenges to which recalibration is complicated.
As with the transition home for babies, the transition home for parents can be disorganizing and difficult. Parents may not only be dealing with their own physical and/or mental health issues as a result of pregnancy, delivery, and hospitalization of their baby, but with the full-time care and adjustment to care in their own home environment. (48-50) Often, the demands of baby care and selfcare are discrepant, resulting in poor sleeping and eating, lack of exercise and social interactions, and other mental health concerns becoming issues that need to be addressed. Unfortunately, these issues may not be addressed quickly and may persist for the first 3-6 months of the family’s life together at home.
Relationship environments are essential for optimal development.
One of the most significant influences on babies’ outcomes is the relationship environment with their primary caregiver. Given the significant neurophysiological and behavioral changes that occur in both newborns and their parents during the first few months after delivery, the development of robust and mutually supportive interactions is fraught with a variety of challenges and successes. These are particularly challenging for parents who come to parenting with significant mental health issues, economic and/or cognitive challenges, few social supports, and/or limited educational backgrounds. Effective interventions have been developed to enhance the parent/baby relationships applied in community settings.
Although effective interventions in communities to promote relationships between parents and their babies have been developed, the application of these programs for parents of medically fragile or early born babies and related research is limited. Having a hospitalized baby presents challenges to early relationship development. A multitude of medical, psychosocial, environmental, cultural, and systems events can challenge early relationship development. Early separation of baby and parent, postpartum medical issues in the postpartum period, family and job responsibilities, grief reactions and fear, poor communication with professionals, as well as restrictive policies and procedures, are but a few of the interfering variables that can affect robust relationship development.
The Infant and Family Centered Developmental Care (IFCDC) Standards address continuity from the hospital to the community.
The IFCDC standards emphasize the importance of collaboration with parents to ensure they are well-prepared to support their baby’s development both in the hospital and after discharge. Each NICU system should engage in collaborative efforts among team members, including parents and caregivers.
The focus should promote and ensure parents’ preparation for transition to community resources, which can be accomplished by providing competent and relevant physical, developmental, and psychosocial services throughout the hospital stay and into the community.
The IFCDC standards also emphasize the need for collaboration with follow-up and community providers who will support their families in the weeks and months after hospitalization.
Conclusion:
Continuity during the transition from intensive care to the family’s home and community presents neurophysiological, psychosocial, and behavioral challenges for both babies and their parents. These occur during a particularly vulnerable time, as the last trimester and the first 3-6 months represent a sensitive period of brain, behavior, and relationship development. Interventions in the hospital should focus not only on neurodevelopmental support and environmental protection but should also emphasize parental involvement in preparation for supporting their baby’s development after discharge. As delineated in the IFCDC standards, it is essential for the intensive care community to not only engage parents as team members and prepare them during hospitalization for post-discharge care, but also to ensure continuity of well-prepared community support and medical follow-up. Currently, the kind of intervention that addresses the specific needs of babies and their parents — early and often, during the first 3-6 months —is not consistently practiced in the United States. There is a need for appropriately trained providers who can sensitively and knowledgably address health, development, relationship, and mental health, development, relationship, and mental health issues for vulnerable families during this vulnerable period.
Since 7 October 2023, 47% of attacks on health care – 65 out of 137 – have proven fatal to at least one health worker or patient in Lebanon, as of 21 November 2024.
This is a higher percentage than in any active conflict today across the globe – with nearly half of all attacks on health causing the death of a health worker.
In comparison, the global average is 13.3%, based on the SSA’s figures from 13 countries or territories that reported attacks in the same period, 7 October 2023–18 November 2024 – among them Ukraine, Sudan and the occupied Palestinian territory (oPt). In the case of oPt, 9.6% of the total number of incidents has resulted in the death of at least one medical professional or patient.
According to the SSA, 226 health workers and patients were killed in Lebanon and 199 injured between 7 October 2023 and 18 November 2024.
In the same period, the SSA registered a combined total of 1401 attacks on health in oPt, Lebanon and Israel – 1196 in oPt, 137 in Lebanon and 68 in Israel.
Civilian health care has special protection
“These figures reveal yet again an extremely worrying pattern. It’s unequivocal – depriving civilians of access to lifesaving care and targeting health providers is a breach of international humanitarian law. The law prohibits the use of health facilities for military purposes – and even if that is the case, stringent conditions to taking action against them apply, including a duty to warn and to wait after warning,” said WHO Representative in Lebanon Dr Abdinasir Abubakar.
International humanitarian law states that health workers and facilities should always be protected in armed conflicts and never attacked. Health facilities must not be used for military purposes, and there should be accountability for the misuse of health facilities.
“There need to be consequences for not abiding by international law, and the principles of precaution, distinction and proportionality should always be adhered to. It’s been said before, indiscriminate attacks on health care are a violation of human rights and international law that cannot become the new normal, not in Gaza, not in Lebanon, nowhere,” said WHO Regional Director for the Eastern Mediterranean Dr Hanan Balkhy.
The majority of incidents in Lebanon impact health workers
The majority (68%) of incidents in Lebanon registered by the SSA impacted health personnel, a pattern seen repeatedly in the last few years, including in Gaza in the past year. In Lebanon, roughly 63% affected health transport and 26% affected health facilities.
Attacks on health care hit twice. First, when health workers lose their lives or when a health centre is obliterated, and again in the following weeks and months when the injured can’t be treated, those who are dependent on regular care don’t receive it and when children can’t be immunized.
“Casualty numbers among health workers of this scope would debilitate any country, not just Lebanon. But what the numbers alone cannot convey is the long-term impact, the treatments for health conditions missed, women and girls prevented from accessing maternal, sexual and reproductive health services, undiagnosed treatable diseases and, ultimately, the lives lost because of the absence of health care. That is the impact that’s hard to quantify,” said Dr Abubakar.
1 in 10 hospitals in Lebanon directly impacted
The greater the blow to the health workforce, the weaker the longer-term ability of a country to recover from a crisis and deliver health care in a post-conflict setting.
Lebanon is a lower middle-income country with a fairly advanced health system that’s been hit hard by multiple crises in recent years. After hostilities in Lebanon escalated in September 2024, the growing number of attacks on health have caused further strain on an already over-burdened system.
Today, the country’s health system is under extreme duress, with 15 out of 153 hospitals having ceased to operate, or only partially functioning. Nabatieh, as an example, one of Lebanon’s 8 governorates, has lost 40% of its hospital bed capacity.
“Attacks on health care of this scale cripple a health system when those whose lives depend on it need it the most. Beyond the loss of life, the death of health workers is a loss of years of investment and a crucial resource to a fragile country going forward,” Dr Balkhy concluded.
So far this year, between 1 January 2024 and 18 November 2024, a total of 1246 attacks on health care were registered globally, in 13 countries or territories, killing 730 health workers and patients and injuring 1255.
Note to editors
The Surveillance System for Attacks on Health Care (SSA), established in 2017 by the World Health Organization, is an independent global monitoring mechanism whose goal is to collect reliable data on attacks on health care and to then identify patterns of violence that inform risk reduction and resilience measures so that health care is protected. The SSA also provides an evidence base for advocacy against attacks on health care.
Skin-to-skin care helps newborn babies in many ways – brain development, regulating heart rate and body temperature, and bonding with their caregivers.
When a baby needs to be in the NICU, skin-to-skin care is especially important, but there can be challenges.
After a baby is born, skin-to-skin contact is a powerful tool to bond with your baby, improve their brain development, and help them regulate their heart rate and body temperature. But when a baby needs to be in the NICU, skin-to-skin care can be more challenging.
“After a routine delivery, moms are encouraged to have skin-to-skin care right away,” said Ajay Talati, MD, medical director at Regional One Health’s Sheldon B. Korones Newborn Center. “If the baby has to go straight to the NICU for treatment, that can’t happen.”
Challenges can remain once a baby is in the NICU, said Kelley Smith, NICU Nursing Manager. If a baby is on an oscillator, a mechanical ventilation device used to help premature or ill infants breathe, they are connected to tubing that has to stay at the same level as their incubator.
“With an oscillator, the tubing is very stiff – it can’t be bent,” Smith explained. “That makes it hard to move the baby into the parents’ arms for skin-to-skin care.”
The NICU team started looking for a solution and found it in an innovative new use for a piece of equipment that is commonly found in other parts of the hospital.
Cardiac chairs are typically used to help cardiac and stroke patients rest in an optimal position. Because the chairs can go up and down, recline, and even lay flat, Smith and Assistant Nursing Manager Heather Burgess saw an opening to use them in the NICU for skin-to-skin care.
“With this chair, we can have the mom or dad sit in the chair and raise the chair to the level of the oscillator’s tubing,” Smith said. “It makes it easier to get the baby out of the incubator.”
Skin-to-skin care helps babies in a number of ways. “After a routine delivery, moms are encouraged to have skin-to-skin care right away,” said Ajay Talati, MD, medical director at Regional One Health’s Sheldon B. Korones Newborn Center.
A generous Regional One Health Foundation supporter stepped up to donate a cardiac chair to the NICU, and the nursing team is now educating patients about its use and making it available to all families that can benefit. Along with families whose baby is on an oscillator, moms who have had a C-section are finding the chair useful.
“Many moms can’t sit upright for 12 to 24 hours after a C-section, and it can be uncomfortable trying to get in and out of a chair,” Dr. Talati said. “We use it whenever a mom or baby needs it. It’s great for when a baby is too sick to be lowered or when a mom has pain after a C-section.”
Burgess said finding a solution was important to the NICU team because skin-to-skin care has many proven medical benefits for babies and moms.
For the baby, skin-to-skin care helps regulate body temperature, breathing and heart rate and improves brain development, Burgess said. For moms, skin-to-skin can help improve breastmilk production, regulate postpartum hormone balance, and reduce anxiety and stress.
There’s also the matter of bonding, which applies not only to new moms, but to all caregivers.
“We encourage parents to do skin-to-skin care in the first week of their baby’s life, especially for very small, very sick babies,” Smith said. “When you have a baby in the NICU, you’re anxious and afraid, so sometimes parents wait until they go home. That can be a missed opportunity for bonding. The sooner we start skin-to-skin, the better off the family unit will be.”
Dr. Talati, Smith and Burgess have seen the value of skin-to-skin care on multiple occasions.
Moms, dads and other caregivers can all take part in skin-to-skin care. “We encourage parents to do skin-to-skin care in the first week of their baby’s life, especially for very small, very sick babies,” NICU Nursing Manager Kelley Smith said.
The first mom to use the chair had impressive results. “Her baby came off the oscillator the next day!” Smith said. “It’s amazing to see. We’ll have babies on an oscillator with an oxygen saturation in the low 90s…then they do skin-to-skin and it shoots up to 100!”
Burgess said another mom provided skin-to-skin care in the NICU every day, and it contributed to her baby getting healthy enough to go home much sooner than originally expected.
Dr. Talati said there is plenty of evidence behind those individual experiences. Factors like better milk production and better feeding, the ability to regulate body temperature and heart rate, and increased oxygen saturation can all help a baby get stronger.
“It’s a lot of little things that can add up to the baby making faster progress toward going home,” he said. “We hope it can speed that up and we can help more babies go home sooner.”
Have you ever wondered how the Neonatal Resuscitation Program (NRP) guidelines are created—and more importantly, who decides what changes and why? In this episode, we take you behind the scenes of the science and collaboration that shape NRP. From the rigorous evidence review conducted by the International Liaison Committee on Resuscitation (ILCOR) to how these findings are translated into bedside practice, you will learn exactly how research becomes reality.
Together, Dr. Gary Weiner and Amanda Williams break down the multi-layered process of evidence evaluation, guideline development, and educational translation, while highlighting the critical role nurses play in shaping the NRP used daily. Whether you are new to NRP or a seasoned instructor, this episode will inspire you to see the program through a whole new lens and recognize the power of your voice in shaping neonatal care.
Discover why NRP is more than a textbook—it is a living, breathing, global collaboration grounded in science and strengthened by the people who use it.
For the past 10 years, I have worked as a pediatrician and neonatal hospitalist in multiple Level 2 NICUs across Georgia and other states. Over time, I have come to a realization that I cannot ignore: there is a significant public health imperative—and a gap in equitable access—when it comes to developmental and family support services in Level 2 NICUs.
Level 3 and 4 NICUs often have consistent access to lactation consultation, feeding therapy, physical and occupational therapy, and even music therapy. In Level 2 settings, those services are less consistently available—sometimes absent altogether. This discrepancy has a lasting impact on infants and families.
The common perception is that if a baby is born at or after 32 weeks and weighs ≥ 1500 grams—the typical admission criteria for Level 2—that they have “made it.” But research tells a different story. Moderately and late-preterm infants, even those who meet Level 2 thresholds, remain at high risk for readmission, feeding difficulties, developmental delays, and long-term neurodevelopmental challenges (1-4). Prematurity in any form is not a short-term hurdle—it is a lifelong risk factor that requires intentional support from the start.
So, why are we not introducing key developmental concepts, early intervention techniques, and consistent family education into Level 2 NICUs? Why are we not equipping nurses and families with the same foundational knowledge and access to services that higher-level NICUs utilize?
The NICU is not only a place for acute medical stabilization—it is a unique window of opportunity to shape lifelong outcomes. Families in Level 2 units should see themselves as vital participants in their baby’s success and be empowered with the tools to support feeding, bonding, sensory development, and early learning before discharge. Nurses should have access to training that enables them to integrate trauma-informed, developmental care principles into their daily practice, even when an entire therapy team is not available on the unit.
I believe it is time to establish a Task Force on Level 2NICU Care, bringing together neonatologists, neonatal hospitalists, nurses, therapists, public health professionals, and parents, to examine the current state of developmental and family support services in these units, identify barriers, and develop scalable strategies for improvement.
Potential strategies include: • Standardized education for nursing staff on early-intervention techniques, family engagement, and trauma-informed developmental care.
• Telehealth access to lactation consultants, feeding/ occupational/physical therapists, and other specialists when on-site resources are limited.
• Parent-education toolkits that cover feeding, developmental milestones, safe sleep, and the importance of follow-up and early-intervention services.
• Structured discharge planning that includes referrals to early-intervention programs and developmental follow-up clinics for all eligible infants.
The public-health impact of closing these gaps is profound. If we can equip Level 2 NICUs with consistent developmental care education and tools, we can reduce readmissions, improve neurodevelopmental outcomes, and strengthen families’ ability to support their child’s growth and resilience.
The babies in Level 2 NICUs deserve the same intentional approach to developmental care as those in higher-level units. They may have “made it” past the highest-risk thresholds, but they have not yet crossed the finish line. We can—and must—do better.
Now is the time to act. Clinicians, hospital leaders, and policymakers must collaborate to prioritize Level 2 NICUs in state and national maternal-child health agendas. By identifying service gaps, piloting telehealth and staff-training models, and measuring family-centered outcomes, we can transform Level 2 NICUs from sites of short-term stabilization into launchpads for lifelong development, resilience, and equity.
Introduction: The huge prevalence of neurodevelopmental disorders underscores the necessity for novel, comprehensive prevention strategies for neuroprotective intervention, particularly in preterm infants. The COVID-19 pandemic has accelerated the transformation of healthcare services, emphasizing the use of digital resources. Given the rapid brain development in infants in the first 1,000 days of life and the demonstrated impact of adaptive neuroplasticity, the implementation of early and ecological interventions are essential for supporting optimal neurodevelopment in this vulnerable population. Aim of this project is to develop a digital tool for parent-led parent-based intervention and assess its feasibility and accessibility.
Materials and methods: We collected evidence on early intervention strategies for preterm infants through a non-systematic review of current literature to develop the platform and created an ad-hoc questionnaire to evaluate the tool’s feasibility and acceptability in our neurological follow-up.
Results: “NE@R” is a digital platform designed to support neurodevelopment through parents-delivered play. The platform offers evidence-based information, videos, and practical activities to enhance motor, cognitive, social, and language development at each developmental phase. We introduce the resource in our clinical setting and collect 100 preterm infants’ families feedback. The majority of parents reported finding the resource beneficial, with many expressing increased confidence in supporting their child’s development.
Discussion: Preterm babies families’ support represents a precious field of intervention both for parents and infants at risk. “NE@R” has proven to be an effective, low-cost tool within our follow-up program, aligning with the principles of family-centered care.
Patricia Odero is an innovation facilitator extraordinaire based in Nairobi, Kenya, working for The Duke Global Health Institute. Patricia is trained in Medicine, Business and Social innovation and uses her skills and experience to help entrepreneurs in West Africa and beyond with funding and growth. She talks about the importance of networks, particularly in health entrepreneurship – long-term relationships and support programmes for organisations of different sizes and stages. Patricia has great advice for entrepreneurs and really interesting stories from the field. You can follow Patricia on Twitter @TrishOdero, BMJ Innovations @bmjinnovations and podcast host Helen Surana @hjsurana.
BMJ innovations is grateful to the World Innovation Summit for Health WISH for making this podcast series possible.
Takeaways
Children born preterm were significantly less likely to complete high school or university compared with full-term peers, according to a large Quebec-based study.
Non-graduation rates were highest among those born extremely preterm (40.2%) and lowest among full-term births (27.1%).
Low maternal education, male sex, unmarried parents, and low neighborhood socioeconomic status were major predictors of poorer academic performance.
The odds of completing high school are reduced among children born preterm vs full-term, according to a recent study published in JAMA Network Open.
Approximately 10% of infants are born preterm, which may cause early exposure to noxious factors and influence brain development, challenging neurodevelopment and mental well-being. Additionally, socioeconomic factors often prevent children from accessing support systems that can mitigate disabilities.
“Few researchers have conducted studies on long-term educational outcomes across the full spectrum of preterm birth using large population-based cohorts that account for other health-related determinants and socioeconomic factors,” wrote investigators.
Assessing preterm birth and education
The birth cohort case-control study was conducted to assess the impacts of preterm birth and sociodemographic factors on educational outcomes. Live preterm births in Quebec, Canada, between January 1, 1976, and December 31, 1995, were included in the analysis.
Each preterm individual was matched with 2 full-term patients, defined as 37- to 42-weeks gestation. Exclusion criteria included multiple pregnancies, triplet births, and death between 1976 and 2019 without Quebec Ministry of Education records.
Extremely preterm birth was defined as under 28 weeks, very preterm as 28 to under 32 weeks, and moderate-to-late preterm as 32 to 37 weeks. Forty-three years of follow-up data was obtained from administrative databases.
High school performance was measured using the final high school average recorded in the Quebec Ministry of Education database, using marks obtained in grades 10 and 11. Covariates included year of birth, birth order, sex, stillbirth history, primary language, matrimonial status at birth, maternal education, and neighborhood socioeconomic status.
Participant characteristics and academic performance
There were 297,820 participants included in the final analysis, 0.6% of whom were born extremely preterm, 4.4% very preterm, 27.9% moderate-to-late preterm, and 67% full-term. Under 11 years of maternal school were reported in 20.6%, 24%, 23%, and 20.3%, respectively.
Preterm birth groups also more often reported primary languages other than French or English, and more recent birth years were reported in those born extremely preterm. Overall, the rate of preterm births in Quebec rose from 4.6% between 1976 and 1980 to 6.1% between 1991 and 1995.
Significant differences were not reported in high school performance based on preterm birth, with final mean scores of 69.4, 70.2, 70.7, and 71 for extremely preterm, very preterm, moderately preterm, and term births, respectively. However, rates of not graduating from high school were 40.2%, 34.4%, 31.1%, and 27.1%, respectively.
This data indicated significantly reduced odds of high school graduation from preterm birth. These patients were also more likely not to graduate from university. Rates included:
83.3% for extremely preterm
80.2% for very preterm
78.2% for moderately preterm
75.8% for full-term
Socioeconomic and demographic influences
In regression analyses, a B coefficient range of 0.15 to 1.45 was reported for the link between preterm status and final high school average. Low maternal education, male sex, low neighborhood socioeconomic status, not being first-born, and mother not married had the most significant B coefficients for low average marks of 4.43, 2.84, 2.30, 2.30, and 1.98, respectively.
These results indicated reduced odds of graduating from high school or university among children born preterm vs their full-term counterparts. Investigators concluded long-term follow-up is needed in both health care and education among individuals born preterm.
This data highlights the importance of preterm birth prediction. Identifying individuals at an increased risk of preterm birth may be more accurate through the use of neighborhood-level indices, according to Daniel L. Kuhr, MD, third-year fellow in maternal fetal medicine at the Icahn School of Medicine at Mount Sinai.
According to Kuhr, an increase in prediction was only noticeable when including individual patient characteristics. This highlights a need to evaluate other social determinants of health that may influence preterm birth risk.
“The best thing that you can do is take a really good history when you meet a patient at the beginning of pregnancy, and really make sure you can get accurate gestational ages of delivery when possible, because we do know that history of a prior spontaneous preterm birth is also a risk factor,” said Kuhr.
One of the first things that comes to mind when I think about the holidays is…food. Whether I’m crowded around a dinner table with family and friends or pulling my favorite cranberry and pear pie out of the oven to take to a holiday gathering, there’s something special about breaking bread with the ones you love.
Food, it seems, has a language of its own. In communities across the globe, food has a unique way of bringing people together. And this holiday season, we wanted to help you connect with your friends, family and with the World Relief community by sharing a few recipes from around the world in our new ebook — Breaking Bread Across Borders: Global Recipes from Refugee Kitchens.
This ebook is filled with stories and recipes from immigrants who are part of World Relief Western Washington’s Commercial and Teaching Kitchen — an innovative program that connects members of the community with their immigrant neighbors through workshops and events led by immigrant chefs while providing low-cost commercial kitchen space for immigrant caterers to rent and run their businesses.
For women like Katya, who owned a bakery when she lived in Ukraine, the commercial and teaching kitchen is a way to bring people joy while pursuing her passion here in the U.S. “I love to bring joy to people with my baking,” Katya said. “You become a piece of people’s special events [when you bake for them]. You become a piece of the joy.”
The formation of the family is interrupted following a Neonatal Intensive Care Unit (NICU) admission, and fathers report experiencing delayed infant bonding due to unit barriers and separation. Fathers state comfort with early infant bonding through language, fearing physical contact with the sick newborn. During hospitalization, active engagement supports ongoing infant/parent vocalization and infant stabilization.
Purpose:
This prospective descriptive pilot study explored the infant’s physiological response to the father’s voice during a live reading activity.
Methods:
After Institutional Review Board approval and consent, 27 infant/father dyads were observed pre/post and during a live reading activity. All infants were in private rooms and positioned supine in open cribs, adjusted to 36 weeks or greater postmenstrual age, in a 34-bed Level III NICU in the Midwest. Outcome measures included cerebral oxygenation, oxygen saturation, heart rate (HR), and respiratory rate. Infants were monitored for 30 minutes prior to father reading, 10 minutes during and 30 minutes post reading.
Results:
A clinically significant increase in cerebral oxygenation was noted, based on near-infrared spectroscopy readings in response to the father’s voice. Most infants had HR stabilization during the father’s active reading time frame.
Implications for Practice and Research:
NICU nurses and staff can encourage a father’s engagement through speaking or reading to their infant. Nursing staff can promote verbal engagement between father–infant dyads by role modeling this behavior at the bedside. NICUs can provide books for families to further encourage exposure to father’s voices. Further study of premature infants at earlier chronological and adjusted ages is needed.
Anxiety disorders are defined and classified in diagnostic systems like the Diagnostic and Statistical Manual of Mental Disorders (DSM, currently version IV-TR, American Psychiatric Association) and the International Classification of Diseases (ICDS) (ICD, currently version 10, World Health Organization). Many anxiety disorders have clinical aspects across multiple systems, such as high levels of anxiety, physiological anxiety symptoms, and behavioural problems such as severe avoidance of fearful situations, and related discomfort or impairment. However, there are distinctions, and it’s worth noting that narrowly classified anxiety disorders like panic disorder, agoraphobia, and subtypes of certain phobias have a lot of phenotypic variety or heterogeneity.
From time to time, all children have worries and fears. However, anxiety in children can sometimes cross the line to a disorder that prevents them from normal everyday concerns doing the things they need to do. It may even prevent them from properly understanding life.
How do we determine whether the child’s worries and fears are more than just passing thoughts?
Here are a few questions to ponder:
• Do they express fear or anxiety on a regular basis, for weeks at a time?
• Is it difficult for them to sleep at night? Do they seem abnormally drowsy or exhausted during the day?
• Is it difficult for them to concentrate?
• Do they seem angry or easily irritated?
Anxiety disorders can manifest itself in a variety of ways in children. Some of the most common are:
Generalized Anxiety Disorder (GAD)
GAD children are overly concerned about a variety of things, including school, their own safety and health, the health of family members and friends, money, and the security of their families. The list could go on indefinitely. A child suffering from GAD may constantly imagine the worst-case circumstance. These anxieties may induce physical symptoms in children with GAD, such as headaches and stomach-aches. Because they are so burdened by their fears, your child may isolate themselves, avoiding school and friends.
Panic disorder
A panic attack is a sudden, acute experience of worry that occurs for no particular reason. The child’s heart may race, and he or she may be out of breath. The child may have tremors, dizziness, or numbness. (If the child is hyperventilating, encourage them to breathe gently and deeply.) Breathing through a brown paper bag can be beneficial.) Panic disorder is diagnosed when the child has experienced two or more of these episodes and is preoccupied with fears of them happening again.
Separation Anxiety Disorder (SAD)
Separation anxiety affects all children to some extent. It’s a normal developmental stage for babies and toddlers. Even older children, especially in new situations, may become clingy with their parents or caretakers. Separation anxiety disorder may affect older children who become especially upset when leaving a parent or another close relative, who have difficulty calming down after saying goodbye, or who become highly homesick and disturbed when away from home at school, camp.
Social phobia
In typical, everyday social circumstances, a child with social phobia experiences extreme anxiety and self-consciousness. This isn’t just a case of timidity. When talking with classmates, answering a question in class, or doing other common activities that require interacting with people, the socially anxious child is afraid of embarrassing themselves. This fear may prevent your child from attending school and participating in extracurricular activities. In severe instances, young children may even be unable to speak.
These are the type of anxiety disorders and their assessments on the children, to be considered by the parents, and treat their children accordingly.
As December arrives—a month shaped by reflection, generosity, and deeper emotions—the Neonatal Womb Warriors community is reminded that kindness is one of the most powerful tools we have for calming fear and nurturing resilience. Many of us began life in fragile circumstances, where uncertainty, hope, and anxiety coexisted side-by-side. Because of that beginning, we understand how small comforts can soothe big worries. The neonatal world teaches us that healing happens moment by moment, and that gentleness, patience, and compassion are essential for helping families and children navigate anxious seasons.
For families with babies in the NICU, the holidays can intensify feelings of overwhelm, isolation, or emotional strain. Parents may carry silent anxiety about outcomes, siblings may sense stress without understanding it, and clinicians may feel the weight of supporting so many families at once. A simple act—sharing a grounding story of your own journey, sending a message of reassurance, offering a listening ear, or just showing presence without expectation—can ease the mental load for someone facing long days beside an incubator. These gestures remind families that they are not alone in managing the fear that often accompanies the NICU experience.
This month, we invite every Womb Warrior to choose a way—large or small—to give back emotionally or practically. Create a comfort bag for parents spending the holidays in the NICU. Donate time to a local children’s charity, NICU support network, or preemie nonprofit. Offer to read aloud or do a calming activity with siblings who may be feeling anxious. Volunteer at a community event that supports vulnerable families, or simply check in on someone who has been quiet. These actions not only lift others but also model for children that kindness is a powerful antidote to anxiety.
The strength of our community lies in its shared empathy—preemie survivors who have lived through uncertainty, NICU families who have learned courage through adversity, and clinicians who bring dedication and steadiness to every fragile moment. When we turn these lived experiences into acts of compassion, we help others feel grounded, less overwhelmed, and more hopeful. Kindness becomes the bridge between anxiety and reassurance, especially during a season that invites us to slow down and connect.
As we move through December, we encourage each of you to commit to one intentional act of kindness each week. Whether it’s offering comfort to a NICU family, expressing gratitude to a clinician, volunteering in your community, or choosing patience with yourself or your child during moments of stress—every act matters. Together, we carry forward the heart of Neonatal Womb Warriors: grounded in hope, strengthened by compassion, and united in helping families and children navigate anxiety with courage and care.
The whatifs/ A book to help kids overcome anxiety/bedtime story
What if my dog run away? what if I forget my homework? what if the sun stops shining? What if my crayon breaks? Will Cora be able to change her worry-filled thoughts into hopeful ones? Find out in this timely picture book about overcoming anxiety.
Healthcare in Senegal is a center topic of discourse in understanding the well-being and vitality of the Senegalese people. As of 2008, there was a need to improve Senegal’s infrastructure to promote a healthy, decent living environment for the Senegalese.
Additionally, the country needs more doctors and health personnel, particularly general practitioners, gynecologists, obstetricians, pediatricians, pulmonologist, and cardiologists. In fact, Senegal has seven doctors per 100,000 citizens, while 32% of rural citizens have no access to medical care at all. Moreover, there is a strong need to have more of these personnel in rural areas: in 2008, Senegal had only twenty full-fledged hospitals, seven of which are in Dakar.
From approximately 1905 to the present, there have been significant shifts in Senegal’s healthcare system, the system’s structures, specific diseases that are problematic in Senegal, as well as issues affecting women and children and access to healthcare in the country. As of 2019, there were 1,347 medical facilities, including 20 major hospitals.
GLOBAL PRETERM BIRTH RATES – Senegal
Estimated # of preterm births: 10 per 100 live births
Problem Statement: Neonatal Intensive Care Unit (NICU) trainees experience high intensity situations under suboptimal physiologic and psychologic conditions that can lead to burnout and/or secondary traumatic stress. The mental health of NICU fellows can have significant impact on their well-being and the quality of patient care they provide. The overall goal of this project is to improve Neonatal Fellow mental health and well-being in a level 3 NICU by using Trauma Informed care (TIC) principles to identify needs that may warrant connection to further resources.
Abstract:
Methods:
Key stake holders were identified: the ACGME director, the fellowship program director, the associate program director, the chief fellow, the psychologist, the fellow cohort, division chief, lead NNP, and the program coordinator. We aimed to develop a wellness curriculum and standardize the frequency of sessions, duration of sessions, attendance of sessions, confidentiality, location and topics. Key drivers rooted in the 6 principles of TIC became the foundation of the topics explored during the Wellness Sessions. These six principles / primary are 1. Safety, 2. Trustworthiness and Transparency, 3. Peer Support, 4. Collaboration and Mutuality, 5, Empowerment, voice, and choice, 6. Cultural sensitivities. These promoted the following standardized topics: Crucial conversations with mentors, Performance anxiety, Debrief challenging cases, debrief death, Navigating personal relationships (motherhood, significant other, daughter/son), Work life balance, Individualizing wellness, Cognitive behavioral strategy for stress management. A force field diagram was the QI tool used to mediate conversations to gain approval for this Wellness curriculum pilot. Driving forces in support of this pilot were having a dedicated NICU psychologist, ACGME recommendation for embedded Wellness training, fellow interest, previous match history, program evaluation demonstrating a gap for wellness training and existing private fellow office space. Restraining forces included scheduling time away from board preparation didactics, patient care and research duties, 360 degree buy in, post-call protected time, literacy of NICU psychologist role, and human bias to new process. Our outcome measure is compliance with monthly meetings characterized by completed monthly sessions from November 2023 to April 2024. The process measure is compliance with attendance for fellows that desired to attend the wellness session and not encounter barriers.
Results:
In the initial 6 months implementation period from November 2023 to April 2024 there was 30% compliance with monthly meetings. PDSA cycles revealed the challenges to completing a session. These included the available protected didactic times were filled with other lectures and case conferences, preparation for In-training-exams (ITE’s), research timelines, graduating fellow interviews, schedule gaps for anticipated and unanticipated medical leaves, and fellow graduation exit procedures. Compliance for attendance of the fellows conflicted with patient care duties and lack of commitment to protected time away from the NICU. Qualitative feedback from fellows was in support of establishing the permanence of this wellness curriculum and they specifically appreciated the topics and the time to pause and reflect on their experiences. Fellows’ feedback included: “mental health sessions are equally as important as the pathophysiology lectures,” the curriculum prioritizes “resetting the mindset more positively” and “improve work-related satisfaction.” This feedback, the start of the new chief fellow term, and persistent advocacy to establish this wellness curriculum enabled this pilot to continue for an additional 6 months. The frequency of sessions has increased in collaboration with program director approving bimonthly sessions.
Conclusions:
Implementation of a fellow wellness program was met with initial resistance, but over time has proven beneficial in fellow satisfaction and performance leading to increased support from key stakeholders, increased frequency of scheduled sessions and reduction in barriers to allow for fellow attendance. Future direction is to incorporate fellow wellness curriculum into monthly didactic schedule and standardize a curriculum to be replicated.
***** Please See Neonatology Today September 2025 Edition to view numerous interesting and informative Abstracts selected by Gravens By Design from the recent 38th Annual Gravens Conference on the Environment of Care for HighRisk Infants and Their Families
The latest statistics from the MSAS reveal a critical shortfall: there is currently only one midwife available for every 1,197 women of reproductive age.
This shortage has left numerous health centers, especially in rural areas, operating without qualified personnel capable of providing prenatal care or safely assisting with deliveries.
In some of the country’s most isolated communities, pregnant women are still forced to travel dozens of kilometers in search of professional medical assistance.
This persistent gap in healthcare access continues to put adolescent girls, expectant mothers, and newborns at risk, especially when it comes to managing high-risk pregnancies.
In response, the government has initiated a targeted recruitment drive under the broader SWEDD+ program—an initiative for Women’s Empowerment and the Demographic Dividend in West Africa.
The project aims to recruit a total of 500 midwives across 11 of Senegal’s most vulnerable regions, where the shortage is most pronounced.
The newly announced recruitment of 220 midwives marks the first wave of this effort, which is supported by key international partners including the World Bank and the United Nations Population Fund (UNFPA).
Beyond simply filling vacant roles, the goal is to ensure that skilled healthcare professionals are present and retained in the country’s most neglected areas—regions often bypassed by young professionals due to poor infrastructure and difficult living conditions.
Authorities hope this measure will significantly reduce maternal mortality, limit preventable childbirth complications, and improve access to essential services for women and adolescents.
However, health experts warn that recruitment alone will not be enough. For the initiative to succeed in the long term, newly deployed midwives will require proper housing, transportation, equipment, and incentives to remain in rural posts.
Despite these challenges, the decision signals a shift in policy direction. While the number of recruits may not fully meet the country’s needs, the move represents a concrete and long-overdue commitment to rebuilding Senegal’s maternal healthcare system from the ground up.
The World Health Assembly has officially designated November 17 as World Prematurity Day! The recent WHO endorsement is a major step forward – calling on governments around the world to prioritize preterm birth in their national health agendas.
“As one of the founding organizations of World Prematurity Day in 2008, we at GFCNI are deeply proud to see it officially recognized by the World Health Organization,“ says Silke Mader. “This milestone is a tribute to our tireless efforts together with parent and patient organizations, healthcare professionals, and advocates around the world. A heartfelt thank you to Doris, whose dedication made this endorsement possible. Together, we have turned a vision into a worldwide movement for preterm babies and their families.”
“This is truly a huge milestone for the global movement for premature babies,” adds Doris Mollel, founder of the Doris Mollel Foundation in Tanzania, whose tirelessly advocacy, supported by the Tanzanian government, has been pivotal in bringing global attention to the needs of preterm infants. “This is just the beginning. Together, we are building a future where every child has a fighting chance, and every life matters.”
The latest statistics from the MSAS reveal a critical shortfall: there is currently only one midwife available for every 1,197 women of reproductive age.
This shortage has left numerous health centers, especially in rural areas, operating without qualified personnel capable of providing prenatal care or safely assisting with deliveries.
In some of the country’s most isolated communities, pregnant women are still forced to travel dozens of kilometers in search of professional medical assistance.
This persistent gap in healthcare access continues to put adolescent girls, expectant mothers, and newborns at risk, especially when it comes to managing high-risk pregnancies.
In response, the government has initiated a targeted recruitment drive under the broader SWEDD+ program—an initiative for Women’s Empowerment and the Demographic Dividend in West Africa.
The project aims to recruit a total of 500 midwives across 11 of Senegal’s most vulnerable regions, where the shortage is most pronounced.
The newly announced recruitment of 220 midwives marks the first wave of this effort, which is supported by key international partners including the World Bank and the United Nations Population Fund (UNFPA).
Beyond simply filling vacant roles, the goal is to ensure that skilled healthcare professionals are present and retained in the country’s most neglected areas—regions often bypassed by young professionals due to poor infrastructure and difficult living conditions.
Authorities hope this measure will significantly reduce maternal mortality, limit preventable childbirth complications, and improve access to essential services for women and adolescents.
However, health experts warn that recruitment alone will not be enough. For the initiative to succeed in the long term, newly deployed midwives will require proper housing, transportation, equipment, and incentives to remain in rural posts.
Despite these challenges, the decision signals a shift in policy direction. While the number of recruits may not fully meet the country’s needs, the move represents a concrete and long-overdue commitment to rebuilding Senegal’s maternal healthcare system from the ground up.
Was your baby born more than 3 weeks early? Premature development differs from full-term, but there’s no need to worry! Let’s explore effective ways to understand and support your baby’s growth and milestones. Premature babies are often born with more extended (straight) positions, while full-term babies get a curled up (flexed) feeling from being in the womb longer. Babies need both flexion and extension to help their motor skill development. Try these activities to aid your preemie’s physical growth and work on their flexion. Always consult your healthcare provider for personalized advice. • Swaddling: Helps bring your baby’s arms to the middle, providing comfort and aiding in muscle development. • Side Lying: Reduces gravity’s impact, making it easier for your baby to move their arms and legs. • Bringing Arms and Legs to Midline: Encourages flexion by helping your baby bring their limbs to the center of their body. • Tummy Time: Strengthens neck, back, shoulder, and core muscles crucial for overall development.
👪 ABOUT PATHWAYS.ORG Pathways.org is a non-profit organization that provides free, trusted resources so that every parent is fully empowered to support their child’s development. Our milestones are supported by American Academy of Pediatric findings. Our resources are developed with and approved by expert pediatric physical and occupational therapists and speech-language pathologists.
If your country or region isn’t yet listed, we’d love your help expanding this network. Share your local preemie-family organization, NICU support group, or foundation by contacting us at NeonatalWombWarriors@gmail.comTogether, we can make sure every family and their communities — no matter where they are — are able to gain needed support. We are stronger together.
Having a baby in the hospital NICU is a very stressful time for all members of a family, including big brothers and sisters. Siblings often feel confused, anxious, or even left out during a NICU stay. Children look to adults for reassurance, so it’s important to guide them through the experience with honesty, love, and consistency.
This guide offers simple, practical tips for NICU sibling support that help kids feel included, valued, and secure during this challenging time.
Helping Children Cope with a NICU Stay
BE CONSISTENT
Maintaining normal routines like bedtime, meals, and school helps young children feel safe. Consistency is especially important during a time when so much else is changing.
SET ASIDE SPECIAL TIME
Even small moments of connection, like reading a bedtime story, a short walk, or a chat in the car, can go a long way. Your time and attention matter more than perfection.
ASK FAMILY AND FRIENDS FOR HELP
Don’t be afraid to lean on your support system. People want to help, but they don’t always know how. Let them know what you need. Ask friends or family to help with school drop-offs or meals. Giving others a chance to help allows you to show up more fully for your children.
