JAPAN



Japan is an island country in East Asia. It is situated in the northwest Pacific Ocean, and is bordered on the west by the Sea of Japan, while extending from the Sea of Okhotsk in the north toward the East China Sea and Taiwan in the south. Japan is a part of the Ring of Fire, and spans an archipelago of 6852 islands covering 377,975 square kilometers (145,937 sq mi); the five main islands are Hokkaido, Honshu (the “mainland”), Shikoku, Kyushu, and Okinawa. Japan is the eleventh most populous country in the world, as well as one of the most densely populated and urbanized. Japan is a great power and a member of numerous international organizations, including the United Nations (since 1956), OECD, G20 and Group of Seven. Although it has renounced its right to declare war, the country maintains Self-Defense Forces that rank as one of the world’s strongest militaries. After World War II, Japan experienced record growth in an economic miracle, becoming the second-largest economy in the world by 1972 but has stagnated since 1995 in what is referred to as the Lost Decades. As of 2021, the country’s economy is the third-largest by nominal GDP and the fourth-largest by PPP. Ranked “very high” on the Human Development Index, Japan has one of the world’s highest life expectancies, though it is experiencing a decline in population. A global leader in the automotive, robotics and electronics industries, Japan has made significant contributions to science and technology. The culture of Japan is well known around the world, including its art, cuisine, music, and popular culture, which encompasses prominent comic, animation and video game industries.
The level of health in Japan is due to a number of factors including cultural habits, isolation, and a universal health care system. John Creighton Campbell, a professor at the University of Michigan and Tokyo University, told the New York Times in 2009 that Japanese people are the healthiest group on the planet. Japanese visit a doctor nearly 14 times a year, more than four times as often as Americans. Life expectancy in 2013 was 83.3 years – among the highest on the planet.
A new measure of expected human capital calculated for 195 countries from 1990 to 2016 and defined for each birth cohort as the expected years lived from age 20 to 64 years and adjusted for educational attainment, learning or education quality, and functional health status was published by the Lancet in September 2018. Japan had the highest level of expected human capital among the 20 largest countries: 24.1 health, education, and learning-adjusted expected years lived between age 20 and 64 years.
Source: https://en.wikipedia.org/wiki/Japan
PRETERM BIRTH RATES – Japan
Rank: 175 –Rate: 5.9% Estimated # of preterm births per 100 live births
(USA – 12 %, Global Average: 11.1%)

COMMUNITY
Resilience is at the core of each and every Neonatal Womb Warrior/Preterm Birth Community member. We have all been challenged and have responded with such great love, commitment, and to the best of our abilities.
From the perspective of a parent who has experienced the death of a preemie baby, and the rigorous commitment it took to support the ultimate well-being of a surviving preterm birth twin, the needless death of our children due to war, school shootings in the USA, lack of adequate healthcare in many global communities, including the USA, the challenges we face as we are called to navigate pandemics and global warming calls my heart to weep at times and my soul to act.
Now more than ever, we have an opportunity in our lives to step in and focus our energies on building strong and resilient solutions that protect, heal, and empower our mutual wellness through collaborative innovation. Together we can engage in creating new systems and resources to act, not react, to the issues heavily impacting our world.
The first step towards effective collaboration with our Pre-term Birth Community and the Global Community starts with a look within. As we look into our individual personal internal habitat in order to develop and secure a solid foundation to carry with us, we acknowledge our personal responsibility and ability to empower our personal well-being and to establish and maintain trust within.
The more we each seek our own health and happiness, the stronger the world becomes. Start with you and yours. Each one of us is called to travel a unique path. Follow your guidance, embrace your journey. Your happiness and well-being itself are transformative. Ultimately, action based on a foundation of love will prosper and triumph. Kathy, Kat and Gannon (the other cat).

The clinical management and outcomes of extremely preterm infants in Japan: past, present, and future
Tetsuya Isayama Division of Neonatology, Center of Maternal-Fetal Neonatal and Reproductive Medicine, National Center for Child Health and Development, Tokyo, Japan Correspondence to: Tetsuya Isayama, MD, MSc, PhD. Division of Neonatology, Center of Maternal-Fetal Neonatal and Reproductive Medicine, National Center for Child Health and Development, Tokyo, Japan. Email: isayama-t@ncchd.go.jp. Submitted Apr 10, 2019. Accepted for publication Jul 08, 2019.

Abstract: There is a wide variation in neonatal mortality rates across regions and countries. Japan has one of the lowest neonatal mortality rates in the world; in particular, the mortality rate of extremely preterm infants (i.e., those born before 26 weeks of gestation) is much lower in Japan than in other developed countries. In addition, Japan has low incidences of intraventricular hemorrhage, necrotizing enterocolitis, and late-onset sepsis, a very high incidence of retinopathy of prematurity, and a relatively high incidence of chronic lung disease. In Japan, general perinatal medical centers (PMCs), which are PMCs that offer the highest levels of care, are required to have an obstetric department with maternal-fetal intensive care units as well as a neonatal or pediatric department with neonatal intensive care units (NICU), in order to promote antenatal rather than neonatal maternal transfer of high-risk cases. The limit of viability of extremely preterm infants is 22 weeks of gestation, and approximately half of them are estimated to receive active resuscitation. The clinical management of extremely preterm infants in Japan are characterized by (I) circulatory management that is guided by neonatologist-performed echocardiography, (II) relatively invasive respiratory management, (III) nutritional management, which entails the promotion of breast milk feeding, early enteral feeding, routine glycerin enema, and the administration of probiotics, (IV) neurological management by means of minimal handling, sedation of ventilated infants, and serial brain ultrasounds, and (V) infection control with the assistance of serial C-reactive protein (CRP) monitoring. Thus, this review provides a brief description of the development of neonatology in Japan, introduces the unique features of Japanese clinical management of extremely preterm infants, and overviews their outcomes.
FULL ARTICLE

Source: https://tp.amegroups.com/article/view/27505/24536
We
this music video!

Novelbright – 愛とか恋とか [Official Music Video]
#Novelbright #愛とか恋とか #関水渚 2,332,778 views Premiered Apr 22, 2022


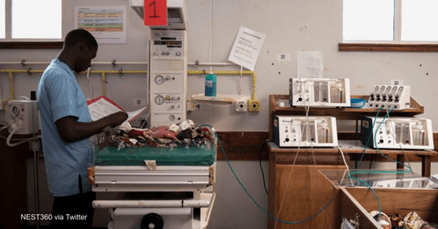
Affordable, Lightweight, Neonatal Incubators – mOm Incubators#HeroSeries

Apr 20, 2022 Innovate UK KTN
15 million babies are born prematurely every single year, and of that about 7% don’t make it due to poor healthcare. Decreasing infant mortality rates by addressing accessibility issues is at the heart of what they do at mOm incubators. CEO and product designer of mOm incubators James Roberts is rethinking the way neonatal healthcare is delivered. Their neonatal incubator is a unique solution that contrasts traditional incubators in that it is a 20 kg portable, collapsible, and accessible solution that provides flexibility to medical staff, allowing them to provide the necessary care to infants whenever and wherever it is needed, in any environment and even during transportation. As any traditional incubator, mOm incubators provide a high spec thermally stable and safe environment for premature infants. However, these particular incubators run on 100 watts in steady state, making them very energy efficient and thus have a low carbon footprint. Innovate UK’s Sustainable innovation Fund allowed the company to perform a usability study to gather data and detailed feedback on how to improve the performance of the incubator. The fund also allowed the company to test their product in a clinical setting for the first time. This technology can benefit thousands of premature babies not only throughout the UK but internationally, changing the landscape for neonatal care on a global scale through a high-tech and sustainable solution.


