


GLOBAL PRETERM BIRTH RATES – ETHIOPIA
Estimated Number Of Preterm Birth Rates – 11.97 per 100 live births
(Global Average: 10.6, USA: 9.56)
Ethiopia, officially the Federal Democratic Republic of Ethiopia, is a landlocked country in the Horn of Africa. It shares borders with Eritrea to the north, Djibouti to the northeast, Somalia to the east and northeast, Kenya to the south, South Sudan to the west, and Sudan to the northwest. Ethiopia has a total area of 1,100,000 square kilometres (420,000 square miles). As of 2022, it is home to around 113.5 million inhabitants, making it the 13th-most populous country in the world and the 2nd-most populous in Africa after Nigeria. The national capital and largest city, Addis Ababa, lies several kilometres west of the East African Rift that splits the country into the African and Somali tectonic plates.
The World Health Organization‘s 2006 World Health Report gives a figure of 1,936 physicians (for 2003), which comes to about 2.6 per 100,000. A brain drain associated with globalization is said to affect the country, with many educated professionals leaving Ethiopia for better economic opportunities in the West.
Ethiopia’s main health problems are said to be communicable (contagious) diseases worsened by poor sanitation and malnutrition. Over 44 million people (nearly half the population) do not have access to clean water. These problems are exacerbated by the shortage of trained doctors and nurses and health facilities.
The state of public health is considerably better in the cities. Birth rates, infant mortality rates, and death rates are lower in cities than in rural areas due to better access to education, medicines, and hospitals. Life expectancy is better in cities compared to rural areas, but there have been significant improvements witnessed throughout the country in recent years, the average Ethiopian living to be 62.2 years old, according to a UNDP report. Despite sanitation being a problem, use of improved water sources is also on the rise; 81% in cities compared to 11% in rural areas. As in other parts of Africa, there has been a steady migration of people towards the cities in hopes of better living conditions.
Source- WHO 2014- https://ptb.srhr.org/
COMMUNITY

Neonatal mortality in neonatal intensive care unit hospitals in Ethiopia remains unacceptably high: a systematic review and meta-analysis: Magnitude and determinants of neonatal mortality in NICU

Gizachew Tadele Tiruneh , Tesega Mengistu Birhanu, Abdurahaman Seid, Mahteme Haile Workneh, Dareskedar Getie, Tenagnework Antefe Abebe, Ambanesh Necho Mulat, Taye Zeru Tadege, Kassahun Alemu Gelaye, Tadesse Awoke Ayele
Abstract
Background: In Ethiopia, the neonatal mortality rate has not shown significant changes over time and is among the highest in the world. This review aimed to explore the pooled magnitude and determinates of neonatal mortality in the neonatal intensive care unit hospitals in Ethiopia.
Methods: The research team retrieved global peer-reviewed journal articles available as electronic databases including PubMed, Popline, and Scopus databases. Random-effects meta-analysis model was used to pool the estimates of the magnitude of mortality among studies. The results were presented as the pooled estimates (odds ratio and proportion) with 95% confidence intervals, at less than 0.05 significant levels.
Results: In this review, 10 studies were included with a total of 8,729 neonates. Of these, 1,779 (20.4%) neonates died in the neonatal intensive care unit. The pooled neonatal mortality rate was 19.0% (95% CI: 14.0-25.0). The neonatal mortality is three times higher among early age (OR: 2.80; 95% CI: 1.45-5.40) and preterm newborns (OR: 3.27; 95% CI: 2.12-5.07) than their counterparts. Early age of the newborn, prematurity, low birth weight, perinatal asphyxia, mode of delivery, hypothermia, late initiation of breastfeeding, and having antenatal care visits were the main determinants for neonatal mortality.
Conclusion: Neonatal mortality in the intensive care unit is high. It is unacceptably high amongst early and preterm neonates. Special care for preterm and early age newborns, timely initiation of breastfeeding, exclusive breastfeeding, and appropriate mode of delivery, essential obstetric and newborn care, and promoting antenatal visits are recommended to reduce neonatal mortality.
Source:https://emjema.org/index.php/EMJ/article/view/1588

Saving babies’ lives in Ethiopia
Paul Driscoll Aug 5, 2021
It was Rahel Beyan’s lifelong ambition to nurse people back to health. In Tigray, Ethiopia, where she lives, she’s been working as a nurse alongside VSO volunteer Miriam Etter to improve conditions at Suhul Hospital – making her dream a reality.

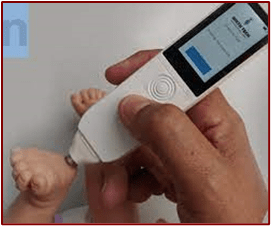
Maternova Enters Distribution Agreement for Preemie-Test, the First Medical Device Capable of Accurately Assessing a Newborn’s Gestational Age