SURROUND THEM WITH FAMILIAR PEOPLE
If you have family members and friends providing child care, have them come to your home as much as possible. With so many changes, having a known and trusted adult around will help younger children cope, especially if they have a difficult time being separated from mom and dad. Familiarity offers comfort when parents are spending long hours at the hospital.
ADAPT THEIR DAILY ROUTINES
Routines are an important part of helping children cope with the NICU. You may have to temporarily change up your child’s routines to align with having a baby in the NICU. If your usual family dinners are now spent at the hospital, try shifting that special time to breakfast or bedtime instead. Flexibility can help kids still feel connected.
LEAVE NOTES OF LOVE
Leave your children love notes and messages when you have to be away. You may even sign some messages from the baby: “I am so lucky to have you as my big sister!” This can help them feel connected to the baby, especially if they can’t visit them.
CELEBRATE THEI ROLE AS BIG BROTHER OR SISTER
Remind siblings how important they are. Make a list of all the things your older children can do that the new baby can’t do and share it with them. Talk about their role in the family and how they will be helping to teach the new baby about these things.
ENCOURAGE YOUR CHILDREN TO TALK ABOUT THEIR FEELINGS
Even if they don’t ask, make time to talk. Let them know that it is okay if they are feeling sad, angry, lonely or frustrated. Let them know that they can tell you if they feel like they need you to spend some time with them. Create space for your children to talk about how they’re feeling by asking simple questions like: “What was the best part of your day?” or “Is anything making you feel sad or worried today?” Let them know it’s okay to feel all their feelings, and that you’re always there to listen.
LET THEM ASK QUESTIONS
Children often have big imaginations and need help making sense of what it means that the baby is in the NICU. Giving them age-appropriate, honest answers can ease their fears. For example: “The baby is in a special place where doctors are helping them get stronger.”
What are they worried about? What do they think might happen? Let their questions guide your conversations.
Model Coping and Resilience
Kids learn by watching you. Show them that it’s okay to be sad or overwhelmed, and that those feelings don’t last forever. Let them see you ask for help, take breaks, and care for yourself.
You Are Not Alone
The NICU experience can be tough on siblings, but it can also bring families closer. The most important thing we can do for our children is to give them support, encouragement, information and most of all reassurance that they are still important members of the family. With thoughtful support and simple routines, you can help your children feel secure, seen, and loved during this time.
The purpose of this research is to evaluate how AI integration in nursing education influences educational and practice performance outcomes, and to understand the roles of technological acceptance and institutional support in this process. Issue: AI’s role in nursing education and practice is not fully understood, particularly in terms of its effects on performance and the barriers to its effective implementation.
Method
A sample of 500 participants was surveyed, and data was analyzed using Smart-PLS 4.0 to assess the direct, indirect, and moderating effects between variables like AI integration, performance outcomes, and institutional factors. Results showed significant positive relationships between AI application in practice and nursing performance, with technological acceptance acting as a strong moderator.
Findings
AI integration in nursing education positively affects nursing performance (p < 0.001). Technological acceptance significantly enhances both educational and clinical outcomes, with interaction effects between technological acceptance and AI integration improving performance (p < 0.001).
Research policy implications
Policy should focus on supporting AI adoption in nursing curricula, with investments in faculty training, technological infrastructure, and fostering technological acceptance to maximize AI’s benefits in healthcare settings.
Conclusion
AI integration is crucial for advancing nursing education and practice, with technological acceptance and institutional support playing key roles in successful AI adoption. The findings underline the importance of targeted policy initiatives to foster these elements.
Introduction
Artificial Intelligence (AI) is rapidly transforming healthcare and nursing, providing new opportunities for education and practice. The integration of AI in nursing education is reshaping the way nursing curricula are developed, while the application of AI in clinical settings is enhancing the efficiency and accuracy of patient care. Despite these advancements, the impact of AI on global nursing education and practice remains inadequately explored, with few studies addressing both its benefits and challenges. This research aims to provide a comprehensive understanding of how AI integration in nursing education influences nursing performance, both in academic and clinical settings, and how AI applications in practice improve patient outcomes and care efficiency (Iqbal et al., 2025)
The adoption of AI in nursing education and practice is growing at an unprecedented rate, offering tools that range from curriculum enhancement through AI-driven learning tools to decision support systems (DSS) in clinical settings. AI is revolutionizing nursing by providing advanced technology for clinical training, decision-making, and patient monitoring (Chowdhury et al., 2021; Rana et al., 2024). However, the integration of AI in nursing education is often challenged by factors such as curriculum development, technology access, and the need for comprehensive training. Similarly, in clinical practice, the application of AI for clinical decisions and patient monitoring is reshaping nursing roles, yet concerns remain about how these technologies affect nursing practice performance (Denecke et al., 2020; Iqbal et al., 2023, 2024). Despite these changes, few studies have explored how these technological advances impact both nursing education and clinical performance in a holistic manner.
Although AI is increasingly being implemented in nursing education and practice, there is a lack of comprehensive research examining the direct effects of AI integration on nursing education performance (NEP) and nursing practice performance (NPP). Moreover, the factors that moderate or mediate the influence of AI such as technological acceptance, institutional support, and infrastructure have not been fully investigated. Understanding how these variables interact can provide valuable insights into the effectiveness and challenges of AI implementation in nursing.
These main three main research questions are:
1. How does AI integration in nursing education (curriculum design, technology access, and clinical training) influence nursing education performance, including academic performance, skill development, and clinical competency?
2. In what ways do AI applications in nursing practice (clinical training, decision support, and patient monitoring) affect nursing practice performance, particularly patient outcomes, satisfaction, and clinical accuracy?
3. How do factors such as technological acceptance and institutional support mediate and moderate the effects of AI integration and application in nursing education and practice?
These main three main research objectives are:
1.To examine the impact of AI integration in nursing education on nursing education performance (NEP).
2. To assess how AI applications in nursing practice affect nursing practice performance (NPP).
3. To analyze the role of technological acceptance and institutional support in moderating and mediating the relationship between AI integration and performance outcomes in nursing education and practice.
This study will provide crucial insights into how AI integration in nursing education and practice affects various performance outcomes, offering actionable recommendations for educators, healthcare policymakers, and technology developers. By exploring the moderating and mediating effects of technological acceptance and institutional support, the research will help identify strategies to overcome barriers to effective AI adoption in nursing. The findings will also contribute to the development of a conceptual framework for evaluating AI’s role in nursing education and practice, promoting more effective and sustainable implementation of AI in these fields.
This study will be conducted using Smart-PLS 4.0 to analyze the relationships between AI integration in nursing education and practice and its impact on nursing performance outcomes. The research will include an examination of the independent variables (AI integration in education and practice) and their effects on the dependent variables (nursing education and practice performance). Additionally, the moderating effects of technological acceptance and the mediating role of institutional support will be explored. This will lead to a set of practical recommendations for the integration of AI into nursing curricula and clinical environments.
Section snippets/Literature review
Artificial Intelligence (AI) has emerged as a transformative force in both nursing education and clinical practice. The integration of AI into nursing education, through innovations in curriculum design, clinical training, and simulation, is reshaping how nurses are trained and prepared for modern healthcare challenges. Similarly, AI applications in nursing practice, such as decision support systems (DSS) and AI-enhanced patient monitoring, are changing the way nurses deliver care, improving
Research methodology
This study will employ a quantitative research methodology to examine the impact of Artificial Intelligence (AI) integration on global nursing education and practice. The research will use Smart-PLS 4.0, a software tool for structural equation modeling (SEM), to analyze the relationships between the variables outlined in the study framework. SEM is chosen due to its capability to handle complex models involving multiple independent, dependent, mediating, and moderating variables (Hair et al.,)
Result analysis and discussion
The path coefficients in Table 1 reveal strong, significant relationships between AI integration and nursing performance outcomes. The T-values consistently exceed the threshold of 1.96, confirming the statistical significance of the direct paths. In Table 2, total indirect effects show meaningful mediating influences, with T-values above 1.96 for most variables, indicating significant indirect relationships. Confidence intervals in Table 3 further validate these findings, with narrow ranges
Conclusion
This study has demonstrated the significant impact of AI integration in both nursing education and practice. The results show that AI Application in Nursing Practice (AIANP) and AI Integration in Nursing Education (AIINE) have substantial positive effects on Nursing Education Performance (NEP) and Nursing Practice Performance (NPP). Key findings include the strong relationship between AIANP and Institutional Support (IS), as well as the enhancement of Technological Acceptance (TA) through AI.
The unpredictable hours of residency make romantic relationships tough—but not impossible. Here’s how to date and maintain a love life during residency.
The long and unpredictable hours of residency make starting and maintaining a romantic relationship tough. But it’s not impossible.
Here’s how to date and make the most of your love life during residency.
First, let’s address the elephant in the room. If you’re going into residency single and haven’t spent much time dating or figuring out what you need from a partner, taking on this challenge during residency will be difficult. Building a deep, romantic relationship requires time, which is something you have very little of in residency.
Even the act of finding a relationship requires a significant time investment. You’ll need to put yourself out there socially, such as going to events or joining community groups, work on your own personal development, and zero in on what you’re actually looking for from a partner.
If this sounds like you as a resident, do not despair. It is possible to find and build a relationship during residency, but you need to understand both what your priorities are and how many hours you have to find and keep that special someone. If finding a relationship in this stage of your life is important to you, you’ll need to intentionally carve out and block time for it, much like when you are studying for boards.
Don’t allow your years of residency to fly by without being intentional about every aspect of your life—this includes your professional development, personal wellness, hobbies and interests, and love life.
If starting a family and settling down is a top priority for you at this stage, you need to act like it. This will mean you have less time for other things, such as research you wanted to pursue, personal hobbies, or binging Netflix shows alone.
Alternatively, you may decide a serious relationship is less important to you at this time, which is perfectly okay too. Don’t fall into the trap of doing what those around you are doing just because it seems like the logical next step. Jumping into a serious relationship or beginning to start a family because you think you should, and not because you want to, is a recipe for disaster.
With that in mind, if dating is a priority for you, it’s time to get serious about identifying your needs.
Identify Your Needs
One of the biggest questions to ask yourself is whether or not you want to be with someone in medicine, as there are pros and cons to both choices.
A partner in a medical field, such as another resident or someone pursuing another healthcare career, will share an understanding of the time-consuming nature and challenges of residency. They are more likely to be comfortable with your limited and unpredictable hours because they experience the same thing. You’ll also have plenty to talk about in the realm of medicine, but this can be both positive and negative.
Your shared interests may keep the conversation going, but you run the risk of talking about medicine all the time. A partner outside of healthcare can offer new topics of conversation, and you can learn new things from each other. Additionally, a non-resident partner can more easily work around your rigid schedule.
If both of you are pursuing a career in healthcare, you may have similarly unpredictable schedules. If you each only have one small sliver of free time, it’s likely they won’t align, making it difficult to carve out time together.
However, your career path is only one small element of determining your own needs.
Are you looking for someone who wants to have children? Are you eager to start that process right away, or do you want to wait a few years? Do you want someone who shares your passion for fitness and wellness? Is preferring Star Trek over Star Wars a deal breaker for you?
By the time you’re in residency, you likely have a better understanding of yourself and what you hope your future will look like. Determine what you’re looking for in a partner to save yourself time during the dating process, as you don’t have any time to waste. However, ensure you’re not too rigid in your quest for love. The more you idealize your perfect partner, the harder your search will be.
After all, no one is perfect, and every relationship involves compromise.
Finding a Partner
After spending time identifying your preferences, it’s time to go out and find that special someone, which is easier said than done, especially for residents.
Unlike treatment algorithms, there are no x + y + z instructions to find a partner. It takes time, patience, and a whole lot of trial and error. Put yourself out there and continue meeting new people. Choose events, groups, and activities that align with your interests so you find someone who shares your values.
For example, if fitness is a top priority for you, join a gym or athletic community group you’re interested in, such as a running club, kickboxing class, or yoga in the park. If religion is an important aspect of your life, make time to go to church or temple events, and get more involved in religious community initiatives. If you’re passionate about books and storytelling, join local library events and begin participating in a book club.
Dating apps can also help you streamline the dating process. If used effectively, they can aid residents who have very little free time. Be sure to choose dating apps that align with your needs. If you’re looking for a serious relationship with someone who wants to start a family, don’t waste your time on an app known for its hookup culture.
If you’re looking for someone who is also in medicine, there are dating apps specifically for healthcare workers, such as ForeverX and DowntoDate.
Use dating apps to your advantage, but understand their limitations. If your residency is in a small town, you will have fewer options. The pros and cons of dating apps and how to optimize online dating are discussed in video on my Kevin Jubbal, M.D. channel.
Maintaining a Healthy Relationship
Starting a relationship is just one part of the equation. As a resident, you’ll have to put in more effort than usual to help maintain it. Here’s how to keep a healthy relationship strong.
1 | Be Clear About What to Expect
The first and most important tip is to be upfront with your partner about what to expect over the next few years. This will be easier if you’re dating a fellow resident or someone in the medical field, but either way, it’s vital that both of you have clear expectations.
Your free time will be very limited. Your schedule may be so hectic at times that all you can do after a long day is go home and sleep. Your free time will also be unpredictable, as you may be on call, which can and likely will result in cancelled plans, sometimes at the last minute. Preparing your partner for these situations from the outset will prevent conflict.
When approaching commitments, use percentages. With what percent confidence can you commit to an event? Is there a 90 percent chance you can make it, a 70 percent chance, or 30? Knowing this upfront will result in fewer misunderstandings and hurt feelings.
If hurt feelings do occur, be sure to allow your partner to vent. Constantly canceling plans will be frustrating for them at the very least, and if they aren’t working in healthcare, your schedule and priorities during this time will be difficult to understand.
Being in medicine in some ways is as close to being in the military as you can get, with an arguably even more unpredictable day to day schedule at times.
Be clear right from the start that you will be under a tremendous amount of stress. This is in no way carte blanche for you to be rude or self-obsessed; however, they should know there will be times when you come home after having been chewed out by an attending or after having lost a patient. You may not always be able to put on a happy face and forget about your day the moment you walk through the door.
2 | Develop Open and Honest Communication
Next, communication is the foundation of any strong relationship, and it’s what will save you during residency. Explain when your shifts are, when you’re on call, and share your exact schedule, but strive to go beyond that. You need to share what’s going on in your inner life as well, including your feelings, concerns, and current energy levels.
Be honest. Don’t put on a brave face. They need to know how to support you through your dark days, which means you need to give them the full and honest picture of the job from the start.
If a patient dies, it’s important to share how it affected you. Don’t act as though your partner can’t help you or pretend you don’t need help when they can see that you do. If you deny your feelings, you’re more likely to crack under the immense pressure you’re under. Plus, you’re taking away your partner’s agency. Of course, they can’t help you with everything, but when they can, let them. If you have the right partner, they’ll be happy to offer you support.
However, remember that communication is a two-way street. Your partner isn’t there just so you can talk at them about how rewarding or challenging it is to be a doctor. They need to know they can vent to you when they are stressed, no matter their career path. Being a teacher, accountant, waiter, or business owner comes with its own stresses. They must be able to talk about their day too.
While the relationship does largely rely on your schedule, it’s not all about you.
3 | Don’t Allow Medicine to Rule Your Life
Next, while it’s important to be honest about your work and how it makes you feel, it shouldn’t be the only thing you talk about, and it shouldn’t rule your lives.
It is essential to take time to decompress before you see your partner and to put a time limit on hospital or clinic talk.
Dr. Joshua Goldman has found success using his drive home to transition his mindset. He has two children, so he uses his commute to move from serious plastic surgeon to playful dad. Dr. Goldman shares how he balances his family and work life in an episode of Day in the Life.
Even though it may not feel like it at times, you are more than just a doctor. Developing a healthy life outside of medicine will aid both your relationship and your career. You’ll be able to go into work fresh and ready to start again, rather than carrying it with you 24/7.
Work with your partner on finding a balance in your conversations. This is especially important if both of you are in residency. It’s great that it’s a passion you both share, but you are more than just residents. What are your hobbies and values outside of medicine? If you have to, make a rule that when on dates or when sharing a meal, you don’t talk about medicine. This will allow you to get to know each other on a deeper level and grow your connection beyond your shared careers.
4 | Intentionally Block Time for Your Relationship
The fourth tip is to intentionally make time for your relationship and your partner. Even with your busy schedule, make specific plans, put them in your calendar, and do your best to commit to them. You may only have a few extra hours each week to dedicate to your partner, but know that any time spent together is better than nothing.
Neglecting time as a couple will erode any relationship. If you’re not careful, those few hours of free time will get eaten up by something else, and before you know it, four weeks will have passed by without the two of you spending any quality time together.
You need to block time for your relationship and ensure being together occurs in some form or another. When your schedule is tight, get creative about blending other commitments. How can you turn tasks like grocery shopping, cooking, or even cleaning the house into a date?
Completing these seemingly boring tasks together will make them more enjoyable while giving you more opportunities to see each other. That said, don’t allow your only time together to be over laundry and dishes, as this is a surefire way to lose that romantic spark.
On days when you only have a few moments to spare, taking the time for a small gesture like bringing home food or flowers or just texting them a kind message can brighten your partner’s day.
Don’t only focus on what you want out of a relationship. What does your partner prefer? You might care about gifts and small gestures while what’s most important to your partner is hearing words of affirmation.
This is commonly referred to as your love language. The five love languages are physical touch, acts of service, quality time, words of affirmation, and gifts.
If you don’t know your preferred love languages, there are plenty of online quizzes you can take. While by no means scientific, they can provide insight into your own needs and preferences as well as your partner’s. If your love languages align, awesome! If they do not, don’t be discouraged. Taking the time to learn more about each other’s preferences will help you both get what you need from the relationship.
This again falls back on effective communication. Neither of you are mind readers. Make every effort to ensure both of your needs are met.
Romantic relationships during residency can be tough—but they’re rewarding too. Residency is tremendously challenging, and having someone you can lean on during this time is extremely valuable.
Neonatal nurses have a major role in helping parents engage with their infant. A high level of parent participation, called Parent-Partnered Care, integrates parents as full partners in the delivery of hospital care to their infants. One parent-partnered intervention that improves infant, parent, and parent-infant outcomes is H-HOPE (Hospital to Home: Optimizing the Preterm Infant Environment). H-HOPE has 2 components: Massage+ and Parents+.
Purpose:
The purpose of this article is to present an evidence-based guide showing how to deliver Parents+ and the implications for nursing practice.
Methods:
The nursing approach to Parents+ includes participatory guidance and social support, which fosters a partnership with parents. The guidelines for using participatory guidance include a detailed description of each teaching/learning session along with implications for nursing practice.
Results:
Parents’ experienced many benefits from participating in the Parents+ sessions. They reported feeling more confident in the care of their infant and more satisfied with learning and delivering Massage+. Additionally, parents also reported less fears handling their infants, increased feelings of bonding/attachment, and a sensitivity/responsiveness to their infant’s behavioral cues.
Implications for practice:
Parents+ presents an opportunity for nurses to help parents engage with their infants and increase their confidence and competence. Parents’ desire a neonatal intensive care unit culture that embraces a comprehensive collaborative approach with healthcare professionals that is individualized to their infant’s health and well-being.
Neonatal nurses have a major role in helping parents engage with their infant and provide direct care. The inclusion of parents as full partners in the care of their infant in the neonatal intensive care unit (NICU) has greatly expanded to include routine caregiving, developmentally supportive care, and engagement with the neonatal team regarding infant healthcare decisions. A high level of parent participation in the care of their infants, called Parent-Partnered Care, is defined as “approaches that center or integrate parents as full partners in the delivery of hospital care to their ill or small newborns.”
One parent-partnered intervention that improves infant, parent, and parent-infant relationship outcomes is H-HOPE (Hospital to Home: Optimizing the Preterm Infant Environment). H-HOPE is a parent-focused intervention that fits within the Parent-Partnered Model of Care where members of the healthcare team partner with parents in care delivery . H-HOPE includes both an infant-focused intervention, Massage+ (formerly termed the ATVV, Auditory, Tactile, Visual, and Vestibular Intervention), and a parent-focused intervention, Parents+. A large body of research documents that Massage+ significantly increases infant alertness, clarity of the infant’s cues, oral feeding and growth, and fosters the development of infant social communication and the parent-infant relationship in hospital. Additionally, Massage+ has been associated with reduced acute care visits and improved parent-infant interaction at 6-weeks corrected age. Massage+ is designed to be provided by parents while Parents+ provides guidance and support from nurses so parents can confidently provide Massage+ with sensitivity to their infant’s cues.
H-HOPE: one model of parent-partnered care.
As an early behavioral intervention for preterm infants and their parents, H-HOPE is designed to be integrated within a culture that supports parents as partners in care. H-HOPE incorporates 3 key elements of Parent-Partnered Care: presence, participation, and engagement. The physical presence of parents is necessary to provide them the opportunity to participate in caregiving activities like Massage+. Parents may participate in care activities with the support of nurses or independently depending upon their confidence and experience. Parents+ requires collaboration between the nurse and parent to teach parents how to understand their infant’s behavior and deliver Massage+. Engagement occurs when a parent is emotionally involved in their infant’s health and healthcare through their actions. Engagement is not fixed, rather it exists along a continuum. Over time, the delivery of H-HOPE by parents increases parents’ confidence in their caregiving and engagement with the healthcare team.
A comprehensive toolkit, including instructions and videos showing the step-by-step process of Massage+ is available to support nurses and parents in the delivery of Massage+ on Pathways.org (https://pathways.org/massage-tool-kit-H-hope) at no cost. Pathways.org also has detailed information and developmental resources for nurses to use during the Parents+ sessions. After completion of Parents+, the website is available for parents.12 These materials and videos are especially helpful for parents to review content at any time. However, detailed guidelines for the nurse to deliver Parents+ is not currently available in the literature. Therefore, the purpose of this article is to present an evidence-based guide showing how to deliver Parents+ and the implications for nursing practice.
PARENTS+ CONCEPTUAL BASIS
Parents+ consists of teaching/learning sessions that help parents understand infant behaviors and cues, shows them the steps of Massage+, and provides experiences that build parent confidence in providing Massage+ guided by their infant’s cues. The conceptual basis supporting Parents+ includes participatory guidance,principles of adult learning and experiential learning.
Participatory guidance occurs when a skilled clinician guides the process of learning how to perform a complex task, with the mutual goal of moving the learner from novice to expert. This approach changes the relationship from “instructor-student” to a collaboration. When using this approach, nurses foster bidirectional communication with parents.
Adult learning involves respecting and integrating what the parent brings to the sessions, such as their own experience in caring for an infant. It is their “history” related to the context of their lives, including their preterm infant, family, socioeconomics, cultural factors, and other responsibilities.
Experiential learning provides opportunities that foster integration of the new experience into the learner’s everyday skills. This learning approach provides hands on practice (Massage+) and supports parents as they gain confidence and competence while interacting with their infants. Experiential learning is also a component of Bandura’s well-known social learning theory widely used as an effective model for behavior change programs.
The learning strategies derived from these concepts promote parent participation and engagement (Parent-Partnered Care), build trust between nurses and parents, and increase parents’ confidence and competence with infant care. The integration of these strategies fosters growing parent competency. One advantage of Parents+ is its strong conceptual approach that assists nurses in conducting parent education that is both planned and effective, allowing nurses to provide consist of support across shifts and nursing assignments. This common understanding of how to conduct parent education is much needed; as noted in a recent scoping review that described the inability of health professionals to articulate the systematic teaching strategies they used.
DESCRIPTION OF THE PARENTS+ SESSIONS
Parents+ consists of 3 to 4 sessions: 2 in-hospital and 1 to 2 post-discharge. The focus of each session is the parents’ engagement with their infant, as they learn to understand their infant’s behavioral cues and how to build the parent-infant relationship. Parents learn about cues both through the nurse teaching about behavioral cues as well as the nurse asking about what cues the parents have seen in their infant and pointing out cues the infant may exhibit during the Parents+ session (Table 1). Through this repeated process, parents learn to read, interpret and respond to engagement and disengagement cues. For example, when their infant is overstimulated and exhibits a potent disengagement cue, the parent learns how to modify his/her behavior to reduce overstimulation (see Session 1 for definitions of engagement and disengagement behaviors below).
TABLE 1. – Parents+ Content: Example Session Questions and Talking Points
Open session with parent concerns
Let’s start by discussing how you’re doing. How are things going for you? Do you have any questions about your baby?
Infant behavioral states
Have you noticed how your infant wakes up? What state is your infant in right now?
Engagement & disengagement cues
These pictures show some ways infants show they are ready to interact with you or want to continue. Which ones have you noticed that your infant does?
Orally directed behaviors
Here are some things infants do to show they are getting ready to eat. What does your infant do when s/he is ready to eat?
Hunger & satiation cues
Here are some things infants do to show they are getting ready to eat or that they are full. What behaviors does your infant have when they are getting ready to eat and when they are full?
Massage+
Massage+ is an activity that stimulates all your infants’ senses and is enjoyable for both of you Massage+ helps infants become alert and ready to feed, so they eat and sleep better. Do you notice any benefits for your infant when doing Massage+? Infants may like some parts and not others. Do the parts your infant likes. Remember to pause if they need a break. How does your infant respond to Massage+?
Back to sleep
Do you know the best position to put your infant in for sleeping?
Signs & symptoms of illness
Before you go home, we’d like to review what you might see in your baby that would need immediate attention.
How to calm a fussy baby
Does your infant ever get fussy? What do you do? Let’s talk about different things that you can do to calm the infant when s/he is fussy.
Feeding is more than eating
Feeding is an important time to relate to your infant Whether breast or bottle feeding, your infant needs to be close to you and have your full attention while feeding. This is a time for you and your infant to relax and enjoy each other
Tummy time
Tummy time is important for your infant’s development and achievement of milestones Let’s review ways you can get tummy time in each day
Developmental milestones
Infants do not develop the same way, but knowing what developmental milestones to be on the lookout for can help you monitor their progress. Let’s review some 0-3 month milestones. Have you seen any of these in your infant yet?
Close session with parent check-in
Do you have any further questions or concerns about what we’ve discussed, or anything else?
Infant behaviors and Massage+ are introduced at the first session and reviewed and practiced in subsequent sessions. While teaching Massage+, the nurse talks about infant behaviors and caregiving, adding new content to each Parents+ session. Content of Parents+ can be divided into multiple smaller sessions to accommodate both parent and nurse time constraints. When this occurs, documentation of parent education in the electronic health record (ideally into the existing parent education documentation) serves as a communication tool between nurses to ensure completion of a Parents+ session, picking up where necessary. If an infant is discharged earlier than expected, missing content can be delivered during the post-discharge visits.
Each Parents+ session follows the same plan:
Address (re-address) parent concerns
Review any previous content
Introduce new content
Complete each session by returning to the parent’s continuing concerns and any questions about their infant.
The focus on parent needs at the beginning and end of each session is in response to the high stress, anxiety and fear many parents report during their time in the NICU. Nearly all parents’ have emotional needs related to caring for their vulnerable infants and are often hesitant about even touching their infant. The psychological distress of having a preterm infant, exacerbated by the stress of the NICU environment, along with the context of parent’s lives outside the hospital, affect their ability to fully participate in caregiving of their infant and engage with the healthcare team regarding their infant and family’s needs. For parents to fully engage during this stressful time, their needs must be addressed in conjunction with the infant’s needs. However, parents are rarely given an opportunity to discuss their own feelings and needs. Parents+ helps mitigate parents’ distress by acknowledging their needs and concerns and asking what they want to learn about their baby to support their learning and engagement.21 While some concerns are too complex to be resolved or may require referrals, simply acknowledging parent concerns helps parents feel heard and builds trust. Detailed guides for each session are available on Pathways.org.
Session 1
The first Parents+ session can be initiated when the parents are physically and emotionally ready, even if the infant is not old enough to receive Massage+ (Massage+ begins when the infant reaches 31-32 weeks postmenstrual age and is physiologically stable). Infants born between 33 and 35 weeks may also begin Massage+ once they are physiologically stable. This first session includes substantial content about preterm infant behaviors and cues that are highly relevant for all parent caregiving and engagement with the infant. Sharing information about preterm infant behavior and cues prior to the infant’s readiness for Massage+ allows parents’ time to become comfortable learning to read, interpret, and respond to their infant’s cues.
During Session 1, 4 content areas related to preterm infant behaviors are discussed. Nurses use active listening to understand parents’ concerns and tailor content to support learning. The session begins with a description of infant behavioral states and engagement and disengagement cues to help parents understand the many behaviors that infants use to express themselves. These cues also include orally directed behaviors (pre-feeding behaviors) and those that indicate hunger and satiation. When working with parents, using the term pre-feeding behaviors is easier for parents to understand. Later in this session, parents learn the steps of Massage+ and practice Massage+ on their infant with guidance. Cues are further reinforced when parents learn to read, interpret, and respond to the infant’s behavior while giving Massage+ to their infant.
Infant Behavioral States: Behavioral states include quiet sleep, active sleep, drowsiness, active alert, quiet alert, and crying. Identifying the infant’s behavioral state indicates readiness or lack of readiness to engage. During the active alert state, the infant’s eyes are open and the infant looks around; arms and legs may be moving, indicating readiness to feed. This state is most optimal for oral feeding, regardless of whether feeding is provided by bottle or breast feeding. During the quiet alert state, the infant’s eyes are open, the infant is calm and ready for social interaction with the parent.
Engagement and Disengagement Cues: These cues are important indicators of the infant’s readiness to interact or needing a break. Both engagement and disengagement cues can be potent (eg, easy to understand such as looking at the parent, or cry) or subtle (eg, difficult cue for the parent to read and interpret such as hands open or grimace). Preterm infants often show more subtle engagement cues such as brow raising, facial brightening, feeding posture, and hands open with fingers slightly flexed. As they mature, the frequency of potent cues increases. Potent disengagement cues include a cry face and halt hand, turning head away, and spitting up. Subtle disengagement cues include fast breathing, gaze aversion, and yawning.
Orally Directed Behaviors (Pre-Feeding): Orally directed behaviors indicate the infant’s readiness to feed. These include mouthing, rooting, tonguing, hand-to-mouth, hand swipes at mouth, empty sucking, sucking on hand, and sucking on tongue.7,30
Hunger and Satiation Cues: Hunger cues include arms and fingers bent, facial grimace or crying, mouthing and sucking movements. Satiation cues include arms relaxed or by the infant’s side, relaxed fingers, infant has a neutral face (no expression), or infant is asleep.26,27,31 These cues provide additional indicators of the infant’s hunger or feeling full. This is important for parents who often want to feed their preterm infant the entire oral feeding even though they are exhibiting satiation cues.
Session 2
Session 2 begins 1 to 2 weeks before discharge. Planning for Session 2 well before discharge allows additional time to address parents’ questions and concerns and to support the parent-infant relationship before heading home. This session also offers additional opportunities to integrate new information with previous learning.
Session 2 content includes signs and symptoms of illness and back to sleep. This information is often already incorporated into discharge education. However, the participatory guidance approach of H-HOPE (Parents+) acts as a reinforcement of the importance of active listening to address parents’ questions with bi-directional communication and incorporating the context of the parents’ needs and concerns as they transition to home. As discussed above, this may include referrals or additional resources to support parent self-care.
Sessions 3 and 4
One or two virtual sessions occur within 2 weeks after parents are discharged home with their infant. Parent feedback from our previous research indicated that this is also a stressful time for parents and they appreciated the additional support and educational content. The purpose of these post-discharge sessions is to offer support to parents, answer questions related to Massage+ and infant behavioral cues that were taught during the first session, as well as infant care. New topics include calming a fussy baby, feeding is more than eating, tummy time, and developmental milestones. Parents are also encouraged to use the Pathways.org App for continuing information about developmental milestones that can be easily downloaded onto their phones.
Depending on the parents’ schedules at home, these 2 sessions can be combined into 1 session. However, the rationale for providing 2 post-discharge virtual sessions was developed as a result of previous research with parents’ who found these visits valuable for their transition to home.
DISCUSSION
The purpose of this article was to present an evidence-based guide showing how to deliver Parents+ and the implications for nursing practice. While parents appreciated Massage+ in previous research studies, they reported high anxiety while handling their infants and not clearly understanding their infant’s behavior. Parent feedback led to the development of Parents+ which offers parent support and guidance to improve outcomes for infants, parents, and the parent-infant relationship. Massage+ is designed to be provided by parents while Parents+ provides guidance and support from nurses so parents can confidently provide Massage+ with sensitivity to their infant’s cues.
Parents+ is a model for collaboration between parents and nurses enabling the delivery of Parent-Partnered Care, and has benefits for parents, infants and nurses, as discussed below. The first Parents+ session was intentionally designed to guide parents in learning and practicing the steps of Massage+ on their infant. When Massage+ is provided by parents, they can see their infant’s positive behavioral responses and growing developmental capacities. The process of providing Massage+, a multimodal dyadic intervention, helps parents’ experience handling their infant and responding appropriately to infant cues; skills that readily transfer to virtually all other caregiving.
Thus, the experience of providing Massage+ begins to build the parent-infant relationship. In both qualitative and quantitative assessments, parents reported feeling more confident in the care of their infant and more satisfied with learning and delivering Massage+. In other intervention and engagement studies, parents reported improved mental health, increased confidence and competence while caring for their infant. Parents also reported less fears handling their infants, feelings of bonding/attachment, and parental sensitive-responsiveness to their infant’s behavioral cues.1Significantly, this response has been proposed as the foundation for the development of the parent-infant relationship.
Benefits for Parents+.
Overall, the benefits of H-HOPE (Massage+ and Parents+) for infants have been well documented in the literature. Infants of different post-menstrual ages (31-36 weeks) responded with improved alertness, increased orally directed behaviors, faster progression from gavage to oral feeding, improved growth, and fewer illness visits after hospital discharge.2,4,6-8 In addition, other investigators reported an improvement in neurodevelopmental outcomes following interventions focused on the parent-infant relationship. Interventions that also include the transition into the home as with Parents+ Sessions 3 and 4 are ideal because this offers additional support for parents and infants post-discharge.
Importantly, Parents+ also benefits staff, providing a practical guide that both novice and expert nurses can use to more effectively help parents engage with their infants. Conducting Parents+ using a participatory guidance approach further develops interactive and teaching skills for nurses. Essentially, the participatory guidance approach can be used for any instruction with parents. These skills foster a culture for parent participation, using bidirectional communication and demonstrating how parents can collaborate with the nurse as a partner. Showing respect and understanding of the parent perspective is particularly salient, as nurses play an important role in making parents feel comfortable and welcome in the NICU environment, as well as increasing their confidence in providing care for their preterm infants.
IMPLICATIONS FOR CLINICAL PRACTICE
Increasingly, the nurse’s opportunity to provide parent support and guidance is challenged by a continually, complex clinical environment, staffing shortages and family stressors. Parents+ presents an opportunity for nurses to help parents engage with their infants and increase their confidence and competence. Physical therapists, occupational therapists, and speech language pathologists trained to administer H-HOPE are well equipped to provide the intervention and can partner with nurses’ to provide these services. However, in most NICUs, the primary responsibility will likely reside with nurses, as they are the only clinicians in the NICU who are at the bedside 24/7. Moreover, evidence-based parent focused developmental approaches to preterm infant care have been shown to affect neurodevelopmental outcomes for infants, driving the need to become a standard of care in the NICU.45 The Vermont Oxford Network issued a statement, “All care is brain care,” to emphasize the importance of developmentally based care for the preterm infant.As NICUs move forward with advancing this type of care, a unit culture that incorporates a developmental and behavioral approach to caregiving by nurses is critical and necessary to achieve optimal outcomes. To support a unit culture of developmental care, staff education and training, from orientation through skill review sessions, is imperative.
The parent perspective can be found in the literature, via feedback from parent advisory groups, and local and national parent support networks (eg, https://nicuparentnetwork.org; https://www.marchofdimes.org/our-work/nicu-family-support; https://handtohold.org; https://www.projectnicu.com). Parents desire a NICU culture that embraces a comprehensive collaborative approach with healthcare professionals that is individualized to their infant’s health and well-being. The goal for all parents is to achieve optimal outcomes for their infant.44 However, this may require more than changing the NICU culture. There are many factors besides NICU culture and socioeconomics that are barriers and challenges for parents. These include insufficient knowledge about how to care for the infant and understanding realistic expectations for growth and development, as well as access to resources to support the parent’s and infant’s needs.
A successful practice change that incorporates the parent perspective also depends upon experienced leadership; operational and clinical leaders who set consistent expectations for implementing and sustaining evidence-based standards of care. In addition, assessment of staffing needs is critical to incorporate a practice change into nursing workflow. Parents need nurses who have the time to help them learn a behavioral intervention like H-HOPE and provide essential developmental care. NICUs where parent education and engagement are highly valued, and a cornerstone of nursing practice, will likely be more willing to accept H-HOPE. It is imperative for NICUs today to focus on meeting the needs of parents’ and infants, address the challenges, and implement evidence-based practices. In addition to assessing staffing needs, each institution must consider other logistical factors, such as reimbursement for services and who conducts the post-discharge sessions. While nursing time inpatient is not reimbursable, outpatient often is, which may cover the 2 post-discharge Parents+ visits. These post-discharge visits could be completed by a discharge nurse or developmental specialist, depending on the resources of each institution.
CONCLUSION
Parents+ is an innovative behavioral intervention with benefits for parents, infants and staff. Parents+ incorporates a model of Parent-Partnered Care, which helps mitigate parent’s distress by addressing parents’ needs and concerns to support their learning and engagement with their infant. The Parents+ sessions are designed to provide education and support during the NICU stay and post-discharge. Understanding the evidence that supports developmental and behavioral care is key to recognizing the rationale for incorporating Parents+ into the standard of care by staff. Incorporating a culture of developmental and behavioral care for parents and their infants is imperative to address their needs, improve outcomes, and advance nursing practice in the NICU.
Summary of Recommendations for Practice and Research
What we know:
Parents+ is a behavioral intervention that incorporates Massage+ to help parents learn their infant’s cues and contributes to optimal neurodevelopmental outcomes. Parents+ is an evidence-based approach to behavioral care in the NICU. Nurses are essential for providing Parents+.
What needs to be studied:
Further research is recommended to identify effective strategies incorporating H-HOPE into neonatal nurses’ workflow. Research is critical to describe how NICUs embrace developmental care as the standard of care. Data are needed to document parent and infant outcomes from the delivery of Parent-Partnered Care.
What can we do today that would guide caregivers in the practice setting considering the use of this evidence for guiding practice?
Provide leadership support for a developmental and behavioral approach to NICU care. Educate nurses on the principles of Parent-Partnered Care. Engage parents to understand the behavioral cues of their infant as a component of their caregiving.
Club cell secretory protein (CC16) is a pneumoprotein that has anti-inflammatory and antimicrobial properties and whose levels are reduced in preterm infants.
Objective
We sought to investigate the role of circulating CC16 in the association of preterm birth (<37 weeks) with lung function and asthma from childhood into young adult life in longitudinal and mediation analyses.
Methods
Using the BAMSE (Swedish abbreviation for Barn/Children, Allergy, Milieu, Stockholm, Epidemiology) birth cohort (2,557 participants and 10,631 longitudinal observations), we assessed plasma CC16 (ages 8 and 24 years), spirometry (ages 8, 16, 24, and 26 years), and asthma (ages 8, 12, 16, 24, and 26 years). Longitudinal associations between preterm birth, CC16, percent predicted values of FEV1/forced vital capacity (ppFEV1/FVC), and asthma were examined in longitudinal multivariable mixed models. CC16 (ages 8-24 years) was tested as a mediator for the relationship of preterm birth to pre- and postbronchodilator ppFEV1/FVC and asthma in adulthood (ages 24-26 years).
