


Serbia, officially the Republic of Serbia, is a landlocked country in Southeast Europe, at the crossroads of the Pannonian Plain and the Balkans. It shares land borders with Hungary to the north, Romania to the northeast, Bulgaria to the southeast, North Macedonia to the south, Croatia and Bosnia and Herzegovina to the west, and Montenegro to the southwest, and claiming a border with Albania through the disputed territory of Kosovo. Serbia has a population of roughly 7 million inhabitants. Its capital Belgrade is also the largest city.
Serbia is an upper-middle income economy, ranked 64th in the Human Development Index domain. It is a unitary parliamentary constitutional republic, member of the UN, CoE, OSCE, PfP, BSEC, CEFTA and is acceding to the WTO. Since 2014, the country has been negotiating its EU accession, with the aim of joining the European Union by 2025. Serbia formally adheres to the policy of military neutrality.
The country provides universal health care and free primary and secondary education to its citizens. The healthcare system in Serbia is organized and managed by the three primary institutions: The Ministry of Health, The Institute of Public Health of Serbia “Dr Milan Jovanović Batut” and the Military Medical Academy. The right to healthcare protections is defined as a constitutional right in Serbia. The Serbian public health system is based on the principles of equity and solidarity, organized on the model of compulsory health insurance contributions. Private health care is not integrated into the public health system, but certain services may be included by contracting.
Source:https://en.wikipedia.org/wiki/Serbia


COMMUNITY

UNICEF delivered a life-saving machine for newborns
A valuable donation to the Institute for Health Care of Children and Youth of Vojvodina provided by Delhaize Serbia
Belgrade, 4 November 2021

The Institute for Health Care of Children and Youth of Vojvodina from Novi Sad received today a therapeutic hypothermia device for asphyxiated newborns, provided by the Delhaize Serbia company as part of the So Small They Could Fit Inside a Heart campaign.
The therapeutic hypothermia device for asphyxiated newborns is intended for treating babies who suffered oxygen deprivation during birth. This device prevents brain damage in these babies by applying a modern controlled cooling method and is worth2,419,000 dinars.
“This valuable device is used for applying a proven therapeutic method in preventing brain damage in newborns, thus saving lives of asphyxiated babies. In the previous period, the Institute received valuable equipment from UNICEF, which helped equip the Institute. However, in order to reach the highest standards in developmental care, professional support we receive from UNICEF experts and partners is equally important. I would also like to thank the Delhaize Serbia company, which provided funds for the purchase of this life-saving device. UNICEF is our reliable partner that knows that many newborn babies need daily support of the health care system, regardless of the crisis, and we are grateful for it,” stated the Director of the Institute, Doc. Dr. Jelena Antić.
In Serbia, 65 thousand children are born every year, 4000 of whom are premature babies, and every day seven new babies require some form of urgent support. Premature birth is responsible for more than 60% of infant deaths in Serbia. The So Small They Could Fit Inside a Heart campaignwas launched by UNICEF late last year in order to provide additional equipment for neonatal units in Serbia, which will also contribute to reducing the mortality of premature babies in the country.
“The Institute for Health Care of Children and Youth in Novi Sad provides care to the most vulnerable babies from all over Vojvodina. For years, it has ensured that every newborn child gets the highest quality support in order to survive and thrive. The Institute is a good-practice example in the country when it comes to the provision of family-oriented developmental care, which also includes conditions for the continuous and irreplaceable contact between mum or dad and baby from the first days of baby’s life.
This is one of the few institutions in Serbia that has managed to preserve this practice during the pandemic, which opens up opportunities for us to jointly support other neonatal intensive care units in Serbia to persist in that endeavour. Maintaining the highest standards of child health care, despite the challenges imposed by the COVID19 pandemic, is a common priority, and we would like to thank Delhaize Serbia for providing the funds to support the most vulnerable, but also the bravest among us, who fight like true “little giants”, said Jelena Zaganović Jakovljević, UNICEF Early Childhood Development Specialist.
The COVID-19 epidemic has also been affecting pregnant women, newborns and children lately, so it is particularly important to invest efforts in adequate treatment of the infected and combating the epidemic, which is not sparing the youngest either. UNICEF has supported the equipping of neonatal units in Serbia, so that the most vulnerable among us, prematurely born babies and ill newborns, are given adequate support to survive and thrive. Starting from 2017, UNICEF has invested a total of 59,628,463 dinars in modernising the operation of the neonatal service in Serbia. The So Small They Could Fit Inside a Heart campaign was supported by the Ministry of Health of the Republic of Serbia.
“Delhaize Serbia has recognised UNICEF as the right partner and supported the modernisation of neonatal units in Novi Sad and Kragujevac, because we are aware of how important it is to help the most vulnerable babies that are also affected by the Corona virus crisis. Helping such small babies to get a chance at life is a reflection of our belief that help should be provided to those who need it most,” said Milica Popović, Corporate Communications Manager at Delhaize Serbia.
In all Maxi, Mega Maxi, Tempo and Shop&Go stores across Serbia, customers have the opportunity to round their bill up to the amount they wish, and in this way support the provision of equipment to neonatal units in our country.
Delhaize Serbia donated a total of 200,000 euros to UNICEF for equipping neonatal units in our country. From this donation, another therapeutic hypothermia device for asphyxiated newborns will be provided to the Kragujevac Neonatal Care Centre, which will also receive the first ambulance for prematurely born and ill newborn babies. Since the start of the campaign, this is the largest private sector donation in the So Small They Could Fit Inside a Heart campaign.
Source:https://www.unicef.org/serbia/en/press-releases/unicef-delivered-life-saving-machine-newborns

Coalition for Preemies – We Help Polish Parents of Preemies and Rescue Ukrainian NICUs
Maria Katarzyna Borszewska-Kornacka, MD, Elzbieta Brzozowska, Adriana Misiewicz, Joanna Nycz