When a mom and baby are cuddling, talking and cooing warmly with each other, making eye contact, listening and responding to each other, they are influencing the very physiological functions that underlie their health.
Relational Health Through the Lens of Emotional Connection

“Toxic stress” as a concept has gained a firm foothold in our health discourse and even crossed over into the mainstream. That’s because we can so clearly see the physiological and behavioral effects it is having on our children.
But what do we do about it? And how do we shift our attention from merely identifying toxic stress as a problem to buffering it? How do we build healthy, resilient children and families?
The American Academy of Pediatrics released a policy statement last year that says the answer lies in fostering relational health between children and adults in pediatric primary care practice.
But how we foster relational health remains up for interpretation. As the policy statement reports, many pediatric and early childhood professionals have long recognized the vital importance of the parent-child relationship, and yet “the elemental nature of relational health is not reflected in much of our current training, research, practice, and advocacy.”
From our perspective here at the Nurture Science Program, there are three central reasons relational health has not become an integral component of pediatric care.
1. Relational Health is still largely considered psychological.
2. Most existing relational health screens look separately at parent or child, take time, and are difficult to code.
3. Within existing frameworks, such as attachment theory, each individual develops a fixed attachment style, which means it does not change. Early intervention then becomes the only hope for the developing child.
Through our lens and work on autonomic emotional connection, we hope to provide a practical, scalable solution.
1. Relational health is biological, physiological, and interpersonal.
Over decades of research we have uncovered that there is something happening between mother and infant when they get emotionally connected—not just in the brain, but on a deep body-to-body level, which is where we can observe and measure it. That is why we call it autonomic emotional connection.
The autonomic nervous system is the nervous system that modulates our stress response; it makes our hearts beat and lungs breathe without our having to think about it; these processes regulate our emotional behavior. When mom and baby are emotionally connected on the autonomic level, they are actually regulating each other’s heart rates and hormones and positively affecting each other’s stress responses. In other words, when a mom and baby are cuddling, talking and cooing warmly with each other, making eye contact, listening and responding to each other, they are influencing the very physiological functions that underlie their health.
It sounds strange, I know. We don’t think of things like cuddling and cooing as science—but they are behavioral manifestations of essential physiological and biological processes happening between two bodies.
And the impacts these behaviors have on our physiology are profound. Through our randomized control trial of Family Nurture Intervention (FNI) in NICU, we found that engaging mothers and children in autonomic emotional connection dramatically improves babies’ development, sleep, stress resilience, attention, cognitive, learning, and language scores. Mothers also saw improved mental health and lower cardiac risk. Five years later, both mother and child still had better physiological regulation and stress resilience (which is important when we’re worried about the effects of toxic stress).
Once parent-facing professionals can understand that relational health produces physiological outcomes and observable behaviors—rather than being an ephemeral concept—they can seamlessly integrate relational health observation into an office visit where they are already checking vital signs and motor skills.
All they need is a brief observational tool that evaluates parent and child in relationship with each other.
2. To measure relational health, we need to observe parent and child interacting with each other face-to-face.
Unlike existing relational health screens that only look at the child or the parent, the Welch Emotional Connection Screen (WECS) focuses on the behaviors between parent and child. It is a quick (20-30 second), easy to use, non-invasive, validated screen that a parent-facing professional can employ while observing a mother and infant interacting face-to-face with the child on the parent’s lap.
The WECS organizes the visible behaviors of their relationship into the following four domains:
- Mutual Attraction (Do mom and baby want to be close to each other?)
- Vocal Communication (Is their vocal tone warm and engaging?)
- Facial Expressiveness (Are they trying to communicate using their faces?)
- Reciprocity (Are they sensitive to each other’s expressed emotions? Do they follow-up with each other?)
In clinical research, pairs who exhibit all of the above receive a high WECS score. And in mother-baby pairs with high WECS scores, we see improved neurobehavioral outcomes, both short and long-term.
In widespread practice, a parent-facing professional can use the WECS, even without formally scoring it, to help identify the families that can most benefit from support.
3. Emotional connection is a state not a trait.
The fact that emotional connection is a state between two people and not a trait of just one person is the most hopeful takeaway from our work. It means we are not fully “baked” with a maladaptive attachment style based on whether our needs were met in childhood. It means your toddler with behavioral problems is not destined to always have behavioral problems. No matter our age or life experience, we can enter into a state of emotional connection and share its health benefits.
Fortunately, the very same behaviors that the WECS observes can also be used to get two people connected—by conditioning the underlying physiological mechanisms of relational health. The context is still sensory—physical touch, eye contact, vocal communication—but the activity is emotional expression.
In a pediatric primary care setting, the intervention is brief: emotional exchange between parent and child, with the child sitting on the parent’s lap. Parents respond to a prompt on an emotional topic (such as “tell your child the story of how you picked their name,” or “tell your child the story of their birth”), in their primary language. The prompt works when it elicits deep emotional expression from the parent.
During FNI (an intervention used in extreme cases, such as preterm birth), mothers are guided through what we call calming cycles. A nurture specialist prompts mothers to express their feelings to their babies while engaging their senses (e.g. skin-to-skin, making eye contact, etc). This emotional expression engages the child’s orienting reflex, and often prompts some kind of response (their oxygen saturation may go up or they may look at their mom for the first time). This cycle continues as parent and child move from mutual states of distress to mutual states of calm. Once calm and connected, we can see evidence that their physiological co-calming mechanism (what we call co-regulation) is in effect. Any further nurturing interactions between them will continue to strengthen and condition that mechanism.
We hypothesize that the mechanism of co-regulation underlies and facilitates all of the physiological improvements, developmental gains, and emotional and mental well-being we see in our results. And because emotional connection and co-regulation feel good, moms and babies will continue to do these sensory and emotional activities, not because they have been told to, but because they want to. That may be part of why mothers and children show physiological benefits related to stress resilience (HRV) even 5 years after the intervention.
It’s Time for a Paradigm Shift
The quality of our relationships can alter the landscape of our physical and mental health, lifelong. Relational health, it turns out, is an absolutely essential part of our wellbeing, and we can foster it by looking through the lens of autonomic emotional connection.
When we do so, we will see that relational health is behavioral and can be observed; its impacts are physiological and can be measured; and it is a state that we move in and out of with our loved ones throughout our lifetimes. The reason to start early, and to target the mother-infant relationship as a mediator of positive effects on relational health, is not merely to prevent later problems, it is to experience maximum benefit at every stage of our lives.
This paradigm shift would necessarily impact the way that health conditions are viewed and treated: by creating environments and relationships capable of fostering the growth and health we all deserve.
Disseminating these tools and practices to researchers, clinicians, and parent-educators has the potential to help children and their families experience deep autonomic emotional connection with each other—opening the door to intergenerational health and thriving.

