

JAMAICA
PRETERM BIRTH RATES – Jamaica
Rank: 92 –Rate:10.2 Estimated # of preterm births per 100 live births
(USA – 12 %, Global Average: 11.1%)

Jamaica is an island country situated in the Caribbean Sea. Spanning 10,990 square kilometres (4,240 sq mi) in area, it is the third-largest island of the Greater Antilles and the Caribbean (after Cuba and Hispaniola).[ Jamaica lies about 145 kilometres (90 mi) south of Cuba, and 191 kilometres (119 mi) west of Hispaniola (the island containing the countries of Haiti and the Dominican Republic); the British Overseas Territory of the Cayman Islands lies some 215 kilometres (134 mi) to the north-west.
With 2.9 million people, Jamaica is the third-most populous Anglophone country in the Americas (after the United States and Canada), and the fourth-most populous country in the Caribbean. Kingston is the country’s capital and largest city. The majority of Jamaicans are of Sub-Saharan African ancestry, with significant European, East Asian (primarily Chinese), Indian, Lebanese, and mixed-race minorities. Due to a high rate of emigration for work since the 1960s, there is a large Jamaican diaspora, particularly in Canada, the United Kingdom, and the United States. The country has a global influence that belies its small size; it was the birthplace of the Rastafari religion, reggae music (and associated genres such as dub, ska and dancehall), and it is internationally prominent in sports, most notably cricket, sprinting and athletics.
Jamaica is an upper-middle income country with an economy heavily dependent on tourism; it has an average of 4.3 million tourists a year. Politically it is a Commonwealth realm, with Elizabeth II as its queen. Her appointed representative in the country is the Governor-General of Jamaica, an office held by Patrick Allen since 2009. Andrew Holness has served as Prime Minister of Jamaica since March 2016. Jamaica is a parliamentary constitutional monarchy with legislative power vested in the bicameral Parliament of Jamaica, consisting of an appointed Senate and a directly elected House of Representatives.
Healthcare in Jamaica is free to all citizens and legal residents at the public hospitals and clinics. This, in theory, includes the cost of prescribed medication. There are long queues at public health facilities. An audit in 2015 identified shortages of manpower, equipment, medications, wheelchairs, stretchers, gloves, beds, and other essential supplies. 3.3% of the national budget is spent on health services. In Jamaica there are over 330 health centres, 24 public hospitals, the University Hospital of the West Indies, a regional teaching institution partially funded by Regional Governments including Jamaica, 10 private hospitals and over 495 pharmacies. There are around 5,000 public hospital beds and about 200 in the private sector.

COMMUNITY

Gov’t to Review Laws That Support Breastfeeding
*** We looked for an update to these actions and did not find formalized and related outcomes in Jamaica yet related to the article below but the future likely holds support for improvement. This improvement in support for breastfeeding reflects a global need for progressive and related action.

SEPTEMBER 18, 2019 WRITTEN BY: OKOYE HENRY
Minister of Health and Wellness, Dr. the Hon. Christopher Tufton, says that stakeholders are being engaged to review and improve national laws that support breastfeeding.
In a message delivered by Public Health Nurse, Debbion Pinnock Harvey, at Westmoreland Public Health Services’ ‘Breastfeeding March and Road Show’ in Darliston on Tuesday (September 17), Dr. Tufton noted that the objective is to create a more enabling environment for mothers to breastfeed in order to improve the health of their babies.
“[This will] also ensure that workers in the informal economy and other vulnerable groups are recognised and protected by national laws. We also encourage employers to implement breastfeeding-friendly workplaces by establishing support facilities such as crèches, breastfeeding rooms and flexible work hours,” he noted.
Dr. Tufton said that the Ministry has spearheaded the development of the National Infant and Young Child Feeding Policy, which has the objective of creating “a sustainable environment that will contribute to a reduction in child mortality and morbidity and improvement in child health and nutrition”.
Meanwhile, the Ministry is encouraging greater family support for lactating mothers as the country marks National Breastfeeding Week 2019 from September 16 to 22.
“Although breastfeeding is the mother’s domain, with close support from fathers, partners, families, workplaces and communities, breastfeeding will improve,” Dr. Tufton said.
Breastfeeding is the responsibility of all, the Minister said. “Wherever you are, you can inform, anchor, engage and galvanise the message of breastfeeding as the fountain of life by raising awareness of the risks and disadvantages of artificial feeding and advocating for greater investment in breastfeeding programmes and policies,” he noted.
The Westmoreland Public Health Services ‘Breastfeeding March and Road Show’ was held under the theme, ‘Empower Parents: Enable Breastfeeding, Now and for the Future!’
The event featured health stakeholders from across the parish, who partnered with parents, schools and the police to make presentations on the benefits of breastfeeding.
Source: https://jis.gov.jim/govt-to-review-laws-that-support-breastfeeding/