Results
Preterm birth was associated with reduced plasma CC16 (−1.15 ng/mL; 95% CI, −1.22 to −1.08; P < .0001), lower ppFEV1/FVC (−1.9%; 95% CI, −3.1 to −0.8; P = .001), and higher risk for asthma (1.83; 95% CI, 1.28 to 2.62; P = .001) across ages 8 to 26 years. CC16 deficits were related to decreased ppFEV1/FVC (P < .0001) and increased risk for asthma (P = .007) in adulthood. Multivariable mediation analyses suggested that CC16 mediated 16% and 9% of the effects of preterm birth on ppFEV1/FVC and asthma in adult life, respectively.
Conclusions
Low CC16 is a potential mediator of the effects of prematurity on lung function deficits and asthma in young adulthood. Future studies should address whether CC16 can be used as a predictive biomarker and, possibly, a therapeutic target in individuals born preterm.
Section snippets
Participants
BAMSE is an observational population-based birth cohort study that enrolled 4089 children born in Stockholm between 1994 and 1996.35 The study design and enrollment process are detailed in this article’s Online Repository at www.jacionline.org. Perinatal data were obtained from the Swedish medical birth register.36 Plasma CC16 levels were measured at ages 8 and 24 years. Spirometry was conducted at ages 8, 16, 24, and 26 years. Asthma questionnaires were answered by parents at ages 8, 12, and
Results
Overall, 2,557 BAMSE participants were included in this study, contributing to a total of 10,603 longitudinal observations for asthma (526 for preterm participants) and 6,109 for lung function (324 for preterm participants). Compared with the 1,532 excluded participants because of missing CC16 and/or phenotypic data, those included were more likely to be females and have older, nonsmoking mothers and higher-educated parents with a history of asthma (Table I). There were no significant
Discussion
In this study—using a large, long-term, population-based birth cohort—we demonstrated that low circulating CC16 levels may mediate part of the effects of preterm birth on lung function and asthma in young adult life, supporting a protective role of CC16 in obstructive lung diseases of individuals born prematurely. These findings highlight the potential of CC16 for risk stratification and, possibly, novel therapeutic strategies for preterm individuals at risk for obstructive lung disease.
Empowering Voices: Honoring the Educators Who Shape Our Journeys
As we begin Neonatal and Preemie Awareness Month, we celebrate not just our survival stories, but the growth and purpose that follow. For those of us who began life in the fragile space of an incubator, this month is a reminder of how far we’ve come—and of the people who continue to help us become who we are meant to be. This November, our theme is “Educators as Warriors of Empowerment”—because teachers, mentors, and guides are often the ones who help transform early struggle into lifelong strength.
Many of us know that being a preemie can mean growing up with a different pace, a different rhythm, or a different way of learning. It’s our teachers who see that difference and choose to nurture it rather than correct it. They are the ones who remind us that resilience isn’t about perfection, it’s about discovery. Whether it’s the preschool teacher who cheered every word we learned to speak, or the university professor who saw our curiosity, these educators become part of our extended story of becoming.
This month, we celebrate their quiet strength—the patience to listen, the creativity to adapt, and the belief that every child’s journey matters. They empower us to see ourselves not as “born early,” but as born with perspective—the ability to find meaning in milestones others take for granted. Through education, we learn to define our own possibilities, rewrite old narratives, and embrace the uniqueness that began long before we could even open our eyes.
To every educator who has walked beside a preemie—thank you for being part of our collective story of empowerment. And to every survivor reading this: remember, your journey didn’t stop at survival. It continues through the lessons you share, the knowledge you seek, and the lives you touch. This month, let’s honor the teachers who reminded us that we are not defined by our start in life, but by how brightly we choose to grow.
The Czech Republic, also known as Czechia and historically known as Bohemia, is a landlocked country in Central Europe. The country is bordered by Austria to the south, Germany to the west, Poland to the northeast, and Slovakia to the southeast.]The Czech Republic has a hilly landscape that covers an area of 78,871 square kilometers (30,452 sq mi) with a mostly temperate continental and oceanic climate. The capital and largest city is Prague; other major cities and urban areas include Brno, Ostrava, Plzeň and Liberec.
Stories of preterm birth are stories of joy and heartbreak, faith and love. Moving and uplifting. They have the power to inspire. This montage is an all-time favourite of ours and reflects the true heart and face of our work to prevent preterm birth. The Australian Preterm Birth Prevention Alliance is eternally grateful to these wonderful women, these mothers of premature babies, for sharing their very powerful stories.
Abstract: The World Health Organization has named climate change as the greatest threat to public health. In the United States, the healthcare sector accounts for 8.5% of greenhouse gas (GHG) emissions. Neonatal Intensive Care Units (NICUs) and the patients and families who rely on their medical interventions and overall guidance are uniquely impacted by climate change. So, what should NICU professionals know, and what should NICU professionals do? NICU clinicians and designers should recognize that healthcare contributes to climate change, which in turn worsens health issues, especially for vulnerable groups affected by social determinants of health. NICU professionals are well-positioned to understand and influence health equity, having participated in related efforts. Insights gained from addressing health equity can inform strategies for approaching climate change. Individuals should advocate within their organization for climate-forward policies and can counsel patients on climate-forward behavior, implementing education programs where possible. NICUs can transition to reusable surgical gowns and linens safely. Additionally, NICU professionals should advocate for decarbonized building systems whenever new construction or renovations are proposed. Hospitals should advocate for integrating sustainability into their operations and culture. Decarbonization plans should be developed and implemented to reduce climate impacts. Healthcare systems should strive to decarbonize their operations and also consider influencing their supply chain. The NICU has a unique opportunity to make a difference.
Introduction: Our most difficult and stressful challenges all end up at the hospital, and especially in the Neonatal Intensive Care Unit. NICU professionals, such as neonatologists, nurses, therapists, administrators, environmental services staff, and facilities staff, intimately know the details of their most challenging cases. The impact on families is profound. . Families do not want others to experience what they have experienced.
Nevertheless, climate change exacerbates health challenges and may ultimately lead to increased NICU admissions, This represents a vicious cycle: providing NICU care produces carbon emissions that lead to environmental harm, which in turn increases NICU admissions. The implications are clear. The NICU must deliver excellent care while reducing its environmental footprint. NICUs, in particular, have a moral imperative and an opportunity to minimize carbon and other environmental impacts. To achieve this goal, what should neonatologists know, and how can they help?
This paper provides an informational overview, citing literature on the climate crisis, the role of healthcare, and the role of the NICU in contributing to the crisis. It briefly considers health equity as a model for both how societal challenges impact the NICU and how NICUs have responded to address these challenges. Then it identifies some practical ways NICUs can reduce their impact on climate change while buttressing the resilience of the patients and families they serve.
What You Should Know
Humans Impact Climate Change
The scientific foundation of climate change is unequivocal. The Intergovernmental Panel on Climate Change (IPCC), in its Sixth Assessment Report confirmed that human activity—primarily the combustion of fossil fuels and deforestation—is responsible for the observed rise in global average temperatures since the pre-industrial era. The Earth’s surface has already warmed by 1.1°C, with current trajectories placing the planet on track to exceed 1.5°C of warming within the next two decades unless emissions are drastically curtailed.
This warming is driving a cascade of systemic changes, including the increasing frequency and severity of heatwaves, wildfires, droughts, storms, and floods; rising sea levels and coastal erosion; ocean acidification; and biodiversity loss. The climate system’s destabilization is not only an environmental phenomenon— it has become a structural determinant of human health.
The IPCC warns that without immediate and drastic reductions in GHG emissions, the world is likely to exceed 2°C of warming by mid-century, a threshold associated with widespread agricultural collapse, mass displacement, and infrastructure failure (6). For healthcare systems, this future portends interrupted services, overwhelmed emergency rooms, supply shortages, and soaring demand for mental health and infectious disease care. Thus, climate action is foundational to public health preparedness and systems resilience.
Climate Change Impacts Health
From the standpoint of healthcare, climate change poses a comprehensive threat to public health, affecting every organ system, population, and location. The World Health Organization (WHO) has called it “the single biggest health threat facing humanity”. Key health impacts include heat-related illnesses and deaths, vector-borne diseases, including malaria, dengue, Lyme disease, and West Nile virus , respiratory conditions: from exposure to fine particulate matte , increasing asthma exacerbations, COPD flare-ups, and cardiovascular morbidity. Climate change poses significant risks to agriculture in a world where 2 billion people lack essential micronutrients . Climate-related trauma, such as displacement, economic instability, and environmental grief, can increase anxiety, depression, PTSD, and substance use disorders, as well as food and water insecurity. These mental health impacts fall most heavily on low-income groups, communities of color, Indigenous peoples, children, and the elderly, who already face structural barriers to healthcare.
Climate Change Particularly Impacts Neonatal and Perinatal Health
Children are among the most vulnerable populations to the health effects of climate change. They are not only physically more susceptible to environmental hazards since they breathe more air and consume more food and water per kilogram of body weight than adults, but also developmentally dependent on the stability of ecological, social, and healthcare systems. Furthermore, exposures during critical developmental windows, particularly in utero and during the neonatal period, can have lifelong implications for respiratory health, neurodevelopment, immune function, and cardiovascular risk . A systematic review found that maternal exposure to extreme heat is associated with a statistically significant increased risk of adverse pregnancy outcomes.
Particulate matter (especially PM2.5) from traffic, fossil fuels, and increasingly wildfires, which are more common due to a changing climate, is associated with increased risk of low birth weight and preterm birth.
Climate Change puts demands on NICU Operations
The climate crisis also poses increasing operational and ethical challenges to neonatal intensive care units (NICUs). Facilities themselves are vulnerable to climate disruptions, including flooding, wildfires, supply chain interruptions, and power outages. Clinicians must now consider climate resilience as a core function of the NICU. This includes investments in redundant power systems, emergency planning for neonatal transport, and sustainable design to ensure uninterrupted care delivery.
The carbon footprint of neonatal care, caused by single-use plastics, energy-heavy incubators, and anesthetic gases, prompts questions about how NICUs can cut emissions while ensuring safety.
Structural/Social Determinants of Health impact NICU Admissions and NICU outcomes Structural and social determinants of health (SDOH) significantly influence neonatal outcomes, especially in NICUs, where medical vulnerability intersects with systemic inequities. Social determinants of health include access to and quality of education, healthcare, neighborhood and built environment, social and community context, and economic stability (15). Recent studies offer strong empirical evidence linking race, socioeconomic status, geography, and language to disparities in NICU experiences and clinical outcomes (16–19). Addressing these determinants is crucial not only for equity but for clinical excellence in neonatal care.
Climate Change Intensifies the Inequitable Impact of Social Determinants of Health
Climate change exacerbates the social determinants of health that already affect children. Infants born into poverty, homelessness, or marginalized communities face a triple threat: they are more exposed to environmental risks, less likely to access high-quality healthcare, and more affected by systemic racism. For example, historically redlined neighborhoods in US cities are more likely to be heat islands, characterized by fewer green spaces and higher rates of air pollution, which correlates with higher rates of chronic disease.
Indigenous children face disproportionate health risks from water insecurity, wildfire displacement, and food system collapse. Worldwide, children in the Global South will bear the most significant disease burden despite contributing the least to the climate crisis.
For neonatologists, these inequities are not abstract. They show up in disparities in preterm birth rates, NICU admissions, and developmental outcomes, trends that will worsen without targeted intervention.
Healthcare is a major contributor to Greenhouse Gas Emissions (GHG)
While healthcare systems are at the frontlines of climate impact, they are also major contributors to the crisis. Globally, healthcare is responsible for 4.4% of net GHG emissions . In the United States, the sector emits roughly 8.5% of national emissions, making it one of the largest institutional sources of pollution.
Emissions arise from energy use, high-impact anesthetic gases such as desflurane and nitrous oxide, pharmaceutical and medical supply chains, patient transportation, waste incineration, and water consumption.
Thus, the Act of Delivering Healthcare Can Cause Harm
Critically, these emissions pose a contradiction to the sector’s mission: the act of delivering care can simultaneously cause harm through environmental degradation. As such, climate mitigation must be reframed as a core component of healthcare quality, safety, and ethics.
Organizations can make a difference despite changing national-level policies.
In this context, a diverse array of actors, including healthcare organizations, nonprofits, local, provincial/state, and national governments, as well as international organizations, have mobilized in response. While the role of nations is important, climate action happens at the provincial/state, local, organizational, and even individual levels. At the time of this writing, several changes to United States federal policy were made. The Office of Climate Change and Health Equity was disbanded by executive order, eliminating one of the few federal bodies explicitly focused on climate equity in healthcare. Additionally, NIH climate and health research funding was paused or eliminated. Even during times of changing federal policy, other actors, including health care organizations, can continue to make progress.
Healthcare Systems Have Made or Maintained Commitments to Decarbonize
In 2025, the Health Sector CARES Pledge (Climate Action, Resilience, and Equity Solutions) was introduced to replace a repealed US Health and Human Services Health Sector Pledge. The CARES pledge invites hospitals and health systems to publicly commit to a 50% reduction in Scope 1 and 2 emissions by 2030, complete Scope 3 emissions inventories within one year, and embed climate resilience and equity into their operations.
Within months of its release, more than 60 systems, including CommonSpirit Health, Providence, and NYC Health + Hospitals, had signed on.
Additionally, the National Academy of Medicine (NAM) has continued to push for sector-wide decarbonization.
It is possible to Decarbonize Building Emissions.
Building utility decarbonization is possible, and several hospitals are making significant progress in their plans to decarbonize. Decarbonizing building and utility emissions involves three fundamental steps: 1. Reduce the consumption of electricity as much as possible; 2. Switch your systems (for example, heating, sterilizers, kitchen equipment, etc.) to run on electricity instead of fossil systems (natural gas, steam, etc.); and 3. Procure electricity from renewable sources. When you have electrified emissions and procured your electricity from renewable sources, you have effectively decarbonized. Reducing energy as a first step enables you to decrease the amount of energy that needs to be electrified, thereby lowering costs.
On the electricity production side, onsite- or offsite-owned zerocarbon energy (such as solar) reduces purchases of emissions from dirty sources. Organizations can enter contracts to procure renewable energy. Within renewable energy purchasing, there is CommonSpirit Health, Providence, and NYC Health + Hospitals, had signed on. Additionally, the National Academy of Medicine (NAM) has continued to push for sector-wide decarbonization.
It is possible to Decarbonize Building Emissions.
Building utility decarbonization is possible, and several hospitals are making significant progress in their plans to decarbonize. Decarbonizing building and utility emissions involves three fundamental steps: 1. Reduce the consumption of electricity as much as possible; 2. Switch your systems (for example, heating, sterilizers, kitchen equipment, etc.) to run on electricity instead of fossil systems (natural gas, steam, etc.); and 3. Procure electricity from renewable sources. When you have electrified emissions and procured your electricity from renewable sources, you have effectively decarbonized. Reducing energy as a first step enables you to decrease the amount of energy that needs to be electrified, thereby lowering costs. On the electricity production side, onsite- or offsite-owned zerocarbon energy (such as solar) reduces purchases of emissions from dirty sources. Organizations can enter contracts to procure renewable energy. Within renewable energy purchasing, there is a concept called additionality. Additionality refers to renewable energy contracts where the purchase results in an increase in the total amount of renewable energy. For example, a contract to purchase renewable electricity from an existing hydroelectric power plant is not additional, since the energy would be placed on the grid regardless of whether you made the purchase or not. An investment in a new wind farm would be additional, since the new wind farm would not exist without purchase. By purchasing additional renewable energy, you are actually reducing greenhouse gas emissions. Decarbonizing existing facilities can be challenging, but there are resources available to support the process. The Guidebook for Decarbonizing Healthcare (www.decarbhealthcare.com) provides helpful information. For new buildings, the ASHRAE/ASHE Decarbonizing Hospital Buildings Guidebook (24) provides a detailed guide focused on the design, construction, and operation of new hospital buildings and major renovations. This guidebook includes a treatment of embodied carbon—the carbon associated with a building’s construction (as opposed to operation), which is helpful. The healthcare industry is focused on decarbonization, and there are practical guides available to help achieve this goal.
What Can “You” Do?
Be Motivated by NICU-led Health Equity Work
You should also be aware of the progress made in thinking on NICU, health equity, and population health, as NICU professionals have played a unique role in this space.
The Neonatal Intensive Care Unit (NICU) plays a pivotal yet often underrecognized role in shaping population health trajectories. Traditionally viewed as acute care settings, NICUs are now being reimagined as launchpads for long-term developmental, social, and community health outcomes. Bold new ideas in design further this trend (25). A growing body of literature supports the integration of NICU care with broader public health models to address disparities and promote lifelong well-being. Several studies stand out.
Population-based NICU care models have been developed to redesign follow-up programs for children at risk of falling through safety nets. For example, Litt et al. propose a Life Course Health Development (LCHD) framework that emphasizes the importance of early experiences in shaping long-term outcomes. Their model encourages NICUs to coordinate care that extends beyond survival, integrating follow-up services, community engagement, and policy reform. The theoretical strength of this model lies in its comprehensive approach to public health through individualized care for neonates .
Equity audits, culturally competent care, and social supports are being developed to mitigate the compounded effects of racial and socioeconomic inequities on neurodevelopmental outcomes post NICU. Neonatologists are proposing new models of neonatal follow-up that emphasize family and child function. For example, leveraging existing staff, a NICU raised the level of social risk screening coupled with referral to resources in the NICU, with effective results.
Moreover, the familiar Vermont Oxford Network Potentially Better Practices for Follow Through are a key acknowledgement of the idea that “As neonatal care providers, we play critical roles in the lives of small and sick newborns and their families and therefore are uniquely positioned to address social determinants of health. Our responsibility to infants and families extends beyond the walls of the hospital or clinic. We must follow through. Follow-through is different from the more typical neonatal practice of ‘follow-up.’ It is a comprehensive approach that begins before birth and continues into childhood. Health professionals, families, and communities must partner to meet the social as well as medical needs of infants and families to achieve health equity”.
These efforts are highly relevant for two reasons. First, climate change will exacerbate health equity challenges. The forward thinking NICU will therefore need to be even more diligent about addressing social determinants of health and disparities, even to maintain its current level of outcomes. NICU professionals should be aware of this and the ways that colleagues have effectively done this work. Second, NICUs have uniquely developed systems to address complex problems that involve both upstream and downstream factors, for which it may initially seem that the NICU has little to no control. This type of thinking and action provides important lessons and motivation as NICUs strategize to impact decarbonization.
At the Individual Level: Empowering Climate-Conscious Healthcare Workers
Individual healthcare workers and patients are often the first points of contact in the climate-health interface. Although their personal choices might seem modest in scale, the cumulative effect across a large workforce and patient population can be profound. For instance, clinicians can make deliberate choices to avoid low-value care, such as ordering unnecessary diagnostic tests or procedures, which then not only reduces patient harm but also curbs resource waste and emissions. Similarly, choosing digital over printed materials, avoiding overuse of disposables, and advocating for reusable equipment where safe are all everyday actions that help reduce waste streams.
Clinicians also influence clinical practice. By counseling patients on climate-resilient behaviors, such as adopting plant-based diets, quitting smoking, and using active transportation like walking or biking, they can advance both individual health and climate goals. Hospitals like Kaiser Permanente have adopted this ethos, offering incentives for green commuting, including subsidized transit passes, bike facilities, and carpooling programs.
Education is essential. Frontline providers who are informed about the health effects of climate change are better equipped to communicate with patients and colleagues, thereby reinforcing a culture of climate literacy and sustainable practices—these actions, while individual, are essential building blocks for larger systemic change.
Neonatologists are uniquely positioned to advance climate-responsive care. Their roles span clinical advocacy, research, systems improvement, and public health engagement. NICU professionals should collaborate with hospital leadership to reduce waste, switch to lower-impact equipment, and improve energy efficiency. Other actionable steps include implementing clinical screening for climate-related risk factors: housing instability, exposure to air pollution, maternal heat stress, and advocacy for policies that reduce air pollution, expand maternal protections during heatwaves, and strengthen infrastructure for birth centers and NICUs.
Additionally, NICU professionals can lend their voices to interdisciplinary coalitions that recognize child health as a core pillar of climate justice. Their authority, rooted in science and ethics, can shape public discourse and health policy.
At the NICU Level: Greening High-Intensity Care Without Compromising Safety
The NICU represents one of the most resource-intensive settings within a hospital. Infants in NICUs often require continuous monitoring, temperature control, oxygen therapy, and sterile environments, all of which demand energy and generate waste. Nevertheless, even here, there are viable strategies for reducing environmental impact without compromising safety.
NICUs can rethink single-use items. Many NICUs have historically relied heavily on disposable gowns, linens, and medical tools to ensure sterility. However, studies suggest that switching to reusable surgical gowns offers both environmental and financial benefits.
NICU professionals should insist that major renovation or new construction projects are designed to use zero operational carbon. The NICU should enthusiastically support any hospital decarbonization efforts. This includes supporting energy reduction projects. NICUs rely on constant power to support incubators, ventilators, and monitors. Retrofitting these spaces with LED lighting, motion sensor controls, and energy-efficient HVAC systems can lead to substantial energy savings.
Additionally, better waste segregation can reduce the overclassification of waste as “regulated medical waste,” which is often incinerated and carries a carbon footprint several times greater than general waste.
Finally, NICUs may consider approaches to manage the use of oxygen and anesthetic gases, especially during surgeries involving neonates. Choosing lower-impact anesthetic agents and using them judiciously not only reduces GHG emissions but also protects staff from exposure.
At the Hospital Level: Embedding Sustainability in Operations and Culture
At the hospital level, climate mitigation must become a central tenet of operational planning. Hospitals are significant consumers of energy, water, and materials, and they generate substantial waste, including high GHG emissions from anesthetic gases and sterilization processes.
A critical area for action is the operating room, which can account for 30% or more of hospital waste. Hospitals like Hackensack University Medical Center have implemented successful initiatives to eliminate the use of desflurane, a potent anesthetic with a global warming potential more than 2,500 times that of carbon dioxide. By switching to sevoflurane or total intravenous anesthesia, they significantly reduced emissions without compromising patient care.
Food services represent another high-impact area. Hospitals serve millions of meals each year, and most of these meals traditionally rely on carbon-intensive meat and dairy products. Transitioning toward plant-forward menus, sourcing food locally, and implementing food waste diversion programs, such as composting and donating excess food, can significantly reduce a hospital’s environmental impact. Several institutions working with Health Care Without Harm have reported cost savings and improved patient satisfaction with healthier, sustainable meals).
Additionally, investing in green building standards, such as LEED certification, for new construction or retrofitting existing infrastructure with high-performance HVAC systems, water recycling systems, and smart building automation can generate long-term savings and enhance resilience. Hospitals like the Cleveland Clinic have reduced their emissions by 20–30% between 2010 and 2020 with a plan to continue improving energy and waste performance.
These changes often require a cultural shift. Hospitals must empower a “green team” of clinicians, facilities managers, and executives to drive change, track metrics, and communicate progress regularly to staff and the community.
At the Health System Level: Leading Climate Action Through Policy and Partnerships
At the top of the pyramid, health systems have the unique capacity to shape supply chains, influence public policy, and lead national or global climate action. They can develop system-wide sustainability roadmaps that set science-based targets for emissions reductions and embed climate goals into governance structures. Large health systems, such as Kaiser Permanente in the US, have achieved carbon neutrality through investments in renewable energy, the elimination of coal-based power contracts, sustainable procurement practices, and aggressive energy efficiency efforts. Their model proves that decarbonization is achievable at scale with proper leadership and investment.
On a broader level, health systems can influence their entire supply chain by prioritizing vendors that meet environmental, social, and governance (ESG) criteria. Given that the majority of healthcare’s emissions are Scope 3 (indirect) emissions from supply chains, procurement reform is one of the most powerful levers available (36).
Finally, resilient infrastructure planning is essential. Hospitals now require climate-resilient infrastructure, microgrids, and emergency plans to ensure they remain operational during floods, wildfires, and extreme heat events.
Organizations that act decisively can not only reduce their environmental footprint but also improve population health, lower costs, and build long-term resilience. Every part of the healthcare system is essential in the move toward climate-smart care.
Conclusion:
Climate change is a threat to public health, impacting children and neonates all around the world, making them more likely to end up in the NICU and more likely to have adverse long-term outcomes. Likewise, climate change will augment health inequities. Like all areas of hospitals, NICUs contribute significantly to greenhouse gas emissions. There is an imperative for NICUs to have a positive impact on the climate. Fortunately, this is possible. By leveraging their unique voice and in-depth understanding of complex problems, NICU professionals can advocate for policies and projects that significantly reduce the carbon footprint of operating the NICU, thereby continuing to save babies and families.
Check out the video to see the best option for your medical practice.
PREEMIE FAMILY PARTNERS
Having a baby in the NICU changes you. Even after your preemie is home, the emotional rollercoaster doesn’t always stop. The stress, anxiety, fear, and trauma of premature birth and intensive care can linger—and that’s completely normal.
In fact, parents of premature babies are more likely to experience postpartum depression, anxiety, and even post-traumatic stress. That’s why supporting your mental health isn’t optional—it’s essential. This article will help you recognize what you’re feeling, know when to seek support, and give yourself permission to heal and thrive alongside your baby.
Common Emotional Experiences for Preemie Parents
You may feel a complex mix of emotions—many of them contradictory:
Joy at progress and milestones
Fear of setbacks or illness
Guilt for not being able to prevent early birth
Grief over the loss of a “normal” birth or newborn experience
Helplessness during the NICU stay
Overwhelmed during the transition home
These are real, valid, and common. There’s no “right” way to feel.
Attending routine well-child exams at Kids Central Pediatrics helps ensure your baby is growing and developing properly, and allows their doctor to detect diseases or illnesses before serious complications arise.
Common Causes of Premature Birth
Understanding why prematurity happens is helpful, though sometimes a specific cause is never found. Common reasons include:
Multiple pregnancies (twins, triplets, etc.)
Maternal infections or chronic conditions (like high blood pressure or diabetes)
Problems with the placenta or uterus
Premature rupture of membranes (water breaking early)
Smoking, substance abuse, or poor prenatal care
History of previous premature births
Often, a combination of factors is involved. Regardless of the cause, your focus now shifts to supporting your baby’s health and development from day one.
Signs You May Be Struggling
It’s okay to feel stressed—but if it starts interfering with your ability to function or connect, it’s time to talk to someone. Look out for:
Trouble sleeping even when baby is sleeping
Constant worry or racing thoughts
Feeling numb or detached from your baby
Crying frequently or feeling hopeless
Panic attacks or shortness of breath
Avoiding social interactions or appointments
Feeling like you’re failing, even when others say you’re doing great
Partners can experience these feelings too, even if they show up differently (withdrawal, irritability, overworking).
Some parents also develop post-traumatic stress disorder (PTSD) after a difficult NICU journey.
You are not weak or broken if you’re experiencing any of this. These are medical conditions that deserve treatment, just like any other.
When and How to Get Help
If your emotions are interfering with your daily life or sense of well-being, reach out early:
Talk to your pediatrician—they often screen parents for mental health, not just babies
Call your OB-GYN or primary care provider
Connect with a therapist—ideally one who understands perinatal or NICU-related trauma
Ask your hospital social worker or NICU follow-up clinic for resources
Getting help isn’t selfish—it’s one of the best things you can do for your baby and your family.
Coping Strategies That Help
While professional support is key, there are daily habits that can make a big difference too:
Talk about it
Share your story with people you trust
Join an online or local NICU parent support group
Practice self-care (even in small doses)
Take a hot shower, short walk, or 10-minute break
Eat nourishing meals and drink water
Ask for help with meals, errands, or childcare
Sleep whenever you can
Trade night shifts with a partner or loved one
Let chores go when possible
Lower your expectations
This is not the time for perfection
Focus on bonding and surviving one day at a time
Celebrate progress
Write down your baby’s wins—and your own
Acknowledge how far you’ve come
Supporting Each Other as Partners
Preemie journeys can be hard on relationships. Open communication, shared responsibilities, and giving each other space to grieve or cope differently are essential.
Ask each other, “How are you really doing?”
Divide tasks fairly, including night feedings, appointments, and household needs
Make time for connection—even if it’s just a short walk or a meal together
What If You’re Feeling Better Now?
That’s wonderful—and also normal. Not every parent develops a mental health condition, and many experience healing as their baby grows stronger. Still, check in with yourself often, especially during big transitions (like going back to work, starting daycare, or hitting developmental milestones).
Your journey as a preemie parent is ongoing, and emotions can resurface at any time.
You are not alone, and you are not failing. The strength it takes to care for a premature baby is immense—but you don’t have to carry it alone. Prioritizing your mental health is not a luxury—it’s a foundation for healing, resilience, and parenting from a place of wholeness.
You deserve support, just like your baby does. Reach out. Speak up. You are worth it.
Families of preterm and sick newborns face unique challenges that require strong support, advocacy, and collaboration. Around the world, dedicated parent and patient organizations provide vital guidance, raise awareness, and drive improvements in neonatal and maternal care. Their voices ensure that the needs of babies and families are heard at every level – from local communities to international policy.
Collaboration Opportunities for Parent and Patient Organizations
If you have already established a charitable parent or patient organization, advocacy group, or self-help initiative, we welcome your interest in collaborating with us. Ideally, your group has a clear vision for supporting families of preterm babies in your region and a defined path toward achieving these goals.
Accepted parent and patient organizations benefit from:
Regular exchange and digital meetings with our global network, including updates on GFCNI’s activities
Workshops and training opportunities designed to strengthen your impact
Access to a worldwide community of organizations eager to share knowledge and experience
Free information and campaign materials, potentially available in your local language
Opportunities to participate as supporters in global awareness campaigns
Occasional involvement in research projects as parent or patient representatives
Our Global Network of Parent and Patient Organizations
Across the world, parent and patient organizations are leading change for preterm and sick newborns and their families. By joining our global network, we create a stronger voice for advocacy, share valuable knowledge and resources, and work together to ensure that every baby and family has access to the care and support they need.
Below, you can explore the wide range of parent and patient organizations that are already part of our international community. If your organization is interested in joining our network, we warmly invite you to contact us at network(at)gfcni.org.
When Nash Keen was born, he weighed just 10 ounces, less than a can of soda. His journey is one of medical innovation, relentless teamwork, and the unique capabilities of University of Iowa Health Care’s Stead Family Children’s Hospital, one of the few places in the world equipped to treat babies born so early.
Nash’s birth came just after crossing the hospital’s 21-week threshold for active intervention — timing that high-risk obstetrician Malinda Schaefer, MD, PhD, called “a new frontier in maternal-fetal medicine.” A multidisciplinary team of 21 neonatologists, nine NICU fellows, and dedicated nurse practitioners, nurses, respiratory therapists, dietitians, pharmacists, physical and occupational therapists, and more sprang into action. They inserted a breathing tube — an extraordinary feat for a baby so small — and began targeted organ support using hemodynamic monitoring, a technique pioneered at University of Iowa that allows clinicians to modify treatment based on real-time assessments of heart function and blood flow.
“When he was first born, his blood pressure was really low,” said neonatologist Amy Stanford, MD. “With hemodynamics, we could see that his heart was functioning well, so we adjusted our approach.” This precision medicine approach cuts the chance of death or major brain bleeding in very premature babies in half.
Over the next six months in the NICU, Nash underwent surgery, received dozens of medications, and was monitored around the clock. “They were on top of it every step of the way,” said his father, Randall Keen.
“They made sure we were well-informed and kept us involved in all the decision-making.”
Today, Nash is learning, playing, and growing like any other two-year-old. His Guinness World Record-breaking outcome reflects the strength of academic medicine: a blend of cutting-edge science, collaborative care, and compassion that gives even the smallest, most vulnerable patients a chance at life.
“Every patient teaches us something,” said Stanford. “And we use those lessons to improve care for the next.”
Scientists linked a maternal gut microbe that degrades key pregnancy hormones to early labor, potentially serving as a predictive risk biomarker.
During pregnancy, expectant mothers often take steps to prepare for the arrival of their baby, such as taking vitamins and supplements and avoiding smoking or alcohol. While a typical pregnancy lasts about 40 weeks, preterm birth—defined as birth before 37 weeks of gestation—can occur and is the leading cause of neonatal and under-five mortality worldwide.
Although much research has focused on the vaginal microbiome and its potential connection to preterm birth, the role of the gut microbiome remains less understood. This gap in knowledge motivated a group of researchers in China to explore the maternal gut microbiome more closely and assess its potential link to preterm birth.
In a recent study, published in Cell Host & Microbe, the team identified maternal gut microbes associated with a higher risk of preterm birth during early pregnancy, especially those that can degrade estradiol, an important pregnancy hormone.2 The researchers hope to further explore this association of estradiol-degrading bacteria as potential predictive biomarkers for preterm birth.
First, the researchers gathered stool and blood samples from two groups of pregnant women—one in early pregnancy and the other in mid-pregnancy. Using metagenome and 16S rRNA sequencing, the team identified similar gut microbiota profiles across the women. From this, they found five prevalent genera: Blautia, Faecalibacterium, Bacteroides, Anaerostipes, and Streptococcus. At the same time, they tracked each woman’s preterm delivery status.
The researchers then turned to statistical models to dive deeper into the relationship between the gut microbiota and factors like gestational duration and preterm birth. Their analysis uncovered 11 specific genera linked to these outcomes, but one species stood out: Clostridium innocuum. This bacterium had the strongest connection to preterm birth.
Intrigued by C. innocuum, the team investigated its role in sex hormone metabolism and found that it makes an enzyme that degrades estradiol, a hormone important in pregnancy. To explore this further, they tested the bacterium’s estradiol degrading ability in female mice across different gestational periods (from early pregnancy to having a near-term fetus) and found that doses of C. innocuum significantly reduced estradiol levels by converting it into estrone. Additional analysis revealed key enzymes in the bacterium that played a critical role in this process.
Because of these findings, the researchers hypothesize that a high prevalence of C. innocuum may dysregulate estradiol levels and increase the risk of preterm birth. However, the team also acknowledged that scientists would need to evaluate more cohorts to validate these findings in broader populations.
“This study suggests that for pregnant women or women preparing to become pregnant, it may be important to monitor their gut microbiome to prevent potential adverse pregnancy outcomes,” said study coauthor An Pan, an epidemiologist at Huazhong University of Science and Technology in a press release.
Liberia, officially the Republic of Liberia, is a country on the West African coast. It is bordered by Sierra Leone to its northwest, Guinea to its north, Ivory Coast to its east, and the Atlantic Ocean to its south and southwest. It has a population of around 5.5 million and covers an area of 43,000 square miles (111,369 km2). The official language is English. Over 20 indigenous languages are spoken, reflecting the country’s ethnic and cultural diversity. The capital and largest city is Monrovia.
Liberia has 5,000 full-time or part-time health workers and 51 Liberian doctors to cater to a population of 3.8 million, according to the 2006 health survey. That’s the equivalent of one doctor serving about 76,000 civilians. Most of the hospitals, clinics and equipment were destroyed as a result of the 14-year civil war from 1989 to 2003. Strengthening the health sector faces financial problems. The government used only 16.8% of the total health expenditure in the country.
Liberia is heavily dependent on the international community for health infrastructure and assistance. International aid organizations assist the government in rebuilding medical facilities and providing basic health care to its citizens. The World Health Organization (WHO) donated equipment and helped provide and assist in vaccinating people to prevent the spread of many infectious diseases.
The Global Alliance for Vaccines and Immunization (GAVI) is investing $160 million to improve Liberia’s health care system and improve the quality of immunization services. The international medical humanitarian organization Médecins Sans Frontières (MSF) helped Liberia after the civil war (2003) by running free hospitals, treating more than 20,000 women and children each year.
Monrovia Liberia: Liberia has received a major boost to its healthcare sector as 26 leading medical professionals from the United States, Canada, Europe, and beyond have arrived for the Liberia Medical Mission (LMM) 2025. The mission, a special initiative led by President Joseph Nyuma Boakai’s administration, represents a transformative step toward improving healthcare delivery across the country.
As part of the mission, over $500,000 worth of life-saving medicines will be distributed across five counties, aligning with President Boakai’s vision for a healthier and stronger Liberia.
The mission’s launch was celebrated with a special reception at the Tea House, Executive Mansion in Monrovia, where President Boakai expressed deep gratitude for the medical team’s commitment to making a difference.
“This mission exemplifies the power of compassion and service,” President Boakai said. “You’ve left the comfort of your homes to bring healing and hope to our people. Liberia is truly grateful for your selfless contributions. My administration is committed to supporting and expanding this mission so that more lives can be saved.”
He reiterated the government’s dedication to modernizing Liberia’s healthcare system, ensuring that medical professionals and facilities are equipped to improve service delivery nationwide.
Expanding Medical Care Across Liberia’s Counties
The Liberia Medical Mission 2025 aims to provide essential healthcare services to thousands of Liberians in need. Over $500,000 worth of medicines will be distributed to hospitals and clinics in Gbarpolu, Cape Mount, Bomi, Grand Bassa, and Montserrado counties. The mission will provide the following critical healthcare services:
• Cataract Surgeries at Emirates Hospital: Restoring vision to patients from Gbarpolu, Bomi, Cape Mount, and Montserrado counties.
• Mental Health Awareness & Training: Focused on trauma-informed care, with training for healthcare workers, educators, and security agencies.
• CPR & Emergency Training: Aimed at enhancing life-saving emergency response skills for 7 security personnel.
• Biomedical Equipment Repairs: At John F. Kennedy Memorial Hospital and other key medical centers to improve service efficiency.
• Specialized Urology Surgeries: Performed by leading urologists at JFK Memorial Hospital.
This initiative is being led by Minister Mamaka Bility, the Minister of State Without Portfolio for Presidential Affairs, and is directly overseen by the President’s Delivery Unit (PDU). Minister Bility spoke on February 21, 2025, at the event, highlighting the government’s unwavering commitment to reshaping Liberia’s healthcare sector.
“This mission reflects President Boakai’s vision for a reformed healthcare system,” Minister Bility stated. “We are honored to host the Liberia Medical Mission again this year, as their critical services will touch and improve countless lives.”
Liberians Abroad Give Back to Their Country
Many of the medical experts participating in this mission are Liberians who have spent years abroad, gaining experience in their fields, and are now returning home to contribute to the development of their country’s healthcare system.
As the mission progresses, President Boakai has called on all Liberians to work together with the medical team to maximize its life-saving impact.
“This is a national effort, and every Liberian has a role to play in ensuring the mission’s success,” President Boakai said. “My administration remains dedicated to advancing healthcare policies and mobilizing resources to build a more resilient healthcare system for Liberia.”
The Liberia Medical Mission 2025 offers free medical checkups, surgeries, and other essential services at no cost to the government or private institutions, making it a crucial component in the country’s healthcare transformation.
A Step Toward a Healthier Liberia
The Liberia Medical Mission 2025 stands as a testament to the collective efforts of both international and Liberian medical professionals who are dedicated to improving healthcare in the country. With the government’s ongoing support, this initiative is set to deliver lasting benefits for thousands of Liberians in need of medical care.
The World Health Organization (WHO) has officially designated Health Canada, the Ministry of Health, Labour and Welfare/Pharmaceuticals and Medical Devices Agency (MHLW/PMDA) of Japan, and the Medicines and Healthcare products Regulatory Agency (MHRA) of the United Kingdom as WHO-Listed Authorities (WLAs), a status granted to national authorities that meet the highest international regulatory standards for medical products.
With these latest designations, WHO expands the growing list of WLAs, now involving 39 agencies across the world, supporting faster and broader access to quality-assured medical products, particularly in low- and middle-income countries (LMICs).