Coalition for Preemies is an organization operating in Poland for ten years – initially as a social movement that brought together people and institutions working for the health of premature babies in Poland, and from 2019 as a Foundation.
The goals of the Foundation have been unchanged for many years – to work for the smallest of the youngest – premature babies and their parents. Our goal is education – starting with the health of pregnant women and preventing premature births, ending with the health of premature babies, their development, and rehabilitation. We reach out to parents of premature babies to help them care for their premature babies and to the general public to help them understand that a premature baby is the most vulnerable person who needs our help. Nobody who has not encountered a premature baby in their environment knows what complications the baby and its loved ones face and how much effort is needed to ensure healthy development.
During the pandemic, we got involved with an international campaign initiated by EFCNI #zeroseparation. It aimed to restore the possibility of visiting preemies in neonatal departments for their parents. In Poland, as part of the #zeroseparation campaign, we included parents of preemies in the group “zero” for vaccination against COVID-19 – the group that could be vaccinated first together with medical staff. We wanted parents of premature babies to be protected from the virus as soon as possible and to be able to visit their children in hospitals. It was possible thanks to the immediate decision of the Ministry of Health after we sent a request on this matter.
In 2021, we launched advice for parents of premature babies with specialists as part of the “Ask for a premature baby” campaign – it consists of a telephone conversation or via online communicators. Parents can talk to a neonatologist, psychologist, pediatric neurologist, lactation consultant, and physiotherapist.
Currently, we are involved in helping premature Ukrainian babies. Together with the Neonatus Foundation, the Tęczowy Kocyk Foundation, and the blogger MatkoweLove, we organized a fundraiser. With the collected money, we finance the purchase of the necessary equipment and medicines for Ukrainian neonatal units and transport the equipment to the neediest hospitals in Ukraine. The President of our Foundation- prof. Maria Katarzyna Borszewska-Kornacka is in constant contact with the national consultant for neonatology in Ukraine, and therefore we know what their needs are. First shipments of medical equipment, drugs, and milk were sent to Lviv, Kyiv, Charkov, Brovary, Ivano-Frankovsk, and Dniepro.
It is possible to donate to the Coalition for Preemies Foundation: https://www.koalicjadlawczesniaka.pl/numer-konta-fundacji-koalicja-dla-wczesniaka-i-dane-do-przelewow-z-zagranicy/
We have also started the “Package for a Newborn” campaign, the purpose of which is to equip Ukrainian babies born in Warsaw with necessities such as clothes for newborns, sizes 50-68, including bodysuits, rompers, socks, hats, nipples, small toys, cosmetics, and hygiene articles.
We also plan to prepare a warehouse of clothes/things useful for newborns, which will be issued in response to the specific needs of single Ukrainian mothers in Poland. From the warehouse, mothers will be able to receive rockers, carriers, scarves for carrying babies, prams, changing mats, bathtubs, and breast pumps.
Since the outbreak of war, we have had over a dozen requests to help in transferring newborns from Ukraine to Poland.
Initially, there were babies of US and UK citizens born in Ukraine, followed by several neonatal transfers or personal admissions of Ukrainian newborns from the border zone brought personally by parents.
Our triage center has different scenarios comprising both stabilization and subsequent transfer to different Polish neonatal/pediatric centers and diagnostic and treatment approaches on site.
Requests regarding medical transfers of premature babies were formulated predominantly by aid organizations, governmental or family activities, and not specifically by medical referrals.
Recently we have received several inquiries about the possibility of admission of newborns/small infants with chronic and/or rare genetic problems. Until now, the utility of the database created for the quick electronic exchange of medical data regarding the transfer of newborns from Ukraine to Poland seems suboptimal as there was perhaps no need for such transfers on a larger scale.
Further information can be found on the Foundation website: Source:https://www.koalicjadlawczesniaka.pl/aktualnosci/

Serbia to Use Cash to Boost Birth Rate, Avert Population Decline
By Misha Savic November 24, 2021
Serbia will triple a cash incentive to parents for their first-born child and prop up support for bigger families to fight a crippling demographic decline, President Aleksandar Vucic said.
“We’re vanishing as a nation,” the Balkan country’s leader told reporters on Wednesday as he announced tripling the one-time incentive for mothers for their first child to 300,000 dinar ($2,862) as of January. Serbia will also increase its existing cash and other support to families to have and raise more children, he said.
The plan comes as Vucic, whose party and allies control an absolute majority in Serbia’s parliament, is gearing up for general elections expected in the spring. Mainstream opposition parties boycotted a previous ballot in 2020 but are likely to challenge Vucic’s dominance in the race that will also include his job.
The average monthly net wage equals $616 in the nation of 6.9 million. The population is falling by around 30,000 a year amid a low birth rate and emigration. The median age is almost 43 years, among the highest in Europe.
Serbia’s current birth rate of 1.5 needs to go up to at least 2.15 just to maintain the current population size, Vucic said.
Additional steps will help young people to stay in colleges and universities even if they become parents while studying, he said. The government is weighing giving grants to young couples of as much as $22,000 to help them buy their first home and start a family, he said.
“We’re getting older and older, and our economic progress will depend on how we ensure the nation’s progress with the demographic measures,” Vucic said.