Hand-held, noninvasive device uses light to identify preterm newborns by analyzing the photobiological properties of the baby’s skin
July 27, 2022
PROVIDENCE, R.I.–(BUSINESS WIRE)–Maternova Inc., empowering global health through innovative solutions, today announced that they have signed an agreement with BirthTech Lda, Portugal, to distribute its Preemie-Test in multiple geographies around the world. The Preemie-Test is the first medical device clinically proven to accurately assess the gestational age of a newborn, which is the major marker of neonatal survival. Maternova has an exclusive distribution agreement across Africa, Asia (except India) and Latin America (except Brazil) and non-exclusive rights in Brazil, India, the United States and Europe. Initial areas of regulatory approval and marketing focus for the Preemie-Test are Peru, Colombia, Philippines, Bangladesh and specific states in India.
Immediately after childbirth, a newborn with unknown or unreliable gestational age often requires resuscitation and hospitalization. Without this critical care, preterm newborns are at risk of mortality or serious, life-long health problems. According to the WHO, every year around 15 million babies are born too early and one million die due to prematurity complications. While most of these lives could be saved with prompt prematurity identification, in the absence of a prenatal ultrasound (often too expensive and not accessible), there has been no reliable method for pregnancy dating.
“The commercial launch of the Preemie-Test is a significant milestone in providing a new way of measuring gestational age and addressing a crucial need in low-resource settings,” said Rodney Guimarães, PhD, BirthTech CEO and the inventor of the device. “With a shared commitment to maternal and infant healthcare, we are proud to work with Maternova and believe its unique distribution network will help us quickly place this cost-effective solution into the hands of healthcare professionals from midwives to obstetricians.”
“I am delighted we were selected to commercialize and distribute the Preemie-Test,” said Meg Wirth, founder and president of Maternova. “Demand for effective and affordable maternal, newborn and child health innovations continues to grow across the globe. The Preemie-Test answers the call for a highly accurate solution that can be used in time-sensitive situations where self-sufficiency and portability are essential to newborn lives.”
Maternova is an exhibitor at the Florida International Medical Expo (FIME 2022) being held at the Miami Beach Convention Center from July 27-29. Representatives, including the inventor of the device, will be at booth V64 to demonstrate the Preemie-Test.
About the Preemie-Test
- Portable, hand-held device
- Rapid, accurate results
- Easy to use
- Noninvasive
- Affordable
The Preemie-Test is the first medical device capable of accurately assessing gestational age within +/- 4 days immediately after an infant is born. The hand-held device features a probe containing light emitters and receivers that is applied against the newborn’s foot and, using mathematical algorithms, can estimate dating in a matter of seconds. This noninvasive optoelectronic device measures the thickness of the skin through backscattering of light using a light-emitting diode, and the battery lasts up to three years allowing hundreds to thousands of measurements. Support is available through a mobile app.
Multiple clinical trials to date have validated the effectiveness and 96% accuracy of the Preemie-Test in Brazil, Portugal, Mozambique, India and Malawi. According to ANVISA, the Brazilian regulatory health agency, this medical device is categorized as Class II Safety: Noninvasive and Medium Risk.
***WE really appreciated access to this Associated Video:

SOL ABA – Yene Nesh – የኔ ነሽ – ملكتي – New Ethiopian music 2022 – (Official video)
#Ethiopianmusic #Sol_Aba #eritreanmusic 1,611,376 views Dec 9, 2022 BAHGNA TV Ethiopian amharic music /Yene Nesh/ 2022/2023 bahgnatv production – Yene Nesh – amharicmusic


HEALTHCARE PARTNERS

National Prevalence of Social Determinants of Health Screening Among US Neonatal Care Units
NOVEMBER 01 2022
Erika G. Cordova-Ramos, MD; Stephen Kerr, MPH; Timothy Heeren, PhD; Mari-Lynn Drainoni, PhD; Arvin Garg, MD, MPH; Margaret G. Parker, MD, MPH

OBJECTIVES
The extent that universal social determinants of health (SDH) screening in clinical encounters, as recommended by the American Academy of Pediatrics, has been implemented in inpatient pediatric settings is unknown. We aimed to determine the national prevalence and predictors of standardized SDH screening in US level 2 to 4 neonatal care units (NICUs), describe characteristics of SDH screening programs, and ascertain beliefs of clinical leaders about this practice in the NICU setting.
METHODS
We randomly selected 100 hospitals with level 2 to 4 NICUs among each of 5 US regions (n = 500) and surveyed clinical leaders from January to November 2021 regarding standardized SDH screening. Responses were weighted for number of level 2 to 4 NICUs in each region and nonresponse.
RESULTS
Overall response rate was 34% (28%–40% by region). Twenty-three percent of US level 2 to 4 NICUs reported standardized SDH screening. We found no associations of hospital characteristics, such as region, size, or safety-net status, with implementation of this practice. Existing programs conducted systematic screening early in the hospitalization (84%), primarily led by social workers (92%). We identified practice variation regarding the type of screening tool, but there was substantial overlap among domains incorporated in the screening. Reported barriers to implementation included perceived lack of resources, inadequate referrals, and lack of an inpatient screening tool.
CONCLUSIONS
The prolonged neonatal hospitalization provides opportunities to systematically address SDH. Yet, only 23% of US level 2 to 4 NICUs have implemented this practice. To scale-up implementation, quality improvement may support adaptation of screening and referral processes to the NICU context.