In addition, the Republic of Korea’s Ministry of Food and Drug Safety (MFDS) – one of the first regulatory authorities to complete the WLA assessment for both medicines and vaccines in October 2023 – has had its listing scope successfully expanded, now covering all regulatory functions.
“This recognition reflects the deep commitment of these authorities to regulatory excellence,” said Dr Tedros Adhanom Ghebreyesus, WHO Director-General. “Their designation as WHO-Listed Authorities is not only a testament to their robust regulatory systems but also a critical contribution to global public health. Strong and trusted regulators help ensure that people everywhere have access to safe, effective, and high-quality medical products.”
Around 70% of countries worldwide still face significant challenges due to weak or inadequate regulatory systems for evaluating and authorizing medical products. The WLA framework promotes regulatory convergence, harmonization and international collaboration, allowing WHO Prequalification Programme and regulatory authorities, especially those in LMICs, to rely on the trusted work and decisions of designated agencies. This collaboration supports efficient use of limited resources, enabling better and faster access to quality-assured life-saving medical products to millions more people.
“The principle of reliance is central to WHO’s approach to regulatory systems strengthening and a cornerstone for effective, efficient and smart regulatory oversight of medical products,” said Dr Yukiko Nakatani, WHO Assistant Director-General for Health Systems, Access and Data. “WHO-Listed Authorities are key enablers in promoting trust, transparency, and faster access to quality-assured medical products, especially in low- and middle-income countries.”
In a world where health threats, including substandard and falsified medical products, know no borders, WLAs also serve as critical pillars of preparedness and equity, making life-saving products available more broadly, rapidly and efficiently.
The designations follow a rigorous performance evaluation process carried out by WHO using its globally recognized benchmarking and assessment tools. These evaluations were reviewed by the Technical Advisory Group on WLAs (TAG-WLA), which convened in June 2025.
Canada, Japan and the UK’s regulatory authorities were previously recognized as Stringent Regulatory Authorities (SRAs). Their designation under the WLA framework marks an important step in moving beyond the old SRA system, while ensuring continuity and stability in global procurement processes of quality-assured medical products.
Launched in 2022 to replace the previous SRA model, the WLA initiative provides a transparent and evidence-based pathway for global recognition of regulatory authorities to facilitate regulatory convergence and reliance. It builds on decades of WHO leadership to help countries work together more closely on regulating medical products, speeding up access to safe, effective and quality-assured medical products for people around the world.
Here is our list of the best team building ideas for healthcare professionals.
Team building ideas for healthcare professionals are exercises, activities, and games that build morale and keep healthcare employees positive and engaged. Examples include daily positive affirmations, Secret Number, and Mystery Diagnosis. The purpose of these activities is to build healthcare teams that are motivated to best serve patients.
List of team building ideas for healthcare professionals
It is not uncommon for healthcare professionals to feel stress and fatigue when under constant pressure. As a result, healthcare leaders must engage in fun and meaningful team building exercises and activities with their teams. Here is our list of the top ideas to improve bonds between teams of healthcare workers.
1. Thanks and Gratitude Circle
If you want to boost communication activities for healthcare workers in your facility, then start by fostering a culture of recognition and gratitude on your team. Building and maintaining a positive work culture can lay the foundation for a strong and successful team of healthcare professionals.
There are different ways you can show gratitude toward your team and make a fun game out of it. Communication is key in any workplace, so we recommend conducting your gratitude activity by getting your entire team together at the end of each day.
You should begin by having all team members sit together in a circle. Then, you can go around the circle and have each employee express gratitude for one teammate. A great way to think about this exercise is to have each participant start with the words, “Today, I want to thank blank.” For example, you could say: “Today, I want to thank Amanda for going above and beyond in treating her patients and helping other members of the team who were struggling with their patients.”
This communication exercise is a meaningful way for all teammates to build camaraderie by sharing words of thanks and gratitude toward other team members. Communication exercises for recognition and appreciation are also a great way to end each day.
2. Daily Positive Affirmations
One of the most beneficial team building activities for caregivers is to practice positive affirmations at work.
Positive affirmations are phrases that can help you build yourself up and overcome negative thoughts.
Here are a few examples:
I am making a difference.
I will show kindness and empathy to every patient.
I will care for myself as I care for my patients.
I help others in their most vulnerable moments.
I am energized and ready for the day.
I will make today a great day.
I am strong.
I am proud of myself and the work I do.
Affirmations like these are ideal for all employees to stay motivated and positive. Caregivers must remain positive as they work with patients dealing with difficult and sometimes life-threatening diseases and disorders.
Positive affirmations can be a great help in allowing employees to free their minds and stay positive, even during a tough day at work. Plus, the whole team can collectively build their positivity and confidence by having employees recite positive affirmations together.
3. Coffee Chats and Tea Time
As a doctor, it can be challenging to make time to socialize with your team regularly. As a result, one of the best team building ideas for doctors is to set aside time each week to socialize with their team over a cup of coffee or tea.
Gathering in the break room with your team can provide the perfect opportunity to get to know each other and take a much-needed break in the middle of a busy day. To make your coffee chat and tea time a success, you should remember to stock up your break room with various coffees and teas.
In addition, you should make a goal for yourself to chat with a new coworker new each week. It can be tempting to talk to your well-known coworkers and friends, but by chatting with a new colleague each week, you will meet different teammates while building new relationships in your workplace.
4. Line Leader
When it comes to communication activities for healthcare workers, the exercise that may help your team most is a nonverbal communication game.
Nonverbal games are an effective way to build communication skills. Instead of relying solely on spoken words, healthcare professionals can learn to look at nonverbal cues and body language to decipher patients’ and colleagues’ needs and wants.
Line leader is a nonverbal communication game in which the group must form a line in a specific order without talking to each other. Instead, teammates must rely on silent cues and body language to get in the correct order while working together. The moderator is the only player allowed to speak in this game.
For example, the game’s moderator can ask the team to get in a line starting from January birthdays through December birthdays. In this case, the first player in the line should be the team member with the first January birthday, while the last player in line should be the member with the last December birthday.
Since players may not speak to each other, they must determine the correct order by using body language and signs. The game Line Leader is an ideal activity that can help healthcare professionals better understand the nonverbal communication cues they may receive from patients or colleagues.
5. Secret Number
A nonverbal communication game your team can play together is Secret Number. To play this game, you should break your group into two teams of three to ten players. These teams will ultimately compete against each other, and it is best if your teams are large.
You should begin the game by designating one player as the moderator. The game’s moderator should communicate instructions or guidelines to other players. The moderator should then give each team a piece of paper and a pencil.
Before the game officially begins, each team should devise a secret code to use throughout the activity. This secret code will come in handy when players get stumped, as they will not be allowed to speak with each other or write anything down.
You can use the following steps to ensure a smooth game:
The moderator gives each team leader a “secret number.”
Each leader should communicate this number to each member of their team one by one. However, the leader should not speak or spell out the number with their hands.
As each team member reads the leader’s nonverbal clues, the player should write down their guess of the secret number.
Once the team leader has communicated with each participant, they should signal to the moderator that their team is finished.
The winner of the game is the team that finishes the fastest and can guess the correct number.
To keep the game exciting, you should switch team leaders for each turn so different players can have the opportunity to lead. Secret Number is a great way to get teams accustomed to nonverbal cues as they engage in friendly competition.
6. Care Packages
Among the different types of healthcare professionals in the workforce, nurses typically feel higher levels of stress and burnout. As a result, one of the most ideal team building exercises for nurses to combat burnout is to have the team leader send out care packages.
By sending care packages to your team, you are sending the message that you care about employee wellbeing.
Here are a few items you can include in your care packages for self-care:
Herbal teas
Bath bomb
Face masks
Candles
Meditation subscription
Positive affirmation cards
Snacks
Assembling care packages is a great exercise to decrease burnout, boost morale, and increase employee satisfaction. A well-rested team of nurses is most likely to provide the utmost level of care to patients.
7. Question of the Day
One of the most classic healthcare team building games is icebreakers. This team building activity works well for new teams that are just meeting each other or teams that want to get to know each other better.
A great icebreaker to begin each shift with is Question of the Day. As part of this icebreaker exercise, designate one person on your team to come up with the day’s question. From there, the employee tasked with creating the question should kick off the icebreaker exercise by stating the question and their own answer. Question of the Day is a great icebreaker to help coworkers learn more about each other.
A few suggestions for Question of the Day prompts include:
What is one important skill that all nurses should have?
If you had an extra hour in your day, what would you do during that time?
If you were not a nurse, what kind of job do you think you would have?
Icebreakers can help teams build unity by learning more about each other. Plus, when a team feels more united, they are more likely to excel in their roles and keep hospital operations running smoothly.
8. Workshops
Workshops provide an excellent opportunity to learn new things while spending time with coworkers. We recommend organizing monthly workshops that employees can attend throughout the work day or on their breaks.
Although the workshop may take place during the workday, it is important to know that these sessions do not have to be directly related to job training or building on-the-job skills. Instead, these workshops should focus on building camaraderie while promoting employees’ well-being.
Here are a few suggestions for the types of workshops that you can get your team excited about:
Yoga and meditation
Healthy habits
Journaling
Resume writing
Networking
Each workshop will provide employees with the opportunity to decompress while learning new skills that can help them in their daily job.
9. Board Games
If you are looking for healthcare team building games to engage your group, start with board games. Board games are a fun and competitive way to get your team to interact.
Some suggestions:
Monopoly
Sorry!
Trouble
The Game of Life
Taboo
Operation
It can be a good idea to keep a handful of board games in your facility’s break room. Having easy access to a few board games allows your team to choose different options to play with teammates during their lunch break or at other team building events.
10. Escape Room
If you are looking for a team building activity that promotes problem-solving and resolution skills, then consider completing an escape room challenge. Escape rooms are activities in which teams are locked in a room full of puzzles and tasks that they must complete to escape.
To successfully complete an escape room, team members must communicate effectively to solve the many puzzles and challenges. You can find a variety of themes to meet the needs and interests of your whole team.
Fun escape room themes include:
Mystery
Science or high-tech
Fantasy
Horror or suspense
Holiday
Although teammates may have differing perspectives and ideas, all players need to work together to escape the room within the given time frame. Escape rooms contain different puzzles and clues that teams must work together to solve, making this activity an optimal choice for a team of healthcare professionals looking to boost teamwork and trust.
11. Team Outing
Engaging with your team outside the workplace can provide a much-needed change of scenery while providing an opportunity to get to know each other and socialize more. Fun activities and team outings can help boost employee happiness and morale.
A few examples:
Happy Hour
Boat ride
Fancy dinner
Karaoke night
Paint and sip class
Science museum
Art museum
When it comes to team building ideas for doctors, you cannot go wrong with visiting a science museum. In fact, a group of doctors may be especially excited to enjoy a trip to the local science museum and spend an afternoon learning and exploring.
12. Mystery Diagnosis
Role-playing is one of the best team building exercises for nurses that can help improve their patient care skills. To conduct a role-playing exercise with your team, you will need to choose one team member who will act as the doctor.
Here are a few steps to keep in mind when participating in this role-playing game with your team:
You can start by having the team “doctor” leave the room. Once this player leaves, the rest of the team should come up with an illness or injury. The players should discuss symptoms and scenarios they can later share with the team’s doctor.
When the doctor comes back into the room, they will diagnose the patient based on the information the remaining players share.
To make the game challenging, you should give the doctor a timeframe of about 90 seconds to fully diagnose the patient.
If the team doctor can provide the correct diagnosis in the given timeframe, then the doctor can be declared the winner. The other players win the game if the doctor fails to provide the correct diagnosis.
You can encourage your staff to act out rare and obscure diseases or illnesses to make the game even more fun. For example, some players may pretend to fall asleep while doing everyday activities. The doctor of the game would then need to understand why patients are exhibiting such strange behavior, and ultimately provide a diagnosis.
Role-playing can be helpful for nurses to build upon their analysis, critical thinking, and problem-solving skills. This role-playing exercise is also a great way for a team of nurses to improve their relationships with each other as a team.
13. Bake-Off
Having a team bake-off is a fun way for your team to show off their baking skills while building collaboration skills.
To host a team bake-off, you should split your group into teams of three. Next, have each team choose a pastry or dessert to bake together. You can provide a two-hour time limit for each team to bake their dessert.
Once the teams have finished baking, you should have a team of judges taste each creation to determine a winner. A team bake-off is a great team building exercise as you can get teammates in the kitchen with each other working together on a tasty dessert.
Conclusion
Team building exercises are a great way to get your team of healthcare professionals more comfortable with each other. These activities also have the power to motivate teams to work more efficiently and in sync with one another, especially when serving patients.
Overall, team building is essential for healthcare professionals and it is a great skill for all teams to master. By engaging in team building exercises, you are taking the right steps toward improving relationships between team members with each other, which can lead to happier employees and satisfied patients.
FAQ: Team building ideas for healthcare professionals
Here are answers to questions about team building ideas for healthcare professionals.
What are team building ideas for healthcare professionals?
Team building ideas for professionals are activities that build camaraderie among healthcare teams while keeping employees motivated and happy. Healthcare professionals need to build their team’s morale and collaboration skills with each other both in and out of the workplace. As a result, team building exercises and activities come in handy when you are looking to form a stronger and more united team.
What are some good team building ideas for healthcare professionals?
There are many team building ideas to engage healthcare teams. Here are a few examples of team building exercises and activities for healthcare professionals:
Icebreaker
Coffee break
Team outing
Escape rooms
Team building activities can motivate employees to work effectively as a team, which can also help employees when they are caring for patients or working hard to solve a problem.
How do you encourage teamwork on healthcare teams?
It is important to encourage your team to work efficiently and collaboratively. A creative way to encourage teams to work together is by organizing team building activities for caregivers and other healthcare professionals.
Team building activities are sure to get your entire team working together as they have fun.
If a baby is born before 37 weeks, they’re considered a preemie, and their senses might develop a bit differently from those of full-term babies. This doesn’t mean you need to worry! Knowing this can help you better understand and support your little one! During pregnancy, babies develop their senses in a specific order: touch, movement and balance, smell, taste, hearing, and vision. But once they’re born, these senses begin to work in reverse order. This means your preemie’s vision and hearing are quickly adjusting to the lights, sounds, and new environment around them. Preemies have their milestones adjusted for their corrected age, but their visual development might align more closely with their actual age. To help your baby’s vision, use toys with black, red, and white colors—these are easiest for them to see in the early months.
There are many different members of the health care team that you may meet in the NICU. Besides a bedside nurse, every baby has a NICU medical team managing the overall care of your baby. Each team is supervised by an attending neonatologist. Below is some basic information on the other members of your health care team.
Attending Neonatologists: Doctors who specialize in the care of newborns (neonates).
Chaplains: Give emotional and spiritual support to families and patients of all faiths and cultures.
Clinical Leaders and Charge Nurses: Senior staff members who are able to take care of any problems or concerns.
Fellows: Doctors that are training to be neonatologists.
Lactation Team: Trained to help you reach your breastfeeding goals and answer any pumping/breastfeeding questions.
Licensed Practical Nurses (LPN): A nurse who works under the supervision of an RN to provide direct patient care. LPNs give much of the same care as RNs, except they do not give IV medicines.
Neonatal Nurse Practitioners (NNP): A nurse who has finished advanced graduate education and training. A NNP can help the Attending Neonatologists and Pediatric Surgeons treat babies and perform certain procedures.
Nurse Case Managers: Registered Nurses who provide care coordination for you and your baby while you are at the hospital. They will also help with the discharge process.
Nutritionists /Dieticians: Make sure babies are getting the right amount of calories and nutrients for the best growth and development. They will also give nutrition education for special diet needs.
Occupational Therapists (O.T.) and Physical Therapists (P.T.): Focus on babies’ movements and motor development. An O.T. may also help with feeding and oral stimulation.
Parent Advisors: Other parents who have had babies in the NICU. They give emotional support to families. Also, they lead the weekly Parent Pizza Night.
Patient Care Assistants (PCA): Also known as Patient Support Assistant (PSA), they work under the supervision of an RN. They can take vital signs, perform heel sticks, give baths, and feed babies.
Pharmacists: Help the doctor prescribe drugs for your baby. They also watch how well the drugs work for your baby and make sure the drug levels are right in the blood.
Registered Nurses (RN): Nurses who specialize in the nursing care of your baby. They assess your baby’s condition and progress and carry out the doctor’s orders. The RN will tell the doctor or NNP if there are any changes in your baby’s condition.
Residents: Doctors who are training to become pediatricians (a doctor who cares for children).
Respiratory Therapists: Manage and adjust the ventilators and other breathing equipment. They perform treatments that help with breathing and lung function.
Social Workers: Give emotional support, crisis intervention, information on community resources, and help with communication between families and the medical team.
Unit Clerks: Often the first people you meet when you enter the NICU. They answer the phone when you call to check on your baby and take care of many of the NICU’s administrative needs.
Volunteers: NICU volunteers have attended special training, and they help with many different tasks in the unit. They can hold and rock babies (if you wish) when parents are not able to.
Tiny fingers grasp at invisible demons as the sterile beeps of hospital monitors become the haunting soundtrack to a newborn’s first memories. This haunting image raises a profound question: Can babies experience Post-Traumatic Stress Disorder (PTSD) from birth? As our understanding of infant mental health grows, researchers and healthcare professionals are increasingly exploring the possibility that even the youngest among us may be vulnerable to the lasting effects of trauma.
PTSD, a mental health condition triggered by experiencing or witnessing a terrifying event, has long been recognized in adults. The American Psychiatric Association reports that approximately 3.5% of U.S. adults are affected by PTSD in any given year. However, the concept of PTSD in infants is a relatively new area of study, challenging our preconceptions about early childhood experiences and their long-term impacts.
As we delve deeper into the realm of infant mental health, it becomes crucial to consider the potential for trauma during the earliest stages of life. The birth process itself, along with the immediate postnatal period, can be a source of significant stress for newborns. This realization has led to a growing awareness of the importance of nurturing infant mental health from the very beginning.
The Possibility of PTSD in Babies: Exploring the Evidence
Current research on infant PTSD is still in its infancy, but emerging studies suggest that babies may indeed be capable of experiencing trauma-related stress responses. While the traditional diagnostic criteria for PTSD were developed with adults in mind, researchers are now adapting these frameworks to better understand and identify trauma in non-verbal infants.
One of the primary challenges in diagnosing PTSD in babies lies in their inability to verbalize their experiences and emotions. Unlike adults who can describe their symptoms and traumatic events, infants communicate their distress through behavioral and physiological cues. This necessitates a different approach to identifying and assessing trauma in the youngest patients.
Despite these challenges, healthcare professionals have identified several signs and symptoms that may indicate trauma in babies. These can include heightened startle responses, difficulty sleeping, excessive crying or irritability, and problems with feeding. Some infants may also exhibit a withdrawal from social interactions or show signs of hypervigilance, constantly scanning their environment for potential threats.
It’s important to note that while these symptoms may be indicative of trauma, they can also be associated with other developmental or medical issues. This underscores the need for comprehensive assessments and a nuanced understanding of infant behavior and development when evaluating potential trauma responses.
Potential Causes of Birth-Related Trauma in Infants
Several factors during the birth process and immediate postnatal period can potentially contribute to trauma in newborns. Complicated or traumatic deliveries, such as those involving emergency cesarean sections, forceps, or vacuum extraction, may be particularly stressful for infants. These interventions, while often necessary for the safety of mother and child, can introduce an element of physical and emotional distress that may have lasting effects.
Premature birth is another significant risk factor for infant trauma. Babies born before 37 weeks of gestation often require extended stays in the Neonatal Intensive Care Unit (NICU), exposing them to a range of stressful experiences. The NICU Stays and Babies: Long-Term Effects, Impact, and Potential for PTSD can be profound, influencing both physical and psychological development.
Separation from parents immediately after birth can also be a source of distress for newborns. The importance of early bonding and skin-to-skin contact is well-documented, and disruptions to this process may contribute to feelings of insecurity and anxiety in infants. This separation is often unavoidable in cases of medical emergencies or when babies require specialized care, but its potential impact on infant mental health should not be overlooked.
Medical interventions and procedures, while often life-saving, can be another source of trauma for newborns. Frequent blood draws, intubation, and other invasive procedures can be painful and frightening for infants, potentially contributing to a heightened stress response and increased risk of trauma-related symptoms.
PTSD in NICU Babies: A Closer Look
Babies who spend time in the Neonatal Intensive Care Unit (NICU) face unique challenges that may increase their vulnerability to trauma-related stress. The NICU environment, while designed to provide life-saving care, can be overwhelming for fragile newborns. Constant noise from medical equipment, bright lights, and frequent handling can disrupt an infant’s developing sensory systems and sleep patterns.
Research on the long-term effects of NICU stays on infant development has revealed a range of potential impacts. These can include delays in cognitive and motor development, difficulties with emotional regulation, and increased risk of behavioral problems later in childhood. While not all NICU graduates will experience these challenges, the potential for lasting effects underscores the importance of trauma-informed care in these critical early days.
Studies examining PTSD symptoms in NICU graduates have yielded intriguing results. A study published in the Journal of Perinatology found that infants who spent time in the NICU showed higher rates of PTSD-like symptoms compared to full-term infants who did not require intensive care. These symptoms included heightened startle responses, difficulty with emotional regulation, and problems with attachment.
It’s important to note that while these findings suggest a potential link between NICU experiences and trauma-related symptoms, more research is needed to fully understand the relationship. The complex interplay of medical, environmental, and developmental factors in the NICU makes it challenging to isolate the specific causes of these symptoms.
Recognizing and Addressing Trauma in Infants
Identifying trauma in non-verbal infants requires a keen eye and a deep understanding of infant behavior and development. Behavioral and physiological indicators of infant distress can include changes in sleep patterns, feeding difficulties, excessive crying or irritability, and withdrawal from social interactions. Some infants may also exhibit physical symptoms such as increased heart rate, rapid breathing, or sweating in response to perceived threats.
The importance of early intervention cannot be overstated when it comes to addressing potential trauma in infants. Research has shown that early experiences play a crucial role in shaping brain development and laying the foundation for future mental health. By identifying and addressing trauma-related symptoms early, healthcare providers and caregivers can help mitigate the long-term impacts and promote healthy development.
Trauma-informed care for newborns and NICU babies is an emerging approach that recognizes the potential for early life experiences to impact long-term well-being. This approach emphasizes creating a nurturing environment that minimizes stress and promotes healing. Key elements of trauma-informed care include minimizing painful procedures when possible, promoting skin-to-skin contact with parents, and creating a calm, low-stimulation environment.
Supporting Infant Mental Health and Preventing PTSD
Promoting infant mental health and preventing trauma-related stress begins with recognizing the importance of early bonding and attachment. Skin-to-skin contact, also known as kangaroo care, has been shown to have numerous benefits for both full-term and premature infants. This practice helps regulate an infant’s body temperature, heart rate, and breathing, while also promoting feelings of security and reducing stress.
Minimizing separation between infants and parents is another crucial aspect of supporting infant mental health. When possible, rooming-in arrangements that allow parents to stay with their newborns can help promote bonding and reduce stress for both babies and parents. In cases where separation is necessary due to medical needs, efforts should be made to facilitate frequent visits and involvement in care routines.
Creating a calm and nurturing environment for newborns is essential, particularly in hospital settings. This can involve reducing noise levels, dimming lights during rest periods, and minimizing unnecessary handling or procedures. In the NICU, practices such as clustered care (grouping necessary interventions to allow for longer periods of undisturbed rest) can help reduce stress on fragile infants.
Providing support for parents of traumatized infants is also crucial. Postpartum PTSD: Recognizing and Overcoming Birth Trauma is a reality for many parents, particularly those who have experienced complicated deliveries or have babies in the NICU. Offering counseling, support groups, and education about infant mental health can help parents better understand and respond to their baby’s needs while also addressing their own emotional well-being.
As our understanding of infant mental health continues to evolve, it becomes increasingly clear that the experiences of our earliest days can have profound and lasting impacts. While the concept of PTSD in babies may still be controversial in some circles, the growing body of research suggests that infants are indeed capable of experiencing trauma-related stress responses.
Ongoing research in the field of infant PTSD is crucial to further our understanding of how early life experiences shape long-term mental health outcomes. As we continue to explore this complex topic, it’s essential to approach newborn and NICU care with a trauma-informed perspective, recognizing the potential for both positive and negative impacts on infant development.
By acknowledging the importance of infant mental health and implementing practices that support early bonding, minimize stress, and promote healing, we can work towards ensuring that every child has the best possible start in life. As we move forward, it’s crucial that healthcare providers, researchers, and policymakers continue to prioritize the mental health needs of our youngest and most vulnerable patients, recognizing that the foundations of lifelong well-being are laid in these earliest moments of life.
Premature infants require specialized care, and nurses need to have specific skills and knowledge to provide this care effectively.
Objective
To evaluate the impact of an on-the-job training program on the improvement of nurses’ knowledge and practice related to creation of a healing environment and clustering nursing procedures.
Methods
From January to April 2022, a study utilizing a one-group pre- and post-test design was conducted at NICUs in governmental hospitals. The study participants involved 80 nurses working in these NICUs. Researchers used predesigned questionnaire and checklist practice to collect the data pre and post the intervention.
Results
37.5% of the participants were aged between 25 and less than 30 years, with a mean age of 28.99 ± 7.43 years. Additionally, 73.7% of the nurses were female, with a mean experience of 9.45 ± 3.87 years. Prior to the intervention, the study found that a majority of the nurses (62.4%) demonstrated poor knowledge. However, after the intervention, a significant improvement was observed, with 60.0% of the nurses demonstrated good knowledge. Likewise, prior to the intervention, the study revealed that the majority of the nurses (83.8%) exhibited incompetent practice. However, post-intervention, a substantial improvement was observed, with 81.3% of the nurses demonstrated competent practice.
Conclusion
On-the-job training had significant improvements in nurses’ knowledge and practices regarding applying healing environments and clustering nursing care. On-the-job training is suggested as an adaptable, effective and low-cost technique to train nurses. To maintain the improvement achieved, ongoing instruction, feedback, assessment/reassessment, and monitoring are encouraged.
Abstract: Effective leadership in today’s dynamic environments rests not simply on experience, but on intentional coaching and apprenticeship. This article explores how coaching emerging leaders through structured apprenticeship models foster transferable skills, organizational continuity, and leadership identity. Drawing on scholarly research in leadership education, youth development, and coaching theory, it outlines actionable strategies for embedding coaching-as-apprenticeship within professional settings. Case studies and frameworks highlight how critical reflection, mentor guided practice, and identity formation synergize to elevate both individual and organizational performance.
Closing teaser: If you are ready to transform your leadership legacy by raising apprentices, not just subordinates, read on to discover how to build, guide, and sustain the next generation of leaders
Introduction: The Leadership Gap and the Coaching Imperative Organizations often struggle with leadership continuity, not because of a shortage of talent, but due to the lack of developmental pathways for emerging leaders. Traditional training is often episodic, outcome-focused, and disconnected from real-world work. In contrast, apprenticeship-style coaching integrates on-the-job practice, guided reflection, and mentor scaffolding, offering a more durable model for leadership development. This approach recognizes that leadership is not merely a set of competencies, but a mindset and identity forged over time. The urgency to shift from transactional leadership development to transformational apprenticeship-based coaching is underscored by the increasing volatility of organizational environments, where agile and empathetic leadership is critical. Coaching emerging leaders through apprenticeship enables them to learn by doing, internalize the organization’s values, and develop the confidence necessary to lead effectively in complex situations.
Coaching Young Leaders: Foundations and Key Benefits:
Research increasingly supports the idea that coaching has a disproportionate impact when targeted at younger or less experienced leaders. Not only do these individuals exhibit higher growth trajectories in leadership identity and self-efficacy, but they also tend to show increased engagement and retention. Coaching becomes a vehicle for establishing positive habits, fostering psychological safety, and creating alignment with core organizational values at the earliest stages of one’s leadership journey. Coaching supports the holistic development of young leaders, improving both their technical capabilities and their emotional intelligence. Moreover, when coaching is introduced early, it becomes embedded in their leadership DNA, making them more likely to coach others in the future. This creates a ripple effect of development, where coaching becomes not just a practice but a cultural norm. Organizations that invest in coaching young talent are investing in a long-term, sustainable leadership pipeline.
Apprenticeship as a Leadership Model:
Unlike ad hoc mentorship, apprenticeships are structured to emulate expert-apprentice learning paradigms found in fields such as medicine or skilled trades. These involve a deliberate, phased progression: observation, participation, leadership with supervision, and finally autonomous execution. Apprenticeships in leadership also emphasize the social construction of leadership identity. Through cycles of feedback and reflective inquiry, the emerging leader gradually integrates personal values with professional expectations. This model positions leadership as an evolving identity, not a static role. Apprenticeship also enables learning from lived experience rather than abstract instruction, reinforcing the importance of real-world exposure, feedback loops, and relationship based development. It fosters humility in the coach and curiosity in the apprentice, setting the stage for deep trust and mutual growth. Apprenticeships elevate leadership development from sporadic training to an intentional journey of transformation.
Shared and Super-Leadership: Enabling Young Leaders:
Shared leadership refers to distributing leadership responsibilities across roles rather than concentrating them in a single position. When younger leaders are empowered to co-lead projects, they not only gain experience but also receive validation as future in-fluences. This approach builds confidence, fosters innovation, and enhances team collaboration. Super-leadership, defined by the ability to help others lead themselves, offers another powerful coaching mindset. Rather than creating dependents, leaders cultivate autonomy, encouraging apprentices to develop their own leadership identities and decision-making capabilities. Super leaders invest in unlocking the potential within others by fostering critical thinking, self-direction, and ownership. These frameworks challenge traditional hierarchical models, favoring instead a collaborative environment where every team member is seen as capable of contributing leadership value. By doing so, organizations not only enhance their leadership capabilities but also foster cultures of empowerment and resilience.
Designing a Coaching-Apprenticeship Program:
Building a coaching-apprenticeship program begins with intentional matching; coaches should be trained not only in their disciplines but also in delivering feedback and reflective questioning. Programs should incorporate a phased structure with clear goals per stage, shadowing opportunities, and assigned leadership responsibilities. Embedding reflection points, journaling, peer discussions, or coach debriefs, creates a feedback-rich environment that accelerates development and reinforces critical thinking. Designing such a program also entails aligning the apprenticeship with the organization’s strategy. What leadership behaviors and mindsets are most critical for your future? These should be embedded in coaching conversations, project assignments, and developmental goals. Regular check-ins, performance reviews, and cross-functional exposure can enhance the apprentice’s understanding of broader business operations. Moreover, integrating the program into HR and L&D systems ensures sustainability, scalability, and accountability.
Case Examples & Research Evidence:
Data from academic institutions and corporations demonstrate measurable improvements in leadership capability, confidence, and identity when coaching and apprenticeship programs are implemented in tandem. One study found that undergraduates who received leadership coaching outperformed their peers in self-evaluation, initiative-taking, and communication. Similarly, organizations that pair junior executives with seasoned leaders on real-world projects report greater succession readiness and improved cultural continuity. For instance, a healthcare system implemented a year-long leadership apprenticeship for high-potential clinical managers, resulting in a 25% increase in internal promotions and significantly reduced turnover. These examples underscore the power of experiential learning and the trust it fosters between generations. The most impactful programs are those that strike a balance between structure and flexibility, allowing apprentices to stretch while remaining supported. The case for apprenticeship is not just anecdotal; it is data-driven and results-proven.
Overcoming Challenges in Coaching Apprentices:
Leaders struggle to find time for coaching or mistakenly default to giving directives. An effective apprenticeship requires a shift in mindset: from command to inquiry, from short-term results to long-term development. Another challenge is the temptation to clone oneself—coaches must resist imposing their exact styles. Instead, they should encourage apprentices to explore and refine their voices, emphasizing authenticity and self-discovery over replication. Leaders must also learn to relinquish control, allowing apprentices to make mistakes, learn, and recover. For the apprentice, imposter syndrome and fear of failure can hinder growth, coaches must be adept at building psychological safety and modeling vulnerability. Lastly, organizational structures must support this effort; when performance metrics favor only short-term outcomes, coaching can be deprioritized. Addressing these challenges requires intention, effective communication, and a commitment across all leadership levels.
Measuring Success and Institutionalizing the Practice:
To sustain apprenticeship models, organizations must define clear metrics of success and integrate coaching into their leadership pipelines. Effective metrics include observable behavior changes, feedback from peers and supervisors, and progression into formal leadership roles. Making coaching part of job expectations, and distributing time in calendars and budgets, signals organizational commitment and reinforces its strategic value. Institutionalizing the practice also requires training and support for coaches. Not everyone is naturally equipped to coach; it must be seen as a skill to be developed. Recognition and reward systems can further encourage participation and excellence. Over time, the goal is to normalize coaching-as-apprenticeship as a cultural standard, not a temporary initiative. When embedded deeply, it becomes self-perpetuating: today’s apprentices become tomorrow’s coaches.
Action Plan – Six-Month Coaching Apprenticeship Template: Month Activity
1. Identify apprentice and coach pair; set mutual goals. Clarify expectations and agree on communication rhythm.
2. Shadowing senior leader in meetings, decision-making, and interpersonal scenarios. Focus on observation and questioning.
¾. Apprentice leads small initiatives or portions of projects under supervision. Provide real-time feedback and adjust tasks as needed.
5. Deep reflection session: discussing key learnings, identify growth areas, and recalibrate developmental objectives.
6. Final project debrief: summarize progress, co-create a personal leadership vision statement, and develop a transition roadmap.
This plan is not a rigid template but a guide for phased development. Each month’s focus allows for a gradual transition from observation to ownership. Coaches facilitate experiences while ensuring support and reflection. By the end of six months, apprentices should not only demonstrate enhanced skills but also articulate a personal leadership philosophy shaped by feedback and experience.
Conclusion:
Coaching young leaders through an apprenticeship approach creates multiplier effects, developing not only leadership skills but also leadership identity, confidence, and organizational continuity. This shifting paradigm, from managing tasks to growing people, challenges leaders to measure legacy by who they raise, not just what they achieve. Investing in apprenticeship coaching today helps ensure stronger, more adaptive organizations tomorrow. By embracing apprenticeship as a strategic imperative, leaders cultivate a lasting impact, one that extends far beyond their tenure and
shapes the trajectory of future generations.
More importantly, the coaching-as-apprenticeship model restores a human-centric ethos to leadership development. It recognizes the power of relationships, trust, and long-term investment in others. It transforms organizations into learning communities, where leaders are not only accountable for business outcomes but also for building capacity in others. The impact ripples outward, from individual apprentices to teams, departments, and entire institutions.
Every seasoned leader has the opportunity —and the responsibility —to create space for others to grow. Leadership, at its best, is not a destination but a legacy to be passed down. Moreover, that legacy is measured not only in profit margins and productivity metrics, but in the readiness, values, and courage of those who follow. Coaching future leaders as apprentices ensures that the mission and values we lead with today endure and evolve through those we mentor tomorrow.
Challenge question: As a leader, are you merely managing today’s results, or are you actively shaping tomorrow’s leaders through intentional apprenticeship?
Health care challenges have long stood in the way of Liberia’s national development. With limited access to quality medical services, many Liberians have found themselves traveling abroad or relying on prayer and hope in the face of serious illness.
But a new chapter is unfolding, one driven by local leadership, global standards, and a bold commitment to change.
Located along the Congo Town back road, WPMC delivers safe, customer-centered, world-class services, all provided by Liberian professionals. Its offerings range from advanced laboratory diagnostics to outpatient care and medical screenings for international visa applicants.
Metering system installation services.
WPMC’s practices are in line with national and international standards and are supported by technologies sourced from the U.S., Europe, and Asia. From the outset, the center has been designed to restore trust in Liberia’s medical system.
The official launch ceremony brought together distinguished guests, including former President Ellen Johnson Sirleaf, health sector leaders, staff, and the general public. The event not only marked a major milestone in health care delivery but also celebrated the vision and leadership that made it possible.
At the heart of WPMC is Dr. Nicole Cooper, the facility’s Medical Director. A passionate health leader, who shared the journey that led to the creation of the center.
“I’ve seen too many people praying outside hospital rooms, hoping that everything aligns just to save a life,” she said. “Too many are forced to leave the country for basic health care because they don’t trust that it can be done here.”
That reality, Dr. Cooper explained, planted a seed back in 2009, the early inspiration behind what would eventually become Wellness Partners. In 2021, she returned to Liberia with the goal of building a system that met international standards but remained accessible and reliable for all Liberians.
She began with Wellness Partners Clinic, a small pilot that tested health care delivery models, affordability, and customer care strategies. From those humble beginnings, the initiative expanded into the full-fledged Wellness Partners Medical Center.
“We’re different,” she said. “We invest in our people, prioritize quality and safety, and put transparency at the center of what we do.”
“Our vision is bold yet simple: to become the safest, most reliable, and most convenient network of medical care in Africa,” she told attendees. “This is what’s possible when we believe in ourselves and build from the inside out.”
Representing the WPMC Board of Directors, Mrs. Monique Cooper Liverpool echoed that sentiment, calling the center “a homegrown solution led by Liberian talent with world-class expertise.”
Also speaking at the event was Mrs. Sophie Parwon, CEO of Benson Hospital, who highlighted the growing contribution of the private sector in Liberia’s health care ecosystem.
“While the government remains the main provider of health services, the private sector is increasingly stepping up, contributing to service delivery, financing, innovation, and capacity building,” she said.
Mrs. Parwon praised Dr. Cooper as a “public health icon” and called on government and development partners to strengthen support for private health initiatives that align with national priorities.
As WPMC opens its doors, it does more than offer medical services. It offers hope, hope for a health care system where Liberians no longer need to look abroad for basic care, where dignity and quality go hand in hand, and where innovation is driven from within.
Objective To assess the feasibility and clinical utility of daytime polysomnography (PSG) in infants ❤ months of age.
Methods A prospective observational study of a convenience cohort analysing PSGs that were conducted for clinical purposes in infants less ❤ months of age, between 1 May 2021 and 31 May 2024. A comparison was made between results for daytime PSG in the neonatal intensive care unit (NICU) and overnight PSG in the sleep laboratory. The type of PSG performed (daytime vs overnight) was based on the workflow of the sleep laboratory. Primary outcomes were successfully completed PSGs (feasibility) and per cent sleep efficiency (clinical utility). Secondary outcomes compared other sleep parameters between groups. Patient and public feedback directly informed the development of the research question and outcome measures.
Results Of 60 PSGs, 28 were daytime and 32 were overnight. Daytime studies had a younger age (median 18 vs 55 days, p<0.001) and shorter median recording time (8.2 vs 10.4 hours, p<0.001). All daytime PSGs were successful, indicating feasibility. After adjusting for age at PSG and total recording time, per cent sleep efficiency was equivalent in the two groups (95% CI −12.4 to 5.7; p 0.456), indicating their clinical utility. For secondary outcomes, daytime PSGs had a higher % rapid eye movement (REM) sleep by 9.9% points (95% CI 1.1 to 18.8; p 0.028) compared with overnight PSG. Parameters that were not different included: frequency of spontaneous arousals, REM latency, sleep latency, Apnoea-Hypopnoea Index and Obstructive Apnoea-Hypopnoea Index. A decline in requests for overnight PSGs and a corresponding increase in daytime PSGs over the course of the study were observed.
Conclusion Daytime PSGs performed in NICU were feasible and provided clinically useful results in infants ❤ months of age. Availability of daytime PSGs performed at the infant’s bedside expands resource capacity and has the potential for cost savings.