Ukraine crisis: Premature babies born into war as deliveries forced to take place in hospital basement

I’m incredibly sad,’ doctor says, ‘babies are going to die because they cannot live in these conditions’
As women are forced to give birth in the basements of hospitals in war-torn Ukraine, health officials have raised fears that not all newborn babies can survive in such conditions.
Devastating images coming out of the Eastern European nation show the makeshift wards being used after medical staff work tirelessly to convert basements of maternity hospitals – all the while, using them as bomb shelters.
Most at risk are premature babies, who require special medical attention in their first few days, weeks or even months of life.
More than 1,000 babies are born in Ukraine per day, according to data from research platform Macrotrends. Of those, around 100 will need some form of neonatal intensive care.
Footage from one perinatal care unit in Kyiv, published by ITV News, showed parents and their
At one point, a man is filmed attending to a tiny baby in an incubator.
The machine beeps momentarily as he reaches for some medical equipment, then the clip cuts to night time where nurses and parents can be seen sat underneath what looks like the building’s water or gas pipes.
Speaking to the broadcaster, Dr Olena Kostiuk, a neonatologist associate professor in Ukraine’s capital city, described how the basement unit was set up in just a few days.
“It’s usually a technical room for water, for electricity and heating… never, never, ever is this space used in this way,” she said. “Very sick babies, babies which we cannot move… they permanently live in the basement.”
Pregnant women and newborn babies in the basement of a maternity hospital converted into a medical ward, and used as a bomb shelter during air raid alerts in Kyiv.
Clearly frustrated, and upset, Dr Kostiuk said plainly that “babies are going to
“I’m incredibly sad,” she added, “for myself the biggest problem is, I don’t know when it’s going to finish and how long our pregnant women, our babies delivered in a basement, our babies have no normal support.”
Over in the city of Zhytomyr, as reported by The Independent earlier today, staff of the maternity ward at Pavlusenko hospital – all taking cover under Russian missile fire – helped a pregnant woman who had started giving birth on the floor of the bomb shelter after the shock of a nearby explosion sent her into labour.
Medical workers show a newborn baby to a woman who gave birth in a maternity hospital basement converted into a medical ward in Mariupol, Ukraine
It came after an airstrike in the city on Tuesday which struck a military base just 200 metres away from the hospital, seriously damaging multiple wards.
Among those worst hit was the maternity wing, where 45 women and 15 newborn babies were being cared for at the time. All were subsequently evacuated to the basement, where they remain.
The Russian strike on Zhytomyr, in Ukraine’s northwest, also hit a residential area and killed at least two people, emergency services said afterwards.
Dr Cora Doherty, a neonatologist speaking on behalf of the British Association of Perinatal Medicine (BAPM), said she had seen the footage from Kyiv’s perinatal centre and was concerned the babies’ care was being compromised.
“We know that if babies do not get the proper care around the time at birth, that particularly if they’re ill, there is an increased risk of death in those babies,” she told ITV News.
And she added: “That’s essentially the, you know, the future denigrate generation there. So, it is really, really important that we support both these mothers and their babies in their plight.”
Four “loud explosions” were heard in the centre of Kyiv late on Wednesday night, with the Kyiv Independent taking to Twitter to advise its readers to take cover in their “nearest shelter” at around
It came as Russian troops appeared to take “complete control” of Kherson, the first major city to be captured during Vladimir Putin’s war.
Igor Kolykhayev, Kherson’s mayor, said in a Facebook post on Wednesday that the Black Sea port had been lost.
He urged the Kremlin’s soldiers not to shoot at civilians and publicly called on Ukrainians to walk through the streets only in daylight and with no more than one other person.
Cars will only be allowed to enter the city to bring food and medicine and other essentials. They must drive at minimum speed and be prepared to stop to be searched by Russian troops, he said.
Mr Kolykhayev added: “Ukrainian flag above us. And to keep it the same, these requirements must be met. I have nothing else to offer yet.”

ALEKSANDRA MLADENOVIC X NENAD MANOJLOVIC – TI MENI, JA TEBI
Oct 21, 2021 IDJVideos.TV

Official music video for “Ti Meni, Ja Tebi” by Aleksandra Mladenović and Nenad Manojlovi

HEALTH CARE PARTNERS

SHEA NICU White Paper Series: Practical approaches for the prevention of central line-associated bloodstream infections\
Pediatrics AUTHOR: SHEA PUBLISHED:MARCH 4, 2022 CURRENT – CLABSI, Clinical Practice, Guidelines, Immunocompromised Patients, Infection Prevention

ABSTRACT:
This document is part of the “SHEA neonatal intensive care unit (NICU) white paper series.” It is intended to provide practical, expert opinion, and/or evidence-based answers to frequently asked questions about CLABSI detection and prevention in the NICU. This document serves as a companion to the CDC Healthcare Infection Control Practices Advisory Committee (HICPAC) Guideline for Prevention of Infections in Neonatal Intensive Care Unit Patients. Central line-associated bloodstream infections (CLABSIs) are among the most frequent invasive infections among infants in the NICU and contribute to substantial morbidity and mortality. Infants who survive CLABSIs have prolonged hospitalization resulting in increased healthcare costs and suffer greater comorbidities including worse neurodevelopmental and growth outcomes. A bundled approach to central line care practices in the NICU has reduced CLABSI rates, but challenges remain. This document was authored by pediatric infectious diseases specialists, neonatologists, advanced practice nurse practitioners, infection preventionists, members of the HICPAC guideline-writing panel, and members of the SHEA Pediatric Leadership Council. For the selected topic areas, the authors provide practical approaches in question-and-answer format, with answers based on consensus expert opinion within the context of the literature search conducted for the companion HICPAC document and supplemented by other published information retrieved by the authors. Two documents in the series precede this one: “Practical approaches to Clostridioides difficile prevention” published in August 2018 and “Practical approaches to Staphylococcus aureus prevention,” published in September 2020.