Neonatology in Beirut, a Country Ravaged by a Financial, Political and Social Crisis
Carine Abi Gerges, MD – December, 2020
While 2020 has been a difficult year for most people, Lebanon has been particularly hit hard by the turn of the decade. In October 2019, thousands took to the streets to demand the overthrow of a corrupt regime. People protested for months while chanting ‘Kellon yaane kellon’ (All of them means all of them) in reference to the entire ruling class. Political and civil unrest rocked the country against the backdrop of an unprecedented economic and financial crisis: the Lebanese pound plummeted in a free-fall, eventually losing over 80% of its value with local banks imposing strict restrictions on cash withdrawals preventing depositors from accessing both their savings and salaries. The Coronavirus pandemic made matters substantially worse. The final blow, however, was the Beirut Port explosion on August 4th, 2020. One of the largest non-nuclear blasts ever recorded, it left 150+ dead with 6,000+ injured, 300,000+ homeless, and many more forever scarred by the detonation of almost three kilotons of ammonium nitrate neglectfully stored in the heart of the capital. Three months later, someone has yet to be held accountable.
The health sector, buckling under the pressure, was not spared and is barely holding in this untenable situation. Not long ago, Lebanon was the medical capital of the Middle East. In Beirut alone, over ten hospitals are fully equipped with neonatal intensive care units (NICU), serving as a referral hub for rural areas and serving hundreds of thousands of patients. Among the 70,000 babies born in Lebanon annually, 12% (9,000) are born prematurely. Additionally, around 9,000 premature births have been recorded among Syrian refugees since 2015, amounting to a total of at least 18,000 documented premature births per year . All patients require appropriate financial health coverage to support their medical management, very costly for admitted neonates.
Prior to the financial crisis, less than half of Lebanese citizens had private or semi-public health insurance plans while the remaining half paid out-of-pocket, partly relying on the Ministry of Public Health (MoPH). As an increasing number of previously insured families lost their jobs and consequently their insurance coverage due to the crisis, many more now resort to an already overwhelmed MoPH to cover their hospital fees. However, some hospitals refuse to admit MoPH-covered patients due to years of accumulated unpaid dues from the government. Soon, only the upper class will be able to afford the estimated $30,000 in costs for the care of a premature baby.
The cost of NICU hospitalization depends on whether the hospital is public or private, as well as the baby’s condition. While most of Beirut’s patients are admitted with frequently encountered cases such as prematurity, hyaline membrane disease, necrotizing enterocolitis, and neonatal sepsis, some infants transferred from peripheral hospitals require acute care for rare metabolic and genetic diseases. Although not studied in this specific context, rural areas have a higher prevalence of births with inborn errors of metabolism, likely due to more frequent consanguineous marriage. With the population in these areas being largely working class, access to high-quality neonatal intensive care is particularly challenging, the crisis making it even worse.
Dany al-Hamod, the director of the NICU at Saint George Hospital University Medical Center (SGHUMC), describes a substantial increase in the number of families unable to afford hospital bills recently, forcing them to run from one non-governmental organization (NGO) to another to gather funds to avoid having to move their child to different facilities, or worse. The situation is even more dire for refugees. Lebanese is host to the second-largest Syrian refugee population and third largest Palestinian refugee population in the world. This population has increased in the last few years, partly due to the influx of over45,000 ‘twice-refugee’ Palestinians, once settled in Syria, fleeing to Lebanon to escape the civil war . Unable to be employed as a result of their refugee status, most do not have access to either public or private health coverage. Instead, they depend on humanitarian organizations to cover their healthcare needs, namely the United Nations Relief and Works Agency for Palestine Refugees in the Near East (UNRWA) and the United Nations High Commissioners for Refugees (UNHCR). These organizations have been essential to the survival of many newborns in this population, especially that they suffer a higher prevalence of neonatal complications due to inconsistent prenatal care, as well as higher rates of consanguinity . These organizations rely entirely on donations and grants, and their ability to cater to their beneficiaries has been severely impacted after the donations they depended on contracted as a result of the ongoing global economic crisis. The severe financial situation that the UNRWA is currently facing threatens millions of refugees and further limits their already minimal healthcare access .
The Carlos Slim Center for Children in the Beirut Governmental University Hospital (BGUH – Karantina) was renovated in 2016 by the NGO ASSAMEH – Birth and Beyond through multiple local and international donations, building the first fully-equipped public NICU. This center’s importance lies in its readiness to “care for those no one cares for.” While only 70% of admitted children are eligible for MoPH-coverage (10), specialized care at this public hospital is provided indiscriminately. Since 2017, six babies found in trash bins and more than twenty-two “undocumented” children have been taken in and treated by the Karantina team (2). Adding fuel to the fire, this center was heavily damaged by the Beirut Port explosion, nearing total collapse. Inside their incubators, babies sheltered from the debris were evacuated within 3 hours. “An apocalypse — one minute was worse than 20 years of war,” says Robert Sacy, head of the Pediatrics Department at the hospital and president of ASSAMEH – Birth and Beyond. What was once a haven for over 1,000 children per year has now been nearly razed to the ground. The remains of paintings of trees, suns, and smiles are now covered with blood on the few walls still standing. What was once joyful is now contaminated with death.
Making matters worse, a surge in the number of cases and ICUs at nearly full capacity, some project that the country might be heading towards an Italy-like scenario if serious long-term precautions measures are not implemented. The daily positivity rate fluctuates between 10 and 20%, and the death toll is 970+ since February 2020. The pandemic appears to be mostly affecting adults, with the case-fatality of children under nine years of age at 0.05% and only one recorded death(7).
Although it has been speculated that neonates, due to their immature respiratory physiology and the immune system, might be at a higher risk for COVID-19 related complications, a review of the literature shows no increased risk of severe disease in infected neonates. Conversely, Martin Filho et al. raised concern about how a cytokine storm in pregnant mothers might increase the likelihood of poor neonatal neurodevelopmental outcomes (6). Associate professor of Neonatology at the American University of Beirut Medical Center (AUBMC), Lama Charafeddine, denied that the pandemic had had any noticeable immediate effects on the rate of perinatal complications or congenital malformations or infections. She did contend, however, that it is too early to draw any conclusions regarding this matter. While COVID-19 does not significantly affect the neonatal and pediatric population, Antoine Yazbeck, head of Neonatology at Serhal Hospital, reports a drop in the overall quality of care and staff morale due to increasing physician burnout. Indeed, as of early November, numbers from the doctors’ syndicate and the order of nurses (5) show that a total of three doctors had died and seventeen admitted to intensive care units, with more than one hundred having been put under home quarantine and over 1,500 nurses having been infected. The pandemic has significantly affected the pediatric healthcare system’s overall capacity, draining it in such that neonatal care is becoming severely compromised.
For physicians around the world, and particularly in Lebanon, working conditions have become increasingly difficult. “We see 4-5 kids per day, on a good day”, reports Yazbeck, who has reported a ten-fold decrease in daily patient attendance to his clinic. Indeed, the pandemic has led many parents – those who have not migrated yet – to opt-out of vaccination programs and avoid routine follow-ups out of fear of exposure. Additionally, due to currency devaluation, consultation fees, still generally fixed at the same price in Lebanese pounds, are much less profitable to the physician (dropping from the equivalent of $60/patient to less than $12/ patient) while still being largely unaffordable for the larger patient population. Maroun Matar, head of the Neonatology Department at Lebanese American University Medical Center (LAUMC), also describes an 80% decrease in his monthly income despite raising his clinic fees by 10% whilst food products and basic necessities witness an inflation rate of more than 400% (3) and half the population is now under the poverty line. Highly qualified and trained physicians, overworked and underpaid, have decided to immigrate for better opportunities abroad. Indeed, over 400 physicians have immigrated in the last couple of months, with more expected to follow suit (8). This has pushed government officials to seek international aid to incentivize doctors to stay in the country by offering financial compensation (8). This exodus of physicians and the shortage of medications and medical equipment (hospital suppliers demanding to be paid in hard currency, largely unavailable on the market) has significantly reduced the quality of healthcare in Beirut, once a regional health hub in the Middle East.
It is crucial to bring to light the difficulties encountered by healthcare workers in developing countries to identify the various factors affecting the quality of care offered to patients. The pandemic has highlighted wide disparities and brought to the fore existing inequalities in developed countries, exposing the need to fill large healthcare delivery gaps to marginalized communities. In a country like Lebanon, shaken by financial precariousness, famine, civil unrest, a large explosion, a mass exodus, and a global pandemic, these disparities have become even more apparent and alarming. This eventful year has highlighted the lack of a national emergency preparedness plan, inadequate infection prevention and control practices, and the absence of an effective healthcare safety net for the uninsured in Lebanon. It is crucial to address these deficiencies for a better-equipped healthcare system in the face of the next blow in order to be able to, at least, give the newborns the gift of time.
Source: http://www.neonatologytoday.net/newsletters/nt-dec20.pdf