Fostering Resilience to Very Preterm Birth Through the Caregiving Environment

Trecia A. Wouldes, BA, MA, PhD1 – October 21, 2022 JAMA Netw Open. 2022;5(10):e2238095. doi:10.1001/jamanetworkopen.2022.38095
Preterm birth remains an important public health challenge for improving the quality of immediate and long-term care of the child and their family. Nearly 1 in 10 live births worldwide are preterm, with higher rates in marginalized populations and developing countries.1 Advances in medical intensive care of these infants mean more infants born very preterm and extremely preterm are surviving. The preponderance of research on children born very preterm has revealed the linkages between numerous risks and acute and long-term adverse health and developmental outcomes for the children, and social and psychological challenges for the families.2 Although children born earlier in gestation are at increased risk for poor outcomes, there is wide variability, with many children doing well. Therefore, research that can identify the protective factors or identify who, when, or under what circumstance some preterm children thrive is essential for informing interventions to assist those preterm children who are at risk of ongoing emotional problems. Very preterm (<32 weeks’ gestational age) and very low birth weight (<1500 g) children are more at risk than their full-term peers for developing internalizing symptoms (eg, anxiety and/or depression). Emerging evidence suggests that maternal sensitivity is a long-term resilience factor in the development of internalizing problems in early adolescence in very preterm children.
McLean et al provide further evidence that supportive parenting of infants born very preterm is associated with more optimal emotional outcomes across early and middle childhood. They report the findings from a prospective, longitudinal cohort study of 186 very preterm neonates (24-32 weeks’ gestational age) recruited from the level III neonatal intensive care unit (NICU) at BC Women’s Hospital in Vancouver, Canada. This report aimed to investigate whether neonatal pain-related stress experienced by neonates in the NICU was associated with trajectories of internalizing behaviors at ages 1.5 (159 children), 3.0 (169 children), 4.5 (162 children), and 8.0 (153 children) years and whether supportive parenting behaviors and lower self-reported parental stress at ages 1.5 and 3 years attenuated this association. Cumulative pain and stress was defined as the number of invasive procedures performed in the NICU. The main outcome was parent reports of child internalizing behaviors measured with the Child Behavior Checklist at every follow-up. At ages 1.5 and 3 years, parental stress was obtained from the Parenting Stress Index, and parent-child interactions were obtained from videotapes of a 5-minute teaching task coded by independent examiners using the Emotional Availability Scale–IV. After accounting for gestational age at birth and neonatal clinical factors, greater exposure to neonatal pain-related stress, related to invasive procedures from birth to NICU discharge, was associated with increased internalizing symptoms across follow-up. At 1.5 years, internalizing behaviors were within the normative range; however, by age 8 years, parent reports indicated that 24 of 153 children (16%) had symptoms that put them in the clinical range for internalizing behaviors. Latent profile analyses of parenting behaviors observed in parent-child interactions at ages 1.5 and 3 years and parenting stress at 3 years identified 3 profiles: average support with average stress, high support with low stress, and low support with high stress. Higher parenting stress at 1.5 years contributed to parent reports of greater internalizing problems across development to age 8 years. At age 3 years, the profile of high support and lower stress was associated with a reduction in the development of parent reports of internalizing behavior across development to age 8 years. Parents in this group demonstrated more behaviors that were characterized as sensitive, nonhostile, and nonintrusive and provided more structure in parent-child interactions.
The Bidirectional Nature of Parenting
Although sensitive supportive parenting in the general population is important for a child’s development, it is even more critical for preterm-born children. However, the communication abilities, atypical behavior, and regulation systems of very preterm-born children can affect the quality of these interactions. McLean et al found at 3 years, but not 1.5 years, children exhibited lower parent-reported internalizing behaviors related to supportive parenting interactions, even after accounting for child behavior in parent-child interactions in a teaching task.
Supportive parenting interactions rely on several social and psychological determinants of the mother-infant dyad, including maternal culture, depression, socioeconomic status, substance use disorders, the home environment, and whether the child was unplanned or unwanted.5 The prevalence rates of posttraumatic stress or acute stress disorders in mothers of preterm infants in the NICU range from 23% to 28%. Several factors contribute to the traumatic stress experienced by parents of preterm infants in the NICU; however, the most stressful aspects of the NICU experience reported by parents were the physical separation from their infant and their feelings of a loss of control and helplessness in their inability to shield their infant from the numerous painful procedures.7 The findings of McLean et al4 show that reduced parental stress and sensitive supportive parenting may temper the association between the effects of neonatal pain-related stressors in the NICU and internalizing behaviors throughout early and middle childhood. Therefore, interventions that help reduce stress should be part of postnatal care for mothers of very preterm children.
Where to Now?
Many of the stressors experienced by neonates and parents in the NICU and after discharge from the hospital have been addressed by interventions in the NICU, such as the Newborn Individualized Developmental Care and Assessment Program. This intervention is designed to identify both what is supportive and regulating, and what is disruptive to infant neurodevelopment. Further approaches include the redesign and reorganization of the NICU environment from large, open bays with multiple babies close to each other, to single-family rooms combined with neuroprotective approaches that emphasize developmentally appropriate care. The transition to single-family rooms aims to protect the infant from intrusive environmental stimuli of open bay NICUs while facilitating parental care and around-the-clock family presence.
Notwithstanding the advances made in caring for these vulnerable infants in the NICU, there are important questions left to answer. Preterm birth is increasing worldwide,1 but most studies on very preterm infants have involved White Western populations. The cohort in the study by McLean et al was predominantly a more mature, well-educated sample of parents (60% White and 84% with partial or complete university degree or postgraduate degree) with universal access to health care. Culture, poverty, and maternal mental well-being strongly influence parenting; therefore, more research is needed to determine who and under what social and psychological circumstances parents of children born very preterm require parenting support.
In addition, parental perceptions and attitudes toward the child born very preterm may be distorted and impact the developing parent-child relationship, particularly in circumstances where the pregnancy was unintended or unwanted. With the recent legal constraints to obtaining terminations for unintended or unwanted pregnancies, maternal mental health, stress, and the financial burden of very preterm birth is likely to escalate, particularly in already marginalized populations. Therefore, research is needed to understand what the potential impact of the lack of access to termination of an unwanted pregnancy will have on parenting very preterm infants.
Source:https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2797555?resultClick=1