American Nurse Journal/Cedars-Sinai Hospital: Fostering nurse-physician collaboration
February 1, 2022
Author(s): Sarah Low, MSN, RN, OCN, CMSRN; Emily Gray, MSN, RN-BC; Amanda Ewing, MD, FACP; Patricia Hain, MSN, RN-BC, NE-BC, FACHE; and Linda Kim, PhD, MSN, RN, PHN, CPHQ
>>>>>>>>>>>>>>><<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<

Eat, Sleep, Console Approach
A Family-Centered Model for the Treatment of Neonatal Abstinence Syndrome
Grisham, Lisa M. NNP-BC; Stephen, Meryl M. CCRN; Coykendall, Mary R. RNC-NIC; Kane, Maureen F. NNP-BC; Maurer, Jocelyn A. RNC-NIC; Bader, Mohammed Y. MD
Advances in Neonatal Care: April 2019 – Volume 19 – Issue 2 – p 138-144
doi: 10.1097/ANC.0000000000000581
Abstract:
Background:
The opioid epidemic in the United States has resulted in an increased number of drug-exposed infants who are at risk for developing neonatal abstinence syndrome (NAS). Historically, these infants have been treated with the introduction and slow weaning of pharmaceuticals. Recently, a new model called Eat, Sleep, Console (ESC) has been developed that focuses on the comfort and care of these infants by maximizing nonpharmacologic methods, increasing family involvement in the treatment of their infant, and prn or “as needed” use of morphine.
Purpose:
The purpose of this evidenced-based practice brief was to summarize and critically review emerging research on the ESC method of managing NAS and develop a recommendation for implementing an ESC model.
Methods:
A literature review was conducted using PubMed, Cochrane, and Google Scholar with a focus on ESC programs developed for treating infants with NAS.
Finding/Results:
Several studies were found with successful development and implementation of the ESC model. Studies supported the use of ESC to decrease length of stay, exposure to pharmacologic agents, and overall cost of treatment.
Video Abstract Available at:

PREEMIE FAMILY PARTNERS
HAPPY MOTHERS DAY VIDEO

Acknowledging and Supporting NICU Moms this Mother’s Day
Leah Sodowick, B.A., Pamela A. Geller, Ph.D., Chavis A. Patterson, Ph.D.