Infant who survived in 1920s sideshow incubator dies at 96
By ASSOCIATED PRESS FEBRUARY 24, 2017

New York Public Library
MINEOLA, N.Y. — Lucille Conlin Horn weighed barely two pounds when she was born, a perilous size for any infant, especially in 1920. Doctors told her parents to hold off on a funeral for her twin sister who had died at birth, expecting she too would soon be gone.
But her life spanned nearly a century after her parents put their faith in a sideshow doctor at Coney Island who put babies on display in incubators to fund his research to keep them alive.
The Brooklyn-born woman who later moved to Long Island, New York, died Feb. 11 at age 96, according to the Hungerford & Clark Funeral Home. She had been suffering from Alzheimer’s disease.
Horn was among thousands of premature babies who were treated in the early 20th century by Dr. Martin Couney. He was a pioneer in the use of incubators who sought acceptance for the technology by showing it off on carnival midways, fairs and other public venues. He never accepted money from their parents, but instead charged oglers admission to see the tiny infants struggling for life.
Horn and her twin were born prematurely in Brooklyn. She told The Associated Press in a 2015 interview that when her sister died, doctors told her father to hold off on a funeral because tiny Lucille, would not survive the day.
“He said, ‘Well that’s impossible, she’s alive now. We have to do something for her,’” Horn said. “My father wrapped me in a towel and took me in a cab to the incubator; I went to Dr. Couney. I stayed with him quite a few days; almost five months.”
Couney, who died in 1950 and is viewed today as a pioneer in neonatology, estimated that he successfully kept alive about 7,500 of the 8,500 children that were taken to his “baby farm” at the Coney Island boardwalk. They remained there until the early 1940s, when the incubators became widely used in hospitals.
He also put infants on display at the World’s Fair and other public venues during his career. There is no estimate on how many still are alive today.
Horn worked as a crossing guard and then as a legal secretary for her husband. She is survived by three daughters and two sons. She said she met Couney when she was about 19 and thanked him for what he had done.
“I’ve had a good life,” she said in 2015.
After a funeral Tuesday, she was buried at the Cemetery of the Evergreens in Brooklyn, next to her twin sister.
Source: https://www.statnews.com/2017/02/24/incubator-baby/

Disaster Preparedness in Neonatal Intensive Care Units
Wanda D. Barfield, Steven E. Krug, COMMITTEE ON FETUS AND NEWBORN and DISASTER PREPAREDNESS ADVISORY COUNCIL – Pediatrics May 2017, 139 (5) e20170507; DOI: https://doi.org/10.1542/peds.2017-0507
Abstract
Disasters disproportionally affect vulnerable, technology-dependent people, including preterm and critically ill newborn infants. It is important for health care providers to be aware of and prepared for the potential consequences of disasters for the NICU. Neonatal intensive care personnel can provide specialized expertise for their hospital, community, and regional emergency preparedness plans and can help develop institutional surge capacity for mass critical care, including equipment, medications, personnel, and facility resources.

FIGURE 1
Model of decision-making based on available supplies: example using respiratory support. The figure shows a model of decision-making based on available supplies, personnel, patient acuity, and surge capacity for pediatric EMCC. CPAP, continuous positive airway pressure; ECMO, extracorporeal membrane oxygenation. Reproduced with permission from Bohn D, Kanter RK, Burns J, Barfield WD, Kissoon N. Supplies and equipment for pediatric emergency mass critical care. Pediatr Crit Care Med. 2011;12(suppl 6):S120–S127. Copyright © 2011 Wolters Kluwer Health.
Conclusions
Infants in the NICU are highly vulnerable in a disaster because of their need for specialized and highly technical support. As such, NICU preparedness is required for optimal disaster response.
- Preparation before a disaster event is critical to optimizing outcomes of NICU patients during public health emergencies and disasters. Health care institutions and providers are strongly encouraged to know and prepare for the most likely disaster scenarios in their communities (eg, hurricane, earthquake, or flood) and also to consider unanticipated events (eg, bioterrorism) that could create a mass casualty event and similarly affect surge capacity and capabilities.
- It is important for NICU teams to fully participate in the emergency- and disaster-planning activities of their facility, health care system, or regional, state, and local emergency management agency. Teams should be part of the periodic disaster simulation drills that are now required in every hospital. NICU teams should actively participate in the design of hospital drills to address the unique needs of NICU patients in situations involving “shelter-in-place,” relocation, and/or evacuation. The use of an incident command structure within the NICU, facility, and community is important to maintain structure and an organized response.
- Neonatal care systems (providers, administration, information technology, and equipment) can develop appropriate staffing support for safe and effective operations during disasters. NICU care providers, in collaboration with their hospital facility, community practitioners, network, and region, need to identify the surge capacity to provide 3 times the baseline critical care resources and sustain this for 10 days during a major public health disaster. An effective response to specific disaster threats, including maintenance of adequate surge capacity, relies on sufficient supplies of age- and size-appropriate MCMs.
- During a disaster, neonatal care providers can maintain situational awareness for decision-making, including patient volume and severity of illness, available equipment, medication, and staffing, transport, evacuation, recovery, and crisis standards of care. Maintaining flexibility is important in adjusting to new situations. Advance planning and coordination with local and state public health and emergency management agencies will additionally support situational awareness and timely decision-making. A process of ethical decision-making and altered standards of care needs to be included in disaster planning.
- In addition to the needs of patients, NICU providers may need to consider the medical and psychosocial needs of postpartum mothers and families. To the extent it is feasible, parents and families should remain in contact with patients. Families may have unique needs and/or require assistance in unusual ways during a large-scale disaster. In addition, plans should be made to recognize and respond to the needs of NICU staff, including self-care and support.
- Although some guidance in this report is based on systematic reviews (eg, H1N1 and mass critical care), much is based on lessons learned from previous disaster events. Preparedness is an ongoing process that changes on the basis of learned experience and evidence. NICU providers should continue to research best practices, neonatal medications and dosing, and the effects of altered standards of care in disasters.
Source:https://pediatrics.aappublications.org/content/139/5/e20170507
*** Our Neonatal Womb Warrior Family and global Maternal and Child health at large are substantially and increasingly affected by the direct effects and challenges climate change and natural disasters invoke on our communities. We are closely exploring these issues and the opportunities offered towards supporting positive change/response to these changes. Education remains foundationally essential towards formulating progressive strategies to interact with the challenges climate change and natural disasters offer. Like the Covid pandemic, physical borders cannot prevent local impacts of increased levels of climate change and natural disasters; and global collaboration towards addressing the associated needs through targeted and effective action in relationship to these elements is vitally essential.