PREEMIE FAMILY PARTNERS

When can babies go home from the NICU
Jul 5, 2020 The NICU Doc
Do you want to know when can babies go home from the NICU? You have been in the NICU for days, weeks, sometimes even months and you are SO CLOSE! Find out what things need to happen for your baby to be discharged from the NICU. How can you best prepare to be ready for the day of discharge. What actually happens the day of discharge? The NICU Doc will go over the things that your baby and you need to be doing to be ready for discharge. And also, I will go over the events of the day of discharge.
*Disclaimer: Although I work in an academic institution and unless stated, the videos posted are of my sole creation. Any opinions, comments, or postings are not a representation or a reflection of our institutions. **Any medical advice or topics discussed are NO substitute for your physician’s advice and care. Actions taken on advice from the videos are done so at your own risk.
CPR Training of Parents of Preterm Babies before Discharge – Experience from a Tertiary Care NICU
Mathew Jisha, MBBS, DNB, Nagar Nandini, MBBS, DCH, DNB, Rajagopal Kumar Kishore, MBBS, DCH, MD, FIAP, DCH, MRCP, FRCPCH, FRCPI, FRACP, FNNF, MHCD

Abstract:
Objectives: To evaluate the feedback of CPR training given to parents of preterm babies discharged from the NICU.
Methods: This was a retrospective study conducted using a questionnaire sent to parents of preterm neonates admitted to a neonatal intensive care unit (NICU) from January 2007 to May 2020. All parents of newborns under 30 weeks gestation who survived to discharge were considered eligible. Parents were given CPR training on a manikin by a Neonatal resuscitation provider (NRP) certified doctor. Babies less than 30 weeks were sent home with a disposable bag and mask after the training of the parents. The responses thus received were analysed.
Results: We analysed data from 60 responses (48.3%). 85% of the parents were given one-on-one training, the rest as classroom training. 68.3% felt that the addition of video demonstrations would be beneficial. 95% of parents said that the training helped increase their confidence in taking care of their babies. 78% felt it did not add to unnecessary parental anxiety. 5 babies received CPR at home, and all were told that the home CPR was successful on assessment at the hospital after the episode. 65% felt a repeat training would be helpful. All the parents educated about CPR opined that this training is essential for discharge preparation.
Conclusion: We conclude that parental CPR training backed by video demonstration prior to the instructor-led session and followed by repeat training after 3 months is desirable in the holistic care of preterm babies post-discharge.
Key Message – Routine CPR education of parents of preterm neonates, backed by video demonstration and repetition of training after 3 months is desirable; it improves the confidence of parents and reduces anxiety in the care of their premature infants.
Introduction: Cardiopulmonary resuscitation (CPR) is an emergency lifesaving procedure performed when the heart stops beating. Around the turn of the 20th century, preterm infants were discharged only when they achieved a certain weight, typically 2000 gm(5lb). Studies have shown that preterm neonates can be sent home earlier without adverse health effects based on physiologic criteria rather than body weight. Evidence has shown that preterm neonates with low birth weight who require neonatal intensive care experience a much higher rate of hospital readmission and sudden deaths during the first year after birth than healthy term infants. The most important predictor of infant survival from an acute life-threatening event (ALTE) is the time from cardiopulmonary arrest to resuscitation. More so in neonates, this is the case, who are likely to suffer a respiratory arrest that responds quickly to resuscitation. This emphasizes the importance of systematic preparation for discharge and good follow-up thereafter of high-risk preterm neonates to reduce the chances of such life-threatening events.
Preterm neonates should demonstrate some physiologic competencies before being discharged from the hospital. These include oral feeding sufficient to support appropriate growth, thermoregulation in a home environment, and sufficiently mature respiratory control. The first two are usually achieved around 34-36 weeks’ postmenstrual age, but the maturation of respiratory control to the point that allows safe discharge may occasionally take up to 44 weeks’ postmenstrual age. Infants born as very or extremely preterm and have a prolonged and complicated stay in the hospital tend to take longer to achieve these competencies. But they may be discharged home much earlier if they exhibit thermostability and reasonable weight gain, as plotted on the Fenton’s growth chart. NICU graduates are discharged when they satisfy the above criteria. Their parents have demonstrated the necessary skills to provide all care components at home, including CPR should the need arise.
At the time of discharge, most parents lack confidence and are anxious about their capability to handle the babies at home. Hence, we thought that our intervention of training parents of neonates born at home. Hence, we thought that our intervention of training parents of neonates born < 34 weeks would help in the holistic care of these babies, including handling emergencies at home post-discharge. Many studies have emphasized that pre-discharge infant cardiopulmonary resuscitation training is essential or highly desirable. As shown by literature, it is a routine pre-discharge requirement in most developed countries, but this training is not reported or published in our country. Based on our hospital protocols, we initiated this training at its inception 13 years ago. We wanted to review our data over these years to see if it has made an impact or a difference.
Materials and methods: This retrospective study was conducted at a tertiary care neonatal intensive care unit in India from January 2007 to May 2020. Informed consent for the survey was taken, and the Institutional Review Board approved the study. Initially, only parents of babies less than 30 weeks gestation were being given the training to perform CPR; however, since December 2019, due to a change in the unit protocol, all parents of babies with gestational age less than 34 weeks were admitted to the NICU were trained and included in the study. Babies (less than 30 weeks initially and less than 34 weeks later), deceased, and babies more than these respective gestational age groups were excluded. Parents of these babies were given CPR training (AHA NRP guidelines) in a language they could understand using a manikin, on the day of the transfer to wards or discharge from the NICU, by an NRP-certified doctor who is recertified every 2 years. The training included a brief description of CPR, when it needed to be initiated, and the steps of CPR, and ended with a physical demonstration of the same on a manikin. Parents were also given a chance to practice the steps on the manikin. Each session lasted around 20 minutes. At no additional cost, a new disposable self-inflating bag and mask were procured for each of these neonates and sent home at discharge after their parents underwent CPR training. The authors prepared a questionnaire/survey in English or the local language on request, with 22 questions. Parents were first called and spoken to and were then messaged a web link to complete this survey. All parents had access to the internet and the necessary device. The data from the survey was later analysed and reported.