Each year on the second Sunday in May, people across the United States and around the globe honor and celebrate mothers (Our use of the term “mothers” includes anyone who identifies as a mother, grandmother, gestational parent, or caregiver.) on Mother’s Day. This holiday is full of joy, celebration, pride, and gratitude for many. There may be hugs, handmade and store-bought cards, photos posted and shared on social media, breakfast in bed, family gatherings, flower bouquets, and tokens of appreciation. Mother’s Day can be challenging and emotionally fraught for some, including mothers with an infant hospitalized in a neonatal intensive care unit (NICU). With the help of NICU staff and providers, mothers can anticipate and cope with the challenges and emotions that they may experience this Mother’s Day, on May 8th. This article will discuss the emotions and challenges NICU mothers may experience on the holiday and suggest ways to acknowledge, support, and celebrate NICU mothers and caregivers.
Parents in the NICU may grieve the loss of anticipated postpartum plans and experiences, such as caring for and bonding with their baby at home. Mothers in the NICU may also grieve the loss of expected holiday events and experiences (1). Grief is one of the many normal and common reactions NICU parents may have. On Mother’s Day and the days surrounding this holiday, mothers in the NICU may feel disappointed, disheartened, and sorrowful if their expectations, visions, and anticipations for Mother’s Day do not match their current reality—one that is often characterized by long hours at their baby’s bedside and concern and worry about their baby’s health and survival. Current realities may also involve difficult decision making about treatment options and endof-life care. NICU parents may be juggling multiple responsibilities, such as caring for older children and work. Parents may also experience physical separation from their baby when the gestational parent is recovering from childbirth, the baby is in an isolette, the baby is undergoing a surgical procedure, or when parents leave the hospital to go home or to their temporary residence. Furthermore, by spending time in the NICU, mothers may miss traditional family gatherings and their usual Mother’s Day celebrations (1). Not being present for these events may exacerbate feelings of isolation as many families begin to reunite after separations due to COVID-19 restrictions.
Some mothers in the NICU may have difficulty or delays in forming their maternal identity due to limited opportunities for caregiving and interacting with their infant, shared caregiving responsibilities with NICU staff providers, disrupted mother-infant bonding, perceived lack of control, and increased psychological distress (2–5). Difficulty or delays in forming maternal and parental identity are part of an array of normal reactions and experiences that a parent may have. In a qualitative examination of NICU mothers’ perceptions of the development of their maternal role in the context of NICU, the thematic analysis revealed that some respondents characterized themselves as mothers only while they were in the NICU; they reported not feeling like mothers when they left the hospital because they were not with their babies or serving as a primary caretaker (3). Researchers have found that mothers’ perceived loss of parental role was one of the most stressful aspects of their infant’s NICU hospitalization (6,7)predictors, and child outcomes associated with NICU-related stress for mothers of infants born very preterm (VPT. For mothers in the NICU who have not yet fully developed their maternal identity or perceive a loss of their parental role, Mother’s Day may feel conflicting and isolating. Of note, mothers in the NICU who have experienced neonatal losses or are anticipating and planning for neonatal loss may experience an intensification of grief and have particularly difficult emotional experiences on Mother’s Day.
We encourage NICU staff and providers to thoughtfully acknowledge and celebrate mothers and caregivers in the NICU this Mother’s Day. Listed below are some suggestions:
Acknowledge Mother’s Day Staff and providers can communicate their acknowledgment of Mother’s Day, even when it may not be a “happy” Mother’s Day for mothers and other caregivers in the NICU. If this is the case, instead of wishing mothers a “happy” Mother’s Day, one can express, “I am thinking about you today on Mother’s Day.”
Validate and reflect emotions – NICU staff and providers can help mothers and caregivers cope with emotions that may arise during this holiday by validating and reflecting on mothers’ expressed feelings. Offering opportunities for parents to share their feelings by asking open-ended questions about how they are feeling and allowing time to listen to the responses can be very empowering for parents. Responding with statements that validate their experience also can be very helpful. For example, one could respond to a mother who expresses grief about the loss of expected Mother’s Day experiences by stating, “it makes sense why you would feel especially sad and disappointed today.”
Provide opportunities for caretaking – If possible, NICU staff and providers can find ways for parents to interact with their babies more on Mother’s Day. For example, mothers could be encouraged to take on a meaningful hands-on caretaking task, like feeding or bathing their baby or changing a diaper. Mothers also can be encouraged to engage in skin-to-skin care.
Encourage mothers to communicate with their babies – On Mother’s Day, NICU mothers can communicate and bond with their babies by reading them a book, story, or poem. Mothers could write and share a personal letter to their babies about their love, their family, and what it means to be their mother. Mothers may also wish to sing to their babies.
Praise mothers’ efforts to care for their babies – On Mother’s Day (and regularly), NICU staff and providers are encouraged to acknowledge and praise mothers’ efforts to care for their babies in the NICU. A simple phrase like “you are doing a great job” can be meaningful and impactful to mothers who may be lacking confidence and feeling uncertain about their maternal role.
Encourage mothers to attend parent support groups – NICU staff and providers can encourage mothers to attend parent support groups on Mother’s Day. Peer sharing of positive and negative maternal experiences in NICU support groups can strengthen social relationships and networks, provide therapeutic benefits, foster feelings of safety and comfort, and encourage parent advocacy (3,9). On Mother’s Day, NICU parent support groups can feature topics related to Mother’s Day. Mother’s Day themed activities, such as scrapbooking, crafting, and even expressive writing or journaling that allow for both positive and adverse feelings can also be incorporated.
Create cards or keepsake gifts for mothers – There are several ways Mother’s Day can be celebrated in the NICU. One way to celebrate the holiday is for NICU staff to take a photo of each baby or each mother with their baby and put it inside of a card that can be placed by the baby’s bedside. Staff may also wish to create small keepsake gifts for mothers. At Denver Health Medical Center, NICU nurses make keychains to give to each mother (8). Each keychain contains a photo of the mom with their baby. Provide scent cloths for mothers Small pieces of soft fabric with the baby’s and the mother’s familiar scent can bring comfort to mothers and babies and help facilitate bonding. The cloth can be placed in the baby’s be against the mother’s skin to absorb scent and then exchanged. The scent cloths can even be shaped like hearts.
Enlist volunteer assistance from past NICU graduate families – Staff and providers can consider enlisting volunteer assistance from past graduate families of the NICU to help support and celebrate mothers in the NICU on Mother’s Day (1). Former NICU mothers and caregivers with first-hand lived experience and expertise could write cards with encouraging and supportive messages to current NICU mothers and assist with running parent activity groups. It is important to remember that each mother in the NICU will experience Mother’s Day differently, and some families may not be open to celebrating or participating in Mother’s Day activities.
As a final note, we would like to acknowledge NICU staff, providers, and readers this Mother’s Day. We recognize those who are mothers, grandmothers, and caregivers. We recognize those who have or have had infants hospitalized in the NICU. We recognize those who have lost children and those who have lost mothers. We recognize those with strained relationships with their mothers, those with strained relationships with their children, those who have chosen not to be mothers, and those who are yearning to be mothers. We honor you all and wish you a peaceful Mother’s Day.
Source:http://neonatologytoday.net/newsletters/nt-apr22.pdf
Timely examination can save premature babies from permanent blindness
By Muhammad Qasim April 20, 2022
Rawalpindi : Over eighty-five per cent of premature babies who weigh less than 1.5 kilograms at the time of birth have a high risk of developing the disorganised growth of retinal blood vessels, which can cause vision problems including permanent blindness.
Babies born prematurely, before 266 days, have many obstacles to overcome in their first fragile weeks, one of which is eye development that can be resolved through screening and surgical procedures to help avoid serious eyesight problems like vision impairment and blindness.
Chief Consultant and Head of Retina Department at Al-Shifa Eye Hospital Dr Nadeem Qureshi said this while talking to the media persons. He said that the blood vessels of the retina develop three months after conception and complete their growth at the time of normal delivery. If an infant is born prematurely, eye development can be disrupted, as the smaller a baby is at birth, the more likely that baby is to develop difficulties, he said.
Using excess oxygen to treat premature babies in the hospitals stimulates abnormal vessel growth in the eyes, with the smallest and sickest having the highest risk of devastating effects of Retinopathy of Prematurity (ROP), he said.
He added that studies have shown that keeping the oxygen saturation at a lower level from birth can reduce the rate of advanced ROP, a blinding eye disorder.
All parents must include a vision screening in their list of baby check-ups between six and twelve months of age as every premature infant deserves the constant attention of an ophthalmologist because of his or her increased risk for eye misalignment, amblyopia, and the need for glasses to develop normal vision.
Dr Qureshi said that Al-Shifa Eye hospital has already signed MoUs with Fauji Foundation Hospital, Combined Military Hospital, and Benazir Bhutto Hospital to treat newborns with vision complications.
Al-Shifa Eye Hospital is the only facility in the SAARC region and among few in the world having the latest equipment and excellent skills to treat newborns having vision complications, he claimed. So far, the trust has treated around 6000 infants in the last seven years and the number is bound to increase as the awareness grows, he said.
He added that we are here to provide free guidance to all the state-owned and private healthcare facilities, including those in other countries, to help save thousands from plunging into darkness for life. The Retina Department of Al-Shifa Hospital has 12 surgeons, assisted by trainees, and it performs Retinal OPD, lasers, injections and surgery every day of the week, said Dr Qureshi.
Average OPD at the Retina Department is 215 patients per day, average lasers are 35 per day, average injections are 50 per day and on average 25 surgeries are conducted daily, he added. A retinal surgery costs around Rs95 thousand, but 75 per cent of patients are treated free of cost, he said.
Source:Timely examination can save premature babies from permanent blindness (thenews.com.pk)

UCSF NICU-How To Do A Swaddled Bath
(Spanish subtitles)
197,922 views Nov 28, 2018
UCSF Benioff Children’s Hospital Oakland


Watch the dramatic moment a preemie leaves his tubes behind and starts a new life (VIDEO)
Aleteia
Paola Belletti – published on 09/14/17aa
Ward Miles Miller’s scary and moving first year of life was captured by his father.
Ward Miles Miller was born on July 20, 2012 — three months early. Fear and anxiety initially overshadowed (but didn’t suffocate) his parents’ joy and hope. The story of Ward’s first year of life is a beautiful, moving, and dramatic one, as told through the video and photos taken by his father Benjamin.
Little Ward received all the medical support possible and necessary until he was able to go home safely; he spent 107 days in the hospital, most of them in an incubator. His mom and dad, Lindsay and Benjamin Scott, are devoted and loving parents who fought for Ward and celebrated every ounce he gained as a milestone.
Today, Ward is navigating the stormy waters of life in a vessel that is stronger and more stable every day.