Futility and Withdrawal of Intensive Care in Term Infants with Brain Injury

Ciara Terry, MRCPI , Breda C Hayes MD, FRCPI
Neonatal brain injury is a major challenge in modern perinatal care, including obstetric and neonatal care. Advances in the care of the newborn, including resuscitation improvements and the introduction of therapeutic hypothermia (TH) for the management of neonatal encephalopathy, have allowed us to sustain and improve life for babies that previously may have been deemed too unwell to continue life-sustaining treatments. From an obstetric perspective, there has been an increase in the detection of serious fetal anomalies with better antenatal scanning regimes and the use of MR imaging in fetal medicine to detect congenital brain malformations.
The decision to redirect the focus of care to comfort-only measures usually follows a detailed neurological examination of the baby in conjunction with neuroimaging (typically MR imaging) aided by EEG monitoring when available. Congenital causes of severe brain dysfunction, such as severe congenital brain malformations (e.g., giant encephalocele, lobar holoprosencephaly) leading to a plan for palliative care following delivery, are encountered. However, most term babies where palliative care is initiated do so following acquired perinatal brain injury. Major conditions that lead to the development of perinatal brain injury include hypoxic ischaemic encephalopathy (HIE), perinatal stroke, perinatal central nervous system infection, and intracranial haemorrhage. Hypoglycaemia can result in brain injury or potentiate injury due to other causes, e.g., HIE.
HIE is one of the commonest reasons for acquired brain injury in the normally formed term newborn. The incidence of HIE is approximately 1.5 per 1000 births, and globally there are 700,000 cases of death or disability from birth asphyxia annually. Therapeutic hypothermia (TH) has resulted in significant improvements in the outcomes of neonates with HIE. However, greater than 40% of neonates who undergo TH will still have impaired neurological outcomes at school-going age. TH does not improve outcomes in babies with severe HIE.
A perinatal stroke is a cerebrovascular event occurring between 20 weeks gestation and up to 28 days after birth. Prevalence has been estimated at 1/1600 to 1/5000 live births and is recognised as the second most common cause of neonatal seizures after neonatal encephalopathy accounting for up to 20% of neonatal seizures . Presentation is usually in the first three days after birth. The outcome of neonates with perinatal stroke is difficult to predict.
Intracranial haemorrhage in term infants is rare but can result in significant neuro disability. Intracranial haemorrhage can be epidural, subdural, subarachnoid haemorrhage, or intracerebral.
Central nervous system infections, including meningitis and encephalitis, can be bacterial, viral, or fungal in aetiology. The incidence of early-onset meningitis is approximately 0.39 per 1000 live births. Herpes virus infection is the most common non-bacterial cause of central nervous system infection, with an estimated incidence of 1 in 50,000 live births, and can lead to severe neurodevelopmental delay.
Being told that their newborn has a brain injury is amongst the most devastating news that parents can receive. Existing data suggests that parents of encephalopathic neonates experience predictable communication difficulties. Medical information is complex and uncertain prognosis is challenging. It is well-accepted that parents value participation in medical decision-making. Parent-centered decision-making is preferred in the NICU when discussing longer term goals and potential harm. The fundamental goal of shared decision-making is to open the process to benefit from both the physician’s and the parent’s respective experiences, knowledge, and beliefs. This does not imply a value-neutral role for clinicians but instead requires a more delicate balancing as an advocate for the baby while respecting parental views. Parents who perceive a shared role in end-of-life decision-making may experience less long-term grief than parents who perceive either making the decision on their own or having no involvement. Palliative care teams are an important source of added support to all caregivers. Attempting prognostication in neonatal encephalopathy is essential to help parents formulate their concept of best interest for their newborn. However, estimating prognosis is complicated by the wide range of potential neurodevelopmental outcomes, evolving course, and role of extrinsic factors like access to rehabilitation. Even in cases of anticipated death, infants may unexpectedly survive. In the face of uncertainty, describing the best case, worst case, and most likely outcome is an effective strategy to characterize the potential range of outcomes.
Clinical history, neurologic examination, serum biomarkers, neurophysiology [amplitude-integrated electroencephalography (aEEG) or EEG], near-infrared spectroscopy, and magnetic resonance imaging have all been studied as predictors of severe neurologic injury and poor outcome, although none is 100% predictive. Serial evaluation over time facilitates discussion regarding anticipated poor prognosis and decision-making for transition to comfort care. Serial assessments with a particular test are more predictive than a single observation. The time over which a test remains abnormal together with the trend over time yields the best information(9). Thus far, brain monitoring in the form of aEEG and conventional EEG seems to be the best objective tools to identify the highest-risk patients. Specifically, a severe depression or burst suppression pattern which persists is suggestive of poor outcome. Magnetic resonance imaging (MRI) is known to retain its predictive abilities when performed in the window of 5-10 days after birth. Where MRI is performed, the pattern and extent of injury remain important predictors of outcome even after TH. However, MRI is sometimes not possible due to clinical instability or accessibility. In these cases, cranial ultrasound is important and predictive if it shows hyperechogenic subcortical grey matter structures (basal ganglia and thalamus) and/or focal parenchymal lesions. The presence of cystic lesions early in the neonatal course is also predictive of poor outcome and helps to identify prenatal injury. Many scoring systems are available and can be applied to help predict outcomes, including the Barkovich and the Rutherford scoring system. The Weeke scoring system is a comprehensive scoring system that assesses several different functional areas of the brain, including motor, visual, and memory. Complete and careful neurological examination remains of critical importance. In predictive models, time to improvement in stage and time to reach no or mild HIE were important predictors of death/disability. The advent of bedside aEEG allows neonatologists to continuously trend the background pattern and hence the degree of recovery alongside serial clinical examination during TH. In cases where clinical examination and EEG are in keeping with profound injury, and there is no sign of improvement over 24-48 hours, MRI brain does not add greatly to prognostication. However, MRI should be considered in this setting if the baby has received anti-epileptic medications, which may affect the reliability of both clinical examination and EEG findings.
The term life-limiting condition refers to any illness for which there is no reasonable hope of cure and where the child is unlikely to survive beyond early adulthood. Many of these conditions cause a progressive deterioration leaving the child increasingly dependent on their family or carers. Such illnesses have been categorised into four categories . The fourth category includes conditions leading to severe disability and the likelihood of premature death, such as severe cerebral palsy and multiple disabilities following brain injury.
Decisions that involve the withdrawal or withholding of life-sustaining treatment should have the child’s best interest as the central focus(7). A futile intervention is different from an intervention that is not pursued because it is not perceived to be in the overall best interests of the child. With shared decision-making, medical facts must be reflected alongside the family’s preferences, values, and goals. Even when care is not futile, care may be against the child’s best interests when the likely harms outweigh possible benefits (6). Perinatal palliative care input is paramount in the care of the term neonate with significant brain injury. Palliative care stages have been defined in the British Association of Perinatal Medicine Framework for Clinical Practice in Palliative Care. This describes a transition period from routine or intensive care to palliative care. Supportive care includes considerations for oral nutrition, hydration, and analgesia. The overall goal of palliative care is to achieve the best quality of life for patients and their families.
In conclusion, decisions around the futility of care and redirection to comfort measures for newborns with brain injury is a complex decision that should only occur following a process of shared decision-making involving all caregivers for the baby. Certainty about prognosis is not possible despite advances in medical care, but clear and honest discussions with parents are paramount to the decision-making process. The involvement of palliative care physicians is recommended in patients with severe brain injury leading to a life-limiting condition.
Source:http://neonatologytoday.net/newsletters/nt-dec22.pdf