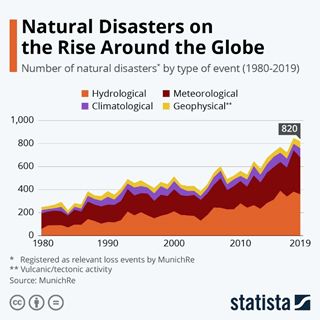
Natural disasters are occurring more frequently with increased ferocity, UN says
- Extreme weather events are occurring more often, experts have warned.
- In the last 20 years, 7,348 major disaster events were recorded globally, claiming 1.23 million lives.
- These events cost $2.97 trillion in economic losses with 8 out of the 10 most-affected countries in Asia.
Extreme weather events have increased dramatically in the past 20 years, taking a heavy human and economic toll worldwide, and are likely to wreak further havoc, the United Nations warned.
Heatwaves and droughts will pose the greatest threat in the next decade, as temperatures continue to rise due to heat-trapping gases, experts said.
China (577) and the United States (467) recorded the highest number of disaster events from 2000 to 2019, followed by India (321), the Philippines (304) and Indonesia (278), the U.N. said in a report issued the day before the International Day for Disaster Risk Reduction. Eight of the top 10 countries are in Asia.
Some 7,348 major disaster events were recorded globally, claiming 1.23 million lives, affecting 4.2 billion people and causing $2.97 trillion in economic losses during the two-decade period.
Drought, floods, earthquakes, tsunamis, wildfires and extreme temperature events caused major damage.
“The good news is that more lives have been saved but the bad news is that more people are being affected by the expanding climate emergency,” Mami Mizutori, the U.N. Secretary-General’s Special Representative for Disaster Risk Reduction, told a news briefing.
Source: https://www.weforum.org/agenda/2020/10/natural-disasters-tsunamis-droughts-floods/

This chart shows how much more common natural disasters are becoming

PREEMIE FAMILY PARTNERS
Your Premature Baby’s Development and Medical Follow-Ups
by Sara Novak Medically Reviewed by Lauren Crosby, M.D., F.A.A.P. on
March 3, 2020

When it comes to premature babies’ development, parents need a big dose of patience. Thankfully, most preemies catch up with the full-term crowd by toddlerhood.
Premature babies are born weeks and sometimes months before their actual due date, often before their nervous systems have fully developed. As a result, they can fall behind full-term babies after they’re born. That doesn’t mean that they won’t develop into perfectly normal and healthy kids, but it does mean that their timelines can be a little different from those of full-term babies.
How will my preemie’s development differ from that of full-term babies? Premature babies develop at a different rate than other babies, and just because your child has passed her due date doesn’t mean she’s all caught up.
Calculate her corrected age. When you’re considering your premature baby’s development it’s important to consider not just the day she was born, but also the original date she was supposed to be born. Calculating your baby’s corrected age can give you a more accurate understanding of whether she is developing at pace. For example, if your baby is 6 months old, subtract the number of weeks your baby was preterm in order to figure out her corrected age. This means that you can’t expect a 6-month-old preterm baby to sit up at the same time a 6-month-old full-term baby would, because they aren’t the same age developmentally. This “corrected age” is used during the first two years of life. By the time premature children are 2 years old, most have caught up on their milestones (so you won’t need to continue to recalculate your little one’s age).
Fine and gross motor skills could take longer. Preemies often take a little extra time to develop both gross- and fine-motor skills and hit baby and toddler milestones such as rolling over, sitting up and taking that first step. Later on, preemies are more likely than full-termers to have learning disabilities, so being aware of what’s normal and what’s not is vital to getting her the help she needs as soon as possible.
Worry less about dates and more about progress. Full-term babies are more likely to be tied to timelines when compared to preemies. With premature babies there’s less of an emphasis on timelines and more on ensuring they are progressing — from pulling up to standing to walking.
What medical follow-ups will I need for my premature baby
First and foremost, keep in regular contact with your baby’s pediatrician. That doctor will be seeing your baby for years to come, so it’s important to involve him or her from the start, even if you’re taking your child to other specialists.
- Make an appointment for a checkup soon after your baby’s release from the hospital. Most doctors will want to see a preemie within a day or two of homecoming. That way, your practitioner can get baseline readings on your premature baby’s weight and general health in order to keep close tabs on him. Note: Make sure you have a discharge summary from the neonatal intensive care unit (NICU), along with a record of your baby’s immunizations in the hospital.
- Schedule dental exams. Premature babies are more likely to suffer from delayed tooth growth and discolored teeth. Schedule your baby’s first dental exam either when your baby sprouts a tooth or when he turns 1.
Other tips on how to handle your premature baby’s development: Of course, it’s easier said than done, but try not to make your baby’s prematurity the only thing you think about. Enjoy and appreciate her for the amazing little person she is — and not as you would a delicate piece of china. It might help to remember these tips:
- Whatever she’s going through might have nothing to do with prematurity. When you’re parenting a preemie, it’s easy to attribute every small bump in the road to your baby’s premature status. But sometimes a baby’s cold is just a cold. And maybe she’s colicky because she’s got colic, not because she was born early.
- Follow your gut. No one knows your baby better than you. If something isn’t quite right, you’re most likely going to be the one to notice first, so don’t underestimate your intuition. Talk to your doctor if something seems off.
You’ve already been on a roller coaster of emotions waiting round the clock for the newest member of your family to finally be released from the hospital. It can be easy to transition that stress to your preemie’s development at home. Patience is a virtue that can’t be underestimated when it comes to your preemie’s development. And don’t worry: She’s going to catch up before you know it!
Source: https://www.whattoexpect.com/first-year/premature-baby-medical-follow-ups.aspx
The NICU Doc Who Works in the NICU and Surrounds Your Baby -Jun 26, 2020
Wanna know who are all the people who surround your baby in the NICU? Want to know who are all the people that work in the NICU? It takes a village to take care of babies. In the NICU, there are medical students, residents, fellows, nurses, neonatal nurse practitioners, neonatologists, and many more. In this video, you can find out all the different people in the neonatal intensive care unit. And in the end, you will learn about someone you would not expect to find in the NICU.