INNOVATIONS

Association of Abnormal Findings on Neonatal Cranial Ultrasound With Neurobehavior at Neonatal Intensive Care Unit Discharge in Infants Born Before 30 Weeks’ Gestation
JAMA Netw Open. 2022;5(4):e226561. doi:10.1001/jamanetworkopen.2022.6561
Original Investigation – Pediatrics April 8, 2022

Key Points
Question What is the association between neonatal cranial ultrasound findings and neurobehavioral examination at term-adjusted age?
Findings In this cohort study of 675 infants born before 30 weeks’ gestation, abnormal findings on cranial ultrasound were associated with decreased tone, poor regulation of attention, and movement outcomes as the infants matured to term-adjusted age.
Meaning Among very preterm infants, abnormal findings on cranial ultrasound identifiable in the first 14 postnatal days were associated with neurobehavior outcomes at or near term-equivalent age and could be used to help counsel and educate parents as well as inform treatment strategies for therapy service in the neonatal intensive care unit and after discharge.
Abstract
Importance Cranial ultrasound (CUS) findings are routinely used to identify preterm infants at risk for impaired neurodevelopment, and neurobehavioral examinations provide information about early brain function. The associations of abnormal findings on early and late CUS with neurobehavior at neonatal intensive care unit (NICU) discharge have not been reported.
Objective To examine the associations between early and late CUS findings and infant neurobehavior at NICU discharge.
Design, Setting, and Participants This prospective cohort study included infants enrolled in the Neonatal Neurobehavior and Outcomes in Very Preterm Infants Study between April 2014 and June 2016. Infants born before 30 weeks’ gestational age were included. Exclusion criteria were maternal age younger than 18 years, maternal cognitive impairment, maternal inability to read or speak English or Spanish, maternal death, and major congenital anomalies. Overall, 704 infants were enrolled. The study was conducted at 9 university-affiliated NICUs in Providence, Rhode Island; Grand Rapids, Michigan; Kansas City, Missouri; Honolulu, Hawaii; Winston-Salem, North Carolina; and Torrance and Long Beach, California. Data were analyzed from September 2019 to September 2021.
Exposures Early CUS was performed at 3 to 14 days after birth and late CUS at 36 weeks’ postmenstrual age or NICU discharge. Abnormal findings were identified by consensus of standardized radiologists’ readings.
Main Outcomes and Measures Neurobehavioral examination was performed using the NICU Network Neurobehavioral Scale (NNNS).
Results Among the 704 infants enrolled, 675 had both CUS and NNNS data (135 [20.0%] Black; 368 [54.5%] minority race or ethnicity; 339 [50.2%] White; 376 [55.7%] male; mean [SD] postmenstrual age, 27.0 [1.9] weeks). After covariate adjustment, lower attention (adjusted mean difference, −0.346; 95% CI, −0.609 to −0.083), hypotonicity (mean difference, 0.358; 95% CI, 0.055 to 0.662), and poorer quality of movement (mean difference, −0.344; 95% CI, −0.572 to −0.116) were observed in infants with white matter damage (WMD). Lower attention (mean difference, −0.233; 95% CI, −0.423 to −0.044) and hypotonicity (mean difference, 0.240; 95% CI, 0.014 to 0.465) were observed in infants with early CUS lesions.
Conclusions and Relevance In this cohort study of preterm infants, certain early CUS lesions were associated with hypotonicity and lower attention around term-equivalent age. WMD was associated with poor attention, hypotonicity, and poor quality of movement. Infants with these CUS lesions might benefit from targeted interventions to improve neurobehavioral outcomes during their NICU hospitalization.
Full Article:
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2790902
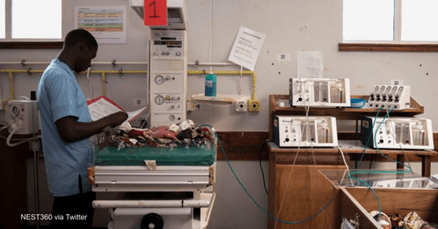
Can a new effort end ‘equipment graveyards’ at neonatal ICUs?
By Catherine Cheney /09 September 2021