More male midwifes in Ethiopia | METROPOLIS

Metropolis Jan 31, 20
In Ethiopia, a large proportion of midwives are men. Like Gashaw, who lost a beloved neighbor during childbirth. Metropolis is a video project by Dutch broadcast organizations HUMAN and VPRO, that started in 2008. Metropolis is made by a global collective of young filmmakers and TV producers, reporting on remarkable stories from their own country or city. More videos and full episodes on http://www.human.nl/metropolis


PREEMIE FAMILY PARTNERS

Without additional support, families of preemies can fall through the cracks
Families of prematurely born babies are calling for increased paid leave, insurance, and mental health support to manage the emotional and economic impacts.

Pamela Appea – March 30th, 2022
Brooke Jones was in her late 20s when she became pregnant with her first child. Employed full-time as a medical assistant in Connecticut, Jones fully expected to work right up until her due date. Jones described her pregnancy as “normal” and didn’t believe she had any symptoms that were significantly worrisome. But that changed when a routine ultrasound at 25 weeks revealed that her amniotic fluid levels were dangerously low. Shortly after, medical professionals realized Jones’ blood pressure had spiked “through the roof,” she told Prism. She was diagnosed with preeclampsia and was admitted to the closest hospital for immediate treatment.
“They told me I might give birth that day,” Jones said. She was subsequently transferred to Yale New Haven Children’s Hospital, where she was treated for a host of other complications, including fluid buildup in her lungs, which meant Jones had to go on medical leave immediately. “I was on autopilot,” she said.
After two weeks of strict hospital bedrest, Jones gave birth to her baby boy at 27 weeks via an emergency C-section. A micro preemie, he weighed only 1 pound, 8 ounces at birth. Earlier in her pregnancy, Jones had carefully thought about her maternity-leave schedule, finances, childcare logistics, and more, but suddenly she needed a whole new plan.
But as Jones discovered, balancing medical care, a lack of work leave and the need for aftercare support and mental health counseling as a caregiver often proves challenging for families with preemies. Jones’ son spent four months in the neonatal intensive care unit (NICU), where doctors treat sick and premature newborns, but her maternity leave only lasted six weeks after he was born, so she had to go back to work long before he was released from the hospital.
In search of emotional and mental health support
Women of color like Jones, who is Black, compose a significant number of parents who give birth prematurely. According to the March of Dimes, over 380,000 babies are born preterm every year in the U.S. about 1 in 10 of every live birth. Black and Indigenous women are 60% more likely to give birth preterm than white women.
For the families of preemies, the whole birth experience can be fraught. Often, preemie caregivers aren’t given a lot of time to process that their baby may have short- and long-term medical, developmental, and other complications that require a NICU stay, high-risk surgeries, and other medical procedures.
Additionally, caregivers can feel overwhelmed and experience a wide range of postnatal mental health issues, including depression, anxiety, guilt, and NICU-specific PTSD.
“The caregivers’ primary need is emotional support. Prematurity is something that is a surprise, and it has a very traumatic effect on the family,” said Tina Tison, executive director of the Tiny Miracles Foundation. The Connecticut-based nonprofit partners with several hospital NICUs in the area to provide counseling, mentoring, and socio-emotional support to preemie caregivers. Jones received peer mentor support and financial assistance from The Tiny Miracles Foundation after the birth of her son, including during his lengthy four-month hospitalization in the NICU.
“Any caregiver takes comfort in knowing that they are not alone,” said Tison.
Aftershocks of the pandemic continue to impact caregivers well after their baby has been discharged from the NICU, according to Dr. Angelica Moreyra, an expert in perinatal mental health at the Children’s Hospital in Los Angeles.
“There is currently an enhanced need for advocacy for our families that we serve due to environmental stressors that create barriers for caregiver presence in the unit such as public transit … changes in school and child care options, increased financial, occupational, and housing instability, and more,” Moreya told Prism. “When caregivers encounter barriers in being able to present in the unit, it impacts the nature of our services, as we are focused on supporting bonding/attachment between caregivers.”
Balancing work and care
Apart from the mental and emotional strain, the economic impact of having a preemie can also be significant. According to the March of Dimes, the average NICU bill starts at $65,000. But depending on surgeries, medical procedures, and other complications, many families are expected to pay hospital bills that are hundreds of thousands of dollars or higher. For many, access to health insurance or emergency state health insurance for preemies is crucial. However, more than 2.2 million women in the U.S. live in “maternity care deserts” where families often lack access to necessary prenatal care or don’t have health insurance to cover the costs.
Prematurely born babies are eligible to receive Medicaid and Supplemental Security Income through Social Security. Regardless of a parent’s income level, state insurance typically covers nearly all of the child’s NICU hospital bills, surgeries, post-discharge medical treatment, and other medical and mental health services for both the caregiver and the baby during their first year. Speech, occupational therapy, physical therapy, and other rehabilitative services are typically covered either through insurance, early intervention, and occasionally through Department of Education public education services after the age of 3-5, depending on the state. However, the process for access to these services is fraught with governmental red tape, making it difficult for caregivers to access.
Even as families face mounting expenses, without extra paid leave caregivers of preemies can find it difficult to hold onto a full-time job given the need for medical appointments, early intervention services, special education services, evaluations, operations, and other treatments for medical issues preemies may struggle with even after “graduating” from the NICU. While Jones’ son’s medical bills and her mental health care were covered by state insurance, her husband ultimately left his job to manage their son’s care and medical appointments.
Working toward policy shifts
As Jones and her husband have looked toward the future and considered having another baby, they’ve become doubtful about the financial feasibility. Without the same state Medicaid services, more paid family leave, and the ability to take time off work for medical appointments, Jones said she was unsure they could afford another child. Her family is far from alone, and advocates for families of preemies argue that a number of policy changes need to be put in place to provide caregivers the support they need, including ensuring universal access to public health insurance programs and a minimum of 12 weeks of paid family leave, with more for families of babies with more significant health and developmental needs. March of Dimes is also pushing for the elimination of racial and geographic disparities in prenatal care and expanded access to coverage for doula and midwifery support to offer caregivers more options both during and after birth.
If she could wave a magic wand around government policy changes for family caregivers, Jones told Prism: “Let us have our time as caregivers with our children. For me, I only got six weeks. Some people are allowed more time. But as a law, I wish it was implemented to give mothers and fathers the [paid] time we need with our kids.”
Source:https://prismreports.org/2022/03/30/additional-support-families-preemies/