With support from the World Health Organization (WHO), the National Public Health Institute of Liberia (NPHIL) and the Ministry of Health concluded a residential hands-on in-country training on genomic sequencing and bioinformatics at the National Public Health Reference Laboratory (NPHRL) from 29 September to 19 October 2024 in Margibi County. Facilitated by a team of experts from the Noguchi Memorial Institute for Medical Research in Ghana, a total of 10 national laboratory technicians received a 2-week intensive training followed by a 1-week practice session.
Genomic surveillance plays a critical role in tracking emerging pathogen variants. It has become a fundamental global public health tool for detecting, monitoring, and responding to infectious disease outbreaks, as demonstrated by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic. During the in-country training, national laboratory scientists analyzed additional mpox-positive samples and detected another mpox strain, clade IIb.
“Before the training, we were reliant on international laboratories to identify the circulating pathogen strains. Now, we have the capability to conduct sequencing and bioinformatics analysis in-country, enabling us to rapidly identify emerging pathogens and their geographic origins,” Francis Omega Somah, laboratory technologist at the National Reference Laboratory in Liberia.
This training is a significant milestone in the integration of pathogen genomics and bioinformatics into public health surveillance, outbreak detection, and investigation, which will enhance disease control and prevention efforts in Liberia. “This is a game-changer for the country as we will now have the national capacity to sequence and characterize pathogens of epidemic prone diseases in our country. We thank WHO for this strategic investment and their continuous technical and financial support towards strengthening Liberia’s capacity to detect and manage epidemics,” said Dr Dougbeh Nyan, Director General of NPHIL.
In 2022, WHO published a global genomic surveillance strategy to support countries in expanding their capacities. Unfortunately, 50% of Member States, including Liberia, lacked domestic sequencing capacity. To address this gap, WHO, under the AFRO HERA project, is supporting six African nations: Liberia, Burundi, the Central African Republic, Comoros, Eritrea, and Togo to establish and strengthen genomic sequencing and bioinformatics capacity, thereby expanding detection and genomic surveillance of epidemic-prone priority pathogens across the African Region. WHO has significantly invested on the continent in infectious disease and genomics surveillance.
“The most important aspect of capacity building is training the right experts. When a country has skilled professionals with the right platform, expertise, and infrastructure, they can respond swiftly and effectively to public health emergencies,” said Dr. Coulibaly Sheik, WHO AFRO Lead Diagnostic and Laboratory Services Unit.
Dr. Peter Clement, WHO Country Representative, thanked the team of facilitators and WHO AFRO for supporting Liberia through the EU-funded project which will strengthen the country’s laboratory systems. “By empowering local experts with the skills to conduct genomic sequencing and bioinformatics analysis, we are ensuring that Liberia is better prepared to rapidly identify emerging threats and implement timely interventions,” said Dr. Peter Clement, WHO Liberia Representative.
The Healing Power of Comfort Pets in Children’s Hospitals
In the high-stakes environment of a children’s hospital, every source of comfort matters. Beyond the dedicated medical staff and cutting-edge technology, one often overlooked hero is the comfort or service pet. These animals, specially trained to provide emotional support, offer more than companionship—they bring a sense of calm, joy, and connection during some of the most challenging times in a young patient’s life.
For pediatric patients, comfort pets can help reduce anxiety, ease feelings of isolation, and even promote healing. A gentle nuzzle or playful paw can break through the walls of fear that sometimes build during hospital stays. Studies have shown that interaction with therapy animals can lower stress hormones, improve mood, and provide a sense of routine and normalcy for children who are often navigating complex medical treatments. In the neonatal context, while the infants themselves may not directly interact with pets, families of NICU babies experience the calming presence of therapy animals, helping them manage stress, fear, and the emotional weight of having a critically ill newborn.
Families may benefit greatly from the presence of comfort pets. Parents and siblings frequently carry their own anxieties as they support a hospitalized child. In the NICU, where the emotional toll is heightened by uncertainty and intensive care routines, therapy animals offer brief but meaningful moments of relief, allowing families to smile, laugh, and connect. These moments can strengthen the parent-child bond, provide emotional grounding, and even support parents’ ability to be present and engaged in their baby’s care.
Healthcare workers often report the positive impact of comfort pets. Long shifts, high emotional demands, and the intensity of neonatal and pediatric critical care can take a toll on staff well-being. Therapy animals provide a moment of grounding and a reminder of the simple joys in life, helping to reduce burnout and improve morale.
In NICUs and pediatric wards alike, the presence of a comfort pet is a win-win: patients receive care enriched by joy, families feel supported, and staff experience a boost in their own emotional resilience.
Our very own Bennie Boo (hypoallergenic, gentle, and loving) may be a perfect candidate for comfort care training in his future. This is a pathway we may consider next year when he turns two.
Anthony gets a lesson from Liberia’s first ever surfer, Alfred Lomax. He doesn’t catch a wave, but locals manage to catch more than enough fish for a fresh seafood feast, served with a beer, of course!
There are three tiers of healthcare in the country:
Subsidized regime, which is financed by the government for unemployed, poor, disabled and indigent people.
Contributive regime, which is financed by workers and employers
Contributive subsidized regime, which is financed by independent workers, technical workers, and self-employed people, but subsidized by the state[16]
Even those for whom care is supposedly provided may have to pay for medical supplies. However, considerable progress in health and overall development was experienced in the country. For instance, there is a substantial increase in health coverage in the nation that is the health insurance coverage from 23% in 2011 to 65% in 2015 (Centers for Disease Control and Prevention n.p). Significantly, updating the list of beneficiaries was the major challenge since the list based on disease prioritization and financial sustainability. Therefore, the first fitness elements, such as migration, poverty education, and gender-based, should be considered in the strategy of hindrance suites.
Government expenditure on healthcare is about $180 per person per year, slightly more than half the average for the Latin American and Caribbean region.
Essentially, there are steps considered by healthcare in the Republic. Firstly, the sponsored organization that caters to the poor, unemployed, and disabled people. Also, the active personnel contained a contributive establishment. Though the low-classes are dependents, the majority of the population is independent on matters of health, according to the Dominican Republic (World Health Organization n.p). Therefore, government expenditure per person is slightly higher in the Dominican Republic compared to other states.
European Standards of Care for Newborn Health/CALL TO ACTION
Europe needs new ideas and solutions to address the disparities in the care of preterm and ill babies. The European Standards of Care for Newborn Health project presents such a solution by providing European reference standards for this health care area.
With its transdisciplinary focus and international composition of the working groups, the project sets new benchmarks for the care of preterm and newborn babies and can serve as a role model for countries in Europe and worldwide. About 220 experts from more than 30 countries accepted to dedicate their free time to work on this ambitious project over several years. At the time of the launch of the standards, 108 healthcare societies and associations as well as 50 parent organisations have accepted EFCNI’s invitation to officially support the newly developed standards.
Through its multi-stakeholder approach, the perspective of parents, healthcare professionals, and relevant third parties were equally considered, aiming at identifying current best practice. Industry partners were involved in the project by supporting it financially. Their representatives could join the Chair Committee meetings in an observing role and they were welcome to share their knowledge and expertise without exerting influence. Initiated by patient (parent) representatives for patients, it is a true patient-centred project and, for the first time, patients were involved in absolutely every step in the development of the standards. All project participants work together in an open and respectful partnership to pave the way for change and set newborn health on the international and national agendas.
On a political level, addressing European Standards of Care for Newborn Health will stimulate a new debate that can help questioning existing structures, identify gaps and deficiencies, and advance national healthcare systems. To read the standards and to learn more about their development, please visit our project website European Standards of Care for Newborn Health.
On the project website, you also find further information like a project report, an information brochure or social media graphics.
The European Standards of Care for Newborn Health now available in Italian – Gli Standard Assistenziali Europei per la Salute del Neonato sono disponibili in italiano
The Italian Society of Neonatology (SIN) and Vivere ONLUS, the Italian National Coordination of Parents’ Associations, took the initiative to translate the standards into Italian, with Italy becoming the first European country to make this important document available in their national language. The first two sets of standards can be downloaded from our project page.
Call to Action for Newborn Health in Europe
The UN Convention on the Rights of the Child has been ratified by 196 countries and proclaims that “the child, by reason of his physical and mental immaturity, needs special safeguards and care, including appropriate legal protection, before as well as after birth”. Article 6 affirms every child has the right to life, survival, and development. Furthermore, children have a right to be cared for by their parents and should not be separated from them, as far as possible (Articles 7 and 9). However, upholding the Rights of the Child in reality remains a major challenge.
The European Standards of Care for Newborn Health help support these rights from the beginning of life by serving as a reference for the development and implementation of binding standards and guidelines on a national and international level. European and national policy makers, hospital administrators, insurers, professional and patient associations, and industry should work together to bring the standards into practice and to ensure quality, equity, and dignity for the smallest.
Download the Call to Action Brochures: The Call to Action is available in about 20 languages and can be downloaded here.
March of Dimes Named 2025 Labor Partner Charity of Choice for United Food and Commercial Workers International Union
ARLINGTON, Va., March 18, 2025 /PRNewswire/ — March of Dimes, the leading organization committed to improving the health of moms and babies, has been named the United Food and Commercial Workers International Union’s (UFCW) Labor Partner Charity of Choice for 2025. As UFCW’s designated national charity partner, March of Dimes and UFCW will work together to support and advocate for healthy pregnancies, strong families, and improved maternal and infant health outcomes in the US.
“For more than 85 years, March of Dimes has stood alongside labor unions to champion the health and well-being of working families,” said Cindy Rahman, President and CEO of March of Dimes. “Our partnership with UFCW builds on this proud legacy, strengthening our ability to advocate for policies, provide essential resources, and drive meaningful change to improve maternal and infant health outcomes. We will work together to ensure that every family—no matter where they live or work—has access to the care and support they need for a strong, healthy start.”
The US remains the most dangerous high-income nation for childbirth, earning a D+ for a third consecutive year in March of Dimes’ latest Report Card, which measures the state of maternal and infant health in the US. Through this partnership, UFCW and its more than 1.2 million members will have opportunities to engage in fundraising efforts, volunteer initiatives, and awareness campaigns aimed at addressing this growing crisis.
“The UFCW Charity Foundation is committed to supporting organizations that make a real difference in the lives of working families,” said UFCW International President Marc Perrone. “March of Dimes has led the fight to improve maternal and infant health for decades, and we are proud to stand with them in this important work. By joining forces, we have the opportunity to help even more families access the care and resources they need for healthy pregnancies and strong futures.”
Partnering with labor unions to protect the health of working families is a cornerstone of March of Dimes’ mission. We’re honored to have strong and long-standing national and local partners like UFCW through our Labor of Love movement, which raises critical funds to pioneer research, advocate for change, and pave the way for greater equity to give all families the best possible start.
Before being named UFCW’s Charity of Choice, UFCW members have actively supported March of Dimes, raising over $3 million through golf outings, sporting clay events, auctions, and March for Babies teams. They have also uplifted the voices of their own members, like Daniel Scott of UFCW Local 1996, whose twins spent time in the neonatal intensive care unit (NICU) after a challenging pregnancy. For families like the Scotts, March of Dimes’ work is more than a cause—it’s a lifeline, ensuring that babies born too soon or facing complications receive the critical care they need.
About March of Dimes March of Dimes leads the fight for the health of all moms and babies. We support research, education, and advocacy, and provide programs and services so that every family can get the best possible start. Since 1938, we’ve built a successful legacy to support every pregnant person and every family. Visit marchofdimes.org or nacersano.org for more information. Follow us on social at @marchofdimes. SOURCE March of Dimes Inc.
Premature birth has consequences across the course of life, including reduced life-expectancy, and the most prematurely born have the worst outcomes [1, 2]. Survivors of prematurity have increased respiratory morbidity and mortality, airflow obstruction, asthma-like symptoms and COPD, and cardiovascular disease [1–4]. A history of prematurity is often not sought in adult clinics [5]. We hypothesised that the long-term consequences of prematurity are insufficiently appreciated, likely with detriment to patient care.
We used an online survey developed by a panel of neonatologists, paediatricians, allergologists and pulmonologists. The survey included 21 items addressing four main topics: 1) awareness level among respiratory care providers regarding the long-term respiratory risks of premature birth; 2) communication of neonatal information between different medical specialties; 3) healthcare journey of preterm babies to paediatricians and other respiratory care providers; 4) the knowledge gaps and potential solutions. The survey was customised to each specialty: seven items were for neonatologists only; three for paediatricians; one each for allergologists and respiratory consultants; five for paediatricians, allergologists, and respiratory consultants; and four for all specialties.
We invited 14 651 neonatologists, paediatricians, allergologists and respiratory consultants from Australia, France, Germany, Italy, Spain, the UK, and the USA to participate, excluding physicians with less than 2 years’ experience; 1002 (7%) responded. A web link was emailed from listings extracted from Chiesi Farmaceutici S.p.A and from proprietary databases of external healthcare providers. All had previously consented to email contact. Two email reminders were sent and incomplete surveys were rejected.
Sample size was opportunistic in the absence of data enabling a power calculation. The survey results were analysed using Microsoft Excel and Microsoft Power BI. All items involved categorical answers, and absolute and relative frequencies were calculated. All frequencies were treated descriptively. No geographical comparisons were performed due to sample size limitations. The questionnaire is available on request from the corresponding author.
Results are summarised in figure 1. Of the 1002 respondents, 91% had been in practice for more than 5 years, and 62% were practising in an outpatient facility. In terms of specialities, 282 (28%) were neonatologists, 183 (18%) paediatricians, 290 (30%) allergologists, and 247 (24%) were respiratory consultants. Figure 1a shows that neonatologists regarded the presence of respiratory symptoms as being most important in the decision to refer. By contrast, for paediatricians, birth weight was the most important factor, irrespective of respiratory symptoms (figure 1b). All specialists highlighted that the most important gap was lack of clear recommendations for follow-up (figure 1c) and the need for continuing medical education programmes (figure 1d). Most (96%) respondents considered prematurity and bronchopulmonary dysplasia (BPD) risk factors for lung diseases in adulthood. Nevertheless, 74% of respondents perceived only moderate to very low awareness among colleagues. Adult pulmonologists perceived the lowest level (85%) of awareness among the specialties surveyed.
FIGURE 1
Reasons for neonatologists (a) and paediatricians (b) to refer preterm-born patients to a respiratory specialist. The gaps and potential solutions to improve the long-term respiratory care of preterm-born individuals are shown in (c) and (d). The bars show the percentage of participants who selected each option. NICU: neonatal intensive care unit; BPD: bronchopulmonary dysplasia.
Most (77%) paediatricians “always” took a perinatal history, compared with allergologists (34%) and pulmonologists (21%). Irrespective of specialty, the proportion who always took this history increased with increasing years of clinical experience. Most (95%) neonatologists shared information on gestational age, birth weight, need for supplemental oxygen and respiratory support, BPD diagnosis and other lung sequelae of prematurity (>80%), and this was consistently reviewed by paediatricians (83%). This information was mainly through medical records (57%) and by oral communication (52%). Allergologists and respiratory consultants used feedback from other physicians (58% and 37%, respectively) and electronic medical records (43% and 26%, respectively) to gather neonatal information. They reviewed less neonatal information, although BPD diagnosis and lung sequelae were reviewed by 72% and 65% of allergologists and respiratory consultants, respectively.
Most neonatologists (99%) shared information with parents and caregivers, and more than 70% of paediatricians and allergologists received information from the caregivers. Only 59% of adult pulmonologists acknowledged receiving information from parents and caregivers.
Most neonatologists (70%) followed up preterm babies for two years, but 27% for only 1–2 years. Most (>75%) of all those surveyed, believed that premature babies should be followed up lifelong.
Most (>80%) allergologists modified clinical management, at least partially, if they were aware that the patient was born preterm. Only 60% of adult pulmonologists adapted management pathways in preterm survivors.
Most (>60%) respondents considered that preterm-born individuals and their parents and caregivers should be empowered to ensure they receive the best respiratory care. Other suggested initiatives were measuring lung function during follow-up from 5 years of age, streamlining access to the perinatal medical history and the development of a portable record with neonatal information. Going forward, the use of a lifelong electronic patient record, accessible to all who are involved in patient care, would likely greatly facilitate communication between specialist groups.
In summary, there is inadequate awareness of the importance of preterm birth for management across the life course; communication between specialist teams is inadequate; and there is lack of clear guidance as to how to follow-up preterm born survivors.
The European Respiratory Society [6], and the American Thoracic Society [7] have published guidelines with conditional recommendations on low strength evidence. However, the former only covered the follow-up of BPD survivors [6], and the latter were limited to the follow-up of preterm-born children and adolescents with respiratory symptoms [7]. These guidelines are limited, not least because we now know that the risk of compromised lung health later in adulthood exists even for early term born infants [4, 8, 9]. However very few paediatricians actually referred extremely preterm or low birth weight babies to a respiratory specialist. An international consensus on how to structure respiratory follow-up remains an unmet need [1, 10].
Most allergologists (80%) and adult pulmonologists (60%) modified diagnostic pathways and treatment approaches, at least partly, when they were aware the patient was born premature. Lack of appreciation of the implications of prematurity across the life course may lead to wrong treatment being prescribed. For example, school-age wheeze and variable airflow obstruction is common in preterm survivors [11]. Some may respond to treatment with inhaled corticosteroids (ICS) [12] but in others there is no evidence of type 2 inflammation so they should not be treated with ICS [13]. They may have dysanaptic airway growth [14], which is known to be associated with poor outcomes in term-born children [15]. More work is needed to determine disease pathology in preterm survivors and to stimulate new research. Trials to stimulate lung development at birth and control airway inflammation in extremely premature babies are underway with stem cell-based therapies, insulin-like growth factor 1 and intratracheal surfactant/budesonide.
Proposed mitigation strategies to improve the current situation include better continuing medical education. Another is empowering patients and caregivers by supplying accurate information which they can ensure is available to subsequent caregivers, including during transition to adult services.
The main strength of the survey is that it includes >1000 physicians from different specialties and countries. There are some limitations. The overall response rate was relatively low, although similar to the British Thoracic Society survey [5], and there is a risk of selection bias. General practitioners were not invited, and this was a mistake given their role in follow-up care.
In conclusion, we need to increase awareness of the long-term implications of prematurity to ensure optimal follow-up for these babies, and design studies to obtain an evidence base for the development of improved guidelines.
Houda M. Abdelrahman; Suzanne M. Jenkins; Michael P. Feloney.
Last Update: November 12, 2023.
When the hymen, a thin membrane of stratified squamous epithelium circumscribing the vaginal introitus, does not spontaneously rupture during neonatal development, it is referred to as an imperforate hymen. An imperforate hymen is a rare cause of primary amenorrhea and can present with obstructive symptoms of the female genital and urinary tracts during the perinatal, pediatric, or adolescent years. Timely diagnosis and prompt treatment are critical. Specific pediatric and gynecologic knowledge and skills are necessary to provide comprehensive, patient-centered care. In addition to the anatomical and physiological aspects of imperforate hymen, its clinical presentation, and potential complications, the psychological impact on affected individuals must be understood. Best practices will ultimately improve patients’ quality of life and reproductive health outcomes. This activity reviews the evaluation and treatment of imperforate hymen and highlights the role of the interprofessional team in improving care for patients with this condition.
Spilling the Tea is an educational series for new preemie moms and dads brought to you by TEACUP Preemie Program®. These brief but in-depth videos will explore aspects of prematurity including emotional and mental effects, the NICU environment, breastfeeding & pumping, reclaiming attachment & bonding, and others. Preemie parents share their experiences through intimate video journals, and experts in infant development and prematurity offer guidance and information. Episode 3: Dads in the NICU, takes you through the emotional rollercoaster experienced by Beau, Chris, and Steve, three preemie dads who have been there. Get ready to be moved and inspired by their stories of resilience, love, and the extraordinary bond they formed with their little miracles.
Mitigating the iatrogenic psychological effects of medical care in the Neonatal Intensive Care Unit (NICU) and beyond is a moral and ethical imperative for quality healthcare delivery. Research has long established the lifelong effects of early childhood adversity, toxic stress, and the critical role of pediatric clinicians in addressing these challenges, and most recently, the American Academy of Pediatrics (AAP) published a clinical report and policy recommendations for the adoption of a trauma-informed paradigm across all child health services. Provenzi and Montirosso confirm that preterm birth is an early adverse experience characterized by exposure to toxic stress and reduced access to the buffering effects of maternal care. Understanding the concepts of infant medical stress and its association with alterations in brain growth and development highlights the biological relevance of a trauma-informed developmental approach to care in the NICU and beyond.
Early life adversity, often mediated through relationships with caregivers, is associated with attachment disturbances, posttraumatic stress disorder (PTSD), and developmental trauma disorder (DTD) in survivors . Experiences of maternal separation and cumulative toxic stress within the NICU have profound implications for infants, families, and the healthcare team . Adversity during infancy is associated with significantly poorer health outcomes, risky health behaviors, and socioeconomic challenges . Parents, too, experience significant emotional and psychological distress, which can persist for decades, further reinforcing the need for trauma-informed approaches to care).
During sensitive and critical periods of development, the experiences associated with critical illness and hospitalization take on new meaning as they direct and disrupt biological processes in the wake of toxic stress. These biological processes, mediated by epigenetic mechanisms, have lifelong implications for an individual’s physiologic and psychological health and wellbeing . Maternal separation is the most significant trauma experienced by all newborn mammals, and preterm and critically ill newborns are no exception . Separation of mother and infant at just two days of age for 1 hour has been linked to a 176% increase in autonomic reactivity and an 86% reduction in quiet sleep . The experience of maternal separation in the NICU becomes the foundation for cumulative toxic stress exposures, ranging from inappropriate sensory stimuli to hazardous hospital routines that do not honor the personhood of the infant. These early stressors compound, leading to long-term health and developmental challenges.
Separation also has profound implications on the parent, leading to depression, anxiety, feelings of helplessness, loss of control, and posttraumatic stress, which may last for decades. These feelings can impact parenting behaviors and the capacity to partner with clinicians in caring for their infant. Understanding the interplay of physical and emotional health, economic and social resources, medical systems, and structural inequities is critical for co-creating compassionate, collaborative, and supportive relationships with infants, families, and clinicians in the NICU.
Trauma-Informed Care:
A trauma-informed approach realizes the pervasiveness of trauma in everyday life, recognizes its signs and symptoms in patients, families, colleagues, and self, and responds to trauma by integrating knowledge and evidence-based best practices that mitigate and prevent trauma into policies, procedures, and language; and resists re-traumatization by ensuring consistency and compassion in service delivery. The core principles of trauma-informed care—safety, trust and transparency, healthy relationships and interactions, empowerment, voice and choice, equity, anti-bias efforts, and cultural/gender affirmation—guide all interactions in the NICU.
Parenting is central to a trauma-informed approach, as caregivers play a fundamental role in mitigating the stress and trauma of early hospitalization. The research underscores the powerful buffering effect of parental presence, engagement, and nurturing care in reducing toxic stress responses and promoting infant resilience . When parents feel supported and empowered in their caregiving role, they experience lower stress levels, increased confidence, and enhanced bonding with their infant. This benefits the family’s emotional well-being during the NICU stay and has lasting implications for child development and attachment security.
The short-term outcomes of a trauma-informed parenting approach include improved neurodevelopmental stability, reduced incidences of apnea and bradycardia, and better weight gain trajectories for preterm infants. Additionally, trauma-informed care has been linked to greater autonomic stability, reduced stress hormone levels, and improved sleep patterns, all contributing to enhanced physiological regulation and early developmental progress . These immediate benefits lay the groundwork for stronger immune function and better feeding outcomes, helping infants build the resilience needed for longterm health and well-being . Parents who are actively involved in their infant’s care through practices such as skin-to-skin contact and responsive caregiving exhibit lower levels of anxiety and depression, leading to a healthier emotional environment for both the child and the family unit .
Long-term, trauma-informed parenting interventions significantly impact developmental trajectories, reducing the risk of cognitive delays, emotional dysregulation, and behavioral challenges in childhood . Secure attachment formed during these early interventions fosters resilience, social-emotional well-being, and stronger parent-child relationships well into adolescence and adulthood. Studies have also linked early trauma-informed care to improved educational outcomes and a reduced risk of mental health disorders later in life .
Providing parents with the knowledge, tools, and emotional support necessary to engage confidently in trauma-informed caregiving is critical in shaping the health and well-being of NICU graduates . By prioritizing the parent-infant dyad and leveraging evidence-based interventions, trauma-informed care offers a transformative model that extends far beyond the NICU walls, laying the foundation for lifelong resilience and well-being. When parents are given the resources to understand their infant’s cues, respond sensitively, and participate actively in care, they develop a sense of mastery and confidence that translates into more substantial, more secure attachments. This engagement benefits the infant’s immediate well-being and fosters a more compassionate, informed approach to parenting that can positively influence future generations.
Clinical Application of Trauma Informed Care:
Parent-driven interventions in the NICU center include parents as active participants in their baby’s care, fostering attachment and reducing trauma. One such intervention is The Zaky HUG®, a therapeutic device designed to extend the parent’s presence by mimicking their hands’ touch, warmth, and scent (Fig. 1). Created by a Ph.D. engineer and former NICU and kangaroo mother, this tool emerged from a deeply personal experience of neonatal hospitalization and has since been developed to support sleep, neuroprotection, attachment, developmental care, pain management, and parental involvement. This device helps create a comfortable, warm, and predictable environment, allowing infants to rest and sleep more peacefully. It is designed to provide the benefits of multiple tools, including positioning, nesting, soothing, and attachment.
Initially motivated by the need to provide connection, continuous comfort, and reduce the association of touch with pain and her own infant’s stress, the creator of this hand-mimetic device applied principles of ergonomics and safety engineering to design a device that fosters secure attachment, supports positioning, predictable experience for the infant, family, and clinicians.
Protected sleep is critical for neurodevelopment and overall well-being. Sleep is a primary driver of brain maturation, memory consolidation, and emotional regulation in preterm and critically ill infants. Interruptions to sleep can disrupt these critical processes, leading to increased stress responses, metabolic instability, and impaired neurodevelopmental outcomes. Ensuring a supportive sleep environment requires balancing between providing necessary medical interventions and minimizing disruptions to natural sleep cycles. Frequent repositioning, environmental disruptions, and inconsistent containment can negatively impact an infant’s sleep-wake cycles. Research by Russell et al. has shown that because these nurturing devices are versatile and work for positioning, nesting, attachment, soothing, and sleep support, they reduce the need for frequent repositioning, offering a stable, soothing environment that promotes restful sleep both during kangaroo care and while in the incubator or crib. These devices help infants transition between sleep states more smoothly, reducing startle reflexes and excessive wakefulness by providing gentle, consistent containment and proprioceptive support.
Additionally, they assist in creating a cocoon-like space that mimics the security of the womb, further enhancing sleep continuity and quality. Further, consensus guidelines advocate for supporting parents in providing frequent, safe, and prolonged skin-to-skin care, reinforcing the role of these interventions in achieving sleep protection . Research has also highlighted that skin-toskin contact improves sleep patterns, stabilizes respiratory rates, and reduces cortisol levels, mitigating the physiological impacts of stress. When infants experience uninterrupted, restorative sleep, they exhibit improved feeding behaviors, enhanced weight gain, and greater autonomic stability, all crucial for their long-term development.
The Pain and Stress Prevention and Management measure prioritizes proactive pain mitigation strategies. By minimizing stress and discomfort, infants can better participate in essential activities of daily living, such as feeding and movement, which further support their growth and development. The integration of non-pharmacologic interventions such as kangaroo care, proprioceptive input, and containment through trauma-informed devices significantly enhances an infant’s ability to self-regulate and cope with stress . Parents play a vital role in this process, providing direct comfort before, during, and after procedures. Studies show that utilizing familiar, comforting sensory stimuli, such as parental scent-infused devices, can effectively minimize procedural stress and discomfort, reinforcing the protective role of parental presence in the NICU.
Activities of Daily Living, including posture, nourishment, and hygiene, are essential to infant development. Establishing predictable and supportive care routines in these areas helps to create a sense of security and stability for infants, reducing stress and promoting optimal development. Ensuring infants receive proper postural support can facilitate musculoskeletal alignment, improve digestion, and reduce discomfort caused by medical interventions. Additionally, consistent caregiving routines help infants develop circadian rhythms, supporting sleep-wake cycles and overall well-being. Kangaroo care safety devices support proper postural alignment, promoting successful breastfeeding and early oral feeding behaviors. One pair of hand mimetic devices further enhances postural stability, allowing for individualized positioning without restricting movement, facilitating optimal comfort and developmental support. These devices can also provide gentle containment, mimicking the boundaries of the womb, which is particularly beneficial for preterm infants adapting to extrauterine life. Furthermore, integrating nurturing devices in caregiving practices encourages parental involvement in routine care activities, reinforcing their role and confidence in caring for their baby even in a high-tech NICU environment.
Finally, Compassionate Collaborative Relationships focus on emotional well-being, self-efficacy, and communication. Clinicians play a vital role in supporting these trauma-informed measures, ensuring that both parents and staff are equipped with the knowledge and tools to facilitate optimal trauma-informed developmental care. These trauma-informed interventions support neurodevelopment and empower parents, reinforcing their role as primary caregivers. By enabling continuous sensory presence and minimizing separation, these devices help establish a sense of predictability, safety, and emotional security for infants and their families. The research underscores the long-term benefits of these interventions, showing reductions in parental stress and anxiety while fostering stronger attachment and advocacy skills.
By integrating trauma-informed devices and caregiving practices, neonatal teams can transform the NICU experience, bridging the gap between medical excellence and human connection. As neonatal care continues to evolve, integrating trauma-informed interventions into everyday practice is not just beneficial—it is imperative for fostering lifelong resilience in the most vulnerable patients. Prioritizing the five core measures for trauma-informed developmental care ensures that every infant and family receives care that is not only evidence-based but also deeply compassionate and developmentally appropriate.
Summary: Recognizing the trauma experienced by babies and families in the NICU is the first step toward transforming and humanizing neonatal care. This recognition must be followed by meaningful action—integrating trauma-informed practices, supporting parental involvement, and embracing innovative, evidence-based products and solutions that prioritize the holistic well-being of infants and their families. Trauma-informed interventions, particularly those that integrate parental involvement and ergonomic design, provide a compassionate, evidence-based approach to mitigating the effects of early life adversity. By centering the voices of parents and clinicians while utilizing trauma-informed tools designed to enhance neurodevelopment and emotional security, we can reshape the NICU experience and the transition to home after discharge into one that fosters healing rather than deepens distress. By leveraging these nurturing strategies, clinicians can enhance infant and family well-being, improve healthcare outcomes and satisfaction, reduce the cost of care, and foster a culture of healing and resilience in the NICU.
This shift requires dedication from institutions, practitioners, and advocates who believe in the profound impact of early experiences. Investing in trauma-informed developmental care is not just a clinical imperative—it is a moral and ethical responsibility that holds the power to transform lives. The NICU should not only be a place of survival but also one of healing, connection, and love. Every baby, every family, and every clinician deserves an environment that nurtures the body and the soul, where science and compassion intersect to create the best possible start for our most vulnerable patients. Through thoughtful, evidence-based approaches, we can transform neonatal care into a support, compassion, and empowerment model for every infant and family. Now is the time to act—to advocate, to innovate, and to implement trauma-informed care that acknowledges the human experience behind every NICU admission. The smallest among us deserve the best care, and it is our collective responsibility to ensure that their earliest moments are filled with safety, love, and hope.
The birth of a premature infant has a profound effect on the family and may require a large portion of parental time, attention, finances, and psychological support. During all this time, the sibling may feel confused and left out of the loop and may resent the amount of time the parents are away with the new infant in the NICU. If the preemie is found to have a disability, these issues are compounded as the parents may be grieving and require further time away to attend several appointments. In this session, Dr. Saigal will discuss strategies to support siblings of premature babies. Dr. Saroj Saigal is a neonatologist and a Professor Emerita at McMaster University, Canada. She is internationally recognized for her long-term studies to adulthood which focuses on the quality of life and consequences of having been born extremely prematurely. She has also participated as a collaborator in several multi-center randomized perinatal clinical trials. Dr. Saigal co-founded Adult Born Preterm International Collaboration (APIC) and invited collaborators from around the world who were doing studies on premature infants in adulthood to participate in data sharing. She is the recipient of many awards from the Canadian Pediatric Society and the American Academy of Pediatrics. She was awarded the 2018 Virginia Apgar Award of the American Pediatric Society for distinguished contributions to perinatal medicine. She was also recognized by her alma mater with the McMaster Faculty of Health Sciences Community of Distinction Award, 2018.
HEALTHCARE PARTNERS
What if a single event could sway health, exercise capacity, learning style, social interactions, and even personal identities–yet individuals had no memory of the event? Adults born preterm are an under-recognized and vulnerable population. Multiple studies of individuals born prematurely, including our 35-year longitudinal study, have found important health concerns that adult healthcare providers should consider in their assessments. Concerns include increased rates of cardiovascular disease, metabolic syndrome, depression, anxiety and attention problems, lower educational attainment and frequency of romantic relationships. A Nordic study of over six million individuals found a linear relationship between gestational age and protection against early adult mortality, with preterm individuals showing 1⋅4 times increased likelihood of early mortality as full-term peers.
At the same time, surviving premature birth has become increasingly common. For the last several decades, nearly one in nine U.S. babies is born early, and now more than 95% survive. Global prevalence and survival data indicate more than 15 million preterm birth survivors annually reach adulthood. This suggests a new population of individuals with emerging healthcare needs for adult health providers.
Birth history should be part of every patients’ medical record.5 Due to the varied risks and prevalence of premature birth, all healthcare practitioners should be aware of the potential for long-term effects. With one in ten 30-year-old patients born preterm, clinical specialists who treat long-term complications of prematurity (i.e., neurology, psychiatry, cardiology) may have more preterm-born patients. Recognizing preterm birth as a cumulative, lifelong risk factor is the first step.
As clinicians and researchers, we have observed the medical community, like society at-large, tends to view prematurity as a health event localized to infancy-something kids outgrow. Ironically, some pediatric providers report limited training and understanding of health complications for children born preterm, and little evidence exists regarding adult practitioners’ knowledge to care for these adults. Preliminary adult primary care guidelines were recently created to screen and manage prematurity-related health complications.
Health risks from prematurity are also risks to equality and justice. Women who bear social risk factors are more likely to give birth early. This includes Black women, those living in socio-economically depressed areas, and women with two or more Adverse Childhood Experiences. The many arms of racism and caste-based inequalities can complicate and worsen the health of people already at risk from preterm birth.
Attention also needs to be drawn to the prematurity research community. To date, research has focused on younger age groups and predominantly White populations. Future research needs to seek out ethnically diverse populations and comprehensively examine potential lifecourse complications of early birth. This is especially important when considering how socioeconomic factors may influence the allostatic load of individuals.
For many born preterm, prematurity is not just a health concern, it’s a matter of who they are. Their perception of health over time, or health related quality of life (HRQL), is a critical outcome. To date, this evidence varies with age, degree of prematurity and reporter; clinicians and parents tend to rate HRQL more negatively than survivors. Preterm-born individuals may not have event memories but, early birth repercussions can reverberate through family narratives and unique life experiences. Some identify as typically developed individuals who happen to have been born early, others as functional and well-adapted “preemies”, and others see prematurity as having colored their lives in negative ways. As prematurity researchers, we aim to uncover and bring awareness to the health outcomes and risks from early birth. A critical need exists for more evidence about adult health following preterm birth and yet, how do we protect individuals with statistically increased risk without unnecessarily pathologizing them?
In clinical practice and research settings, we can take the opportunity to listen to people who were too young as patients to speak for themselves but have riveting and complex stories about preterm birth’s effects. We are aware of just one other published qualitative study about the experiences of adults born preterm. Because most adult healthcare providers have yet to acknowledge and factor this experience into patient care, individuals born preterm are finding alternative avenues to be seen. Adults born preterm report seeking online community and support, connecting globally with people over shared early life experiences, while simultaneously making their needs and identities known.
As a research team, we strive to avoid labels for people born early but have nonetheless found that they are, in often subtle ways, a special group. They beat the odds as infants. Their birth and subsequent survival affected their families and communities in unprecedented ways. As clinicians and researchers, we can attend to the health risks of those born premature while acknowledging and celebrating their unique strengths and perspectives, often resulting from their early life experiences.
Fellows Column: The Quiet Strength of The Toybox Inn 11
Kevin Kafaja, MS III
As a third-year medical student, I had rotated through cardiac, neuro, and general ICUs. Each one buzzed with alarms and urgency, charged with adrenaline. But the NICU was different. It didn’t scream. It whispered.
My mother is a pediatrician, and I spent much of my childhood in the corners of her clinic—listening in on patient visits and soaking in the soft rhythm of care. I thought I understood Peds. But the NICU was something else entirely. It was intimate. Intentional. There were hours of serenity—gentle beeping monitors, quiet footsteps—but the stillness could break in an instant. A desaturation alarm. A sudden change. A Code White echoed overhead, and then the team would move—fast, focused, all hands in motion.
That’s where I met her—in the corner of the NICU, they lovingly called Toybox Inn 11, home to some of the tiniest, most vulnerable patients. Her crib was tucked neatly within that space, surrounded by soft blankets, daily goal charts, and quiet victories.
She was born on January 9th at just 31 weeks and 1 day, weighing 940 grams. Her mother’s pregnancy had been complicated— monochorionic diamniotic twins, Twin Anemia-Polycythemia Sequence (TAPS), and maternal hyperthyroidism managed with antithyroid medication. She was delivered via C-section under emergent conditions, including ruptured membranes and maternal fever. She required a partial exchange transfusion and respiratory support on 100% FiO₂ shortly after birth.
When I met her on March 5th—Day of Life 55—she had already fought through respiratory distress syndrome, anemia of prematurity, hyperbilirubinemia, and bradycardic spells. She was breathing room air, feeding fully by mouth, and steadily gaining strength. She was growing stronger, one quiet breath at a time.
In my mind, I called her The Little Engine. I loved toy cars growing up—tiny vehicles that raced like giants. She reminded me of that: small but full of force. Her strength wasn’t loud. It was steady. Unshakable.
At first, I was cautious. How do you care for someone so small? But the NICU team showed me—how to cradle her safely, how to monitor her saturation, how to read her tone and anticipate spells. She’d had a few brief episodes—one during a feed, another while asleep—but none in the final 72 hours before discharge.
The Toybox wasn’t just a clinical space. It was a nursery in progress. A pink blanket draped above her crib. A chart titled “My Day” tracked goals and daily wins. Books sat at her bedside— Goodnight Moon and When I Grow Up I Want to Be…, the latter filled with colorful flaps. I’d read it while keeping watch, wondering who she might become and what her future might hold.
Around her were all the quiet markers of care: diapers, wipes, a milk warmer, and an infant stethoscope. Her corner of Toybox Inn 11 was filled with love and progress, written in the smallest details.
Every Wednesday, during interdisciplinary rounds, we reviewed her journey: apnea monitoring, growth tracking, iron and Epoetin for anemia, and feed progression—35 mL of fortified formula every 3 hours. Her hemoglobin held at 9.9, and her reticulocyte count was strong at 5.4. She crossed the 2000-gram milestone. Each marker is a step closer to going home.
Her mother was a constant presence—gentle and calm. Watching her feed and hold her daughter reminded me that medicine begins not with machines but with presence.
She stayed in the NICU for 2 months and 8 days, and on March 18th, she went home—discharged at 40 weeks and 6 days corrected age, weighing 2170 grams. Her final measurements were length 43 cm, head circumference 34 cm, and abdominal girth 27 cm. She left wrapped in pink, lying in her open crib, breathing independently on room air.