Just outside of San Francisco, product engineers at a manufacturer and supplier of health technologies are hard at work on devices to save newborn lives in settings far different from this bayside facility.
The 3rd Stone Design warehouse features a display of lifesaving technologies for newborns, including a continuous positive airway pressure — or CPAP — machine that the team helped develop.
The company is part of a global coalition of organizations working to get such devices to babies in low-income countries, where they confront inequity from the moment they’re born. The coalition is called Newborn Essential Solutions and Technologies, or NEST360, and it targets neonatal intensive care units.
Infants born in sub-Saharan Africa or Southern Asia are 10 times more likely to die during the first month of life compared with those born in high-income countries, due in part to a lack of access to medical devices. About 75% of babies born prematurely can be saved with the right medical care.
“People who come up with product ideas are not the same people who figure out how to sell something, and the people who figure out how to sell it are not the same people who figure out how to service it.”
But when health facilities end up with devices that are not designed with their constraints in mind — or when staffers lack training in using these tools and there are no plans to fix products when they break — potentially lifesaving technologies can end up in what are often called medical equipment graveyards.
NEST360, which aims to reduce newborn mortality in sub-Saharan African hospitals by 50%, is trying to change that. It’s taking what it describes as a “holistic approach” to neonatal care — distributing newborn health technologies, educating clinicians and technicians on how to maintain these tools, and supporting local innovators to build the technologies that work best for their contexts.
The coalition launched in 2019, with an initial focus on Malawi, Kenya, Tanzania, and Nigeria. From the beginning, NEST360 has said there is a need for not just low-cost technology but high-quality distribution. With assistance from 3rd Stone Design, which helped develop a new nonprofit called Hatch Technologies, NEST360 may have found the end-to-end solution for distribution that it sought.
Hatch provides distribution and support services for devices designed for newborn care units in sub-Saharan Africa. And partners involved in NEST360 say they hope it can serve as a model for ensuring medical equipment reaches low birth weight and premature babies in time to save their lives.
Steve Adudans, Kenya country director at the Rice360 Institute for Global Health Technologies — which is also part of the NEST360 partnership — has seen many examples of donated medical devices piling up instead of being used in neonatal ICUs.
“We need to bury the medical equipment graveyards,” he said during an online webinar on innovations in newborn health in Africa organized by The Elma Philanthropies, one of NEST360’s funders. “That’s what NEST is about.”
The NEST360 bundle of technologies includes 18 medical devices focused on areas including temperature stability, respiratory support, and neonatal jaundice treatment. Each of them meets target product profiles for newborn care in low-resource settings developed by NEST360 in partnership with UNICEF.
Many of the NEST360 technologies that meet these operational and performance characteristics were developed by innovators focused on low-resource settings, where it is often impossible to repair products made by corporations that impose restrictive warranties, lock their software, and limit access to spare parts.
But these devices cannot fulfill their vital potential when they are introduced into a broken system, Adudans said.
NEST360 needed a solution to get products from manufacturers to distributors to facilities in the countries where it works. That’s where Hatch Technologies comes in.
Often, nations with the highest rates of neonatal mortality receive donated equipment that fails when placed in environments with unreliable electricity, temperature variation, and too much dust and dirt.
Bottom of Form
But even when countries can procure medical supplies, they often don’t know which devices would work best for their settings. So they end up with cheap devices that break because they are poor quality or high-end ones that never get fixed because maintenance is too expensive, said Dick Oranja, CEO at Hatch Technologies.
Based in Nairobi, Kenya, Hatch Technologies launched in March 2020 with a mission to transform the way newborn care devices are distributed, supported, and used in Africa. To date, Hatch has helped NEST360 distribute almost 2,000 pieces of equipment reporting over 95% functionality, meaning they are working as they should. It is starting with support from the same backers as NEST360 but is an independent nonprofit that could continue to seek support elsewhere.
Hatch uses asset tracking — with a bar code-type sticker on each of its products — to follow each shipment from the initial logistics and warehousing to shipment and ultimately the use of the device.
“Distributors will mention they provide a level of service. They have to assure their customers. But the truth of the matter is distributors do not offer targeted service,” Oranja said. “We measure customer service parameters a routine medical equipment manufacturer will not measure.”
Beyond delivering medical devices, Hatch installs the equipment, trains staffers, and stops by to see how the technology is working, based in part on its measure of the functional status of the equipment — meaning whether it is being used as intended or at all.
A number of supply chain bottlenecks prevent newborn health products from reaching babies in low-income countries during critical moments of life and death.
“People who come up with product ideas are not the same people who figure out how to sell something, and the people who figure out how to sell it are not the same people who figure out how to service it and support it,” Robert Miros, CEO at 3rd Stone Design, told Devex.
That reality is part of what led 3rd Stone Design to work with partners to develop Hatch Technologies.
NEST360’s expanded model, which includes Hatch, reflects a growing understanding that no matter how innovative medical devices are, they are only one part of the solution to saving newborn lives. The other crucial piece is distribution.
Hatch Technologies began after Miros and his colleagues formed a task team to brainstorm the effort together with other NEST360 partners and funders. They drew on the expertise of 3rd Stone Design’s Danica Kumara, a director of product management who formerly worked on medical device efforts in Southeast Asia, and Vikas Meka, a senior product manager who was formerly a senior adviser on global health innovation at the U.S. Agency for International Development.
Now that NEST360 has launched in four African countries, it intends to demonstrate a path to scale across the continent, said Rebecca Richards-Kortum, director at the Rice360 Institute for Global Health Technologies, during the webinar.
But what turned the tide on newborn survival in the United States and the United Kingdom was a network of neonatal ICUs — “a regional system with people and products that are ready to help babies,” she said.
So as NEST360 partners with Hatch Technologies to bridge the gap from manufacturers to distributors and ensure that lifesaving medical devices can reach health care facilities, it is also calling for stronger hospital systems for newborn care.
Source:https://www.devex.com/news/can-a-new-effort-end-equipment-graveyards-at-neonatal-icus-99571

The transition to the artificial uterus should be as natural as possible. Photo: Bart van Overbeeke
Without gasping for air safely in the artificial womb