Common NICU Discharge Tests
While you’re learning all you can about your baby’s care, the discharge coordinator or case manager is planning your baby’s final tests and making preparations for discharge. Common discharge tests are explained here, but not all NICU babies require all of the tests discussed. Ask your baby’s nurse what to expect as discharge draws near.
Eye exam
If your baby was 30 weeks’ gestation or less or weighed less than 1,500 grams (3 pounds, 5 ounces) at birth, they will have an eye examination at between 4 and 7 weeks of age. Babies born after 30 weeks’ gestation and weighing between 1,500 and 2,000 grams may also have this type of eye examination if they had an especially difficult NICU course. Follow-up exams will be scheduled if the findings of the first exam warrant them. The exam is to identify any changes in the eye tissue caused by retinopathy of prematurity.
Hearing test
Hearing tests—also called audiology screenings—are done in most nurseries before discharge. Electronic sound and response monitoring determine if your baby can hear. Environmental conditions, such as surrounding noise or a crying baby, can cause inconclusive results, however. If this happens, a retest should be scheduled in a more controlled environment. If your baby responds to your voice or to noise-making toys held where they can’t see them, there is usually no reason for concern.
After discharge, your child’s hearing should be monitored by your health care provider at periodic health exams. If you are concerned about your baby’s hearing, never hesitate to insist on a more extensive hearing exam. These are available at a pediatric audiologist’s office or in pediatric outpatient rehabilitation centers.
Newborn metabolic screening
Every baby is tested soon after birth to identify some rare but potentially serious or life-threatening conditions. The number of tests varies by state. Newborn metabolic testing can yield inconclusive results if the baby is very premature, is critically ill or needed a blood transfusion prior to metabolic testing. If the screening test suggests a problem, your baby’s doctor will speak directly with you and will order follow-up testing. Become aware of the screening test results prior to discharge from the NICU and communicate the findings with your community pediatrician.
Blood count
A final hematocrit or hemoglobin and reticulocyte level are usually done the week of discharge. Although it’s unlikely, your baby might be anemic and either need a blood transfusion or iron medication to help their bones make new red blood cells. If so, follow-up lab tests will usually be done in the pediatrician’s office or an outpatient clinic.
Sleep study (pneumogram)
Infants with continuing apnea and bradycardia may have a special test to help determine the cause of these episodes. Depending on your region of the country, the test is called a sleep study, a pneumocardiogram, or a pneumogram. Philosophies vary regarding the use of pneumograms, and not all NICUs use them. A pneumogram does not answer every question about the baby’s apnea and bradycardia, and interpretations of the test vary regionally. The American Academy of Pediatrics (AAP) states that “pneumograms are of no value in predicting sudden infant death syndrome (SIDS) and are not helpful in identifying patients who should be discharged with home monitors.”
Cranial ultrasound
If your baby was born younger than 30 weeks’ gestation, she has probably had several ultrasounds of her head to detect intraventricular hemorrhage. Some NICUs will perform a cranial ultrasound or other brain imaging study near the time of hospital discharge for babies weighing less than 1,000 grams at birth. Your neonatologist may also suggest magnetic resonance imaging near your baby’s original due date to help predict the need for early intervention services and ensure the best possible developmental outcome. Sometimes a different brain imaging technique may show abnormalities that a screening ultrasound will not. This does not mean that the initial ultrasounds were misinterpreted, but merely that each test has limitations.
Last Updated 1/24/2023: https://www.healthychildren.org/English/ages-stages/baby/preemie/Pages/Getting-Ready-to-Leave-the-NICU.aspx

Father’s Perspective on Breast Feeding: A Cross-Sectional Questionnaire Based Study

Aparna Velmurugan, Prahankumar Rajendran, Manaikandan Mani
Abstract
Introduction
Despite global efforts to promote exclusive breastfeeding, the rates in India have been in the sub-optimal range. Higher levels of paternal support and encouragement are linked to better maternal confidence in breastfeeding. This study was aimed to assess the knowledge, attitude, and practice of fathers of infants towards the importance of breastfeeding practices.
Method
Fathers of infants visiting the Pediatric OPD, were interviewed with a structured, pre-tested questionnaire after obtaining written informed consent. This is a cross-sectional study where 158 fathers were given the questionnaire on knowledge, attitude, and practice about breastfeeding along with the sociodemographic details. The sections of the questionnaire were scored using the five-point Likert scale.
Results
Among the 158 fathers who participated in the study, majority (51%) had moderate scores in knowledge, attitude, and practice about breastfeeding. Around 131 fathers (83%) have not received any counseling about support and their role in breastfeeding and majority (58%) fathers felt the need to get education and training regarding parenting skills. Around 66% of the fathers were aware of the ideal duration of exclusive breastfeeding. About 35% of the fathers were not comfortable letting their wives breastfeed the child in public places. Around 25% of the participants had the idea that breastmilk production is reduced after child delivery through Cesarean section.
Conclusion
Fathers should have active participation during maternal check-ups, delivery, and antenatal counselling. This will help a better bonding and may lead to successful and prolonged breastfeeding. Educating fathers may help in increasing breastfeeding rates and duration.
Source:https://journals.sagepub.com/doi/abs/10.1177/09732179221130670