Her discharge plan included a high-calorie formula, follow-up with her pediatrician for weight and EPO management, appointments at the High-Risk Infant Clinic, and a referral to the Regional Center within 1–2 months. I was there the day she left. I watched her resting peacefully in her open crib, bundled and ready to go. Her parents arrived later after I had already stepped away. But when I heard she had gone home—to reunite with her twin brother—it felt like a quiet victory. One we all shared.
In The Toybox, I learned that strength doesn’t always shout. Sometimes, it weighs just over two kilograms, sleeps under a pink blanket, and softly breathes while growing stronger every day.
She was my patient. But more than that, she was my teacher. And in that quiet corner of the NICU, I learned that even the smallest hearts can leave the most lasting marks.
– Adults born preterm report experiences of social exclusion such as being bullied
– They report high sensitivity, reduced stress resilience and tire more easily
– Many report that family, peer and mental health support has helped them most
– Prematurity should be recognized as lifelong condition by health professionals
– Many express gratitude for their life and lead a good life
Abstract
Background
Adults born preterm face greater social, cognitive, mental and physical challenges in adulthood than their full term born peers according to longitudinal studies. In contrast, little is known about the lived experiences of adults born preterm.
Objective
The study investigates the lived experiences of adults born preterm across the life course and their views on health care support.
Methods
A qualitative study of 21 participants completing semi structured interviews analyzed through content analysis.
Results
Over half of adults born preterm report trauma and feeling of otherness since early childhood, high sensitivity to the environment, higher introversion/shyness and social or performance related anxiety. Over half reported that their parents were traumatized by the preterm birth and tried to compensate by overprotective parenting that, however, stifled them becoming independent. Over half experienced bullying victimization and many have continuing mental health problems. Overload by demands in school or work is a consistent theme that makes it hard to have the energy to socialize. Many received physical therapy in childhood and most had psychotherapy in adulthood. Many feel that health professionals trivialize the long-term effects of prematurity and most find support from their parents or peer network.
Conclusions
Prematurity has significantly shaped the life of adults born preterm. Greater awareness and recognition of the unique needs of this group are essential to provide adequate support. Existing services fail to address these needs highlighting an urgent demand for enhanced social and psychological services for educational and workplace settings.
Top 10 Neonatology Startups with Cutting-Edge Medical Devices
Magdalena Sroka, Content Writer 30.08.2024
Neonatology startups aim to take care of newborns, especially premature babies. These highly vulnerable beings require exceptional care, as even the smallest changes can significantly impact their health and development. Sometimes, even the experience and knowledge of doctors aren’t enough to save the little one. Therefore, in a world where technology plays an increasingly vital role, neonatology startups become invaluable support for medical care. By combining advanced technology with specialized knowledge, it is possible to provide newborns, particularly those born prematurely, with the best care and a chance for a healthy start in life.
Necessity is the mother of invention. When designing medical devices for newborns, it is crucial to remember that they will serve the most fragile patients. This often requires an unconventional and comprehensive approach to problem-solving. In this article, we present 10 neonatology startups, whose innovative ideas have the potential to transform this field of medicine.
Neonatology Startups Which Can Shape The Future
AMNION LIFE Amnion Life is working on an advanced incubator called AmnioBed, designed to replicate the conditions inside the womb. The goal is to support the development of premature infants by regulating temperature, protecting the skin, and managing fluids. The device is intended to provide warmth, humidity, and protection to newborns in a way that prevents hypothermia and water loss.
PRAPELA Founded in 2018, Prapela is a startup developing a device that uses vibrations to improve breathing patterns and sleep in newborns. This is aimed at helping stabilize breathing and oxygenation, particularly in infants suffering from apnea, intermittent hypoxemia, and neonatal opioid withdrawal syndrome (NOWS).
PEDIAFEED PediaFeed’s mission is to improve the feeling process for newborns who struggle with it. The company is developing a special type of tube for neonatology and pediatric patients, which minimizes the risk of tube displacement. It is also designed to be easy to insert and remove both in hospitals and at home, while causing minimal discomfort to the baby. Without proper nutrition it is hard to provide a healthy development.
PREGANBIT PRO This startup has developed a telemedical device for monitoring fetal well-being through cardiotocography (CTG). The portable device enables remote diagnostics and allows regular monitoring of the health of both mother and baby, including fetal heart rate and uterine contractions. Thanks to this technology, women can perform tests at home between medical visits, with results being transmitted and analyzed by doctors. Pregnabit Pro aims to enhance early detection of potential risks, increase pregnancy safety, and provide peace of mind to expectant mothers.
ZOUNDREAM Zoundream utilizes artificial intelligence and sound recognition to develop technology that can identify and interpret different types of newborn’s cries. The technology not only focuses on distinguishing the baby’s needs (hunger, tiredness) but is also capable of alerting parents to potential pathologies or developmental disorders. Zoundream’s goal is to provide a tool that enables faster responses to an infant’s needs while offering better support for parents.
VENTORA Ventora aims to create a device that allows precise real-time monitoring of airway pressure in newborns. The company is working on a solution that improves the process of mechanical ventilation while minimizing the risk of complications associated with traditional ventilation. Additionally, Ventora’s device is designed to assist in selecting the best therapy for the youngest patients.
OTONEXUS OtoNexus is a startup developing a diagnostic device (in the form of an otoscope) to detect middle ear infections and distinguish their origins in children and infants. The technology behind it is based on ultrasound, which enables quick and precise diagnosis, helping doctors make informed treatment decisions. Moreover, this approach could reduce the number of misdiagnosed and unnecessary antibiotic treatments.
BAMBI MEDICAL Bambi Medical has developed a wireless system for monitoring the vital signs of newborns, such as breathing, pulse, and temperature. Their solution replaces traditional invasive methods that rely on wires and cables. This provides greater comfort and freedom of movement for preterm infants, and is also gentler on the skin. The device sends data to the NICU monitor and alarm system, collected via a silicone strap placed on the baby’s chest, and alerts when apnea occurs.
PREEMIE SENSOR Preemie Sensor is working on an advanced device to analyze breast milk for nutrient content, specifically measuring fat, protein, and caloric value. The sensor is paired with software, allowing for the monitoring and optimization of nutrient intake by babies. Ensuring proper nutrition reduces the likelihood of complications associated with prematurity.
OWLET BABY CARE Owlet Baby Care is a startup specializing in the creation of smart devices for supervising the vital signs of infants, such as heart rate and blood oxygen levels. The data is collected via socks worn on the baby’s foot and then displayed in a mobile app. This technology provides continuous monitoring, giving parents peace of mind and a chance to feel less stressed and anxious.
Summary
The solutions developed by these neonatology startups not only make it easier to monitor and manage the health of the youngest patients, but also enhance the safety and comfort of both children and their parents. Although not all devices are available on the market yet. Some are awaiting certification, yet they offer hope for saving more premature babies. Thanks to these innovations, the future of neonatal care is becoming increasingly promising, bringing relief and peace of mind to families around the world. Good job startupers! 🫶
If you’re interested in supporting or helping shape the future of neonatal care, don’t hesitate and get in touch with us!
New evidence from a world-leading Victorian study following premature babies into adulthood shows that babies born before 28 weeks’ gestation are doing surprisingly well as young adults in their twenties.
In a paper published in PEDIATRICS, new data released from the Victorian Infant Collaborative Study (VICS) 1991-92 cohort reveals insights from the 25-year point of the long-term study.
The study, co-led by the Royal Women’s Hospital and Murdoch Children’s Research Institute (MCRI), shows that extremely prematurely born adults are just as likely to have completed secondary school, be in paid work, and be in a romantic relationship, compared to their peers born at full term.
Dr Lauren Pigdon, Research Officer at MCRI, analysed the new data from the unique Australian geographic cohort who were recruited at birth and followed for 25 years.
“A strength of this study is that it represents the earliest survivors of the post-surfactant era to navigate the transition into adulthood and fills a gap in knowledge,” Dr Pigdon said.
The introduction of exogenous surfactant in the early 1990s was a game changer in treating respiratory distress syndrome in newborn intensive care. Since then, there has been a dramatic rise in survival of infants born extremely preterm (younger than 28 weeks’ gestation) or with extremely low birthweight (less than 1000g).
With increased survival rates of even the tiniest babies, concerns arose that these tiny babies might have increased chances of health and developmental problems as children and adults. And that this may in turn have an impact on their transition into adult life. But is this true?
“Our data paints a positive and encouraging picture,” Dr Pigdon said. “There were minimal group differences in self-reported general interpersonal relationships, satisfaction with different aspects of life, and current smoking behaviour.”
However, Professor Jeanie Cheong, Consultant Neonatologist at the Women’s and Co-Group Leader of the Victorian Infant Brain Studies group at MCRI, said there were some differences between the groups.
“More adults born extremely preterm had their main income source from government financial assistance and more had not yet moved out of the parental home compared with their peers born full term,” Professor Cheong said.
“Data from the past 25 years has allowed us to look at how, over time, care has improved for Victoria’s youngest and most vulnerable patients,” Professor Cheong said.
“While survival rates have gone up, we now also know that these babies have the chance to become fully functional members of our society.
“Findings from our study are relevant when counselling families after their baby is born, to put into perspective what the long-term outcomes may mean for their child.”
Meet Duane:
Duane has certainly grown up since he was born extremely premature at 26 weeks’ gestation in March 1992. He weighed only 886 grams at birth.
“I was so tiny that my father’s wedding ring could fit all the way up my arm to my shoulder,” Duane remembers.
After a happy and normal childhood, Duane completed high school and became a competitive slalom skier, trying out for the Australian National Team. While he is an experienced downhill racer avoiding major obstacles, Duane faced a few health issues and injuries in his early 20s.
Duane is now a professional skiing and snowboard instructor. He follows the snow seasons and enjoys living and working abroad. He spent a long time in Austria, where he completed a sports diploma in Innsbruck, and now speaks German fluently.
Currently, Duane is keen for his torn ACL in the knee to heal. Then he plans to hit the slopes again and has offers to work in the USA, Japan and Europe.
Objectives: Imperforate hymen (IH) is one of the most common obstructive congenital anomalies of the female genital tract. In this condition the hymen occludes the vaginal opening obstructing effluent discharge. Early diagnosis is possible, as new-born vaginal secretions stimulated by maternal oestrogen cause hymenal bulge, which is an abnormal finding.
The aim of this abstract is to highlight potentially missed opportunities for a neonatal diagnosis of IH. Delayed presentations are associated with significant morbidity such as chronic and severe abdominal pain, acute urinary retention, obstructive uropathy and endometriosis.
A full physical examination of the new-born within 72 hours after delivery is the required standard of the New-born and Infant Physical Examination Screening Programme (NIPE) and National Institute of clinical Excellence (NICE) quality standard 37, statement 7. This includes anogenital examination looking at patency of orifices at birth and at 6 weeks check.
Methods: We conducted a survey, using Survey Monkey portal with the objective to review current clinical practice in postnatal examination. The link was distributed via WhatsApp and email to paediatric trainees, general practice trainees and clinical fellows at our trust and London wide.
Responses were collected over 12 weeks. Following questions were asked looking for a yes or no response.
– Do you perform a genital examination in NIPE?
– Are you aware that NIPE recommends complete examination of the genitals to check for normal
appearance and patency?
– Do you examine for hymenal opening in female babies by separating labia?
– Are you aware of the findings in imperforate hymen?
– Are you aware of the consequences of delayed diagnosis of imperforate hymen?
– Have you ever picked up an imperforate hymen in neonatal examination?
Results: Out of 220 doctors, 132 responded to the survey questions which resulted in a 60% response rate.87.8% performed a genital examination as a part of NIPE.78.7% were aware that normal patency and appearance of the genitals must be checked. Only 25.7% were examining hymenal opening by separating the labia majora and 35.6% were aware of the findings of IH. 7 out of 132 doctors had made a diagnosis in the neonatal examination. 60% were aware of consequences of a delayed diagnosis.
Conclusion: Our survey highlights insufficiencies in female new-born genital examination. There is a need for increased awareness amongst clinicians about this condition, as there exists a window of opportunity to make an early diagnosis and minimise suffering and morbidity.
🌍 WARRIORS: A Global Conversation for Preemie Survivors
Premature birth doesn’t end at discharge—it echoes throughout life. As survivors, we are not defined by our early start—we are defined by our strength, our resilience, and the legacy we choose to build. From the NICU to adulthood, our stories carry both scars and strength. And now, more than ever, the world needs our voices.
The NW Warriors community reflects a growing global collective—of preemie survivors, families, clinicians, researchers, and advocates—who recognize that prematurity is not a condition left behind in infancy. It is a thread woven into identity, healthcare, and social equity across the lifespan. Whether you were born early, raised a NICU warrior, or cared for one—you are part of a movement greater than any diagnosis.
💥 Why the Warrior Movement Matters
Prematurity is not just a medical event—it’s a lifelong journey. Survivors grow into athletes, educators, scientists, artists, and caregivers. Some carry physical or emotional complications. Others carry memories of separation, struggle, or stigma. All carry a story of endurance.
This is a historic moment. For the first time, the world is witnessing a full generation of NICU survivors reaching adulthood in global numbers. Their experiences bring urgency to overlooked conversations—on trauma-informed care, long-term health, and identity. Their insights are reshaping how neonatal care is defined, not just in the early days, but across the life course.
We are not just patients. We are architects of change. We are storytellers. We are warriors.
🌐 A Growing Global Dialogue
Across countries and cultures, NICU survivors and neonatal communities are coming together. We are asking new questions:
What does it mean to be born too soon—and grow into your power?
How can we center survivor experiences in clinical and policy conversations?
What role does memory, trauma, or advocacy play in healing?
How do we recognize preterm birth not just as a medical statistic, but as a lived reality that shapes lives and futures?
There is no single answer. But there is space for all of us here. Some find their power through writing, art, research, or mentorship. Others speak through quiet acts of presence and parenting. Some fight for structural change. Others simply want to be heard, held, and understood.
What unites us is this: We were born into adversity—and we rise with intention.
🛡️ Rewriting the Narrative
As adults born preterm, or as families and clinicians who lived that journey, we are no longer hidden in hospital charts or lost in long-term data. We are here—visible, vocal, and unafraid to lead.
This movement doesn’t require permission. It begins in honest conversations, in shared memory, in reclaiming our stories from silence. It grows as we listen to each other, uplift survivor narratives, and demand that care systems honor the full trajectory of human life.
We are not asking for pity. We are offering power. We are not defined by fragility. We are evidence of strength. We are not waiting. We are rising.
✊ Join the Conversation
Wherever you are—in policy, in practice, in healing, in hope—this conversation is yours. The warrior journey is not just about what we survived. It’s about what we build next.
MEET THE YOUNG CLIMATE PRIZE COHORT! After Mohammed Anowar fled Myanmar with his family to a refugee camp in Bangladesh, he saw hundred of trees being cut down and decided to start a climate hub. The Community Climate Action Initiative aims to tackle pressing climate challenges such as heatwaves, landslides, and flooding through a multifaceted approach. The project includes a Tree Planting Campaign designed to combat deforestation and mitigate heat impacts by increasing local green cover. Complementing this, Climate Awareness Sessions are held to educate community members in the Kutupalong refugee camp about climate change and effective resilience strategies. Additionally, Youth Leadership Training is provided to equip young leaders with the skills needed to advocate for climate action and promote sustainable practices. The initiative is expected to yield a range of positive outcomes, including an improved local environment, heightened climate awareness, and a cadre of empowered youth spearheading climate resilience efforts in the community.
Singapore has a generally efficient healthcare system, even though health expenditures are relatively low for developed countries. The World Health Organisation ranks Singapore’s healthcare system as 6th overall in the world in its World Health Report. Singapore has had the lowest infant mortality rates in the world for the past two decades. In 2019, Singaporeans had the longest life expectancy of any country at 84.8 years. Women can expect to live an average of 87.6 years with 75.8 years in good health. The averages are lower for men.[479] Singapore is ranked 1st on the Global Food Security Index.
Financial Considerations: Medical professionals often face significant student loan debt, which can impact career choices and personal life decisions.
Technological Integration: The integration of technology like telemedicine and electronic health records is transforming how doctors provide care and stay updated with medical advancements.
Communication In Medicine: Effective communication skills significantly enhance doctor-patient relationships and improve treatment outcomes, emphasizing their importance alongside medical knowledge.
In the fast-paced and ever-evolving world of medicine, doctors and residents commit to a lifelong calling. These dedicated individuals spend countless hours honing their expertise, driven by a deep commitment to patient care and medical excellence. While the white coat and stethoscope symbolize readiness and a passion for their practice, the reality of their journey is far more complex, filled with challenges and responsibilities that often play a crucial role in shaping their careers and the care they provide.
This article goes beyond common perceptions, revealing ten surprising facts about doctors and residents that highlight the depth and complexity of their roles. Whether you’re a medical student preparing for the road ahead, an educator nurturing future providers, or a healthcare professional seeking deeper insight, these realities offer a fresh perspective on the field.
Understanding these intricacies fosters greater appreciation, resilience, and professional growth, ensuring that the next generation of physicians is equipped not only with medical knowledge but also with the tools to thrive in both their careers and personal well-being.
Fact 1: Many Doctors Face Student Loan Debt Long Into Their Careers
Becoming a doctor is one of the most rewarding professions, but the financial burden is significant. Many physicians graduate with over $200,000 in student loan debt, impacting career choices and personal milestones. Here are ways that student loan debt can impact medical professionals:
Influences Specialty Decisions: Some choose higher-paying fields over passion-driven specialties.
Delays Major Life Events: Homeownership, marriage, and family planning may be postponed until studies are completed.
Requires Strategic Financial Planning: Understanding repayment options and budgeting is crucial.
Fact 2: Doctors Must Continually Update Their Knowledge
Medicine evolves rapidly, requiring lifelong learning to provide optimal patient care. Continuing education ensures physicians stay updated on the latest research, treatments, and technologies. Here are some reasons why:
USMLE And CME Requirements: Ongoing exams and certifications keep doctors current.
Medical Advancements: New treatments, AI tools, and clinical protocols evolve constantly.
Efficient Learning Strategies: Consistent review of clinical content allows doctors to maintain their medical mastery and mitigate skill decline.
Fact 3: Technology Is Transforming How Doctors Practice Medicine
Technology is revolutionizing healthcare for the better and improving efficiency. Below are some ways technology is changing the healthcare game:
Electronic Medical Records (EMRs): Digitally store and organize patient health information, improving accessibility, documentation accuracy, and care coordination.
Telemedicine: Expands access to remote and underserved populations.
AI And Automation: Enhances diagnostics, workflows, and patient care.
Fact 4: Many Doctors Pursue Research Alongside Clinical Practice
For many doctors, the desire to discover new medical knowledge is as strong as the calling to patient care. Many doctors balance clinical work and medical research to push the field forward.
Medical research:
Advances Evidence-Based Medicine: Research findings shape treatment protocols.
Improves Patient Outcomes: Clinical trials lead to breakthrough therapies.
Strengthens Analytical Skills: Evaluating data sharpens clinical decision-making.
Fact 5: Communication Skills Are As Important As Medical Knowledge
Beyond expertise, strong communication enhances patient trust and treatment outcomes by ensuring clarity, collaboration, and understanding. Below are some communication skills that medical professionals should value:
Clear Explanations: Helps patients make informed decisions.
Interdisciplinary Teamwork: Ensures seamless care coordination.
Active Listening: Strengthens doctor-patient relationships.
Fact 6: The Number Of Female Physicians Is On The Rise
In recent years, the medical field has witnessed a transformative shift as the number of female physicians steadily increases. Women now make up over 50% of U.S. medical school students, creating a more inclusive healthcare environment.
This change not only reflects broader societal advancements but also heralds a new era where diverse perspectives lead to more comprehensive patient care. Here are a few reasons why this trend is a positive force in the medical community:
Enhancing Patient Perspectives: Women in medicine improve representation and inclusivity.
Expanding Leadership Roles: More female doctors are entering executive positions.
Shaping Mentorship And Education: An increasing number of programs support future generations of female physicians.
As more women enter the field, efforts to support career advancement, mentorship, and leadership opportunities continue to grow. These changes contribute to a more balanced healthcare workforce, ensuring that medical education and patient care reflect the diverse needs of the communities they serve.
Fact 7: Residents Are Both Students And Employees
Residents face a tough battle, as they are expected to balance learning with employment. The responsibilities of patient care, combined with a deep, unyielding commitment to mastering the breadth and depth of medical knowledge, create a unique dynamic.
Residents deal with:
Hands-On Experience: Residents manage cases under supervision, participate in medical procedures, and deliver expert care in high-stakes environments.
Long Hours And High Stress: Demanding schedules prepare residents for independent practice.
Balancing Education And Work: Requires strategic planning and smart time management to stay sharp.
At the heart of every successful treatment plan lies a strong doctor-patient relationship. This dynamic significantly impacts treatment outcomes, as trust and communication form its foundation. Here’s why this bond is essential to a positive healthcare experience:
Empathy Improves Patient Engagement: Positive experiences with doctors encourage patients to follow treatment plans accordingly.
Communication Enhances Understanding: Simplified explanations of medical conditions and solutions lead to informed decisions.
Trust Strengthens Compliance: Patients are more likely to return for follow-ups and engage in routine check-ups when they trust their healthcare provider.
Developing effective communication and interpersonal skills allows physicians to foster meaningful connections with their patients. When patients feel understood and respected, they are more likely to adhere to medical advice and treatment plans, ultimately leading to improved health outcomes.
Fact 9: Wellness Programs Are Becoming More Common In Medical Training
The rumors are true: Becoming a doctor is an incredibly long and arduous process. Thankfully, in recent years, wellness programs have been developed to support students and residents with healthy coping mechanisms. These initiatives, including the ones listed below, are a testament to the growing recognition of the demanding pressures faced by medical students and residents and their impact on mental health and overall well-being.
Mental Health Support: Resources such as counseling help prevent burnout.
Work-Life Balance Strategies: Encouraging self-care and mindfulness.
Peer Support Networks: Strengthening community and resilience.
Fact 10: Global Health Opportunities Are Available To Doctors And Residents
Joining global health initiatives allows medical professionals to see firsthand the different healthcare challenges that occur worldwide. This experience can be pivotal in developing resilience and adaptability, skills that are crucial in any medical setting. For residents, these opportunities can be eye-opening, offering real-world applications of their clinical skills in diverse environments. Here’s why global opportunities can be beneficial for the careers of doctors and residents:
Exposure To Diverse Medical Environments: Broadens clinical expertise and adaptability to different clinical settings.
Develops Problem-Solving Skills: Teaches current and aspiring healthcare providers how to work with resource-limited care strategies.
Strengthens Public Health Impact: Contributes to underserved communities worldwide.
These opportunities enrich one’s medical expertise and broaden perspectives on health disparities, resource management, and cultural sensitivity.
Final Thoughts
The road to becoming a doctor is filled with challenges, sacrifices, and unexpected realities, yet it remains one of the most enriching careers. Understanding these crucial facts about doctors fosters greater empathy and appreciation for those dedicated to medicine. While the path is demanding, each step brings the opportunity to grow, refine skills, and make a meaningful impact on patient care.
By embracing a structured and comprehensive approach to medical education, future providers can develop true mastery. Investing in both clinical knowledge and personal well-being ensures not only success in training but also longevity and fulfillment in practice. Whether you’re a medical student, resident, or educator, every effort you make strengthens your ability to provide exceptional, compassionate care, shaping the future of healthcare for the better.
REALLY IN LOVE Written by: Benjamin Kheng Produced by: Benjamin Kheng, Evan Low Performed by: Benjamin Kheng Mixed & Mastered by: Charlie Kurata Spatial Audio Master by: Luke Nicholas Foo
Team from KKH, SGH aims to develop screening tool to identify women at risk of premature births
SINGAPORE – Her son weighed just 700g when he was born at 24 weeks after she spent the two weeks prior in hospital due to vaginal bleeding and cervix dilation.
Ms So Bee Leng’s son, Ethan Ang, was born in 2017 with multiple disabilities stemming from his extreme prematurity. At seven days old, he underwent his first major surgery when his intestines were operated on.
For the next five years, he underwent four more major operations, which included implanting a cochlear hearing device, laser eye surgery to help with his vision and placing a feeding device through his belly to the stomach.
It is currently a challenge to identify mothers at risk of giving birth to premature babies as the only gauge is when mothers have had previous preterm births, like Ms So, said Professor Teoh Tiong Ghee, director of maternal and child global health and care transformation at KK Women’s and Children’s Hospital (KKH).
To proactively reduce and prevent prematurity, a 10-member team of doctors specialising in newborn care and high-risk pregnancies from KKH and Singapore General Hospital (SGH) will start work on a new Preterm Pregnancy Prevention Programme in October.
The team aims to create a national database of all preterm pregnancies to identify risk factors, and then use this information to develop a screening prediction tool that can accurately assess the risk of preterm pregnancies.
A baby born before 37 full weeks of pregnancy is considered to have been born preterm or prematurely. A preterm baby’s organs may not be fully developed.
A full-term pregnancy typically lasts about 40 weeks, and babies’ birth weights typically range from 2.5kg to 4.5kg.
Globally, 13.4 million babies – 10 per cent of all births – are born prematurely each year and one million die from preterm complications.
Prematurity is the leading cause of death for children under five.
In 2023, 8.2 per cent of births in Singapore were premature, slightly lower than the 8.8 per cent recorded in 2014.
Recalling the dilemma she faced when told she might deliver early and her baby would develop health complications, Ms So, 38, said: “I was given the choice to either terminate the pregnancy or continue with bed rest in the hospital until I gave birth.
“After weighing the pros and cons, and discussing with my husband, we decided to carry on and accept whatever may come in the future.”
When she conceived again in 2023, her doctor told her she was at risk of another premature delivery. She was referred to the Preterm Birth Clinic at KKH’s Stork Centre, where she was closely monitored.
She underwent a procedure to stitch her cervix – the birth canal opening – when she was 12 weeks along, paving the way for the full-term birth of her daughter, Alysha Ang, at 38 weeks.
Called a cervical cerclage, the procedure is done to help the cervix hold a pregnancy in the womb to prevent preterm birth.
Dr Ilka Tan, a senior consultant at KKH’s department of maternal foetal medicine who oversaw Ms So’s care during her second pregnancy, said that infants are able to survive outside the uterus at 24 weeks.
She added that though there are rare cases of infants surviving when born at 22 or 23 weeks, the “outcome is still not very good” for these babies.
Acknowledging that there have been reports from around the world of some babies born around 22 weeks who have survived, she said: “Those are single anecdotal cases, but it’s not the norm.”
If diagnosed through screening and predictive tests early, mothers who are at risk of preterm births can undergo various treatments to help them bring the pregnancy to term, Dr Tan said.
These include taking the hormone progesterone and getting a cervical cerclage.
The Preterm Pregnancy Prevention Programme will use information collated to study common characteristics among women who deliver prematurely. This in turn can be used to develop a prediction tool to identify expectant mothers who are at risk of preterm births early, so that preventive measures can be taken.
“What we’re trying to do is to get all these demographics, and use biomarkers from blood and cervical length measurements, to try to predict each woman’s personalised risk so as to target with specific therapy,” said Prof Teoh.
The programme is funded by a $500,000 grant from Far East Organization.
Besides the child potentially suffering long-term health consequences and an increased risk of disability and developmental delays, the parents and the rest of the family experience long-term stress too, Prof Teoh noted.
“Some have to stop work to look after the kid. So not only does it have a psychological impact on the family, it’s got a big financial impact as well,” he added.
Dr Tan also leads the Preterm Birth Clinic at KKH that provides specialised care for women who may have a higher risk of having premature babies.
The clinic began operations in July 2021 and had 100 patients that year. In 2024, 402 patients were referred to the clinic from January to September.
Ms. So said she received personalised care and attention at the Preterm Birth Clinic to help her carry her second child to term.
“I was seen by the same doctor – it wasn’t random. So I felt well-looked after and relieved. I was assured that there was a plan to help me, and that was important.”
Skin-to-skin cuddling with a parent has lasting cognitive benefits for premature babies, according to a new Stanford Medicine study. Preemies who received more skin-to-skin contact, also known as kangaroo care, while hospitalized as newborns were less likely to be developmentally delayed at 1 year of age, the study found.
The research, which was published online July 11 in The Journal of Pediatrics, showed that even small increases in the amount of skin-to-skin time made a measurable difference in the babies’ neurologic development during their first year.
“It’s interesting and exciting that it doesn’t take much to really improve babies’ outcomes,” said the study’s senior author, Katherine Travis, Ph.D., who was an assistant professor at Stanford Medicine when the study was conducted and is now an assistant professor at Weill Cornell Medical School and Burke Neurological Institute.
The study’s first author is Molly Lazarus, a clinical research coordinator in pediatrics previously at Stanford Medicine and now at Weill Cornell Medical School.
The intervention is simple: With the baby only in a diaper, a parent holds the baby on their chest, next to their skin. But because hospitalized preemies are small and fragile, and often hooked to lots of tubes and wires, holding the baby can seem complicated. Parents may need help from their baby’s medical team to get set up. That work is worth it, the study showed.
“It didn’t matter if the baby was from a high- or low-income family; the effects we found were the same. And it didn’t matter if the baby was sicker or less sick—both responded to this treatment,” Travis said.
Neurological complications are challenging
Over the last 50 years, preemies’ survival rates have improved dramatically thanks to better treatments for many of the complications of prematurity, which is defined as being born at least three weeks early. For instance, neonatologists have developed effective approaches to help preemies breathe, even with immature lungs, while in the neonatal intensive care unit.
But premature birth still leaves babies at risk for long-term neurodevelopmental problems, including developmental delays and learning disabilities. Doctors and families have long hoped for treatments they could use during the newborn period to prevent such challenges.
“Ultimately, we want our patients to be healthy kids who can achieve the same milestones as if they didn’t come to the NICU,” said study co-author Melissa Scala, MD, clinical professor of pediatrics. Scala is a neonatologist who cares for preemies at Lucile Packard Children’s Hospital Stanford.
“Our finding legitimizes skin-to-skin care as a vital intervention in the neonatal intensive care unit to support our goal of getting that child out of the hospital, able to learn and develop,” Scala said.
Skin-to-skin care was first used in low-income countries to boost babies’ survival, where it is often used for healthy infants born after full-term pregnancies. In rural or impoverished areas, it is an essential way to keep newborns warm, promote parent-child bonding and facilitate the start of breastfeeding.
It’s been slower to catch on in the United States, especially for premature babies, who generally receive high-tech intensive care. But a growing body of research suggests that the practice has benefits for preemies’ brains, possibly because it could offer some of the same developmental inputs they would have received if they had not been born early.
More skin-to-skin was better
The research team reviewed medical records for infants who were born very prematurely, meaning at least eight weeks early, and were cared for at Lucile Packard Children’s Hospital Stanford between May 1, 2018, and June 15, 2022. Nurses in the hospital’s NICU had begun making notes in patients’ medical charts about developmental care practices, including the amount of time parents held babies skin-to-skin, shortly before the study began.
The study included 181 preemies who did not have genetic or congenital conditions known to affect neurodevelopment and who had received follow-up evaluations after they left the NICU. All very premature babies are eligible for care through California’s High Risk Infant Follow-Up program until age 3. The program provides developmental testing and connects families to appropriate therapists if their children have developmental delays.
The study used records from follow-up evaluations that the babies received at 6 and 12 months’ adjusted age, meaning their ages were corrected to account for how early they were born.
The evaluation included measures of visual-motor problem solving in standard tasks (such as dropping a cube into a cup) and expressive and receptive language skills (such as turning to see where the sound of a bell is coming from).
In addition to accounting for infants’ gestational age (how early they were born), the outcomes were adjusted for families’ socioeconomic status and for four common complications of prematurity: bronchopulmonary dysplasia, a breathing complication; brain hemorrhage, or bleeding; sepsis, an infection of the bloodstream; and necrotizing enterocolitis, an intestinal condition.
The infants in the study were born, on average, at about 28 weeks’ gestation, or about 12 weeks before their due dates. They stayed in the hospital for an average of about two and a half months.
Babies in the study averaged about 17 minutes a day of skin-to-skin care, usually in sessions lasting more than an hour but occurring less than two days per week. Seven percent of families did not do any skin-to-skin care, and 8% did more than 50 minutes per day.
Small increases in the amount of skin-to-skin care were linked to large differences in 12-month neurodevelopmental scores. An average of 20 minutes more per day of skin-to-skin care was associated with a 10-point increase on the scoring scale used for neurodevelopment. Similar to an IQ test, the scale has an average of 100 points; a score of 70 or less suggests significant developmental delays.
The frequency and duration of skin-to-skin contact predicted 12-month cognitive scores even after controlling for possible confounding factors, including the infant’s gestational age and medical complications, and the family’s socioeconomic status and frequency with which they visited the NICU.
How does it work?
Although the study was not set up to explore how skin-to-skin care benefits babies’ brains, the researchers have some educated guesses.
“We think of the womb as our benchmark for preterm babies. In utero, a fetus is physically contained, listening to the maternal heartbeat, hearing Mom’s voice, probably hearing her digest her sandwich,” Scala said. “In the NICU, they’re not next to anybody, and they hear the fan in the incubator; it’s a very different environment. Skin-to-skin care is probably the closest we can get to mimicking the womb.”
Parents can also benefit from skin-to-skin care, and this in turn may benefit their newborns, the research team said.
“The environment of the NICU is very stressful for parents and babies, and skin-to-skin care may buffer that,” Travis said, noting that it is not unusual for parents with a very tiny, sick baby to develop post-traumatic stress disorder.
In addition, many preemies are not developmentally ready to breastfeed, and skin-to-skin care can provide an alternate way to promote bonding between parents and babies.
The researchers hope their findings will motivate medical teams to help parents provide skin-to-skin care in NICUs across the country and will encourage parents by showing them the long-term benefits of this simple but important technique.
Packard Children’s recently expanded its infant developmental care program by hiring neurodevelopmental nurse practitioners, more physical and occupational therapists, a psychologist, and child life and music therapy experts for their NICU and intermediate care nurseries. The expanded team can make customized developmental care plans for high-risk infants.
Scala hopes other hospitals will follow suit.
“I would love for people to see this as part of the medical plan, not just something nice we’re doing, but to be really intentional about it,” Scala said. “Our findings underscore the value of having parents on the intensive care unit, doing this important part of infant care.”
Imagine giving birth at 22 weeks—facing the uncertainty, the emotional rollercoaster, and the challenges of an 8-month NICU stay. For Asma, this journey was life-changing, but it also ignited her passion for advocacy, helping other parents navigate the NICU experience with confidence and strength. Join us as Asma shares: ✅ Her raw & real experience as a NICU mom to baby Cylia Maria ✅ The emotional & logistical challenges of a long NICU stay ✅ The transition home—what she wishes she knew ✅ How sharing her story has fueled her passion for advocacy & parent empowerment ✅ Guidance for parents: questions to ask & how to take an active role in their baby’s care.
It can be very stressful having a baby in the NICU. During this time, it is helpful to include siblings as much as possible; to explain in simple terms what is happening with your new baby; to reassure them that they have not caused the baby to be early, sick, or small; and to remind them that they are not the source of your current worries. Most of all, you should reserve special time just for them, and remind them daily of your constant and unconditional love. More than ever, they need to feel secure, valued, safe, and loved by you and others.
Platypus Media is proud to offer a number of NICU sibling support resources. We hope these will be meaningful and useful for families experiencing the difficulty of having a child in the NICU.
The Come Home Soon coloring book series (available for baby boys and girls, in both English and Spanish) will help you guide your children to an understanding of why their baby sister or brother is in the NICU, and what they can do to help.
Rich and Creamy for Our Preemie, by Naomi Bar-Yam, ACSW, Ph.D., available in English and in Spanish, is a coloring book about how the NICU, milk banks, and families work together to help preemies.
Here is a list of other NICU sibling support resources:
Hand to Hold sibling support webpage (www.HandToHold.org) offers sample activity pages and NICU video tour.
No Bigger than My Teddy Bearby Valerie Pankow describes the NICU experience through the eyes of a new big brother.
My Brother is a Preemie/My Sister is a Preemie:A Children’s Guide to the NICU Experienceby Abraham R. Chuzzlewit & Dr. Jos. A. Vitterito II gives a child-friendly introduction to the NICU.
The Invisible Stringby Patrice Karst reassures children that even when loved ones are apart, they are always in each other’s hearts.
Keep reading for a list of organizations that help preemie families…
Different Dream serves as a gathering place for parents with special needs children.
Hand to Hold provides resources and support to parents of preemies, babies with special health care needs and new parents who have lost a baby.
Human Milk Banking Association of North American provides information and resources on donor milk banking for parents and health care providers. It also sets safety guidelines for all non-profit mothers’ milk banks in North America.
Kangaroo Mother Care promotes skin-to-skin contact, a universally available and biologically sound method of care for all newborns, and preemies in particular.
La Leche League International is a mother-to-mother breastfeeding support organization. They are a source of information and firsthand accounts related to providing preterm babies with breastmilk.
Managing the Neonatal Intensive Care Unit is an article from the Loyola University of New Orleans’ online nursing resource center. A great resource for students, professionals, and even parents of babies in the NICU.
March of Dimes (MOD) has a wealth of information about the NICU. They support an online community especially for NICU families. March of Dimes NICU Family Support programs operate in many NICUs. (Also available in Spanish.)
NICU Parent Support Site provides information, resources, and encouragement to reassure and support NICU parents.
Prematurity strives to support preemie parents by providing information on prematurity and preemie care.
Preemie Parent Alliance(PPA) represents a number of organizations that help support the parents of preemies and strives to improve the quality of the care they provide.
Preemie World brings together parents and professionals in the NICU. They strive to educate and help make the transition to home easier for everyone.
Ronald McDonald House serves as a home away from home for families with children receiving medical treatment. Families can do laundry, eat freshly cooked meals, sleep in private rooms, and gain/give support with other families.
Supplemental Security Income (SSI) and Medicaid Programs provide financial assistance for NICU medical expenses. Eligibility for assistance is determined by a baby’s birth weight rather than an income. You must apply for these programs shortly after your baby is born. Ask your social worker or care manager for assistance.
WIC (Women, Infants, and Children) provides nutritious foods to supplement diets, information on healthy eating, and referrals to health care for women, infants, and children up to 5 years. Even if you have been denied Medicaid due to financial reasons, you might still qualify for WIC.
Fetal heart rate (FHR) patterns are a critical tool for assessing a baby’s well-being during pregnancy and labor. Nurses must understand how to interpret these patterns to ensure safe care. Here are the key takeaways:
Baseline FHR: Normal range is 110-160 bpm. Below 110 bpm (bradycardia) or above 160 bpm (tachycardia) may signal distress.
Nurses must act quickly on abnormal patterns by repositioning the mother, administering oxygen, or preparing for emergency delivery. Accurate monitoring, documentation, and clinical judgment are essential for ensuring the safety of both mother and baby.
The moonlighter had just returned with our dinners when the code alarm sounded. Almost simultaneously, our pagers went off “Code infant 3312.” We all knew who it was. The 23-week gestation, two-day-old baby had coded earlier in the afternoon and had been doing poorly since. Oxygen saturations were in the low 80s despite maximal support, and blood pressures were marginal on dopamine, dobutamine, and epinephrine drips. Upon entering the room, we found the infant with saturations in the 40s and a heart rate in the 50s. We quickly assumed our positions around the warmer. The resident began chest compressions, the respiratory therapist hand bagged, the fellow at the head of the bed assessed the airway and ordered fluid pushes and medications, the bedside nurse administered the medications, and I, the attending physician, oversaw it all. The nursing staff also rapidly began their roles, one opening the crash cart and drawing up drugs, another charting, and multiple others observing and ready to assist if needed.