APR 07, 2022
An artificial uterus significantly increases the chances of survival for extremely premature babies. That is why researchers at TU Eindhoven are doing a lot of research on this topic. One of the biggest challenges is preventing the fetus from breathing oxygen just after birth, because that is harmful to the not yet mature alveoli. The solution? A wound spreader, coupling elements and a biobag filled with amniotic fluid.
The development of the artificial uterus has accelerated in recent years, not least because of the Perinatal Life Support partnership, which includes TU Eindhoven. According to Professor Frans van de Vosse (Professor of Cardiovascular Biomechanics within the Faculty of Biomedical Technology) and Guid Oei (Gynecologist and part-time Professor within the Faculty of Electrical Engineering), within ten years it should be possible to significantly increase the chances of survival and quality of life of extremely premature babies via a so-called incubator 2.0.
QUALITY OF LIFE
In the Netherlands alone, 700 children are born extremely prematurely each year – between 24 and 28 weeks. Almost half die, while a large proportion retain permanent health problems because organs have not yet matured. “Think of lung problems or brain damage,” clarifies Frank Delbressine (Assistant Professor of Industrial Design). “We want to increase both the life chances and the quality of life of newborn babies with an artificial uterus.”
Delbressine is the supervisor of PhD student Juliette van Haren. Together with a group of Industrial Design students, she is concerned with, among other things, the way in which childbirth should take place. One of the biggest challenges is to prevent the fetus from gasping for air just after birth (in this case by caesarean section). The birth procedure to the artificial uterus should be as natural as possible, which is why Van Haren is developing a safe way for the premature baby to be transferred from the natural uterus to the artificial uterus.
LUNG ALVEOLI NOT FULLY GROWN
“We want to prevent the fetus from breathing oxygen, because the alveoli are not yet mature and can be damaged. A 24-week-old baby belongs in an artificial amniotic fluid environment, and we’re trying to mimic that. The transition from the real uterus to the artificial one must occur in a way that the baby barely notices, both physically and mentally, that he or she is being taken to a different location,” explains Delbressine.
The principle works as follows: a so-called wound spreader holds open the wound created by the C-section, after which a biobag filled with artificial amniotic fluid is attached to the wound spreader via a connector. The baby can then be carefully transferred to the artificial uterus at the correct temperature via a glove in the biobag.
Delbressine: “A filled biobag may sound crazy or disrespectful at first, but this is exactly how the fetus is ‘wrapped up’ in the womb as well, we are trying to imitate that as real as possible.”
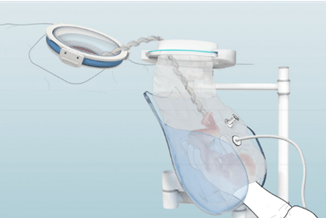
The baby can be carefully transferred to the artificial uterus via the biobag at the correct temperature, through a glove.
CERTIFICATION
The system that Van Haren is currently developing consists of several components. Think, for example, of a mechanism that supports the doctor during transfer, as the combination of fetus and fluid can become quite heavy.
Of all these parts, the wound spreader is already in medical use and therefore clinically certified. The rest of the system is completely new and must go through a rigorous clinical approval process. Delbressine: “That’s logical, what we are doing is brand new. Pioneering. It will therefore be years before we can actually start using this system.”
The two are in close contact with the working field, such as specialists from the Máxima Medical Center in Eindhoven. Van Haren: “It’s a nice interaction, we get a lot of feedback from doctors. They have the medical knowledge, we know how to design systems.”
SENSES
There is a lot involved in developing the artificial uterus itself. Elements must be taken into account that you might not immediately think about at first. Delbressine: “At 24 weeks, the senses are still developing, and babies are sensitive to light, sound and vibrations. The impulses they receive in the natural womb we try to imitate in the artificial womb. The senses need to be stimulated, but in such a way that the brain can handle it. This is still work in progress”
There is still a lot of work to be done before the system can actually be used. We’re talking years. For Delbressine and Van Haren, no problem. Their driving force is in helping children. Van Haren: “Improving the lives of premature babies and increasing their chances of living a beautiful life, that’s what we ultimately do it for.”
COOPERATION
Perinatal Life Support is a larger partnership that conducts research into a ‘Perinatal Life Support’ system. Partners are TU/e, the universities of Aachen and Milan, and the companies LifeTec Group and Nemo Healthcare. In 2024 the European funding (from Horizon 2020) ends, then the prototype of the artificial uterus must be ready. After that, the preclinical and clinical tests and the certification process will start.


Nature: free, accessible, healing

Forest Bathing | Shinrin-Yoku | Healing in Nature | Short
Learn how to create healing experiences in nature for yourself and your loved ones. Visit the link for a course on Shinrin-yoku / Forest bathing. Learn calming nature meditations, forest bathing exercises, and mindfulness activities that reconnect us with nature and ourselves. Please share the forest calm and spread some healing.
City Dweller? You can do this!
SELF GUIDED FOREST BATHING/UNIVERSITY OF WASHINGTON BOTANICAL GARDENS



We’re Going On A NATURE HUNT

Nov 24, 2020 Stories For Kids
Come join in the adventure of a nature hunt. This book is written by Steve Metziger and illustrated by Niki Sakamoto. Thanks for listening!

Medical empirical research on forest bathing (Shinrin-yoku): a systematic review
Abstract
Aims
This study focused on the newest evidence of the relationship between forest environmental exposure and human health and assessed the health efficacy of forest bathing on the human body as well as the methodological quality of a single study, aiming to provide scientific guidance for interdisciplinary integration of forestry and medicine.
Method
Through PubMed, Embase, and Cochrane Library, 210 papers from January 1, 2015, to April 1, 2019, were retrieved, and the final 28 papers meeting the inclusion criteria were included in the study.
Result
The methodological quality of papers included in the study was assessed quantitatively with the Downs and Black checklist. The methodological quality of papers using randomized controlled trials is significantly higher than that of papers using non-randomized controlled trials (p < 0.05). Papers included in the study were analyzed qualitatively. The results demonstrated that forest bathing activities might have the following merits: remarkably improving cardiovascular function, hemodynamic indexes, neuroendocrine indexes, metabolic indexes, immunity and inflammatory indexes, antioxidant indexes, and electrophysiological indexes; significantly enhancing people’s emotional state, attitude, and feelings towards things, physical and psychological recovery, and adaptive behaviors; and obvious alleviation of anxiety and depression.
Conclusion
Forest bathing activities may significantly improve people’s physical and psychological health. In the future, medical empirical studies of forest bathing should reinforce basic studies and interdisciplinary exchange to enhance the methodological quality of papers while decreasing the risk of bias, thereby raising the grade of paper evidence.
Source:https://environhealthprevmed.biomedcentral.com/articles/10.1186/s12199-019-0822-8

Windsurfing Serbia Surduk 2020 50 kts
lunelun – Dec 8, 2020 un
Windsurfing in Serbia on Danube river. Wind 50 kts, sales 3.7-4,7 m2, boards 74-100l.