INNOVATIONS

Variation in NICU Head CT Utilization Among U.S. Children’s Hospitals
RESEARCH ARTICLE| JANUARY 09 2023 Megan M. Shannon, MD – Heather H. Burris, MD, MPH – Dionne A. Graham, PhD https://doi.org/10.1542/hpeds.2021-006322
OBJECTIVES:
Evaluate nationwide 12-year trend and hospital-level variation in head computed tomography (CT) utilization among infants admitted to pediatric hospital NICUs. We hypothesized there was significant variation in utilization.
METHODS:
We conducted a retrospective cohort study examining head CT utilization for infants admitted to the NICU within 31 United States children’s hospitals within the Pediatric Health Information System database between 2010 and 2021. Mixed effects logistic regression was used to estimate head CT, head MRI, and head ultrasound utilization (% of admissions) by year. Risk-adjusted hospital head CT rates were examined within the 2021 cohort.
RESULTS:
Between 2010 and 2021, there were 338 644 NICU admissions, of which 10 052 included head CT (3.0%). Overall, head CT utilization decreased (4.9% in 2010 to 2.6% in 2021, P < .0001), with a concomitant increase in head MRI (12.1% to 18.7%, P < .0001) and head ultrasound (41.3% to 43.4%, P < .0001) utilization. In 2021, significant variation in risk-adjusted head CT utilization was noted across centers, with hospital head CT rates ranging from 0% to 10% of admissions. Greatest hospital-level variation was noted for patients with codes for seizure or encephalopathy (hospital head CT rate interquartile range [IQR] = 11.6%; 50th percentile = 12.0%), ventriculoperitoneal shunt (IQR = 10.8%; 50th percentile = 15.4%), and infection (IQR = 10.1%; 50th percentile = 7.5%).
CONCLUSIONS:
Head CT utilization within pediatric hospital NICUs has declined over the past 12-years, but substantial hospital-level variation remains. Development of CT stewardship guidelines may help decrease variation and reduce infant radiation exposure.
Source:Variation in NICU Head CT Utilization Among U.S. Children’s Hospitals – PubMed (nih.gov)

Keypoints in movement analysis graphically displayed
Artificial intelligence and video as a resource to timely discover anomalies in premature babies
Published November 15, 2022

Due to an increased risk of various problems concerning growth, movement and development, premature babies are in need of special care. According neonatologist and professor of Pediatrics at the UMC Groningen, Arie Bos, it is important for early detection to discover possible anomalies on time in these premature babies, to minimize the consequences at a later age. In a movement analysis based on video images, such anomalies could be better assessed with the assistance of artificial intelligence.
At the University Medical Center Groningen (UMCG) 80 to 120 premature babies are admitted anually to the hospital from the provinces Groningen, Friesland, Overijssel and Drenthe. The babies end up on the Intensive Care Neonatology, which is the only intensive care unit for neonates out of eight hospitals in the Northern Netherlands. Due to a premature birth of ten weeks or more before the due date, these babies need special care. When the neonates are no longer in need of intensive care, they are transferred to one of the eight regional hospitals. There, the care is taken over by a pediatrician and the child is closer to the parents.
Periodic check
Periodic checks are of great importance in the case of an extreme preterm. Parent and child will visit the outpatient neonatology clinic of the UMCG during prebooked appointments to discover potential areas of concern in the development at an early stage. This consists of five moments in total, the first of which takes place when the baby is six months old and the last taking place when the child is eight years old.
The NeoLifeS cohort
To learn more about the development and most sufficient treatment of premature babies, the need arose for a central database of all the hospitals. In 2016, Bos together with his colleagues started NeoLifeS, a cohort with the purpose to identify problems and risk factors, and to improve the care for prematures. Premature babies are more at risk of various issues with growth, movement and development – including spasticity.
Within this cohort, data is collected on health and development issues of premature babies. The database contains information on the brain, lungs, eyes, respiration, the gastrointestinal system, infections, the placenta and on the start and course of the pregnancy of mother and child. Bos: “By systematically collecting and assessing clinical data of all the hospitals, of completed questionnaires by parents, and of movement patterns of the baby at three months past the calculated age, we can improve our intensive care for premature babies even further. After all, we want a bright and healthy future for these vulnerable kids.”
Since the start in 2016, after receiving permission from the parents, all clinical data of prematures has been collected from the moment of birth and stored in one databank. At present, the databank contains the data on 340 babies that were born before 30 weeks and/or weighed less than 1000 grams.
Movement analysis with own smartphone
Babies are often allowed to go home with the new parents if they are as old as they would originally be on the mother’s due date. This almost always occurs from one of the regional hospitals. Afterwards, it is essential that measurements are put in place to record the movements of the baby. Throug these measurement moments the baby is monitored for, amongst other things, spasticity. Spasticity occurs regularly and is often caused by a brain haemorrhage as a complication of preterm birth.
At the moment, spasticity is often only discovered after eighteen months. In the past this occured under the watchful eye of the specialist at the hospital, however, now, it can take place in a home environment, as the baby’s movements can be viewed with a smartphone. This new situation results in less stress for both parent and child, which ultimately provides a more reliable image.
Based on the video images, it is possible to determine whether there is a normal development or a potential anomaly as soon as three motngs. In this case, a rehabilitation specialist can be quickly called in for issues regarding arm and hand functions as a consequence of spasticity and these effects can be minimized when the child is older.
Timely recognition of certain patterns
The recorded video images are subsequently sent to the UMCG, where the NeoLifeS-team starts an analysis. The researchers watch approximately six to eight videos an hour, whereby it only takes 5 to 10 minutes of video to determine whether there is a case of normal or abnormal movement patterns and whether there is a need for closer examination. If it is suspected that there is a higher risk of a deviation in the motor development (especially spasticity), a consultation with the parents and the regional pediatrician is advised to refer to a rehabilitation center.
Bos explains: “The movement patterns at the age of three months is extremely important. With children that develop normally, you will see small, moderate speed, dancelike movements of the entire body, so in the shoulders, arms, hips, legs, torso and neck; then here, then there. Children who have a spastic movement disorder later on, do not display these movements at all. This knowledge has existed for a while, but only in the last few years we have discovered that by starting targeted therapy early, we can greatly improve the future results of children with spasticity.”
Technology as an essential factor
Neolook Solutions supports NeoLifeS with the development and expansion of the used movement analysis, which is internationally known as the General Movement Assessment (GMA). Marco D’Agata, Managing Director at Neolook Solutions: “UMCG is the national academic expertise center for the General Movement Assessment. If we want the GMA to be accessible for those thousands of children who are at risk every year in the Netherlands, just like in other countries, than we better work together with existing parties such as NeoLifeS.”
Neolook thinks ahead: where previously the specialist received the parents in the hospital or the nurse came by the house to record the video, it is now possible to virtually visit the parents. A livestream provides the nurse or the specialist with a direct view of the child. This takes less time and causes less stress for both the parent and the child. The video is then safely stored at the UMCG for the team of NeoLifeS to watch and analyse the video at a suitable moment.
Innovation with Artificial Intelligence
The next step in the process is to apply artificial intelligence. By visualizing the movements in the video with so-called ‘key points’ (key points which together form a wire figure of the child), potential deviations can be recognized by artificial intelligence software. Artificial intelligence makes it possible to automatically detect certain patterns in the movement of new-born babies. The application of the abovementioned form of artificial intelligence in the movement analysis of NeoLifeS can enable the specialists whom assess the movements to be more efficient and better supported in the assessment process.
The results from the recording are graphically displayed for the specialist, with any peculiarities being highlighted. Thus, the specialist can immediately investigate possible anomalies. The application of artificial intelligence in the movement analysis therefore supports the specialists in their tasks and speeds up the assessment process.
D’Agata: “You cannot use just any livestream. Parents need to be coached live, because the quality has to be good. Then, we can overlay the 23 key points on the small body, mapping simple and complex movements for the specialist.”
At the moment, NeoLifeS works on the direct application of AI on livestream videos in an international consortium. It is therefore possible to act more rapidly, leading to earlier detection of potential anomalies in premature babies.
More about cohorts and biobanks
Currently, there are 175 cohorts and biobanks at the UMCG. These cohorts and biobanks collect data over extended periods, as well as body materials for future medical scientific research. The Cohort and Biobank Coordination Hub (CBCH) unites all these cohorts and biobanks, supports researchers and stimulates new research and cooperations.
Telemedicine Improves Rate of Successful First Visit to NICU Follow-up Clinic