Results: During the study period, parents of 126 preterm babies were trained, out of which parents of 84 neonates were attempted to be contacted. The overall response rate to the survey was 71.4%, as shown in Figure 1. We analysed the data of 60 responses we received, and the following results refer to only those that participated in the survey. 46.6% of the babies were between 32-34wks as seen in Table 1. 27 were twins (with one survivor of a pair), and the rest were singleton babies. 85% of the parents were given one-on-one training, the rest as classroom training; however, only 23% of these parents perceived that classroom training may be better than one-on-one training. A majority of 95% found that the training given was easy to follow, and 68.3% thought that providing a video demonstration and one-on-one training would be more helpful. Bag and mask were used in 58% for demonstration. Only manikins with the demonstration of mouth-to-mouth breathing and chest compressions were used for the rest. 63.3% of parents thought it would be good to use a bag and mask for training. Of the total number who responded, 92% understood in what way CPR helped babies in an acute life-threatening event. 90% of them felt that they could identify when their babies required CPR.
Most parents (95%) said that the training helped increase their confidence in taking care of their babies. 78% felt it did not add to unnecessary parental anxiety. 5 babies received CPR at home. Of these babies, 3 received CPR in the first week after discharge and 2 after a month since discharge from the hospital, as shown in Table 2. 4 recovered from the episode quickly following home CPR. All parents correctly followed the steps as they had been advised to initiate CPR according to the assessment at the hospital after the episode. These parents, who found themselves in a situation that needed CPR, felt that they could execute it as taught. 67% of parents said that after three months, they could still recollect the steps of CPR taught during the training session. The need for repetition of training was felt by 65%, and they opined that it should be conducted after a time interval of 3 months since the last session. All 60 parents educated on CPR thought that this training is an essential part of discharge preparation.
Discussion: The American Heart Association (AHA) educates more than 9 million persons annually about CPR. Parents need to be trained in infant CPR. In the United States, 2230 infants (<1 yr. of age) died of sudden infant death syndrome (SIDS) in 2005, making it the third leading cause of death there. Drake et al. found that parents considered CPR a priority when asked to rank discharge teaching topics in order of importance.
We chose to do this study as CPR training is an important aspect of pre-discharge preparation for parents of preterm babies, as has been shown previously. Still, it is not routinely being done in most hospitals in our country, as evidenced by the lack of literature on the same. We hypothesised that getting feedback from parents who had received training in infant CPR would give us an overview of the effectiveness and scope for improvement of what we consider an essential practice.
Conventionally, CPR is taught using a combination of didactic instruction and hands-on practice, followed by a written test. Most of our parents had one-on-one training sessions, occasionally a group training. It was a manual demonstration, and in response to the questionnaire, parents did express that a video-backed demonstration would be more helpful. Brannon et al. used an instructional video as an adjunct to the instructor-led demonstration. The group concluded that CPR is a psychomotor skill, so learning it requires more than just acquiring knowledge. Practice with a manikin is essential to ensure competence. An effective video instruction, while most likely cannot totally replace an instructor-led class, could be helpful in learning infant CPR. A literature review by Parsons et al. opined that teaching infant CPR to parents of high-risk neonates is considered beneficial in decreasing mortality. However, the evidence for this is very limited. The overall trend is supportive of CPR training. It increases parental confidence and decreases anxiety levels. Parents’ memory of knowledge regarding CPR decreases over time. Our survey also showed similar findings. At discharge, the training did seem to have boosted their confidence in taking care of their newborn, and it did not add to the overall anxiety among most parents. In those instances where CPR was required at home, parents could resuscitate and then bring their infant to the hospital for continuing care. It was heartening to learn that the training was hugely successful, considering that most parents had understood when to use CPR and how it helps resuscitate. The aim is to increase this to 100%. Parents of one baby who required home CPR could not self-assess the effectiveness of CPR given. Henceforth, our training should also focus on educating parents on assessing the baby post-resuscitation. All parents were given adequate pre-discharge teaching regarding other aspects of their preemies’ care and the resuscitation training that we provided. Wintch et al. showed that 80% of their subjects who required CPR post-discharge survived complete resuscitation efforts after full cardiopulmonary arrest and were neurologically intact. In all of our 5 babies who required home CPR, parents had correctly followed the steps as they had been advised to initiate CPR as per the post-resuscitation assessment done once they reached the hospital.
The AHA gives CPR training kits to parents of high-risk neonates at discharge at a nominal fee. Providing these kits to carry home may also be useful. Hence, we also provide a complimentary manual resuscitator kit with masks of two sizes to parents of those born <30 wks., and neonates born at 30-34 weeks who are discharged after a very stormy course in NICU.
The inability to retain learned CPR skills has been researched. Studies have documented deficits in retention and performance skills beginning as early as 2 weeks after initial instruction, with continued deterioration up to one year later. The peak incidence of SIDS occurs between 1 and 4 months of age, so long-term retention of infant CPR skills is critical. Therefore, it has been reported that 3 to 6 months after initial instruction is the optimal timeframe for recertification. Most of our parents, too, felt the need for a repeat training session 3 months after the first one.
The limitation of this study was the sample size, which could have been better. The contact details of many parents were either changed or unavailable. There is also an element of recall bias as the survey was conducted after a long time for some. One of the main reasons for more responses from parents in recent years was a better recall. As it was a retrospective study, contacting and convincing parents to take the survey was arduous. Not all parents agreed to participate. Some did not receive phone calls and some responded by saying they were busy and would not be able to complete the survey. Also, during the study period, there was a change in unit protocol, and parents of all preterms, 34 wks. were being trained instead of those only <30 wks. as was done previously. We noticed that there were babies in the gestational age group of 30-34weeks who had episodes of apnoea at home and thereby changed the Unit protocol to include these parents to improve outcomes in these babies. The study’s strengths were the simplicity of the survey method used and the number of responses we received, considering that the oldest of the babies whose parents responded was born 13 years ago.
Conclusion: Our study shows that parental CPR education seems to have improved their confidence in the care of these preemies and has not added to general parental anxiety. All parents also agreed that it is an essential step in the pre-discharge planning of preterm babies. Parental CPR training backed by video demonstration before the instructor-led session and followed by repeat training after 3 months is vital in the holistic care of preterm babies post-discharge and is highly recommended at all centres catering to this major subgroup of neonates admitted to the NICU.
*** Access in-person and online training through numerous resources worldwide- Ask your health care provider
PLEASE ENTER HERE TO ACCESS GRAPHS/CHARTS