For Family and Friends

Being a parent of an infant in the Neonatal Intensive Care Unit (NICU) is very different than having a newborn at home. When you have a newborn you are trying to squeeze tasks in around their changing, feeding and sleeping schedule. When your child is in the NICU, household tasks get crammed into the brief periods between sleeping, pumping, sterilizing, working, perhaps eating and trips to the NICU. If you are lucky, you have a short trip to the hospital and are able to return home easily, but that often means you are getting home in the wee hours of the morning. If you live further away, you may end up seeking out overnight accommodations.
Regardless of your proximity to the hospital, all parents have one thing in common; they are barely home and when they are at home they are physically and mentally exhausted.
Many people offer help to parents of infants in the NICU by saying “Let me know if you need some help”. This is great and lets the parents know they are not alone. The problem is that parents are often reluctant to admit they need help, or they just don’t know what help they need. The best thing you can do is to make a specific offer to help them. Parents, you just need to accept those offers.
If you are not sure of what things you can do to help here are some ideas:
- If they have other children, pets or aging parents, offer to take care of them.
- Make them a home cooked meal in a container they don’t have to wash and return to you.
- Arrange to drop by and help with the housework.
- Offer to pick up their laundry and return it washed and folded.
- Help with the house, cut the lawn, shovel the driveway, and/or make the house look lived in.
- Pick up their mail and sort addressed mail from unaddressed mail so they can quickly look at bills and important items.
- Do some grocery shopping for them.
- Ask them “What can I do to help you ? “
- Drive parents back and forth to the hospital.
- Respect the parents’ wishes about how they want to mark the birth. Some may wish to celebrate. Others may want to wait until the baby is home. It is for the parents to decide and for you to support their wishes.
- Learn about prematurity, but don’t feel the need to share what you’re learning with the parents. Be careful about what resources you use, especially if you’re researching online.
- Try not to be offended if parents exclude you temporarily. The NICU can be difficult and some people turn inwards in order to cope.
- Shop for necessities when the baby is discharged from the hospital.
- Respect the rules of the NICU. Don’t visit if you’re sick or if people close to you are sick.
- Respect the privacy of other parents and their babies.
- Offer to communicate with other family and friends so that the parents don’t have to spend all their time updating everyone.
- Coordinate other offers of help so that the parents don’t need to organize who does what.
- Resist the urge to compare the new baby with other babies. Please don’t make comments on size or weight, and please don’t talk about other birth experiences unless you have personal experience as a parent of a premature baby.
- Keep offering help when the baby is home. The first few months can be isolating and difficult and parents can really use continued assistance.
- When a baby goes home, remember that preemies, especially during the winter months, are at risk for infections and sickness. Never visit the parents and baby at home if you’re sick, and respect their wish to keep their baby healthy. They are not being over-protective. They are being good parents.
These things will help to relieve the pressure that they are under and allow them to focus on caring for their child.
Note: these points are also things that would be appreciated by any new parent or anyone with a critically ill family member.
Source: https://www.cpbf-fbpc.org/

Life After The NICU | Meet Dr. Nathalie Maitre,
Dr. Nathalie Maitre is a neonatologist and developmental specialist who is the Director of the NICU Follow-up Program and NICU Music Therapy Program at Nationwide Children’s Hospital. She works with a diverse team of scientists, engineers and therapists who all believe strongly in the need to identify children at high-risk for disabilities as early as possible, in order to optimize recovery after the neonatal period.
Break Time for Nursing Mothers
Federal law (USA) requires employers to provide reasonable break time for an employee to express breast milk for her nursing child for one year after the child’s birth each time such employee has need to express the milk (Section 7 of the FLSA). Employers are also required to provide a place, other than a bathroom, that is shielded from view and free from intrusion from coworkers and the public, which may be used by an employee to express breast milk.
General Guidance
- WHD Fact Sheet #73, Break Time for Nursing Mothers under the FLSA (Spanish Version)
- Break Time for Nursing Mothers Frequently Asked Questions (FAQs)
- Break Time for Nursing Mothers under the FLSA (Microsoft® PowerPoint®)
- Break Time for Nursing Mothers Poster (Spanish)
- Break Time for Nursing Mothers Employee Rights Card
- FLSA Handy Reference Guide
- How to File a Complaint
Source: https://www.dol.gov/agencies/whd/nursing-mothers

HEALTHCARE PARTNERS

Panelists discuss how to manage wellness during pandemic winter
Trisha Korioth Staff Writer December 02, 2020 Pediatrician Wellness

Be honest. How much time are you spending on self-care right now? For many pediatricians, the answer is “Not enough.”
To be effective in practice, pediatricians must take care of themselves, according to panelists at an AAP town hall, Physician Resilience in the Time of COVID-19.
Anne R. Edwards, M.D., FAAP, AAP chief population health officer, led panelists in a discussion on how to address high stress levels, communicate and connect, give and get help, replenish resilience and maintain a growth mindset.
Connect with others
The pandemic has caused patient volume to drop and forced practices into new routines. Robert J. Riewerts, M.D., FAAP, of Southern California Permanente Medical Group and KP Care Management Institute, noted a silver lining. Phone time at his practice increased from between 3% and 7% to about 40% as pediatricians reached out to check in on patients and families.
Early in the pandemic, Dr. Riewerts’ group also arranged weekly discussions with expert to allay concerns about the virus. Pediatricians unaccustomed to seeking support from colleagues were encouraged to reach outside their comfort zone.
“This year, physicians are being stretched to the limits in all kinds of specialties,” he said. Supporting one another can help pediatricians model a positive example for their patients.
Routine team check-ins can build support within practices and hospitals, according to Riva Kamat, M.D., FAAP, co-lead of the AAP Section on Hospital Medicine Subcommittee on Provider Wellness and a hospitalist at Inova Fairfax Hospital for Children.
Dr. Kamat suggests asking colleagues if they are feeling stressed. “Then let them, what I call, ‘slime you.’ Let them share what’s bothering them.”
Because most problems cannot be solved in one vent session, Dr. Kamat said it is important to stay connected with the person. She asks colleagues how they would like her to check in again, such as by text or a phone call. Her institution also uses accountability partners to ensure people are taking care of themselves.
COVID-19 has isolated us in every way, said Melanie L. Brown, M.D., M.S.E., FAAP, chair of the AAP Section on Integrative Medicine Executive Committee and member of the Wellness Advisory Group. But that shouldn’t stop pediatricians from maintaining connections. This can be done locally or through AAP connections such as Extension for Community Healthcare Outcomes groups, collaboration sites and COVID-19 discussion boards ( login required).
“Being able to find connections with other like-minded colleagues, you’re also modeling for other people the importance of them also finding connections,” she said.
Refuel resilience
The dark days of winter can be challenging for many, which is why pediatricians should take time to figure out what refuels their resilience and identify barriers preventing them from replenishing it, said Christine Moutier, M.D., chief medical officer, American Foundation for Suicide Prevention.
“Sometimes, we react in ways that we are pleased with and other days we don’t. We don’t have to feel like that is fate,” she said. “We can actually make small tweaks that allow us to have whatever that substance is, that reservoir of resilience, that will allow us to keep drawing from that moment by moment.”
Ideas include meditating, journaling, exercising, getting outdoors and confiding with like-minded colleagues.
Dr. Moutier also cautions not to make major life decisions when extremely stressed. Pediatricians should be aware of tendencies toward anxiety or depression, shed stigmas and be proactive.
Manage your mindset
When stress reaches a boiling point, Dr. Moutier suggests trying the “Put It In Perspective” approach to redirect thoughts from irrational to rational. The approach, developed by Martin E.P. Seligman, director, University of Pennsylvania Positive Psychology Center, includes four steps:
- Ask yourself: What is the worst possible situation?
- Force yourself to think about the best outcome.
- Then consider what is most likely to happen.
- Finally, develop a plan for the most realistic scenario.
When problems fester, Dr. Moutier said, “Give yourself the gift of just a moment of time that’s set aside to work that through. Any time and effort we spend on that is going to bear fruit for us.”
Dr. Brown added, “Taking care of yourself is not selfish. It’s what’s needed in order for you to go out and then care for others.”
Resources
- Connecting with the Experts: A COVID-19 Townhall Series
- AAP Physician Health and Wellness webpage
- American Medical Association’s Steps Forward series
Source: https://www.aappublications.org/news/2020/12/02/wellness120220