January 2023 Lilly Watson, BA; Christopher W. Woods, MSN, RN, NNP-BC; Anya Cutler, MS, MPH; John DiPalazzo, MPH, MS; Alexa K. Craig, MD, MS, MSc
ABSTRACT
OBJECTIVES:
NICU graduates require ongoing surveillance in follow-up clinics because of the risk of lower cognitive, motor, and academic performance. We hypothesized that multiple programmatic changes, including availability of telemedicine consultation before hospital discharge, would improve NICU follow-up clinic attendance rates.
METHODS:
In this retrospective study, we included infants who survived and were premature (≤29 6/7 weeks/<1500 g) or had brain injury (grade III/IV intraventricular hemorrhage, stroke or seizure, hypoxic ischemic encephalopathy). We compared rates of follow-up for the early cohort (January 2018-June 2019; no telemedicine) with the late cohort (May 2020-May 2021; telemedicine available); and performed a mediation analysis to assess other programmatic changes for the late cohort including improved documentation to parents and primary care provider regarding NICU follow-up.
RESULTS:
The rate of successful 12-month follow-up improved from 26% (early cohort) to 61% (late cohort) (P < .001). After controlling for maternal insurance, the odds of attending a 12-month follow-up visit were 3.7 times higher for infants in the late cohort, for whom telemedicine was available (confidence interval, 1.8-7.9). Approximately 37% of this effect was mediated by including information for NICU follow-up in the discharge documentation for parents (P < .001).
CONCLUSIONS:
Telemedicine consultation before NICU discharge, in addition to improving communication regarding the timing and importance of NICU follow-up, was effective at improving the rate of attendance to NICU follow-up clinics.



As highlighted in the video above, I believe that learning how to hold our ground and maintain a positive perspective when difficult and unexpected situations arise in life may allow us to learn new ways to overcome difficult situations, cope with our emotions, and build our resilience.
Recently, I was met with an unexpected and very challenging situation in my personal life that has required an internal response of focus on building my personal resilience in order to best move forward with the task at hand.
As preemie survivors and global neonatal community members we are innately resilient, learning to overcome the challenges in life we have been dealt. As we know, it isn’t about what happens to us in life, it is about how we respond.
As surfers are pushed to be present in the moment in order to ride the waves they chase, we too learn to surf the waves of life.
What have the challenges in your life taught you to overcome and revealed to you about yourself? How have such experiences helped you develop your character, integrity, and sense of self so that you may rise on the other side as a stronger, more composed, and introspective individual?
Moving into 2023 my hope is that the collective challenges we have experienced as a global community over the past few years and the challenges we face as individuals may compel us to stand grounded and even more composed as we work to pursue excellence in our lives and strive to give the best of ourselves to ourselves, to our family, to our friends, to our mentors, to our communities and to our world.
Wishing you and our global neonatal community fruitful abundance and enhanced resilience for 2023!

I did Paragliding in Ethiopia….**Just Awesome**
Ferils Mad World Apr 5, 2022 #addisababa #ferilsmadworld
Hey, Ferfam I had a wonderful experience doing the paragliding activity organized by #greathikers in Ethiopia. We traveled to Sandafa city which is on the outskirts of #addisababa. It was such a beautiful experience, gliding in the air like a bird, It is a once-in-a-lifetime experience. The activity is done by a professional from Bulgaria, and it’s such a smooth ride. Watch the vlog on #ferilsmadworld and don’t forget to shower your love