Source:http://neonatologytoday.net/newsletters/nt-may22.pdf

Day in the life of a DOCTOR: Shadowing NICU NURSE PRACTITIONER (ft. premature babies)
Babies born at 22 weeks (5.5 months) can survive!! Join me in the largest NICU in Canada and learn about the lifesaving treatments for premature babies! I’ll be shadowing Nikki, a nurse practitioner who works in the neonatal ICU. Plus you’ll meet baby Kalani who was born at 23 weeks and her mother, Paola.



The National Coalition for Infant Health explains why all preemies — regardless of how prematurely they’re born or what challenges they face — deserve proper care and appropriate health coverage.
The National Coalition for Infant Health explains why all preemies — regardless of how prematurely they’re born or what challenges they face — deserve proper care and appropriate health coverage.


The science of nurturing and its impact on premature babies

May 31, 2017
A long-term study on helping preterm babies, using the simplest of interventions, is showing signs of promise. In part two of our story, William Brangham explores the study’s outcomes, as well as questions about the complex past of the doctor behind it.


HEALTH CARE PARTNERS

Preterm birth and Kawasaki disease: a nationwide Japanese population-based study

Published: 08 October 2021
Abstract
Background
Previous studies showed that preterm birth increased the risk for hospital admissions in infancy and childhood due to some acute diseases. However, the risk of preterm children developing Kawasaki disease remains unknown. In the present study, we investigate whether preterm birth increased the morbidity of Kawasaki disease.
Methods
We included 36,885 (34,880 term and 2005 preterm) children born in 2010 in Japan. We examined the association between preterm birth and hospitalization due to Kawasaki disease using a large nationwide survey in Japan.
Results
In log-linear regression models that were adjusted for children’s characteristics (sex, singleton birth, and parity), parental characteristics (maternal age, maternal smoking, paternal smoking, maternal education, and paternal income), and residential area, preterm infants were more likely to be hospitalized due to Kawasaki disease (adjusted risk ratio: 1·55, 95% confidence interval: 1.01–2.39). We then examined whether breastfeeding status modified the potential adverse effects of preterm birth on health outcome. Preterm infants with partial breastfeeding or formula feeding had a significantly higher risk of hospitalization due to Kawasaki disease compared with term infants with exclusive breastfeeding.
Conclusions
Preterm infants were at a high risk for Kawasaki disease, and exclusive breastfeeding might prevent this disease among preterm infants.
Impact
- Previous studies showed that preterm birth increased the risk for hospital admissions in infancy and childhood due to some acute diseases, however, the risk of preterm children developing Kawasaki disease remains unknown.
- This Japanese large population-based study showed that preterm infants were at a high risk for Kawasaki disease for the first time.
- Furthermore, this study suggested that exclusively breastfeeding might prevent Kawasaki disease among preterm infants. Full Study available.
Source: https://www.nature.com/articles/s41390-021-01780-4

Relationships between overwork, burnout and suicidal ideation among resident physicians in hospitals in Japan with medical residency programmes: a nationwide questionnaire-based survey

2022 Mar 10;12(3):e056283. doi: 10.1136/bmjopen-2021-056283.Masatoshi Ishikawa 1 2
Abstract
Objectives: This study examined the relationships between overwork, burnout and suicidal ideation among resident physicians working in hospitals throughout Japan.
Design: A nationwide, questionnaire-based survey.
Setting: Participating hospitals (n=416) were accredited by the Japanese Medical Specialty Board to offer medical residency programmes in 19 core specialties. Surveys were conducted in October 2020.
Participants: Valid responses were obtained from 4306 physicians (response rate: 49%).
Outcome measures: Items pertaining to the Japanese Burnout Scale, depressive tendencies and suicidal ideation were included in questionnaires. Multiple regression analyses were performed: suicidal ideation was the response variable; sex, age, core specialty, marital status, income, weekly working hours and workplace (ownership, number of beds, number of full-time physicians and regional classification) were explanatory variables.
Results: Regarding the Japanese Burnout Scale, the highest score was recorded for ‘sense of personal accomplishment’, followed by ’emotional exhaustion’ and ‘depersonalization’. Increased emotional exhaustion and depersonalisation were associated with longer working hours, but there was no such trend for sense of personal accomplishment. Depressive tendencies and suicidal ideation were noted in 24.1% and 5.6% of respondents, respectively. These percentages tended to increase when respondents worked longer hours. Several factors were significantly associated with suicidal ideation: female sex (reference: male, OR: 2.08, 95% CI: 1.56 to 2.77), ≥12 million yen income (reference: <2 million yen, OR: 0.21, 95% CI: 0.05 to 0.79), ≥100 working hours/week (reference:<40 hours/week, OR: 3.64, 95% CI: 1.88 to 7.04) and 600-799 hospital beds (reference: <200 beds, OR: 0.23, 95% CI: 0.07 to 0.82).
Conclusions: Many Japanese residents demonstrated a tendency to experience burnout and suicidal ideation. Female sex, low income, long working hours and insufficient hospital beds were associated with suicidal ideation. To ensure physicians’ health and patients’ safety, it is necessary to advance workstyle reform for physicians.
<a href=”http://Abstract Objectives: This study examined the relationships between overwork, burnout and suicidal ideation among resident physicians working in hospitals throughout Japan. Design: A nationwide, questionnaire-based survey. Setting: Participating hospitals (n=416) were accredited by the Japanese Medical Specialty Board to offer medical residency programmes in 19 core specialties. Surveys were conducted in October 2020. Participants: Valid responses were obtained from 4306 physicians (response rate: 49%). Outcome measures: Items pertaining to the Japanese Burnout Scale, depressive tendencies and suicidal ideation were included in questionnaires. Multiple regression analyses were performed: suicidal ideation was the response variable; sex, age, core specialty, marital status, income, weekly working hours and workplace (ownership, number of beds, number of full-time physicians and regional classification) were explanatory variables. Results: Regarding the Japanese Burnout Scale, the highest score was recorded for ‘sense of personal accomplishment’, followed by ’emotional exhaustion’ and ‘depersonalization’. Increased emotional exhaustion and depersonalisation were associated with longer working hours, but there was no such trend for sense of personal accomplishment. Depressive tendencies and suicidal ideation were noted in 24.1% and 5.6% of respondents, respectively. These percentages tended to increase when respondents worked longer hours. Several factors were significantly associated with suicidal ideation: female sex (reference: male, OR: 2.08, 95% CI: 1.56 to 2.77), ≥12 million yen income (reference: <2 million yen, OR: 0.21, 95% CI: 0.05 to 0.79), ≥100 working hours/week (reference:<40 hours/week, OR: 3.64, 95% CI: 1.88 to 7.04) and 600-799 hospital beds.)
Source: https://pubmed.ncbi.nlm.nih.gov/35273058/

Protecting workers’ health and safety: Online training resources at your fingertips
28 April 2022

Everyone deserves to work in a place that is healthy and safe. Each year on 28 April, we celebrate World Day for Safety and Health at Work to raise awareness of this right and the steps we can take to ensure it is a reality for workers across the globe.
Training is key. Nearly half of the world’s population works. Providing workers with the latest occupational health and safety knowledge can help protect them from work-related injuries, diseases and deaths. This is especially important during public health emergencies like the COVID-19 pandemic.
Workplaces have played an important role in both the spread and mitigation of COVID-19. Health workers of all kinds have been particularly affected by the pandemic. Not only have they been sick, they have suffered adverse effects of prolonged use of personal protective equipment, fatigue and mental health problems, violence and harassment and exposure to hazardous disinfectants.
The pandemic has stimulated many work settings around the world to expand telework and hybrid work arrangements. All these can impact the health, safety and wellbeing of workers.
So the World Health Organization (WHO) is offering free online courses on these topics on its OpenWHO.org learning platform. Materials are available in multilingual and low-bandwidth formats to maximize access.
WHO has also collaborated with partners like the International Labour Organization (ILO) on additional training materials to protect health workers and responders and prepare workplaces for future health emergencies. To access these learning resources, please visit the links below.
- COVID-19 and work: Staying healthy and safe at work during the COVID-19 pandemic (OpenWHO): This course is intended to guide workers and their representatives, business leaders, managers, as well as occupational health and safety professionals in protecting their workplace during the COVID-19 pandemic.
- Healthy and safe telework (OpenWHO): This course provides guidance to teleworkers and their managers on protecting and promoting health and wellbeing while teleworking.
- Occupational health and safety for health workers in the context of COVID-19 (OpenWHO): All health workers require knowledge and skills to protect themselves and others from the occupational risks they encounter, so that they can work safely and effectively. This course consists of five sections in response to these needs.
- All-Hazard Rapid Response Teams Training Package (WHO Health Security Learning Platform): The all-hazard Rapid Response Teams Training Package is a structured comprehensive collection of training resources and tools enabling relevant training institutions to organize, run and evaluate face-to-face training for Rapid Response Teams tailored to country specific needs.
- Occupational safety and health in public health emergencies: a manual for protecting health workers and responders (WHO/ILO publication): This manual provides an overview of the main occupational safety and health risks faced by emergency responders during disease outbreaks and other emergencies, such as natural disasters, chemical incidents, radiological emergencies and emergencies involving conflicts. The intent is to assist organizations and workplaces to better prepare and respond to these events.
- HealthWISE – Work Improvement in Health Services (ILO/WHO publication): HealthWISE is a practical, participatory quality improvement tool for health facilities. The HealthWISE package consists of an Action Manual and a Trainers’ Guide to combine action and learning. Topics include occupational safety and health, personnel management and environmental health.
Source:https://www.who.int/news-room/feature-stories/detail/protecting-workers–health-and-safety–online-training-resources-at-your-fingertips