We quickly fell into our all-too-familiar routine, counting “one, two, three” for chest compressions, followed by “breath.” Over and over again. “Ten mils normal saline,” said the fellow, followed by “epi, point 0 five” every five minutes. The intern took over the chest compressions after about 10 minutes, but the cadence remained the same. Blood was bubbling up the endotracheal tube, indicating the presence of a pulmonary hemorrhage. A nurse was dispatched to retrieve emergency-release blood from the blood bank. The saturation and heart rate were steadily falling.
The mother was literally rolling on the floor, wailing, “Save my baby! Save my baby!” over and over again.
Despite several rounds of fluids and epinephrine plus a push of the blood, the baby continued to deteriorate. I knelt beside the mother, put my hand on her shoulder, and asked her to listen. She immediately stopped her wailing and looked me in the eye. I told her that her baby was dying, that we were going to stop CPR as it was not working, and that her baby’s brain had been irreversibly damaged. She nodded in agreement.
“Stop,” I said. The scene instantly shifted from the hustle and bustle of a code to a stony silence pierced only by the sobs of the mother whom the nurses had assisted into a recliner chair. The monitor was turned off, the ventilator and lines were disconnected, syringes and other debris were removed from the bed, and the baby was wrapped in a blanket and placed in mom’s arms. The nurses began their familiar postmortem care routine. The fellow auscultated the baby’s chest and confirmed the death.
We returned to the workroom and ate Chinese takeout. I had cashew shrimp. I conducted a debrief during our meal, asking everyone how they felt. The intern was visibly shaken, with a tear trickling down her cheek. It was July, and this was the first death of a patient in her charge since she had become a real doctor. “His life slipped through my hands when you told me to stop,” she said. One of the upper-level female residents hugged her as she sobbed for a while before regaining her composure and resumed picking at her food.
For myself and the fellow, this death was one of many, but each death is new all over again and is a fresh reminder of our human frailty.
Few outside our world would understand a situation like this. We were eating while a baby had just died and a mother was grieving. For her, life had just changed forever. For us, we had to nourish ourselves to have the strength to continue caring for the living. Nothing taught in medical school can prepare one for these moments. They must be experienced first-hand, processed, and reflected upon. Doing so is what gives us the strength to move forward.
4 actions health leaders must take to show doctors they are valued
It takes more than words to show gratitude to physicians. These concrete steps can help doctors feel valued and protect against burnout.
Physician Health – By Georgia Garvey, Contributing News Writer Mar 18, 2025
Good health care leaders realize that physicians need more than free food and thank yous to thrive. Well-meaning expressions of appreciation that do not address the root cause of burnout or stress cannot alleviate physicians’ stress or stave off burnout the way that truly feeling valued can.
But it takes more than knowledge to change a work environment—it takes concrete action.
“Many leaders know the importance of teamwork and communication,” said Jill Jin, MD, MPH, an internist and senior physician adviser for professional satisfaction and practice sustainability at the AMA. “But where they kind of struggle is, how do you actually support the individual at a level that is meaningful for them?”
Dr. Jin discussed “muffin rage,” a phrase that came about as a result of a 2021 Los Angeles Times op-ed by Jillian Horton, MD, when she—deep in the throes of work-related burnout and distress—happened upon a “resident appreciation” event handing out muffins.
“Muffin rage is what we feel when there is a vast chasm between our actual needs and what another person or an institution thinks we need,” Dr. Horton wrote.
Dr. Jin spoke alongside Jane Fogg, MD, MPH, physician director of organizational transformation for the AMA, in a recent webinar on how health care organizations can make doctors feel valued, which highlighted an AMA STEPS Forward® playbook on the topic.
During the event, Drs. Jin and Fogg touched on some of the ways that health systems, organizations and leaders can take actions that will make physicians feel valued in a way that avoids muffin rage, a crucial effort with implications for physician well-being, burnout and even the quality of patient care.
In fact, physician turnover can cost organizations anywhere from $500,000 to $1 million or more for every physician who leaves.
“Aside from it being the humane thing to do, there is also a financial benefit—a business case—for investing in your people,” Dr. Jin said.
For those looking to lessen the load on physicians, a key avenue to pursue is helping them understand the crucial role they play in their organization. Dr. Jin pointed out that research shows feeling valued correlates strongly with lower burnout rates, mentioning a 2022 study published in JAMA Health Forum that found physicians who felt valued had a 37% burnout rate, compared with 69% for those who did not.
As the leader in physician well-being, the AMA is reducing physician burnout by removing administrative burdens and providing real-world solutions to help doctors rediscover the Joy in Medicine™.
Help physicians know their worth
Once the importance of feeling valued as a key mitigator for physician burnout has been understood, Drs. Jin and Fogg said, the next step is determining what, exactly, helps physicians know and understand their worth in an organization.
Instead of superficial gestures like the one described in Dr. Horton’s piece, Dr. Jin said there are ways to effectively communicate gratitude to physicians. Those ways have much more to do with actions than with words.
Some key ways to show doctors they are valued, as described by Drs. Jin and Fogg, were to support:
Schedule flexibility and autonomy.
Paid time off (PTO).
Professional development.
Individual resilience and self-care.
Care during and after trauma.
Make work-life balance a priority
Often it can be difficult to justify costly changes aimed at improving physicians’ work conditions, said Dr. Fogg, but overwork and lack of autonomy in matters such as scheduling result in burnout, which is even more expensive.
“Productivity is a pressure that we often feel because of falling revenues across the health care landscape,” she said. “With pressure to fill our schedules, we can lose valuable time for our continuity patients. This tension between being productive and being available to our own patients often lies in how we design and manage our schedules.”
The key, Dr. Fogg said, is giving doctors the ability to “co-design the scheduling processes with their operational team. Make sure you partner with operational leaders to have a physician voice in designing the optimal schedule system for patient access, continuity, and work life balance.”
PTO is another area of concern for organizations looking to create a culture of value, Dr. Jin said.
Health care leaders can be role models in taking time off themselves, and organizations can proactively block off vacations, celebrate time off and resist the impulse to praise working while out of the office. Physicians’ responsibilities should also be fully covered when they’re on vacation, and compensation models and appointment schedules should take PTO into account.
Support the physician as a person
To show a physician that they are more than just a cog in the machine, their professional development must be supported, recognizing their individual aspirations and passions beyond the clinical practice of medicine.
“Feeling valued means the people around you—your supervisor in particular—know who you are, what excites you and what makes you passionate” outside the confines of the clinic or hospital corridor, Dr. Fogg said. “Asking physicians about their long-term goals and offering opportunities to get involved in a variety of activities outside of clinical practice can create a stronger sense of feeling valued. Some opportunities for growth include teaching, research, process improvement initiatives, leadership, community engagement and more.
And, said Dr. Jin, while “self-care” is not a replacement for—and should not be the major focus of—systemic efforts to reduce burnout, organizations can support an individual’s resilience by helping physicians set boundaries, prioritize tasks and limit their distractions. Leadership also should provide resources for and support physicians in self-care, promote collegiality and create spaces for breaks.
Additionally, the credentialling process should remove questions about mental health care so they don’t discourage physicians from seeking care if needed.
“Burnout is not a sign of mental illness, but there is a lot of overlap that happens when we are severely distressed by the way in which we’re practicing and what we’re witnessing in our practices,” she said.
For more information on this and other topics, explore the AMA STEPS Forward open-access toolkits and playbooks, which offer innovative strategies that allow physicians and their staff to thrive in the new health care environment. These resources can help you prevent burnout, create the organizational foundation for joy in medicine and improve practice efficiency.
Combat physician burnout
Event: American Conference on Physician Health (ACPH) Sept. 11-13, 2025, focusing on steps organizations can take to improve physician well-being
CME: How health systems can reduce physician burnout
Calculate: See the cost of physician burnout to your organization
Video: Latest trends in physician burnout by specialty
Question Do individuals born preterm have a higher risk of short-term and long-term mortality compared with those born at term?
Findings In this cohort study of 4 998 560 births, individuals born preterm had a higher risk of mortality from birth to age 36 years, with the highest risk observed from birth through early childhood. The risk of mortality varied by gestational age at birth and was more pronounced at lower gestational ages.
Meaning The findings of this study suggest that preterm birth is associated with increased risk of death from infancy to adulthood.
Abstract
Importance Preterm birth (PTB) is a leading cause of neonatal mortality. However, evidence on mortality beyond the neonatal period is limited, especially in North America.
Objective To examine associations of PTB with all-cause and cause-specific mortality from birth through 23 to 36 years of age.
Design, Setting, and Participants This population-based matched cohort study of live births in Canada included individuals born between January 1, 1983, and December 31, 1996, and followed up until December 31, 2019. Data were analyzed from June 1, 2023, to April 30, 2024.
Exposure PTBs, between 24 and 37 weeks’ gestation (with gestational age [GA]-specific subcategories of 24 to 27 weeks, 28 to 31 weeks, 32 to 33 weeks, and 34 to 36 weeks) compared with term births (37-41 weeks’ gestation).
Main Outcomes and Measures All-cause mortality and cause-specific mortality were the main outcomes. Risk differences (RDs) and risk ratios (RRs) were estimated for all-cause mortality using log-binomial regressions and hazard ratios were estimated for cause-specific mortality using Cox proportional hazards regression models (censoring individuals who died from other causes) within prespecified age intervals (ages 0-11 months and ages 1-5, 6-12, 13-17, 18-28, and 29-36 years). Observed confounding was accounted for using coarsened exact matching on baseline characteristics.
Results Of 4 998 560 births (54.2% male), 6.9% were born preterm (with GA-specific subcategories of 0.3% born at 24-27 weeks, 0.6% at 28-31 weeks, 0.8% at 32-33 weeks, and 5.1% at 34-36 weeks). During a median of 29 years of follow-up, 72 662 individuals died (14 312 born preterm and 58 350 at term). PTB was associated with an increased risk of death in all age intervals, with the highest RDs and RRs from birth through infancy (ages 0-11 months) (RD, 2.29% [95% CI, 2.23%-2.35%]; RR, 11.61 [95% CI, 11.09-12.15]) and in early childhood (ages 1-5 years) (RD, 0.34% [95% CI, 0.31%-0.36%]; RR, 2.79 [95% CI, 2.61-2.98]) and the lowest RDs and RRs among those between ages 18 and 28 years (RD, 0.07% [95% CI, 0.04%-0.10%]; RR, 1.13 [95% CI, 1.07-1.19]). We identified increased risks of mortality associated with several causes, including respiratory, circulatory, and digestive system disorders; nervous system, endocrine, and infectious diseases; cancers; congenital malformations; and conditions originating in the perinatal period. No associations were found for external causes of deaths. Associations by GA categories suggested lower risks with higher GA.
Conclusions and Relevance The findings of this population-based matched cohort study suggest that individuals born preterm were at an increased risk of death from birth until their third and fourth decades of life, with higher risks as GA decreased. Some of these associations may have been partly due to underlying health determinants that affected PTB and mortality. These findings suggest that PTB should be recognized as a risk factor for mortality and could inform preventive strategies.
1Department of Neonatology, University Hospitals Dorset NHS Foundation Trust, Dorset, United Kingdom
2Department of Development and Regeneration, KU Leuven, Leuven, Belgium
3Department of Pharmaceutical and Pharmacological Sciences, KU Leuven, Leuven, Belgium
4Department of Hospital Pharmacy, Erasmus MC, Rotterdam, Netherlands
Introduction
Neonates and infants are commonly referred to as “therapeutic orphans” due to the overall scarcity of therapeutic interventions that have been developed and tailored to their needs and specific characteristics (1, 2). This is well known by care providers and researchers active in this field, but is perhaps less on the radar of authorities, funding bodies or the broader public. There is significant health inequity when comparing newborns to other age populations in terms of specific drug and device development and therapeutics (1, 2). In addition there are health inequities in the provision of neonatal care globally which require special attention in terms of improvement (3).
Bronchopulmonary dysplasia, neonatal seizures, poor growth, necrotizing enterocolitis (NEC) and short bowel, hypoxic-ischemic encephalopathy, retinopathy of prematurity (ROP), neonatal infections and sepsis hereby serve as a non-exhaustive list of “orphan conditions” in need of more equity, through adequately and urgently funded research and improvement.
The good news is that there have been increased efforts, in recent years, by researchers and regulatory bodies to focus on the provision of drugs, devices, and treatment modalities tailored for neonatal use, while further advocacy remains an obvious need (2, 4, 5). This brings perspective and explains the initiative taken to organize a focused research topic on what is on the horizon as well as recent advances.
Overview of the topics covered
We targeted emerging or new aspects related to monitoring, diagnostics and therapeutics in neonatal care for the current research topic. Fortunately, this research topic was perceived as very relevant by the research community, as 135 authors expressed their interest as contributors, resulting in 20 accepted papers. This serves as a signal of the importance to continue to work on this topic.
Post-hoc, and in a somewhat arbitrary way (because of overlap in these subcategories) these papers were subdivided by the editors into different subcategories, with focus on (1, 5 papers) perinatal biomarkers in blood and urine and how these relate to or predict outcomes, (2, 6 papers) adaptations of existing and newly emerging equipment in neonatal units, (3, 3 papers) needed advances in pharmacotherapy, (4, 3 papers) machine learning or deep learning applications in neonatal care, and finally, (5, 3 papers) underreported aspects of contemporary NICU care, with a focus on the holistic nature of care for the infant and the family.
Perinatal biomarkers in blood and urine and how these relate to or predict outcomes
Two papers focused on biomarkers related to gestational diabetes, with reflections and data on maternal and neonatal outcomes. Postnatal maternal levels of glycated albumin and hemoglobin A1c in mothers of large-for-gestational-age (LGA) informed us of the relevance of accurate diagnosis during pregnancy. This is because postpartum women without diagnosis during pregnancy had higher glycated albumin values, associated with LGA and associated complications (Železnik et al.). Interestingly and related to this paper, Yin et al. reported on a untargeted metabolomics study in women with gestational diabetes, with the recommendation of a maternal serum metabolite panel to forecast neonatal adverse outcomes (hypoglycemia and macrosomia) (Yin et al.).
Other papers focused on the use of vitamin D, acid-base and biomarkers associated with fetal growth restriction with impaired neurodevelopmental outcome. In a cohort of 217 preterm neonates, a multivariate regression analysis identified antenatal steroids as protective, and lower birth weight, duration of ventilation, sepsis and the serum 25-(OH)D vitamin as risk factors to develop ROP (Yin et al.). Musco et al. reported on a systematic review on blood biomarkers indicating risks of adverse neurodevelopmental outcome in fetal growth restricted infants (Musco et al.). While the authors retrieved some data on neuron specific enolase and S100B, the overall conclusions reflect a call for further research. Finally, an association between lactate levels in umbilical cord blood and cerebral oxygenation in preterm neonates was studied as a secondary outcome analysis (Dusleag et al.). In non-asphyxiated preterm neonates with respiratory support, lactate levels were negatively associated with cerebral and arterial oxygenation. In term neonates without respiratory support, no associations were observed.
Adaptations of existing and newly emerging equipment in our units
In a review on emerging innovations in neonatal monitoring, Krbec et al. concluded that there is an urgent, still unmet need to develop wireless, non- or minimal-contact, non-adhesive technology, capable to integrate multiple signals in a single platform, tailored to neonates (Krbec et al.). Related to this call of action, Svoboda et al. reported on their pilot experience with contactless assessment of heart rate, applying imaging photoplethysmography (Svoboda et al.). Rectal and axillary temperature monitoring on admission were compared in a cohort of preterm (n = 80, <32 weeks gestational age) by Halabi et al., reporting that rectal measurement was likely more reliable in the event of hypothermia (Halabi et al.). Ultrasound-guided measurement of anterior cerebral artery resistive index in the first week of life in 739 preterm neonates (<35 weeks) was not associated with subsequent co-morbidities on admission or during neonatal stay (asphyxia, sepsis, NEC) (Singh Gill et al.). A case series of neurally adjusted ventilatory assist to rescue pulmonary interstitial emphysema in 5 extremely low birth weight infants illustrated the potential value of this ventilatory equipment and strategy and need for further study (Chen et al.). Finally, van Rens et al. compared a conventional to a modified Seldinger technique (a dedicated micro-insertion kit) for peripherally inserted central catheter (PICC) placement, illustrating the relevance of developing “low risk, high benefit” type of medical devices, adapted to the specific needs of neonates (van Rens et al.).
Advances needed in pharmacotherapy
The currently available medicines and dosing regimens in neonatal care are limited and there is an urgent need for improvement in this domain. This was illustrated by articles on sepsis, septic shock and steroids. Inequity in provision of neonatal care across the globe ought to be a major focus of improvement. Gezahegn et al. described the outcome in neonates admitted with sepsis in Harar (Ethiopia). Low white blood cell count, desaturation, preterm birth, absence of prenatal maternal care, and chorioamnionitis were important risk factors for sepsis-related mortality (Gezahegn et al.). Addressing these prognostic factors hold the promise to act as levelers to improve outcomes. A pilot study compared noradrenaline and adrenaline as first line vasopressor for fluid-refractory sepsis shock (Garegrat et al.). Both interventions were comparable to resolve the septic shock, while the overall mortality (13/42, 30%) remained significant, highlighting the need for better diagnostic and therapeutic options. Finally, in a systematic review, outcome of postnatal systemic corticosteroids (hydrocortisone to dexamethasone) were compared as reported in randomized controlled trials (Boscarino et al.). The authors concluded that dexamethasone appeared to be somewhat more effective than hydrocortisone in improving respiratory outcomes, but with inconclusive but relevant concerns on the uncertainties on long-term neurodevelopmental outcome, again highlighting the need for better therapies for prevention and management of chronic lung disease of prematurity.
Machine learning or deep learning applications in neonatal care
Artificial intelligence is a rapidly advancing area with fast evolving clinical applications in healthcare, including in the NICU (6). It is no surprise that the current research topic also contains papers illustrating its relevance to improve our practices and outcomes. Two papers hereby focused on NEC, and a 3rd paper on prediction of significant patent ductus arteriosus (PDA). In a mini-review, Cuna et al. reports on the various pathophysiological processes underlying NEC endotypes, and how artificial intelligence holds the promise to influence further understanding and management (Cuna et al.). An approach to enhance surgical decision making in NEC is illustrated by Wu et al. Based on x-rays from 263 neonates diagnosed with NEC (94 surgical cases), a binary diagnostic tool was trained and validated, with Resnet18 as approach applied (Wu et al.). For PDA, an ultrasound-based assessment of ductus arteriosus intimal thickness in the first 24 h after birth was applied in 105 preterm neonates. A prediction model for closure on day 7 included birth weight, mechanical ventilation, left ventricular end-diastolic diameter, and PDA intimal thickness (Hu et al.). Such models can be considered to better target future study, integrated in a precision medicine approach. Use of AI and big data have the potential to significantly improve our understanding of neonatal conditions and also support neonatal researchers in asking better research questions.
Underreported aspects of contemporary NICU care, holistic care
As part of this research topic, we also accepted papers reporting on the use of music on pain management, on multisensory stimulation to improve maternal milk volume production, and parents’ experiences related to congenital cardiac surgery. All these 3 papers reflect the need for holistic care and to further integrate the perspectives of (former) patients and parents into neonatal practice.
In a systematic review, Ou et al. demonstrated that music is an effective intervention to relief procedural pain (e.g., Premature Infant Pain Profile score) in preterm neonates, as it reduced some markers of stress, and improved blood oxygen saturation (Ou et al.). Multisensory stimulation (audiovisual, or audiovisual + olfactory) compared to a control setting improved maternal milk volume production, with evidence of positive effects of both interventions, even more pronounced if both interventions are combined (Cuya et al.). Finally, a quantitative analysis of parent’s experiences with neonates admitted to NICU with a congenital heart disease reinformed us on the importance of actively focusing on parental experiences of care (Catapano et al.).
From advances in neonatal care to implementation
In our opinion, this research topic nicely illustrates the diversity in ongoing clinical research activities, that all hold the promise to improve our clinical management practices, with the overarching aim to improve neonatal outcomes. There is an urgent need to focus on the current health inequities in the provision of care to neonates (3). The trend towards a “neuro” dedicated NICU care is an illustration on how relevant progress may occur. This progress is based on improved neuromonitoring techniques (7), improved management and precision medicine in the field of anti-epileptic drugs (8), and integrating families as partners in neonatal neuro-critical care and similar improvement programs (9). The good news is that we are already experiencing a shift in the right direction. The neonatal community and all other relevant stakeholders need to work better together to improve the pace and scale of this improvement.
Improvement Project to Reduce Uncontrolled Pain and Improve Staff Satisfaction
Sprecher, Alicia MD; Roeloffs, Kimberly NNP; Czarnecki, Michelle L. APN; Labovsky, Kristen MD; Kissell, Anna PharmD; Hornung, Genesee MSN, RN; Uhing, Michael MD Editor(s): Dudding, Katherine PhD, RN, RNC-NIC, CNE; Nist, Marliese D. PhD, RNC, Section Editors Advances in Neonatal Care 25(1):p 18-27, February 2025. | DOI: 10.1097/ANC.0000000000001234
Abstract
Background:
Postoperative pain management in the neonatal period is an area of high variability and a source of staff dissatisfaction. Pain management is a key component of high-quality care; however, pain assessment in infants is difficult and analgesics can negatively impact the developing brain.
Purpose:
We aimed to improve postoperative pain control for infants in our neonatal intensive care unit (NICU), limit variability in the approach to pain management, and increase staff satisfaction.
Methods:
This project was completed between April 2019 and March 2022 with sustainment tracked through December 2023. Interventions took place in a 70-bed level IV NICU using quality improvement methodology. Interventions included efforts aimed at improving pain assessment as well as development and implementation of a pain management guideline. Outcome measures included frequency of uncontrolled postoperative pain and measures of staff satisfaction. Process measures included compliance with pain assessment cadence and guideline recommendations. Opioid exposure within 24 hours of surgery was included as a balancing measure.
Results:
Pain management was assessed in 811 infants: 392 prior to guideline implementation, 273 during implementation, and 146 during sustainment period. Uncontrolled postoperative pain decreased from 26% pre-implementation to 18% post implementation and into the sustainment period. Staff satisfaction improved from 67% to 83%. These improvements were associated with decreased variability in postoperative pain management and a decrease in postoperative opioid exposure.
Implications for Practice and Research:
The use of a postoperative pain management guideline can improve pain control, decrease drug regimen variability, decrease opioid exposure, and increase staff satisfaction.
In Singapore, where skyscrapers rise and medicine meets innovation, a new kind of wellness journey is unfolding—one led by the smallest among us.
Our Womb Warriors who began life in the NICU are not just survivors—they are thrivers, growing through challenges and emerging with strength forged in the most fragile beginnings. Today, health and wellness for these preemie survivors extends far beyond the hospital walls. It means developmental follow-up, skin-to-skin care, nutrition support, and emotional well-being—not just survival, but quality of life.
Singapore’s approach is inspiring. With personalized risk assessments, neurodevelopmental care programs, and parent-empowering tools like kangaroo care, the wellness journey begins from day one. And studies now confirm what many NICU parents already knew in their hearts: the closeness, love, and presence of family are as powerful as any machine.
As our Warriors grow, their wellness becomes more than a checklist—it becomes a rhythm. Physical therapy. Play. Sensory exploration. Nourishment. Love. And for the parents walking beside them? Wellness looks like deep breaths, long walks, and the quiet courage to ask for help.
Whether your little one is a few months or a few years out of the NICU, this season is a reminder: wellness isn’t a destination—it’s a daily act of love.
Spring into Strength
Spring is a season of becoming—of blooming boldly, stretching softly toward the light, and waking up to what’s possible. For our Womb Warriors, it’s also a reminder that wellness is not about perfection—it’s about progress, presence, and power.
Whether you’re a preemie kid discovering new abilities, a teen navigating your story, or an adult survivor reclaiming your narrative, this season invites you to grow on your terms. Your early beginnings may have been fragile—but your spirit is anything but.
Health and wellness don’t have to look the same for everyone. What matters most is listening to your body, honoring your journey, and celebrating how far you’ve come.
🌸For Kids
Make movement magical—build obstacle courses, splash in puddles, or stretch like your favorite animal.
Explore foods that help you grow strong: yogurt parfaits, rainbow fruit plates, or protein-packed pancakes.
Practice deep breathing with bubbles or belly-breathing “dragon breaths.”
🌱For Teens
Journal your thoughts under a tree or start a mood-boosting playlist for mental clarity.
Try out yoga, trail walks, or a new sport—your strength isn’t defined by speed, but by showing up.
Fuel yourself with purpose: balanced snacks, hydration, and sleep that heals.
🌞For Adults
Redefine strength: maybe it’s finishing a workout, setting boundaries, or resting when you need to.
Revisit your NICU beginnings—use them to empower your healthcare choices and connect with your past.
Create a spring ritual: a morning stretch, a quiet walk, or a personal mantra. Wellness isn’t trendy—it’s transformative.
In Singapore, hospitals are leading the way in early screenings and personalized care to help preemies not just survive, but thrive. That same spirit of innovation and renewal lives in each of us.
So here’s to you—this spring, let’s grow wildly. Heal gently. Thrive loudly. Because once a Neonatal Womb Warrior, always a Warrior—and you are in full bloom.
The Path to Wellness | Alysha Aziz | TEDxHolyTrinitySchool
Wellness is a journey. In this insightful talk, learn about the PATH model: Perception, Analysis, Trial and Error, and Habits, as a framework for achieving personal well-being. This talk empowers audiences to embrace the process and find a path to a healthier, more fulfilling life. Hi everyone, I’m Alysha! I am a student in grade 11 and I’m one of the speakers for TEDEd’s Empowerment event. Having been part of the club since grade 9 and now as president, I’m really excited to share my talk with everyone! I’ll be talking about wellness and taking autonomy over your own mental health. I’m super excited that this is our first charitable event and can’t wait to see you all there!
10-minute guided meditation for kids 🧘 mindfulness for kids 🕊 Bye Bye Worry Balloons🎈 Worry-Free 💛
Relax, breathe, and feel calm with this simple meditation for kids. In this guided meditation for kids, we’ll say ‘bye-bye’ to worries and hello to happy thoughts. ☀️🎈
Would You Rather? Spring Edition! | Fun Fitness For Kids | This or That | Spring Workout | GoNoodle
Mr. Hassell’s Brain Breaks
Exercise your body and mind with this Spring themed brain break! In this fun and engaging workout video, we play a game of “Would You Rather” by picking our favorite Spring choices and performing exercises!! Perfect for a PE warmup, classroom brain break and at home workout!
Written by published children’s author, Jennifer Marino Walters, “Surprising Spring” tells the simple story of the beauty that Spring brings and its many flowering surprises.
Wave House Sentosa located on the sandy beaches of Sentosa is Asia’s only installation in an archipelago of global Wave Houses that stretches from Durban in South Africa, San Diego in California, Santiago in Chile, and Mallorca in Spain. Singapore has long been a crossroads for surfers seeking the perfect waves at beaches around Southeast Asia, however the island itself lacks the giant waves which surfers long for. With its opening, Wave House Sentosa puts Singapore on the global surfer destination map with its perfect and world famous 10′ FlowBarrel wave.
Slovakia, officially the Slovak Republic, is a landlocked country in Central Europe. It is bordered by Poland to the north, Ukraine to the east, Hungary to the south, Austria to the west, and the Czech Republic to the northwest. Slovakia’s mostly mountainous territory spans about 49,000 km (19,000 sq mi), hosting a population exceeding 5.4 million. The capital and largest city is Bratislava, while the second largest city is Košice.
Healthcare in Slovakia has features of the Bismarck, the Beveridge and the National health insurance systems. It has public health system paid largely from taxation. The cost of national health insurance is shared between the employees and the employers. The part of these taxes are paid by the employees as a deduction from theirs wages and the remaining part of these taxes is paid as compulsory contribution by employers. Sole traders pay the full amount of these taxes.
These taxes are managed by health insurance companies. Current healthcare system has 3 health insurance companies, namely Union (12,4%), Dôvera (32,4%) and Všeobecná zdravotná poisťovňa (55,2%)(market share). Všeobecná zdravotná poisťovňa is a state-run insurance company, the other two are private. These insurance companies have contracts with outpatient clinics, hospitals, rehabilitation centres, pharmacies, etc. Despite this, not everywhere and not always the insurance company covers the costs. The costs are not covered for all medicines, or the full price of them. Also, it is not covered dental treatment.
The government pays health insurance for children, students, pensioners, invalids, people performing activities for a church, religious or charitable community, etc.
CR’s experts say it’s much safer for children to wear their winter coat backward and on top of their car seat harness.
“You better bundle that baby up or she’s going to catch a cold!” I knew before I turned around what was happening: The well-meaning lady in the grocery store parking lot wanted to know why my child didn’t have a coat on in her car seat, even though it was the middle of winter.
The reason? Because a bulky coat and a child car seat can be a dangerous combination. As a general rule, winter coats should not be worn underneath a car seat harness because that can leave the harness too loose to be effective in a crash.
Research priorities for preterm lung health research across the lifespan: a community priority setting partnership
Author affiliations – Naomi R Hemy1 Amber Bates1 Belinda Frank2 Anne McKenzie2 Shannon J Simpson1 3
Abstract
Background It is essential to embed patient and public perspectives into every stage of the research journey, including setting the future research agenda. The substantial gaps in our understanding of prematurity-associated lung disease presented a timely opportunity to determine the community’s research priorities.
Objective To conduct a priority setting partnership (PSP) to determine the top 10 research priorities for preterm lung health.
Design We undertook a modified James Lind Alliance methodology comprising three main stages: (1) an idea generating survey with open questions to ascertain the community’s most important ideas for future preterm lung health research, (2) prioritisation survey to distill the main themes into a shortlist of 20 and (3) consensus workshop where participants were tasked with ranking their final top 10. This PSP is reflective of the view of preterm-born individuals, parents of preterm children and healthcare professionals in an Australian healthcare setting.
Results We collated 144 submissions from the idea generating survey from which 27 prioritisation themes were developed. From the 150 prioritisation survey responses, the 20 themes receiving the most votes were taken to the consensus workshop. Participants identified the following top 10: (1) lifelong impacts; (2) interventions, treatments or supports; (3) ongoing lung health follow-up; (4) diagnostic tools, resources and education for primary healthcare providers; (5) resources to inform and empower families; (6) relationship to physical health and developmental issues; (7) preventing and/or treating lung infections; (8) additional supports, resources and research for minority groups; (9) impact on mental well-being; and (10) likelihood of asthma diagnosis.
Conclusion Priorities identified through the PSP will be invaluable in informing future research into prematurity-associated lung disease.
Following important research in neonatology / newborn medicine from around the world
I have written frequently about my concerns with “NDI” as an important measure of neonatal outcomes, indeed, it seems to be often thought of as if it were the only important measure. It has very often been included as part of a composite outcome measure “death or NDI”.
So why am I disturbed about the use of NDI as a primary outcome measure? NDI is itself already a composite measurement, including some indicator of delayed development (most commonly one of the various iterations of the Bayley Scales of Infant Development), some severity of motor disorder expected to be permanent, i.e. Cerebral Palsy, some severity of hearing loss, and some severity of visual impairment. It was a composite invented by neonatologists and follow up specialists as a way of trying to quantify the impacts of adverse cerebral impacts of prematurity. There are many problems with this, both in the actual importance of each component of NDI, and also in the permanence of the finding. For example, most infants with low scores on developmental screening tests at 2 years do not have intellectual impairment at follow up. In the follow up of the CAP trial, for example, only 18% of babies who had a low Bayley score at 18 months (version 2 MDI <70) actually had a low IQ at 5 years (WPSII <70). This is unlike CP, for which a diagnosis at 2 years is very accurate (not 100%, but appears to be about 95% PPV) as a predictor of long term motor dysfunction, but the severity of the problem can vary, especially after a diagnosis at 2 to 3 years, where about 1/3 of infants will change their classification on the GMFCS, either to a higher or a lower score. Visual and auditory impairments seem to be more permanent and invariable, but are a much smaller part of the NDI.
And, of course, combining NDI with death as part of a composite outcome implies that they are equally important, and means that an intervention which decreases death may not be found to be significant is there is an increase in low BSID scores in the survivors (for example).
Do parents of babies who are labelled as having NDI think that their infants are impaired? That is the question asked in a new publication from the follow up centres across Canada (Canadian Neonatal Follow-Up Network, CNFUN). Richter LL, et al. Parental and Medical Classification of Neurodevelopment in Children Born Preterm. Pediatrics. 2025. Over 1000 very preterm infants are involved in the study, and their parents were asked if they thought that their child had a developmental impairment when they attended a follow-up clinic appointment, but before they completed the standardised evaluation. They then had their evaluation and were classified as having no NDI or :
“to have a mild-moderate NDI if they had any 1 or more of the following: CP with GMFCS 1 or 2; Bayley-III motor, cognitive, or language composite scores 70 to 84; hearing loss without requirement for hearing devices or unilateral visual impairment. A child was considered to have a severe NDI if they had any 1 or more of the following: CP with GMFCS 3, 4, or 5; Bayley-III motor, cognitive or language composite scores <70; hearing aid or cochlear implant; or bilateral visual impairment.”
As this table shows, there was poor agreement between what the parents thought, and what the standardised evaluation stated. Most of the disagreements were parents considering their infants to not be impaired, or to be less impaired than the standard classification. There were 185 infants with “severe NDI” according to the definition above, only 23 parents thought their child was severely impaired, in contrast, among the 596 with no NDI, there were 11 parents who found their child to have severe impairment, and 104 thought they had mild-moderate impairment.
Some of the details of the analyses are quite interesting, for example, the small number of infants with serious CP, GMFCS 4 or 5, were mostly considered to have moderate or severe impairment by parents. The cognitive scores of infants who agreed that their infant, with CNFUN defined severe NDI, had at least moderate impairment were lower (median 70) than those who disagreed (median 80).
Many problems faced by families with ex-preterm infants are not captured by “NDI”. This is reflected, I think, by those parents who thought their child was impaired despite not satisfying CNFUN definitions, such infants were much more likely to be using technology at home, and more likely to have been referred for occupational therapy, or to see a psychologist or other therapist. Needing re-hospitalisation also made parent more likely to agree that their infant had an impairment.
Because we haven’t measured some of the things that impact families, such as behavioural disturbances, feeding problems, and sleep disruption, we really don’t know if they are affected by any of our NICU interventions. It wouldn’t surprise me if some interventions, ranging from postnatal steroids to skin-to-skin care or light cycling, might have major impacts on those outcomes. We just don’t know.
What should we do about findings such as these newly published data, and others from the Parents’ Voices project? Defining a single ‘yes or no’ outcome variable is the old-fashioned way of designing research and determining the benefit of an intervention. There are much better ways of comparing outcomes between groups, ways which can take into account the variety of outcomes, and the preferences of parents. It takes some extra work to define the kind of ordinal outcomes which reflect the values of parents and the relative importance of each component, but that is hugely preferable to using composite outcomes which implicitly value each component as being equivalent. Being dead, having a Bayley Cognitive composite of 69, having severe visual loss all qualify as “dead or severe NDI”, but the implications are enormously different.
In the future outcomes we measure should focus on how infants function, and should recognize that the answer to the question “how is your child doing?” is not a dichotomous choice.
Appropriate protein intake is crucial for growth and development in children born preterm. We assessed the effects of high (HP) versus low protein (LP) intake on neurodevelopment, growth, and biochemical anomalies in these children.
Methods
Randomised and quasi-randomised trials providing protein to children born preterm (<37 completed weeks of gestation) were searched following PRISMA guideline in three databases and four registers (PROSPERO registration CRD42022325659). Random-effects model was used for assessing the effects of HP (≥3.5 g/kg/d) vs. LP (<3.5 g/kg/d).
Results
Data from forty-four studies (n = 5338) showed HP might slightly reduce the chance of survival without neurodisability at ≥12 months (four studies, 1109 children, relative risk [RR] 0.95 [95% CI 0.90, 1.01]; P = 0.13; low certainty evidence) and might increase risk of cognitive impairment at toddler age (two studies; 436 children; RR 1.36 [0.89, 2.09]; P = 0.16; low certainty evidence). At discharge or 36 weeks, HP intake might result in higher weight and greater head circumference z-scores. HP intake probably increased the risk of hypophosphatemia, hypercalcemia, refeeding syndrome and high blood urea, but reduced risk of hyperglycaemia.
Conclusions
HP intake for children born preterm may be harmful for neonatal metabolism and later neurodisability and has few short-term benefits for growth.
Impact statement
Planned high protein intake after birth for infants born preterm might be harmful for survival, neurodisability and metabolism during infancy and did not improve growth after the neonatal period.
Protein intake ≥3.5 g/kg/d should not be recommended for children born preterm.
Conclusion (Full Study)
Planned high protein intake in the first weeks after preterm birth had few benefits and may be harmful for survival, neurodisability and biochemical abnormalities in neonatal care. However, there are few data beyond the toddler period and considerable unexplained heterogeneity. Longer-term follow-up and an individual participant data meta-analysis of existing trials, including data on total energy intake, would be helpful to clarify the effects of high protein intake for children born preterm.
Personalized communication with parents of children born at less than 25 weeks: Moving from doctor-driven to parent-personalized discussions
Marlyse F. Haward a, Antoine Payot bc, Chris Feudtner de, Annie Janvier bc
Abstract
Communication with parents is an essential component of neonatal care. For extremely preterm infants born at less than 25 weeks, this process is complicated by the substantial risk of mortality or major morbidity. For some babies with specific prognostic factors, the majority die. Although many of these deaths occur after admission to the intensive care unit, position statements have focused on communication during the prenatal consultation. This review takes a more comprehensive approach and covers personalized and parent-centered communication in the clinical setting during three distinct yet inter-related phases: the antenatal consultation, the neonatal intensive care hospitalization, and the dying process (when this happens). We advocate that a ‘one-size-fits-all’ communication model focused on standardizing information does not lead to partnerships. It is possible to standardize personalized approaches that recognize and adapt to parental heterogeneity. This can help clinicians and parents build effective partnerships of trust and affective support to engage in personalized decision-making. These practices begin with self-reflection on the part of the clinician and continue with practical frameworks and stepwise approaches supporting personalization and parent-centered communication.
Section snippets
Part 1: Antenatal consultation
Current recommendations for the antenatal consultation focus on equalizing knowledge imbalances by providing parents with physician-derived sets of information to facilitate rational, data-driven choices.14 These information sets span short and long-term morbidities, survival and mortality statistics determined by physicians, with little input from parents. Although recommendationssuggest exploring values, they fall short in acknowledging the ‘process’ of relationship building.
Part 2. Communication during the neonatal hospitalization
Parent-centered communications during neonatal hospitalizations follows similar concepts. This section will add how continuity of care and ‘good parenting beliefs’ can help manage uncertainty, hope, and realism. We will consider the case of Ms. Gladwell.
Part 3. Dealing with death: the importance of a stepwise approach
Generally, for babies born at less than 25 weeks, neonatal death occurs relatively early when the infant does not respond to interventions, often within the first 3 days of life for the most immature babies.84 Other babies die when respiratory support is removed after death is judged inevatable, or for quality of life concerns.15 For parents like Ms. Gladwell, when death is not immediate, time permits knowledge to be acquired and values to be clarified influencing how choices are interpreted.