Life of a COVID-19 Nurse at Harborview’s ICU | UW Medicine
Working 84-hour weeks. Isolating from children and partners. Comforting patients who are dying alone. Tending to a beloved teammate’s battle with a life-threatening illness. At Harborview Medical Center’s COVID-19 ICU, these are the new challenges that nurses take on every day during the coronavirus pandemic. Despite the stress and uncertainty, they find strength in the importance of their work. “I knew what I was getting into, and I chose it,” one nurse explains. “I was meant to be a nurse.”
*** The pandemic has hit our healthcare provider community/workforce, already globally experiencing a severe provider shortage crisis, hard and will significantly set back the development of new providers available to care for our extensive family members. The road to becoming a physician, nurse and within so many related healthcare provider specialties is often a very long hard journey, now expanded in length (months to years) due in part to a shortage of clinical opportunities to train. Please support our global healthcare community. Lives depend on it!

Still Want to Be a Doctor Post COVID-19?
How the pandemic could influence the next generation of healthcare professionals
by Jessica Gold, MD, and David Rettew, MD May 4, 2020
Every applicant to medical school has to write a personal statement. It does not have a prompt, but the understood question has always been, “Why do you want to be a doctor?”
Being a physician has always been considered a noble and honorable profession, but ever since COVID-19, physicians, along with the nurses and other healthcare professionals working on the front lines, have become bona fide heroes. The public now sees these courageous men and women risking their lives for others (sometimes without the protective equipment they need) while isolating themselves from their own families to do so.
In photos, their battle-tested faces reveal compassion and fatigue, but, perhaps more than anything, resolve. These pictures and the accounts that come with them have commanded respect and admiration, and have elevated medical professionals to new heights.
But with this adulation has come an enormous cost. As of last month, more than 200 doctors and nurses across the world have died from the novel coronavirus. Such grim numbers have shocked both the public and those already in or considering a career in healthcare. Yes, these careers involve hard work, life or death levels of responsibility, and many stressful situations, but actual danger — that’s only been there in the fine print and has been mostly avoidable for those wishing to do so, at least for those practicing in the U.S.
Until now.
In New York City hospitals and other places that have treated high numbers of COVID-19 patients, many doctors who might have reasonably believed that their career paths would have circumvented close contact with deadly viruses are finding themselves being called into action. Psychiatry residents are working in ICUs, and outpatient primary care doctors are getting enlisted to staff overflow units and field hospitals. For more risk-averse people thinking that being a physician was a cerebral and predictable line of work, it may be time to look elsewhere.
According to the Association of American Medical Colleges (AAMC), the number of applicants to medical school has been a roller coaster over the past 40 years. Since about 2003, however, there has been a steady increase in numbers. The current rise in applicants has occurred through both economic booms and recessions and has occurred despite what many have observed as an erosion in the level of trust and prestige afforded to physicians due to factors such as ties to the pharmaceutical industry and the public’s increasing attraction to “alternative” types of treatment. This rediscovered respect for doctors could make the number of applicants rise even more steeply, but there’s certainly no guarantee.
“I think with COVID-19, we just don’t know,” says Geoffrey Young, PhD, who is the AAMC’s senior director of Student Affairs and Programs and has worked on three medical school admission committees. He does not, however, predict that the current pandemic will scare off a significant amount of applicants as many applicants “at their core, have a service orientation” and “have a desire to have a positive impact on the environment around them,” he said.
For these individuals, “it’s not just a profession, it’s a calling,” Young said, noting that he wonders if there well could be an influx of medical school applications similar to the increase of people joining the armed forces after 9/11. This makes sense, as physicians have, especially lately, often been compared to soldiers, with their healthcare workspaces likened to battlefields.
On social media, a number of actual and future medical students have weighed in on this conversation. The opinions are expectedly mixed, but the majority view the pandemic as a reason to enter medicine if mostly to become an advocate for changing the system.
For example, one medical student in emergency medicine (EM) wrote, “Perhaps this reflects my bias, as someone aspiring to EM, but I feel like this is going to inspire a lot of people. Particularly people who know things could have gone better, need to go better, and want to work on making that possible.”
Another first-year medical student agreed, stating that “the next generation of doctors … tend to be enraged by the status quo. If they had an existing predilection to medicine, they’ll be even more enticed because of the opportunity for radical change.” A third-year in New York added, “I know we all see an issue and think we can change it, but this really is unprecedented and if this isn’t time to try to push the field in the right direction idk what is.”
A few premedical undergraduate students agreed, voicing that their interest and desire to go into medicine had increased as a result of COVID-19. One noted, “This has motivated me even more to be a doctor — we clearly need more physician-activists and more healthcare workers in positions of power.” A mom of a 16-year-old interested in medicine contributed by stating, “My 16-year-old daughter has always flip-flopped on [the] idea of going into medicine (infectious disease specifically) & she is now more energized & feels more sure this is what she wants to do. (I realize she’s 16 & may change, but…) I think it feels more meaningful now than ever.”
One physician poignantly wrote on Twitter, “My hope is that the outpouring of support will restore the feelings of the honorable profession that it is, rather than having people feel like replaceable worker bees. More inspiration, less desperation. One thing[s] for sure — expect change.”
Some, however, have begun to question their specialty choice or motivation for medicine altogether. A fourth-year medical student wrote, “I can imagine the numbers for Emed and IM going down for the next few years, people are naturally going to want to avoid the frontlines. Also, this might affect applications to med school as a whole. These are unprecedented times and people are rightfully spooked …Fear drives people’s actions more than anything else. Also, who wants to be in a position where you’re begging your employer for proper gear, and might be reprimanded for speaking out.”
A third-year added, “It was discouraging for ME (and I’m an MS3!) to see the mistreatment of my future colleagues … I think this will discourage those who are in it for monetary reasons or familial pressure but fuel the flame for those w/humanitarian goals.”
The last comment speaks to the possibility that while the number of applicants may not vary significantly due to the pandemic, the characteristics of those applicants will. While applicants to healthcare professions are hardly monolithic when it comes to their personality or motivations, a study in PLoS One from 2016 found that most medical students fit one of two personality profiles. One was labeled “resilient” and described students who were vigorous and industrious but a bit more on the materialistic side. The other was labeled “conscientious” and included those with higher levels of anxiety.
People with either of these profiles could get pulled in different directions when it comes to how attractive a career in medicine appears post-COVID-19. Noted personality researcher and psychiatrist Robert Cloninger, MD, PhD, who was the senior author of this study, speculates that those with the resilient profile may be “more likely to risk a dangerous job” but are also “unlikely to do things involving sacrifice for others.”
The second profile, by contrast, could be further inspired by the pandemic to help others but more concerned about their own safety. Putting it all together, it would certainly be reasonable to expect a decrease in applicants looking for secure and safe ways to make a good living and an increase in those who, as they say, like to run towards the fire.
Of course, there’s nothing wrong with the applicant pool we already have, who tend to be smart, dedicated, and compassionate people — many of whom are looking for that magic balance of a meaningful career and good job stability and security. That said, the stirring demonstrations of bravery, sacrifice, and persistence coming from the physicians and other healthcare professionals who have answered the call against the coronavirus is going to be a tough act to follow. Many of course will try, and the new crop that does may well be even more prepared to step up to our next major healthcare threat while simultaneously changing the way that healthcare is delivered.
In the years to come, there may well be a number of applicant essays that read “I want to be a doctor because of COVID-19.”
Source: https://www.medpagetoday.com/infectiousdisease/covid19/86299