New Survey Shows That Up To 47% Of U.S. Healthcare Workers Plan To Leave Their Positions By 2025
Jack Kelly Senior Contributor Apr 19, 2022

The Covid-19 pandemic unleashed wave after wave of challenges and feelings of burnout for United States healthcare workers, and unless changes are made to the industry, nearly half plan to leave their current positions, according to a new report examining the work environment and industry’s future for clinicians.
Elsevier Health, a provider of information solutions for science, health and technology professionals, conducted its first “Clinician of the Future” global report. It revealed current pain points, predictions for the future and how the industry can come together to address gaps—including that 31% of clinicians globally, and 47% of U.S. healthcare workers, plan to leave their current role within the next two to three years.
Dr. Charles Alessi, chief clinical officer at Healthcare Information and Management Systems Society (HIMSS), said, “As a practicing doctor, I am acutely aware of the struggles today’s clinicians face in their efforts to care for patients.” Alessi continued, “This comprehensive report from Elsevier Health provides an opportunity for the industry to listen—and act—on the pivotal guidance given by those on the frontlines. I commend this important initiative and look forward to next steps in supporting our doctors and nurses.”
In the new report from Elsevier Health, published two years after the Covid-19 pandemic began, thousands of doctors and nurses from across the globe revealed what is needed to fill gaps and future-proof today’s healthcare system. The comprehensive “Clinician of the Future” report was conducted in partnership with Ipsos and uncovered how undervalued doctors and nurses feel, as well as their call for urgent support, such as more skills training—especially in the effective use of health data and technology—preserving the patient-doctor relationship in a changing digital world and recruiting more healthcare professionals into the field. The multiphase research report not only understands where the healthcare system is following the Covid-19 pandemic, but where it needs to be in 10 years to ensure a future that both providers and patients deserve.
Jan Herzhoff, president at Elsevier Health, said, “Doctors and nurses play a vital role in the health and well-being of our society. Ensuring they are being heard will enable them to get the support they need to deliver better patient care in these difficult times.” Herzhoff added, “We must start to shift the conversation away from discussing today’s healthcare problems to delivering solutions that will help improve patient outcomes. In our research, they have been clear about the areas they need support; we must act now to protect, equip and inspire the clinician of the future.”
There has never been a greater need for lifting the voices of healthcare professionals. The global study found 71% of doctors and 68% of nurses believe their jobs have changed considerably in the past 10 years, with many saying their jobs have gotten worse.
The “Clinician of the Future” report includes a quantitative global survey, qualitative interviews and roundtable discussions with nearly 3,000 practicing doctors and nurses around the world. The data helps shed light on the challenges impacting the profession today and predictions on what healthcare will look like in the next 10 years, according to those providing critical patient care.
According to the report, 56% of respondents said that there has been growing empowerment amongst patients within the last 10 years, as people take charge of their health journeys. When referring to soft skills, 82% said that it’s important for them to exhibit active listening and empathy to the people they serve. Furthermore, nearly half of clinicians cite the allocated time they have with patients as an issue, as only 51% believe that the allotted time allows them to provide satisfactory care.
To ensure a positive shift moving into the future and to fill current gaps, clinicians highlight the following priority areas for greater support:
- Clinicians predict that over the next 10 years “technology literacy” will become their most valuable capability, ranking higher than “clinical knowledge.” In fact, 56% of clinicians predict they will base most of their clinical decisions using tools that utilize artificial intelligence. However, 69% report being overwhelmed with the current volume of data and 69% predict the widespread use of digital health technologies to become an even more challenging burden in the future. As a result, 83% believe training needs to be overhauled so they can keep pace with technological advancements.
- Clinicians predict a blended approach to healthcare with 63% saying most consultations between clinicians and patients will be remote and 49% saying most healthcare will be provided in a patient’s home instead of in a healthcare setting. While clinicians may save time and see more patients, thanks to telehealth, more than half of clinicians believe telehealth will negatively impact their ability to demonstrate empathy with patients they no longer see in person. As a result, clinicians are calling for guidance on when to use telehealth and how to transfer soft skills like empathy to the computer screen.
- Clinicians are concerned about a global healthcare workforce shortage, with 74% predicting there will be a shortage of nurses and 68% predicting a shortage of doctors in 10 years’ time. This may be why global clinicians say a top support priority is increasing the number of healthcare workers in the coming decade. Clinicians require the support of larger, better-equipped teams and expanded multidisciplinary healthcare teams, such as data analysts, data security experts and scientists, as well as clinicians themselves.
“While we know that many nurses are leaving the profession due to burnout, we also know that the pandemic has inspired others to enter the field because of a strong desire for purposeful work,” said Marion Broome, Ruby F. Wilson professor of nursing at Duke University’s School of Nursing. “We must embrace this next wave of healthcare professionals and ensure we set them up for success. Our future as a society depends on it.”
Looking To The Future
“Ultimately, we asked clinicians for what they need, and now it’s our responsibility as a healthcare industry to act,” said Dr. Thomas “Tate” Erlinger, vice president of clinical analytics at Elsevier Health. “Now is the time for bold thinking—to serve providers and patients today and tomorrow. We need to find ways to give clinicians the enhanced skills and resources they need to better support and care for patients in the future. And we need to fill in gaps today to stop the drain on healthcare workers to ensure a strong system in the next decade and beyond.”
INNOVATIONS
Artificial Intelligence Getting Smarter! Innovations from the Vision Field