Conclusion
Parents and families will live with these experiences for the rest of their lives. How they remember the communication process and care their infants received depends on their perceptions of the relationships built with clinicians and their ability to ‘justify’ what happened within the context of their values. Behaviors that make them feel disrespected or their infant not valued can leave lasting impressions, whereas trusting partnerships solidifies their roles as parents.
Here’s another video in our Journey Through Medicine series where we talk about what it was like for us to have a child while both completing our medical residencies. There’s never a perfect time to have a child during medical training, but here’s how we made it work. #medicalschool#residency#doctorcouple
Neuroprotective therapies in the NICU in preterm infants: present and future
Nature–Neonatal Neurocritical Care Series – 19 December 2023
Abstract
The survival of preterm infants has steadily improved thanks to advances in perinatal and neonatal intensive clinical care. The focus is now on finding ways to improve morbidities, especially neurological outcomes. Although antenatal steroids and magnesium for preterm infants have become routine therapies, studies have mainly demonstrated short-term benefits for antenatal steroid therapy but limited evidence for impact on long-term neurodevelopmental outcomes. Further advances in neuroprotective and neurorestorative therapies, improved neuromonitoring modalities to optimize recruitment in trials, and improved biomarkers to assess the response to treatment are essential. Among the most promising agents, multipotential stem cells, immunomodulation, and anti-inflammatory therapies can improve neural outcomes in preclinical studies and are the subject of considerable ongoing research. In the meantime, bundles of care protecting and nurturing the brain in the neonatal intensive care unit and beyond should be widely implemented in an effort to limit injury and promote neuroplasticity.
Impact
With improved survival of preterm infants due to improved antenatal and neonatal care, our focus must now be to improve long-term neurological and neurodevelopmental outcomes.
This review details the multifactorial pathogenesis of preterm brain injury and neuroprotective strategies in use at present, including antenatal care, seizure management and non-pharmacological NICU care.
We discuss treatment strategies that are being evaluated as potential interventions to improve the neurodevelopmental outcomes of infants born prematurely.
Compassionate Inquiry is a psychotherapeutic method developed by Dr. Gabor Maté that reveals what lies beneath the appearance we present to the world. Using Compassionate Inquiry, the therapist unveils the level of consciousness, mental climate, hidden assumptions, implicit memories and body states that form the real message that words both express and conceal.
PREEMIE FAMILY PARTNERS
Your friend or family has finally brought their preemie baby home from the NICU, and you’re excited to meet their little miracle, but unsure of how to approach the family altogether.
Don’t worry, as long as you stick to these simple do’s and don’ts written by a preemie mom, visiting a premature baby will be a happy and smooth time for everyone!
Do Listen to the Preemie Parents’ Conditions (and Comply)
Before visiting a premature baby, ask the parents if they are ready to receive visits in their home. And under which terms.
Don’t miss out!
You know the drill, if you want to be part of Preemie Mom Tip’s email list, subscribe below! You’ll receive weekly emails that will help you on your journey. We are preparing a new and improved FREE resource library, sign up and be the first to know once it’s ready!
Top of Form
It’s not uncommon that when we take our babies home, the doctors impose a no visit rule until we can complete the first vaccination schemes (which more often than not include at least three shots of the Synagis shot.) The complete process can take up to three months.
We didn’t allow almost any visit from friends or family until my son was around four months old (2 months old adjusted), some of our friends were understanding, and some weren’t.
We knew that we were doing what was best for our son, so we stuck to it!
If your friend says it’s OK to visit their baby, find out if they have any special request for your visit.
Some of the petitions may seem weird but know that they come from a very real place (the NICU), and visiting a premature baby during her first months is much like visiting babies in the NICU: short and strict.
Some parents may ask you to keep your cell phones at the entrance of the house (phones are full of germs), wash your hands for five minutes, visit straight from home, or tie your hair, take a shower just before visiting, or wear a surgical face mask. Whatever it is, by doing as they say you’ll help protect their baby and their peace of mind.
Do Bring Extra Clean Clothes for Interacting with the Preemie Baby
This is especially true if you are visiting a premature baby after being all day outside of your home.
The street is full of germs and contamination, and we preemie parents tend to develop a germ-vision.
By bringing freshly laundered clothes and changing into them as soon as you arrive at the house you are visiting you will show them that you are on their side, and support their every measure to keep their baby safe.
It is even more likely that they will let you hold the baby if you do this since she won’t be directly exposed to dirty clothes.
Do: Wash your Hands as Soon as you Enter, Wash your hands thoroughly.
Make sure you wash the space between your fingers, your palm, and the back of your hand.
Even so, many of us neglect this standard practice.
When a baby is in the NICU, the nurses teach us parents about the importance of hand-washing, the correct techniques to do so, the right moment to do it. We wash our hands so frequently that we get rashes most of the time (since the NICU soap is strong.)
It is second nature to us to wash our hands when visiting babies!
Having said all this, once our babies are bigger and stronger, we’ll be a bit laxer about this. After all, germs do help develop the immune system, we just don’t want to expose our miracles before they are ready for this!
Do Keep the Visit Short and Simple
There will be time for the lengthy visits that you may be dreaming about. In the months and years to come, you’ll be able to kiss and smooch the baby to your heart’s content, and stay during weekends, afternoons, and evenings!
But right now, the preemie family may be in need of some alone time. And though seeing you will surely help them, keep your visit under 30 minutes if possible.
Most breastfeeding moms need time adjusting to… well…breastfeeding, but this is especially the case of us preemie moms. We came from pumping our way in the NICU to actually breastfeeding a baby. That transition takes time to get used to.
Additionally, like all new parents, we are most likely to be sleep-deprived. Partly because our babies wake us up all night and partly because of the monitors beeping or ourselves waking up to check that the babies are doing fine.
Keeping a short visit is a long time investment in your relationship with NICU families.
Don’t Go if You’re Not Feeling Well
If your head hurts, your throat is sore or your nose itches, reprogram your visit.
Even if you are feeling well but visited someone who has had the flu within seven days before your visit you may be carrying the virus, so it’s also best to reprogram.
RSV and pulmonary infections are dangerous for preemies.
Ollie had simple flu when he was 12 months old and turned into pneumonia and bronchiolitis in less than 24 hours. We had to rush him to the ER because he wasn’t breathing. He was in the hospital on oxygen for ten days until he recovered. The younger the baby, the higher the risk of infection.
We limited our visits to non-flu visitors until Ollie was well over 8 months. And, we still ask everyone who may be sick to wear a facemask. We don’t overprotect our son, he goes to crowded places and has had the flu several times by now at 24 months. But we still don’t want to risk it by letting someone with the flu hold him without wearing a facemask.
Don’t Hold the Preemie Baby
Unless the parents ask you to hold their baby, don’t press them into it.
You’ll have plenty of opportunities. Just make them feel comfortable by knowing that you are OK just looking at the baby. If they are comfortable with you holding her, they will let you know.
Also, to keep on the safe side, avoid kissing the baby and holding her hands.
Don’t Compare their Preemie to any Other Baby
As preemie parents, the greatest joy in the world comes with sorrow.
We love our baby and wouldn’t change him for anyone else, nor would we want him to be any different. So we try not to compare our baby to anyone else’s. But, sometimes it is inevitable, and we internally cave in.
My son looked like a newborn during his first four months. He didn’t smile until he was eight months old and had to go through weekly Physical Therapy to move his hands and arms. He is healthy, bright, and has no significant delay. But when the children of my friends were smiling, walking, and talking, he wasn’t, and it’s human nature to worry and to compare them.
It gets even worse when people pity my boy or openly compare him to others. It feels as if they are undermining us as if they don’t know or don’t care about our background.
A few months ago a fellow mom who has a son two months younger than Ollie (but bigger and heavier), raved on and on about how small and fragile my Ollie was. She held him without my permission and said that she remembered the times when her son was smaller. She went as far as to congratulate me for being so chill and not overprotecting him. He was evidently so weak (to her eyes.) She seemed to be following an anti-manual for visiting a premature baby.
Needless to say, I despised every second we spent together, and I’ve never seen her again.
Don’t Talk about other Full-Time Pregnancies
Us moms also grieve about the weeks that we should have been heavily pregnant and weren’t.
Sometimes I see other moms complaining about their heavy wombs. Begging for their babies to come early so that they can stop being feeling uncomfortable. I understand that they don’t know what they are saying, but it hurts.
My son was born at 31 weeks, which means that I missed out on nine weeks of pregnancy. Some women dream about their pregnancies their whole lives. They imagine them picture perfect, so we miss what we didn’t have. And in some cases, what we’ll never have.
So it’s better to play it safe and stay clear of that topic.
That’s a Wrap
I’m sure you’ll love visiting a premature baby. Take it one step at a time and be patient with us preemie parents. We do want what’s best for our children, even if sometimes it is hard to express ourselves.
Most of all, you’ll see how powerful and miraculous a person can be, no matter how small!
Have you visited a preemie recently? Are you planning a preemie visit? Or, are you a preemie parent and would like people to know how to plan their visits? Tell us all about it in the comment section!
Empathy — the capacity to identify others’ needs and emotions, and to provide supportive care that meets those needs.
Our recent research shows that parents who express empathy toward their teenagers may give teens a head start in developing the skill themselves. In addition, adolescents who show empathy and support toward their friends are more likely to become supportive parents, which may foster empathy in their own offspring.
Starting in 1998, teens came to the university every year with their parents and closest friend, and a team of researchers recorded videos of their conversations. Researchers observed how much empathy the mother showed to her 13-year-old when her teen needed help with a problem. We measured empathy by rating how present and engaged mothers were in the conversation, whether they had an accurate understanding of their teen’s problem, and how much help and emotional support they offered.
Then, each year until teens were 19 years old, we observed whether teens showed those same types of empathic behaviors toward their close friends.
A decade later, when some of those same teens were starting to have children of their own, we surveyed them about their own parenting. We also asked them about their young children’s empathy. For example, parents rated how often their child “tries to understand how others feel” and “tries to comfort others.”
We found that the more empathic a mother was toward her teenager at age 13, the more empathic the teen was toward their close friends across the adolescent years. Among teens who later had kids themselves, the ones who had shown more empathy for close friends as adolescents became more supportive parents as adults. In turn, these parents’ supportive responses to their children’s distress were associated with reports of their young children’s empathy.
Why it matters
The ability to empathize with other people in adolescence is a critical skill for maintaining good relationships, resolving conflict, preventing violent crime and having good communication skills and more satisfying relationships as an adult.
Adults want teens to develop good social skills and moral character, but simply telling them to be kind doesn’t always work.
Our findings suggest that if parents hope to raise empathic teens, it may be helpful to give them firsthand experiences of being understood and supported.
But teens also need opportunities to practice and refine these skills with their peers. Adolescent friendships may be an essential “training ground” for teens to learn social skills such as empathy, how to respond effectively to other people’s suffering, and supportive caregiving abilities that they can put to use as parents. Our lab’s most recent paper presents some of the first evidence that having supportive teenage friendships matters for future parenting.
What’s next
We’re continuing to follow these participants to understand how their experiences with parents and peers during adolescence might play a role in how the next generation develops.
We’re also curious to understand what factors might interrupt intergenerational cycles of low empathy, aggression and harsh parenting. For example, it’s possible that having supportive friends could compensate for a lack of empathy experienced from one’s family.
While it’s true that you can’t choose your family, you can choose your friends. Empowering teens to choose friendships characterized by mutual understanding and support could have long-term ripple effects for the next generation.
*We checked to confirm these organizations are still active in February, 2025.There was only one resource we were unable to locate. We have also attached the website links!
12 Preemie Support Groups For New Parents, Because You Can’t Go It Alone
It really does take a village for preemie parents by Kinsey Gidick Nov.24, 2020
Only the parents of a premature baby can understand the emotional toll it takes to care for such a fragile child. That’s why finding a community of parents and caretakers who have been through similar circumstances is so important. Fortunately, there are many online resources for parents experiencing the challenge of navigating the NICU and raising a premature baby, from preemie support groups to virtual counseling sessions to even social media accounts.
While each is different, the focus is the same: to provide a space where preemie parents can bring their worries, wins, and concerns to each other and get help and feedback from those going through the same situations. 380,000 babies are born before 37 weeks gestation each year in the U.S. per March of Dimes — that’s 1 out of every 10 American babies. That’s a lot of babies receiving extensive medical intervention including respiratory support, invasive treatments, and extended Neonatal Intensive Care Unit stays. In many cases, these spaces are like lifelines for parents who are afraid of not only the unknown, but the known as well.
Rather than shoulder that burden alone, preemie support groups offer all kinds of resources from chat rooms to virtual mentors, podcasts to classes. It’s the kind of care one won’t often find in a clinic or hospital — ongoing assistance a preemie parent can turn to whether a child is 3 weeks or 3 years old.
1. A space for NICU transition support
Graham’s Foundation, a not-for-profit support group based in Ohio, was founded with a mission that no one should experience prematurity alone. To that end, the organization has a number of programs designed to help pre-term birth families including NICU transition to home care packages, preemie parent mentors who can be contacted 24/7, an app called MyPreemie, and many online forums for parents to engage with other preemie families. –https://www.grahamsfoundation.org/
2.A community of peers
Hand to Hold is an organization created to guide preemie families through the long journey from a NICU stay to home, as well as provide comfort and support in times of loss. To do so, the website maintains forums for its 63,000 online community members. But it’s not just for preemie families. There are also resources for NICU professionals including podcasts and an ambassador program of bedside support volunteers who visit NICUs and provide additional help. –https://handtohold.org/
3.A place for bereavement support
Bereavement support is something all too many families of premature babies need. And High Risk Hope is one place they can find it. The 501(c)3 believes that “there is no foot too small that it cannot leave an imprint on this world.” To do so, the Florida-based organization connects families with other organizations to provide ongoing grief support and counseling. –https://highriskhope.org/
4.One-on-one care
Support 4 NICU Parents Support 4 NICU Parents aims to improve psychosocial support for NICU parents and enhance training and support for NICU healthcare providers, ensuring families and babies thrive together. –https://www.pqcnc.org/node/13721
5.Parental Zoom chats
Tiny Miracles is a nonprofit charity based in Fairfield County, Connecticut, that is dedicated to helping families with premature babies. Like many premature baby groups, it offers all kinds of resources for families, but its most popular offerings are free weekly Zoom support chats that anyone can join. Held every Thursday at 8 p.m. EST, they’re a way for people to get to know other parents beyond a virtual chat room or forum.-https://www.projectsweetpeas.com/
6. Material support
Care packages, hospital events, peer-to-peer support, financial aid, educational materials, these are all the work of Project Sweet Peas. Families can reach out directly for all of the above and receive the care they need from this nonprofit. And for those who have simply been touched by a premature birth and want to give back, they can donate to Project Sweet Peas’ effort which has sent 23,126 NICU care packages to families and 4,909 bereavement boxes as well.-https://www.projectsweetpeas.com/
7.Facebook Preemie Page
Social media sites, like Facebook, are a natural home for support groups and the Parents of Preemies/Premature Babies is one of the biggest for this specific demographic. With 15.3K members, it’s a private group you must ask to join. It was started in 2007 when founder Heather Armstrong writes that she couldn’t find a similar support space. It invites members to discuss topics related to the raising of premature children but doesn’t allow fundraising, self-promotion, or requests for medical advice. It includes parents of preemies from around the world.-https://www.facebook.com/groups/2304668997
8. Helping hand from March of Dimes
Not every hospital has a March of Dimes NICU Family Support program, but it’s worth inquiring should a family find itself with a baby in the newborn intensive care unit. The nonprofit that’s committed to improving the health of mothers and babies organized its NICU Family Support program to provide families with essential materials during their child’s NICU stay. Those include things like “keepsake booklets for their NICU baby, a guide for parenting in the NICU, and a NICU guide” according to the organization’s website. For families with an infant having a shorter NICU stay, March of Dimes provides materials as well. There’s also a helpful app where families can explore their questions and concerns.-https://www.marchofdimes.org/find-support/compassbymarchofdimes
9.Support for babies less than 2 pounds
Premature babies are not a monolith. There are varying levels of prematurity and some of the most at-risk children are those born less than 2 pounds and before 27 weeks. That’s why the Micro Preemie Parents Facebook support page exists, to be there for parents of these special children. Only parents of so called “micro preemies” will be accepted to the private page. Once in, they can expect to be able to join conversations specific to this very unique experience with other parents and guardians who understand where they’re coming from. –https://www.facebook.com/groups/micropreemiemoms
10. A Space for Black Preemie Parents
Black Preemie Parents Community is a Facebook group just for Black parents to find “support, advice, share stories, or just vent as you go through your journey.” It’s a small group with less than 400 members providing those who join with an intimate circle of friends to reach out to during challenging times. –https://www.facebook.com/groups/blackpreemieparentscommunity
11. Where to go when they grow
The premature parenting journey doesn’t end when a child leaves the NICU. It’s a lifelong path and one that might find parents looking for support well into their child’s teens and twenties. For that there’s Parents of Older Preemies. Another Facebook group, this 1.5K member page is for “parents to share their stories of their preemie(s) and how far they have come in their lives in a caring and supportive environment. This group shares triumphs, setbacks, frustrations and positive advice to others that are on their continued “preemie journey.”-https://www.facebook.com/groups/276697059074997
12. Visual Support
Preemie baby support isn’t limited to Facebook and nonprofit organizations. Instagram has also become a network where people kind find kinship in navigating life with a preemie. For instance, preemiesupermoms is an Instagram page dedicated to prematurity awareness. The page posts images of premature babies along with inspiring quotes and stories
For families looking for someone to listen or a place to gather strength, these organizations are here to help. All families need to do is ask. –https://www.instagram.com/preemiesupermoms/
INNOVATIONS
EDITORIAL: What is new on the Horizon in Neonatology? Recent Advances in Monitoring, Diagnostics, and Therapeutics in Neonatal Care
Introduction
Neonates and infants are commonly referred to as “therapeutic orphans” due to the overall scarcity of therapeutic interventions that have been developed and tailored to their needs and specific characteristics . This is well known by care providers and researchers active in this field, but is perhaps less on the radar of authorities, funding bodies or the broader public. There is significant health inequity when comparing newborns to other age populations in terms of specific drug and device development and therapeutics . In addition there are health inequities in the provision of neonatal care globally which require special attention in terms of improvement .
Bronchopulmonary dysplasia, neonatal seizures, poor growth, necrotizing enterocolitis (NEC) and short bowel, hypoxic-ischemic encephalopathy, retinopathy of prematurity (ROP), neonatal infections and sepsis hereby serve as a non-exhaustive list of “orphan conditions” in need of more equity, through adequately and urgently funded research and improvement.
The good news is that there have been increased efforts, in recent years, by researchers and regulatory bodies to focus on the provision of drugs, devices, and treatment modalities tailored for neonatal use, while further advocacy remains an obvious need (2, 4, 5). This brings perspective and explains the initiative taken to organize a focused research topic on what is on the horizon as well as recent advances.
Overview of the topics covered
We targeted emerging or new aspects related to monitoring, diagnostics and therapeutics in neonatal care for the current research topic. Fortunately, this research topic was perceived as very relevant by the research community, as 135 authors expressed their interest as contributors, resulting in 20 accepted papers. This serves as a signal of the importance to continue to work on this topic.
Post-hoc, and in a somewhat arbitrary way (because of overlap in these subcategories) these papers were subdivided by the editors into different subcategories, with focus on (1, 5 papers) perinatal biomarkers in blood and urine and how these relate to or predict outcomes, (2, 6 papers) adaptations of existing and newly emerging equipment in neonatal units, (3, 3 papers) needed advances in pharmacotherapy, (4, 3 papers) machine learning or deep learning applications in neonatal care, and finally, (5, 3 papers) underreported aspects of contemporary NICU care, with a focus on the holistic nature of care for the infant and the family.
Perinatal biomarkers in blood and urine and how these relate to or predict outcomes
Two papers focused on biomarkers related to gestational diabetes, with reflections and data on maternal and neonatal outcomes. Postnatal maternal levels of glycated albumin and hemoglobin A1c in mothers of large-for-gestational-age (LGA) informed us of the relevance of accurate diagnosis during pregnancy. This is because postpartum women without diagnosis during pregnancy had higher glycated albumin values, associated with LGA and associated complications (Železnik et al.). Interestingly and related to this paper, Yin et al. reported on a untargeted metabolomics study in women with gestational diabetes, with the recommendation of a maternal serum metabolite panel to forecast neonatal adverse outcomes (hypoglycemia and macrosomia) (Yin et al.).
Other papers focused on the use of vitamin D, acid-base and biomarkers associated with fetal growth restriction with impaired neurodevelopmental outcome. In a cohort of 217 preterm neonates, a multivariate regression analysis identified antenatal steroids as protective, and lower birth weight, duration of ventilation, sepsis and the serum 25-(OH)D vitamin as risk factors to develop ROP (Yin et al.). Musco et al. reported on a systematic review on blood biomarkers indicating risks of adverse neurodevelopmental outcome in fetal growth restricted infants (Musco et al.). While the authors retrieved some data on neuron specific enolase and S100B, the overall conclusions reflect a call for further research. Finally, an association between lactate levels in umbilical cord blood and cerebral oxygenation in preterm neonates was studied as a secondary outcome analysis (Dusleag et al.). In non-asphyxiated preterm neonates with respiratory support, lactate levels were negatively associated with cerebral and arterial oxygenation. In term neonates without respiratory support, no associations were observed.
Adaptations of existing and newly emerging equipment in our units
In a review on emerging innovations in neonatal monitoring, Krbec et al. concluded that there is an urgent, still unmet need to develop wireless, non- or minimal-contact, non-adhesive technology, capable to integrate multiple signals in a single platform, tailored to neonates (Krbec et al.). Related to this call of action, Svoboda et al. reported on their pilot experience with contactless assessment of heart rate, applying imaging photoplethysmography (Svoboda et al.). Rectal and axillary temperature monitoring on admission were compared in a cohort of preterm (n = 80, <32 weeks gestational age) by Halabi et al., reporting that rectal measurement was likely more reliable in the event of hypothermia (Halabi et al.). Ultrasound-guided measurement of anterior cerebral artery resistive index in the first week of life in 739 preterm neonates (<35 weeks) was not associated with subsequent co-morbidities on admission or during neonatal stay (asphyxia, sepsis, NEC) (Singh Gill et al.). A case series of neurally adjusted ventilatory assist to rescue pulmonary interstitial emphysema in 5 extremely low birth weight infants illustrated the potential value of this ventilatory equipment and strategy and need for further study (Chen et al.). Finally, van Rens et al. compared a conventional to a modified Seldinger technique (a dedicated micro-insertion kit) for peripherally inserted central catheter (PICC) placement, illustrating the relevance of developing “low risk, high benefit” type of medical devices, adapted to the specific needs of neonates (van Rens et al.).
Advances needed in pharmacotherapy
The currently available medicines and dosing regimens in neonatal care are limited and there is an urgent need for improvement in this domain. This was illustrated by articles on sepsis, septic shock and steroids. Inequity in provision of neonatal care across the globe ought to be a major focus of improvement. Gezahegn et al. described the outcome in neonates admitted with sepsis in Harar (Ethiopia). Low white blood cell count, desaturation, preterm birth, absence of prenatal maternal care, and chorioamnionitis were important risk factors for sepsis-related mortality (Gezahegn et al.). Addressing these prognostic factors hold the promise to act as levelers to improve outcomes. A pilot study compared noradrenaline and adrenaline as first line vasopressor for fluid-refractory sepsis shock (Garegrat et al.). Both interventions were comparable to resolve the septic shock, while the overall mortality (13/42, 30%) remained significant, highlighting the need for better diagnostic and therapeutic options. Finally, in a systematic review, outcome of postnatal systemic corticosteroids (hydrocortisone to dexamethasone) were compared as reported in randomized controlled trials (Boscarino et al.). The authors concluded that dexamethasone appeared to be somewhat more effective than hydrocortisone in improving respiratory outcomes, but with inconclusive but relevant concerns on the uncertainties on long-term neurodevelopmental outcome, again highlighting the need for better therapies for prevention and management of chronic lung disease of prematurity.
Machine learning or deep learning applications in neonatal care
Artificial intelligence is a rapidly advancing area with fast evolving clinical applications in healthcare, including in the NICU (6). It is no surprise that the current research topic also contains papers illustrating its relevance to improve our practices and outcomes. Two papers hereby focused on NEC, and a 3rd paper on prediction of significant patent ductus arteriosus (PDA). In a mini-review, Cuna et al. reports on the various pathophysiological processes underlying NEC endotypes, and how artificial intelligence holds the promise to influence further understanding and management (Cuna et al.). An approach to enhance surgical decision making in NEC is illustrated by Wu et al. Based on x-rays from 263 neonates diagnosed with NEC (94 surgical cases), a binary diagnostic tool was trained and validated, with Resnet18 as approach applied (Wu et al.). For PDA, an ultrasound-based assessment of ductus arteriosus intimal thickness in the first 24 h after birth was applied in 105 preterm neonates. A prediction model for closure on day 7 included birth weight, mechanical ventilation, left ventricular end-diastolic diameter, and PDA intimal thickness (Hu et al.). Such models can be considered to better target future study, integrated in a precision medicine approach. Use of AI and big data have the potential to significantly improve our understanding of neonatal conditions and also support neonatal researchers in asking better research questions.
Underreported aspects of contemporary NICU care, holistic care
As part of this research topic, we also accepted papers reporting on the use of music on pain management, on multisensory stimulation to improve maternal milk volume production, and parents’ experiences related to congenital cardiac surgery. All these 3 papers reflect the need for holistic care and to further integrate the perspectives of (former) patients and parents into neonatal practice.
In a systematic review, Ou et al. demonstrated that music is an effective intervention to relief procedural pain (e.g., Premature Infant Pain Profile score) in preterm neonates, as it reduced some markers of stress, and improved blood oxygen saturation (Ou et al.). Multisensory stimulation (audiovisual, or audiovisual + olfactory) compared to a control setting improved maternal milk volume production, with evidence of positive effects of both interventions, even more pronounced if both interventions are combined (Cuya et al.). Finally, a quantitative analysis of parent’s experiences with neonates admitted to NICU with a congenital heart disease reinformed us on the importance of actively focusing on parental experiences of care (Catapano et al.).
From advances in neonatal care to implementation
In our opinion, this research topic nicely illustrates the diversity in ongoing clinical research activities, that all hold the promise to improve our clinical management practices, with the overarching aim to improve neonatal outcomes. There is an urgent need to focus on the current health inequities in the provision of care to neonates (3). The trend towards a “neuro” dedicated NICU care is an illustration on how relevant progress may occur. This progress is based on improved neuromonitoring techniques (7), improved management and precision medicine in the field of anti-epileptic drugs (8), and integrating families as partners in neonatal neuro-critical care and similar improvement programs (9). The good news is that we are already experiencing a shift in the right direction. The neonatal community and all other relevant stakeholders need to work better together to improve the pace and scale of this improvement.
The prenatal shunt, ductus arteriosus (DA), typically closes during the cardio-pulmonary transition at birth. We evaluated maternal and neonatal factors associated with delayed closure of DA in term-born neonates.
Method
We conducted a retrospective cohort study that included full-term neonates from the prospective observational Copenhagen Baby Heart cohort study. We assessed the association between maternal and neonatal factors and delayed ductal closure.
Results
We included 19,566 neonates, of whom 48% were female. Echocardiography was performed at a median age of 12 (IQR:9-15) and eight (IQR:2-13) days for neonates with no DA and an open DA, respectively. Associations with delayed ductal closure included maternal obesity adjusted risk ratio=2 (95%CI:1-3.8), maternal hypothyroidism during pregnancy aRR=2.02 (95%CI:1.2-3.4), low Apgar 2.6 (95%CI:1.2-6), high weight aRR=1.81(95%CI:1.2-2.6), and length at birth aRR=1.7(95%CI:1.1-2.6).
Conclusion:
The identified risk factors for delayed ductal closure in term-born neonates may help increase clinical attention and improve neonatal care.
UNICEF 2025 Global Outlook: Prospects for Children in 2025 – Building Resilient Systems for Children’s Futures
17 February 2025
Prospects for Children in 2025: Building Resilient Systems for Children’s Futures is the latest edition of Global Outlook, a series of reports produced each year by United Nations Children’s Fund (UNICEF) Innocenti – Global Office of Research and Foresight, which look at the key trends affecting children and young people over the following 12 months and beyond.
In this new report, new and intensifying crises for children – including climate change, conflict and economic instability – are shown to be closely interconnected.
For instance, climate change is disrupting the water cycle, leading to widespread water scarcity, threatening food production and livelihoods across the economy. This disruption poses direct and indirect risks to children, as it impacts the availability of safe water, food, and family income.
The report also notes that debt burdens are forcing governments to cut essential public services, including those related to water, sanitation, and hygiene. These challenges are compounded by a lack of investment in long-term development.
According to UNICEF, rising geopolitical tensions and competition among nations are hindering the implementation of solutions that will protect young people’s lives and build more resilient futures for them.
The report calls for resilient national systems that prioritize children’s health, education and wellbeing, and emphasizes the importance of including children’s rights in climate action.
Empathy and compassion is the foundation of the powerful bond we share as a community. It’s more than just understanding the struggles of others—it’s about truly connecting with their experiences and emotions. As we continue on our journey from the neonatal unit to where we are today, empathy strengthens our resilience and fosters a sense of unity. This connection gives us the strength to support one another, celebrate our victories, and face challenges together.
In the video you’re about to watch, we’ll dive deeper into how our shared experiences and collective empathy can empower us to not only overcome adversity but also to thrive. It highlights the importance of understanding and supporting each other, offering both comfort and encouragement in meaningful ways. Through storytelling and the exchange of our journeys, we create a community that is stronger, more resilient, and ready to face whatever challenges come our way.
I wanted to share this video because it perfectly encapsulates the power of empathy and how, together, we can elevate each other. It’s a reminder that even in difficult times, we are never alone—our shared experiences and collective strength can light the way forward.
Let’s continue to harness the power of empathy as we watch and reflect on the message in this video. Together, we are unstoppable.
What Is The Difference Between Empathy, Sympathy, and Compassion
The Power of Emotional Competency
Expert Reveals the Truth About Empathy, Sympathy and Compassion | Doug Noll
This video shows you the difference between empathy, sympathy, and compassion
• Sympathy is pity-based and is selfish
• Empathy is a learned skill
• Compassion is empathy with an impulse to relieve distress
This video is for our younger friends to help them understand empathy, which means caring about how others feel and being kind to them. Mark Ruffalo and Murray Monster from Sesame Street will show us what empathy is and give fun examples of how we can be kind and helpful to others. I wanted to share this video because it’s a great way for younger kids to learn how to show empathy and support for their friends and family. Let’s watch and see how we can all use empathy to make the world a kinder place! Enjoy watching!
Sesame Street – Empathy With Mark Ruffalo
This video is perfect for helping young students understand what empathy is. Murray Monster and Mark Ruffalo talk about what empathy means and go through several examples. Use this helpful video for introducing important social skills to your K-2 students!
Quiksilver & Roxy Czech and Slovak Surfing Championship 2022












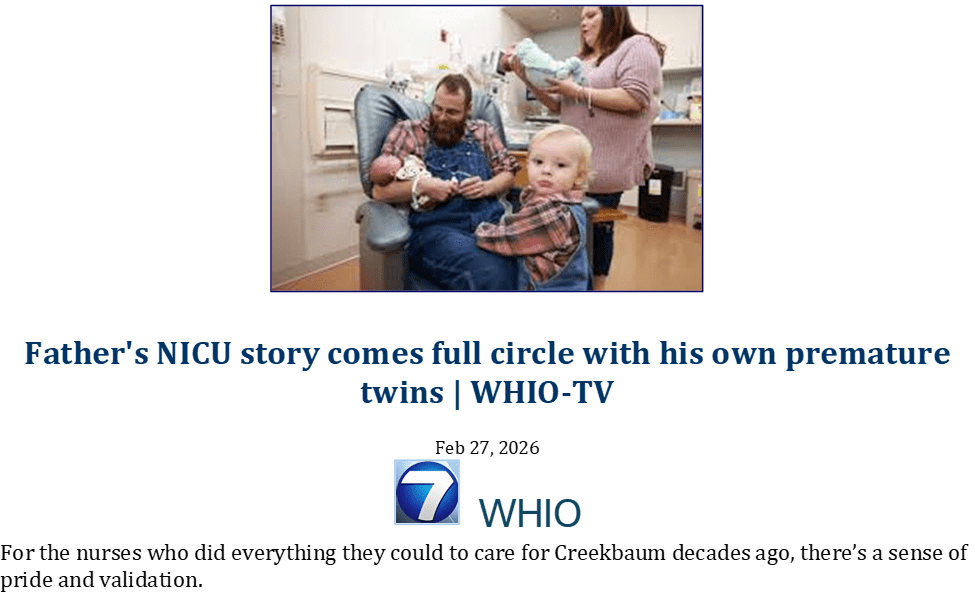



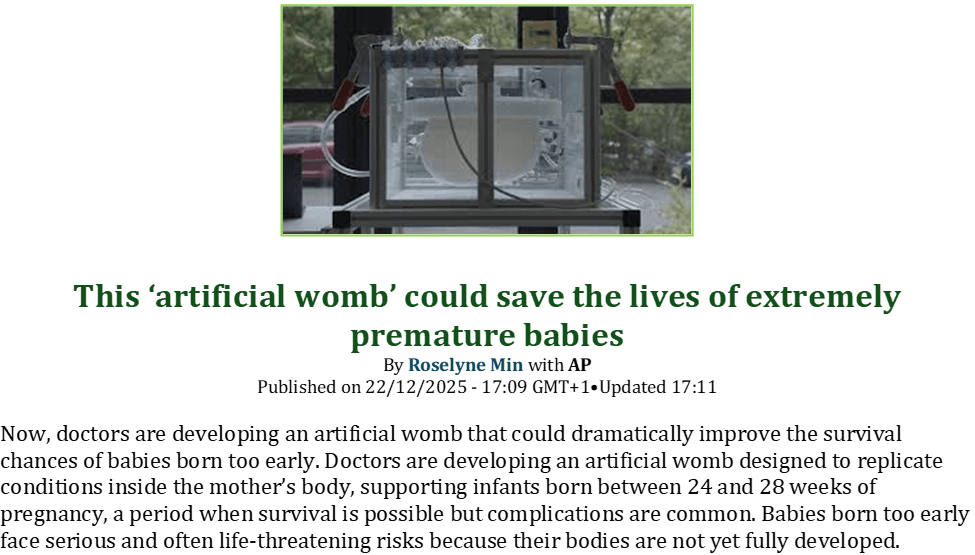
























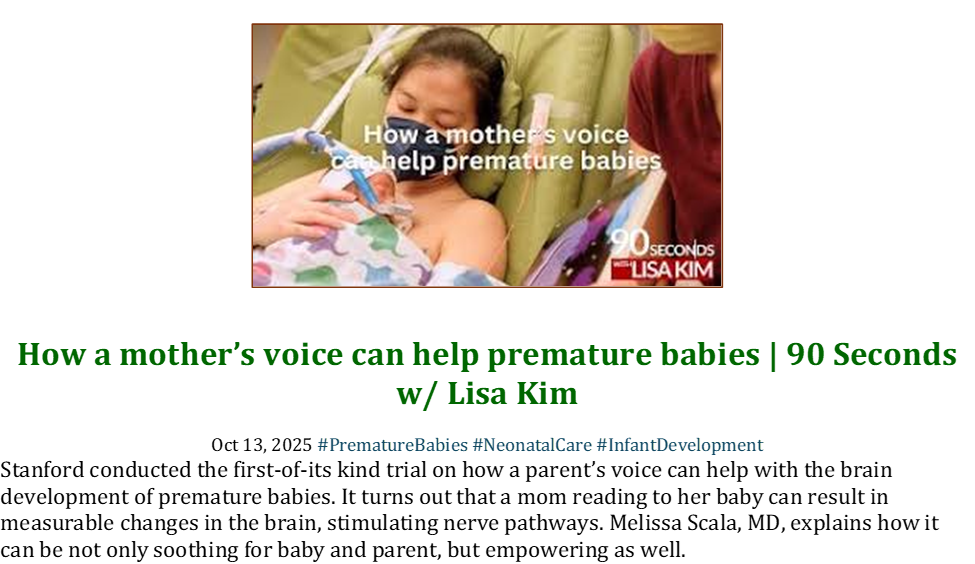





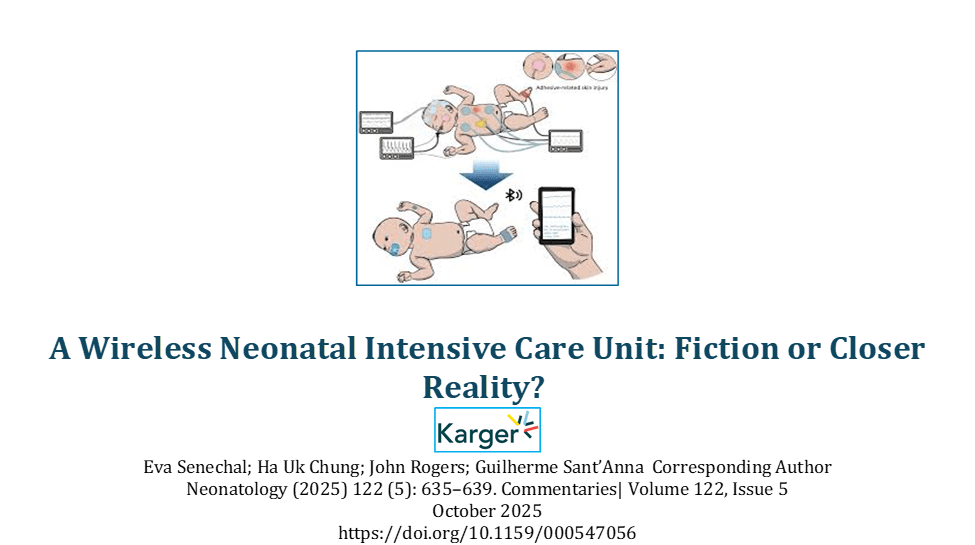









































































































































































































































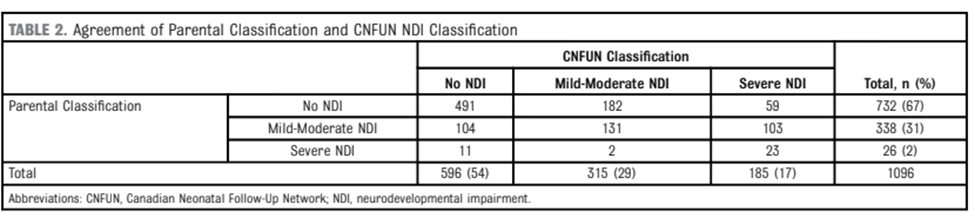


























{kind=link}
{kind=link}