INNOVATIONS
Preterm children’s long-term academic performance after adaptive computerized training: an efficacy and process analysis of a randomized controlled trial
Published: 12 September 2020 – Julia Jaekel, Katharina M. Heuser, Antonia Zapf, Claudia Roll, Francisco Brevis Nuñez, Peter Bartmann, Dieter Wolke, Ursula Felderhoff-Mueser & Britta Huening

Abstract
Background
Adaptive computerized interventions may help improve preterm children’s academic success, but randomized trials are rare. We tested whether a math training (XtraMath®) versus an active control condition (Cogmed®; working memory) improved school performance. Training feasibility was also evaluated.
Methods
Preterm born first graders, N = 65 (28–35 + 6 weeks gestation) were recruited into a prospective randomized controlled multicenter trial and received one of two computerized trainings at home for 5 weeks. Teachers rated academic performance in math, reading/writing, and attention compared to classmates before (baseline), directly after (post), and 12 months after the intervention (follow-up). Total academic performance growth was calculated as change from baseline (hierarchically ordered—post test first, follow-up second).
Results
Bootstrapped linear regressions showed that academic growth to post test was significantly higher in the math intervention group (B = 0.25 [95% confidence interval: 0.04–0.50], p = 0.039), but this difference was not sustained at the 12-month follow-up (B = 0.00 [−0.31 to 0.34], p = 0.996). Parents in the XtraMath group reported higher acceptance compared with the Cogmed group (mean difference: −0.49, [−0.90 to −0.08], p = 0.037).
Conclusions
Our findings do not show a sustained difference in efficacy between both trainings. Studies of math intervention effectiveness for preterm school-aged children are warranted.
Impact
- Adaptive computerized math training may help improve preterm children’s short-term school performance.
- Computerized math training provides a novel avenue towards intervention after preterm birth.
- Well-powered randomized controlled studies of math intervention effectiveness for preterm school-aged children are warranted.
Source: https://pubmed.ncbi.nlm.nih.gov/32919388/

What Keeps Neonatal Nurses Up at Night and What Gets Them Up in the Morning?

Walden, Marlene PhD, APRN, NNP-BC, CCNS, FAAN; Janssen, Dalton W. MSN, RNC-NIC; Lovenstein, Austin MA, BS
Editor(s): Dowling, Donna PhD, RN, Section Editors; Schierholz, Elizabeth PhD, MSN, NNP-BC, Section Editors
Advances in Neonatal Care: December 2020 – Volume 20 – Issue 6 – p E102-E110
Abstract
Background:
Occupational stress in neonatal nursing is a significant professional concern. Prolonged exposure to morally distressing patient care experiences and other healthcare issues may lead to worry among nurses. When worry becomes excessive, nurses and advanced practice registered nurses may lose joy that gives meaning to their work. Enhancing meaning in work may have a positive impact on nurse satisfaction, engagement, productivity, and burnout.
Purpose:
To explore neonatal nurses’ top professional satisfiers and top professional worries and concerns.
Methods:
A descriptive study was conducted in a convenience sample of neonatal nurses to identify the top professional satisfiers that get them up in the morning and the top professional worries and concerns that keep them awake at night.
Results:
Complete data were available for 29 neonatal nurses. The top professional satisfiers were caring for infants and families, making a difference, witnessing resilience, intellectual challenge of specialty, positive working relationships with colleagues, and educating parents and families. The top professional worries and concerns were staffing, missed care, workload, making a mistake, and failure to rescue.
Implications for Practice:
Healthcare and professional organizations must develop strategies to address occupational stress in today’s complex healthcare environment. Identifying professional worries and concerns may help nurses navigate challenging and distressing situations. Furthermore, understanding nurses’ professional satisfiers may promote personal and professional resiliency and help organizations create healthier workplace environments.
Implications for Research:
Future studies are needed to test effective interventions that may promote professional satisfaction and help neonatal nurses cope with occupational stressors.

Preterm autism spectrum disorder risk linked to changes in cerebellar white matter

Children’s National Hospital Nov 8, 2019
A study in experimental models suggests that allopregnanolone, one of many hormones produced by the placenta during pregnancy, is so essential to normal fetal brain development that when provision of that hormone decreases – as occurs with premature birth – offspring are more likely to develop autism-like behaviors. Lead study author Claire-Marie Vacher, Ph.D., explains the work of the Neonatology and Neonatal Neurology and Neonatal Neurocritical Care teams at Children’s National.