Posted on February 8th, 2022 by Michael F. Chiang, M.D., National Eye Institute
One of many health risks premature infants face is retinopathy of prematurity (ROP), a leading cause of childhood blindness worldwide. ROP causes abnormal blood vessel growth in the light-sensing eye tissue called the retina. Left untreated, ROP can lead to lead to scarring, retinal detachment, and blindness. It’s the disease that caused singer and songwriter Stevie Wonder to lose his vision.
Now, effective treatments are available—if the disease is diagnosed early and accurately. Advancements in neonatal care have led to the survival of extremely premature infants, who are at highest risk for severe ROP. Despite major advancements in diagnosis and treatment, tragically, about 600 infants in the U.S. still go blind each year from ROP. This disease is difficult to diagnose and manage, even for the most experienced ophthalmologists. And the challenges are much worse in remote corners of the world that have limited access to ophthalmic and neonatal care.
Artificial intelligence (AI) is helping bridge these gaps. Prior to my tenure as National Eye Institute (NEI) director, I helped develop a system called i-ROP Deep Learning (i-ROP DL), which automates the identification of ROP. In essence, we trained a computer to identify subtle abnormalities in retinal blood vessels from thousands of images of premature infant retinas. Strikingly, the i-ROP DL artificial intelligence system outperformed even international ROP experts [1]. This has enormous potential to improve the quality and delivery of eye care to premature infants worldwide.
Of course, the promise of medical artificial intelligence extends far beyond ROP. In 2018, the FDA approved the first autonomous AI-based diagnostic tool in any field of medicine [2]. Called IDx-DR, the system streamlines screening for diabetic retinopathy (DR), and its results require no interpretation by a doctor. DR occurs when blood vessels in the retina grow irregularly, bleed, and potentially cause blindness. About 34 million people in the U.S. have diabetes, and each is at risk for DR.
As with ROP, early diagnosis and intervention is crucial to preventing vision loss to DR. The American Diabetes Association recommends people with diabetes see an eye care provider annually to have their retinas examined for signs of DR. Yet fewer than 50 percent of Americans with diabetes receive these annual eye exams.
The IDx-DR system was conceived by Michael Abramoff, an ophthalmologist and AI expert at the University of Iowa, Iowa City. With NEI funding, Abramoff used deep learning to design a system for use in a primary-care medical setting. A technician with minimal ophthalmology training can use the IDx-DR system to scan a patient’s retinas and get results indicating whether a patient should be sent to an eye specialist for follow-up evaluation or to return for another scan in 12 months.
Many other methodological innovations in AI have occurred in ophthalmology. That’s because imaging is so crucial to disease diagnosis and clinical outcome data are so readily available. As a result, AI-based diagnostic systems are in development for many other eye diseases, including cataract, age-related macular degeneration (AMD), and glaucoma.
Rapid advances in AI are occurring in other medical fields, such as radiology, cardiology, and dermatology. But disease diagnosis is just one of many applications for AI. Neurobiologists are using AI to answer questions about retinal and brain circuitry, disease modeling, microsurgical devices, and drug discovery.
If it sounds too good to be true, it may be. There’s a lot of work that remains to be done. Significant challenges to AI utilization in science and medicine persist. For example, researchers from the University of Washington, Seattle, last year tested seven AI-based screening algorithms that were designed to detect DR. They found under real-world conditions that only one outperformed human screeners [3]. A key problem is these AI algorithms need to be trained with more diverse images and data, including a wider range of races, ethnicities, and populations—as well as different types of cameras.
How do we address these gaps in knowledge? We’ll need larger datasets, a collaborative culture of sharing data and software libraries, broader validation studies, and algorithms to address health inequities and to avoid bias. The NIH Common Fund’s Bridge to Artificial Intelligence (Bridge2AI) project and NIH’s Artificial Intelligence/Machine Learning Consortium to Advance Health Equity and Researcher Diversity (AIM-AHEAD) Program project will be major steps toward addressing those gaps.
So, yes—AI is getting smarter. But harnessing its full power will rely on scientists and clinicians getting smarter, too.

MaineHealth Innovation: Augmented Reality for Neonatal Resuscitation
Jan 26, 2022 MaineHealth
Helping newborns in distress is the goal of Augmented Reality Technology for Medical Simulation (ARTforMS) – an immersive experience that layers AR over traditional manikins. Learn how MaineHealth Innovation is supporting pediatric hospital medicine and critical care experts, Dr. Mary Ottolini and Dr. Michael Ferguson, as they continue leading a pilot with the software application at Maine Medical Center and throughout the MaineHealth system.


Association of Prenatal Exposure to Early-Life Adversity With Neonatal Brain Volumes at Birth
Original Investigation Pediatrics April 12, 2022
Regina L. Triplett, MD, MS1; Rachel E. Lean, PhD2; Amisha Parikh, BS3; et alJ. Philip Miller, AB4; Dimitrios Alexopoulos, MS1; Sydney Kaplan, BS1; Dominique Meyer, BS1; Christopher Adamson, PhD5,6; Tara A. Smyser, MSE2; Cynthia E. Rogers, MD2,7; Deanna M. Barch, PhD2,8,9; Barbara Warner, MD7; Joan L. Luby, MD2; Christopher D. Smyser, MD, MSCI1,7,9
Author Affiliations Article Information
JAMA Netw Open. 2022;5(4):e227045. doi:10.1001/jamanetworkopen.2022.7045
Key Points
Question: Is prenatal exposure to maternal social disadvantage and psychosocial stress associated with global and relative infant brain volumes at birth?
Findings: In this longitudinal, observational cohort study of 280 mother-infant dyads, prenatal exposure to greater maternal social disadvantage, but not psychosocial stress, was associated with statistically significant reductions in white matter, cortical gray matter, and subcortical gray matter volumes and cortical folding at birth after accounting for maternal health and diet.
Meaning: These findings suggest that prenatal exposure to social disadvantage is associated with global reductions in brain volumes and folding in the first weeks of life.
Abstract
Importance: Exposure to early-life adversity alters the structural development of key brain regions underlying neurodevelopmental impairments. The association between prenatal exposure to adversity and brain structure at birth remains poorly understood.
Objective: To examine whether prenatal exposure to maternal social disadvantage and psychosocial stress is associated with neonatal global and regional brain volumes and cortical folding.
Design, Setting, and Participants: This prospective, longitudinal cohort study included 399 mother-infant dyads of sociodemographically diverse mothers recruited in the first or early second trimester of pregnancy and their infants, who underwent brain magnetic resonance imaging in the first weeks of life. Mothers were recruited from local obstetric clinics in St Louis, Missouri from September 1, 2017, to February 28, 2020.
Exposures: Maternal social disadvantage and psychosocial stress in pregnancy.
Main Outcomes and Measures: Confirmatory factor analyses were used to create latent constructs of maternal social disadvantage (income-to-needs ratio, Area Deprivation Index, Healthy Eating Index, educational level, and insurance status) and psychosocial stress (Perceived Stress Scale, Edinburgh Postnatal Depression Scale, Everyday Discrimination Scale, and Stress and Adversity Inventory). Neonatal cortical and subcortical gray matter, white matter, cerebellum, hippocampus, and amygdala volumes were generated using semiautomated, age-specific, segmentation pipelines.
Results: A total of 280 mothers (mean [SD] age, 29.1 [5.3] years; 170 [60.7%] Black or African American, 100 [35.7%] White, and 10 [3.6%] other race or ethnicity) and their healthy, term-born infants (149 [53.2%] male; mean [SD] infant gestational age, 38.6 [1.0] weeks) were included in the analysis. After covariate adjustment and multiple comparisons correction, greater social disadvantage was associated with reduced cortical gray matter (unstandardized β = −2.0; 95% CI, −3.5 to −0.5; P = .01), subcortical gray matter (unstandardized β = −0.4; 95% CI, −0.7 to −0.2; P = .003), and white matter (unstandardized β = −5.5; 95% CI, −7.8 to −3.3; P < .001) volumes and cortical folding (unstandardized β = −0.03; 95% CI, −0.04 to −0.01; P < .001). Psychosocial stress showed no association with brain metrics. Although social disadvantage accounted for an additional 2.3% of the variance of the left hippocampus (unstandardized β = −0.03; 95% CI, −0.05 to −0.01), 2.3% of the right hippocampus (unstandardized β = −0.03; 95% CI, −0.05 to −0.01), 3.1% of the left amygdala (unstandardized β = −0.02; 95% CI, −0.03 to −0.01), and 2.9% of the right amygdala (unstandardized β = −0.02; 95% CI, −0.03 to −0.01), no regional effects were found after accounting for total brain volume.
Conclusions and Relevance: In this baseline assessment of an ongoing cohort study, prenatal social disadvantage was associated with global reductions in brain volumes and cortical folding at birth. No regional specificity for the hippocampus or amygdala was detected. Results highlight that associations between poverty and brain development begin in utero and are evident early in life. These findings emphasize that preventive interventions that support fetal brain development should address parental socioeconomic hardships.
Source:https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2790989
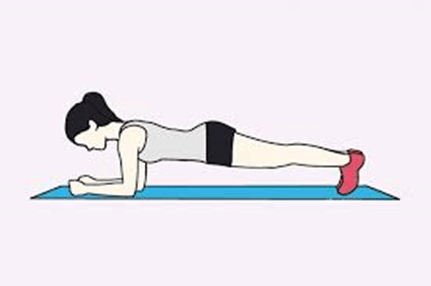
Muscle-strengthening activities are associated with lower risk and mortality in major non-communicable diseases: a systematic review and meta-analysis of cohort studies
Momma1, Ryoko Kawakami2, Takanori Honda3, Susumu S Sawada2
Correspondence to Dr Haruki Momma, Department of Medicine and Science in Sports and Exercise, Tohoku University Graduate School of Medicine, Sendai, Miyagi, Japan; h-momma@med.tohoku.ac.jp

Abstract
Objective: To quantify the associations between muscle-strengthening activities and the risk of non-communicable diseases and mortality in adults independent of aerobic activities.
Design: Systematic review and meta-analysis of prospective cohort studies.
Data sources: MEDLINE and Embase were searched from inception to June 2021 and the reference lists of all related articles were reviewed.
Eligibility criteria for selecting studies: Prospective cohort studies that examined the association between muscle-strengthening activities and health outcomes in adults aged ≥18 years without severe health conditions.
Results: Sixteen studies met the eligibility criteria. Muscle-strengthening activities were associated with a 10–17% lower risk of all-cause mortality, cardiovascular disease (CVD), total cancer, diabetes and lung cancer. No association was found between muscle-strengthening activities and the risk of some site-specific cancers (colon, kidney, bladder and pancreatic cancers). J-shaped associations with the maximum risk reduction (approximately 10–20%) at approximately 30–60 min/week of muscle-strengthening activities were found for all-cause mortality, CVD and total cancer, whereas an L-shaped association showing a large risk reduction at up to 60 min/week of muscle-strengthening activities was observed for diabetes. Combined muscle-strengthening and aerobic activities (versus none) were associated with a lower risk of all-cause, CVD and total cancer mortality.
Conclusion: Muscle-strengthening activities were inversely associated with the risk of all-cause mortality and major non-communicable diseases including CVD, total cancer, diabetes and lung cancer; however, the influence of a higher volume of muscle-strengthening activities on all-cause mortality, CVD and total cancer is unclear when considering the observed J-shaped associations.
Source: https://bjsm.bmj.com/content/early/2022/01/19/bjsports-2021-105061



How to Tap Into Your Joy
Author and Certified Professional Coach Sep. 20, 2017, 12:52 PM EDT

“Whether you think you can, or you think you can’t– you’re right”. ― Henry Ford
I love this quote, I believe it applies to so much in life. There is no doubting perception is powerful. What could be added to the above quote, is that regardless of what we think, the object of our heart’s desire is always right here ― whether or not we think it exists.
In relation to joy, this is wonderful news because it speaks to the idea that the experience of joy is always available to us. It’s not something we have to tirelessly search for or jump through hoops to arrive at. Rather, it’s something we can access right now in this very moment, if we choose.
If that seems like it’s too easy to be true, try these 5 added tips and see if they may help you tap into your joy.
1. Listen for Joy
The fast track way to accessing our personal joy is to be still and quiet enough to hear our unique inner voice and spirit. Often the outside noise drowns out the wise voice within is. When we give ourselves the space to really listen, it becomes very clear our joy is right below the surface just waiting to play. When we listen, our joy will show us the way.
2. Keep Joy Simple
Joy is not complicated and neither is accessing it. We don’t need to read endless books, listen to podcasts and spend copious amounts of money searching for joy. It’s much easier to take the simple route. Sometimes it’s a matter of reminding ourselves we are all worthy and capable of experiencing joy, it’s as simple as knowing our joy lives within us.
3. Just Be Joy
I love the idea that in order to have something — whether it’s love, peace, joy etc. that we must first be the very thing we are wanting. If we want joy, we can start by ‘being joy’. We can be joyful in our thoughts, the words we speak, our interactions with others and our overall demeanor. We humans are blessed to have the creative license to actually try on and be whatever it is we most want — that’s amazing!
4. Laugh Your Way to Joy
Laughing is powerful. Laugh at yourself, laugh with a friend, laugh with your pet. Whatever you do, be sure to laugh as often and as loud as you can. It’s nearly impossible to not feel joy when you are midway through a belly laugh with happy tears streaming down your cheeks. Laughter is a gift that’s available to us all the time. There isn’t a limit to how often we can bust a gut. The more we laugh, the greater sense of joy we feel and spread out into the world.
5. See Joy
If you want to prove to yourself that joy exists everywhere, all the time, see what happens when you start looking for the evidence of it. Try it out for a day, I dare you. When we start seeing joy in the faces of people around us and the pure magnificence of our surroundings, we experience a deep feeling of joy within ourselves. Breathe it all in. Give yourself the gift of becoming an expert at finding joy in the most mundane and simplest places. You may be surprised to see how much joy exists in our world, and even more so in recognizing it’s always present within you.
Source:https://www.huffpost.com/entry/how-to-tap-into-your-joy_b_59c29c13e4b0f96732cbcaf7

After a week of working hard on studies and research I decided to take a break this weekend to escape London and visit the coastal city of Brighton. Taking the time to try new things, explore new places and go on an adventure even for a day is something that can bring great joy in our lives. Having the opportunity to explore the seaside, swim in the Atlantic ocean and enjoy my first proper English fish and chips was a delight. Finding balance and slowing down to enjoy the simple moments in life is empowering and instrumental in helping us build our relationship to better know ourselves and positively grow our friendships with others.

Kanoa Igarashi 🇯🇵 is bringing surfing home to Japan!
Jul 23, 2021 Olympics
Kanoa Igarashi is a Japanese-American surfer who has competed professionally worldwide since 2012. He was the youngest rookie on the World Surf League Championship Tour in 2016 and collected more Round One wins than any other surfer. He talks to the Olympic Channel about going all-in, pressure, what the Olympics symbolise, and more. Enjoy watching this interview with Kanoa Igarashi!