Family history is a predictor of current preterm birth
American Journal of Obstetrics & Gynecology MFM
Available online 11 November 2020, 100277 Original Research

This work was presented as a poster (number 674) at the Society for Maternal-Fetal Medicine Pregnancy Meeting, Dallas, TX, February 3, 2018.
Author links open overlay panel AmandaKoireMD, PhDabDerrick M.ChuMD, PhDbcdKjerstiAagaardMD, PhDbcde
Background
Reliable prediction of spontaneous preterm birth remains limited, particularly for nulliparous and multiparous women without a personal history of preterm birth. Although previous preterm birth is a risk factor for recurrent preterm birth, most spontaneous preterm births occur in women with no previous history of preterm birth.
Objective
This study aimed to determine whether patients’ self-reported maternal family history of preterm births among siblings and across 3 generations was an independent risk factor for spontaneous preterm births after controlling for potential confounders.
Study Design
This was a retrospective analysis of a prospectively acquired cohort using a comprehensive single, academic center database of deliveries from August 2011 to July 2017. The objective of the current analysis was to evaluate the risk of preterm birth among women with and without a family history of preterm birth. All subjects in the database were directly queried regarding familial history across 3 generations, inclusive of obstetrical morbidities. Index subjects with probable indicated preterm birth (eg, concurrent diagnosis of preeclampsia; hemolysis, elevated liver enzymes, and low platelet count; or placenta previa or placenta accreta) were excluded, as were nonsingleton pregnancies. Univariate and multivariate analyses with logistic regression were used to determine significance and adjusted relative risk.
Results
In this study, 23,816 deliveries were included, with 2345 (9.9%) born prematurely (<37 weeks’ gestation). Across all subjects, preterm birth was significantly associated with a maternal family history of preterm birth by any definition (adjusted relative risk, 1.44; P<.001), and the fraction of preterm birth occurring in women with a positive family history increased with decreasing gestational age at which the index subjects of preterm birth occurred. For nulliparous women, a history in the subject’s sister posed the greatest risk (adjusted relative risk, 2.25; P=.003), whereas for multiparous women with no previous preterm birth, overall family history was most informative (P=.003). Interestingly, a personal history of the index subject herself being born preterm presented the greatest individual risk factor (adjusted relative risk, 1.94; P=.004).
Conclusion
Spontaneous preterm birth in the current pregnancy was significantly associated with a maternal family history of preterm birth among female relatives within 3 generations and notably sisters. The risk persisted among gravidae without a previous preterm birth, demonstrating the capacity for familial history to independently predict risk of spontaneous preterm birth even in the context of a negative personal history. This study provides evidence that self-reported maternal family history is relevant in a US population cohort and across more distant generations than has previously been reported.
Source:https://www.sciencedirect.com/science/article/pii/S2589933320302706

Sensory processing patterns of young adults with preterm birth history
Ayla Günal ,Serkan Pekçetin &Çiğdem Öksüz
Pages 288-292 | Received 05 May 2020, Accepted 14 Sep 2020, Published online: 24 Sep 2020
Abstract:
Purpose/aim
This study aimed to evaluate the sensory processing abilities of young adults with a history of preterm birth and the factors affecting these abilities.
Materials and methods
Thirty-seven young adults with preterm birth history were included. After recording their sociodemographic data, sensory processing functions were evaluated using the Adolescent/Adult Sensory Profile. The participants’ data were compared to normative samples.
Results
Mean score was 43.51 ± 8.29 for sensory sensitivity, 44.45 ± 9.19 for sensation avoiding, 33.43 ± 8.45 for low registration, and 47.97 ± 9.91 for sensation seeking. Compared to normative samples, 78% of participants in sensation avoiding quadrant, 62% of participants in sensory sensitivity quadrant, 40% of participants in low registration quadrant and sensation seeking quadrant had atypical scores. When sensory profile scores were analysed according to mode of birth, percentages of typical sensory sensitivity and sensation avoiding were low in both the normal vaginal and caesarean delivery subgroups. When analysed by gestational age at birth, ratios of abnormality in sensation avoiding were similar between individuals with very early, early, and late preterm delivery history. Statistically significant difference was found in low registration and sensation avoiding quadrants according to mode of birth (p < .05). There were no statistically significant sex-based and gestational age at birth differences in any of the four quadrants of the sensory profile in the preterm group (p > .05).
Conclusion
These results showed that young adults with preterm birth history have differences in sensory processing compared to the general population and should be evaluated for sensory processing patterns.
Source:https://www.tandfonline.com/doi/abs/10.1080/08990220.2020.1824904?journalCode=ismr20
WARRIORS:

Kat’s Corner
We are a powerful and motivated community seeking health and well-being in turbulent times.
As a global community 2020 offered challenges that, like a NICU/preterm birth experience, we likely did not anticipate. We have all endured these challenges, making significant transitions while living through a global pandemic. While 2020 has separated many of us in our professional and personal realms it has also inspired us to create new solutions to a variety of complex problems.
Our hearts wept knowing many of our new family members were initially faced with prolonged separation from their babies as the pandemic emerged. Data analyses and intelligent planning eventually led to dynamic policies that offered balance and supportive care to the neonates (our brothers and sisters), their families and caregivers.
We consistently and enthusiastically search for resources that target and provide effective treatment for preverbal trauma survivors (a large part of our population). Resources for identifying, acknowledging, and providing effective treatment for preemie preverbal trauma survivors is currently dim. CALL TO ACTION 2021: We ask that the Global Healthcare Community increase attention and research while cultivating effective treatment options towards the mental health and well-being specific to our pre-verbal PTSD Warrior needs in 2021, with increased necessity!
For the families and community members: your stories, voices and engagement is vital to the progression towards health for our entire Community. Warriors: seek, with compassion, your preterm birth stories from family members. The process of sharing the experience may be healing for you as well as for your family members.
To our courageous healthcare workers, we hope that 2021 will bring about improved systems of logistical, technological, social, and resource support to empower you in the work you do each day to support the lives of those that you care for. Most of all, we Thank You for your service and wish for you abundant health and healing.
WARRIORS: Let’s take on this New Year with deep intentions to make it a Great one!

Feel The Rhythm with Shama Beckford and Ivah Wilmot
Feb 23, 2018 SURFER

They say you can’t teach style. They’re right, of course, but oh do we wish they were wrong. If silky surf aesthetics could be easily taught, then Jamaican standouts Shama Beckford and Ivah Wilmot would be welcome in front of the class. In this edit, we get a closer look at the approaches of these two magnetic surfers, whether their laying down buttery lines at Lower Trestles or over concrete in a skatepark. Beckford and Wilmot bring a unique flair to everything they do both in and out of the water, which surfing can always use more of. Keep an eye on these two up-and-coming Caribbean islanders, and be sure to take notes.

