Democratic Republic of the Congo

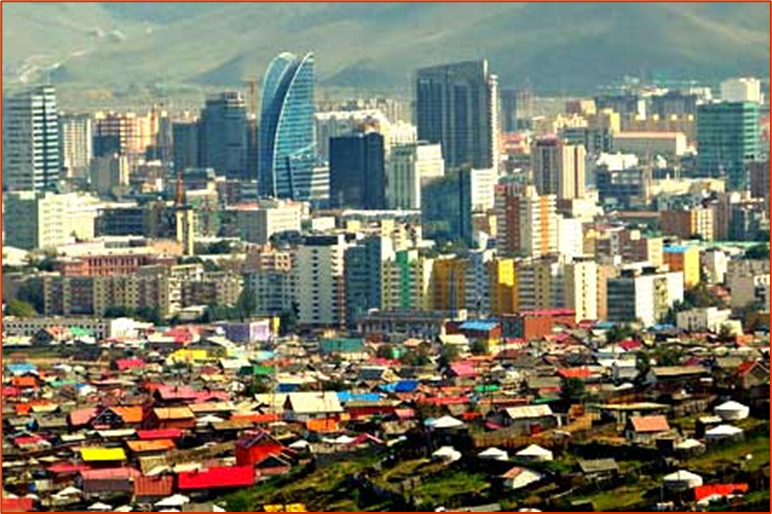
The Democratic Republic of the Congo, also known as Congo-Kinshasa, Congo-Zaire, Congo DR, DR Congo, DRC, or simply either Congo or the Congo, is a country in Central Africa. By land area, the DRC is the second-largest country in Africa and the 11th-largest in the world. With a population of around 105 million, the Democratic Republic of the Congo is the most populous Francophone country in the world. The national capital and largest city is Kinshasa, which is also the economic center. The country is bordered by the Republic of the Congo, Central African Republic, South Sudan, Uganda, Rwanda, Burundi, Tanzania (across Lake Tanganyika), Zambia, Angola, the Cabinda exclave of Angola, and the South Atlantic Ocean.
Health problems have been a long-standing issue limiting development in the Democratic Republic of the Congo (DR Congo). The Human Rights Measurement Initiativefinds that the Democratic Republic of the Congo is fulfilling 73.1% of what it should be fulfilling for the right to health based on its level of income. When looking at the right to health with respect to children, the Democratic Republic of the Congo achieves 96.6% of what is expected based on its current income. In regards to the right to health amongst the adult population, the country achieves 100.0% of what is expected based on the nation’s level of income. The Democratic Republic of the Congo falls into the “very bad” category when evaluating the right to reproductive health because the nation is fulfilling only 22.8% of what the nation is expected to achieve based on the resources (income) it has available.
https://en.wikipedia.org/wiki/Democratic_Republic_of_the_Congo#Further_reading
- GLOBAL PRETERM BIRTH RATES – Democratic Republic of the Congo
- Estimated # of preterm births: 12.4 per 100 live births/Global Average: 10.6
- Source- WHO Preterm Birth Rate (Per 100 Live Births)

COMMUNITY
African region’s first-ever health workforce investment charter launched
06 May 2024
Windhoek – The World Health Organization (WHO) Regional Office for Africa and partner organizations today launched the region’s first-ever health investment charter that aims to align and drive sustainable investment in the health workforce.
With a bold target of halving the African region’s critical 6.1-million health workforce shortage by 2030, the African Health Workforce Investment Charter will mobilize and align domestic and partner funding to strengthen, grow and retain the continent’s health workforce, especially in rural and primary health care settings.
“Any discussion about the delivery of health care services must acknowledge that, for these services to be rendered and rendered effectively, we need feet on the ground,” said Honourable Dr Saara Kuugongelwa-Amadhila, Namibia’s Prime Minister. “For the health professionals to do their work effectively, they must be well resourced and capacitated in the best ways possible.”
In addition to shortages, the African region faces many other health workforce challenges, including, rising unemployment, excessive out-migration and low quality of training. Low health investment and limited prioritization of the health workforce have critically exposed health systems. Investment in health, especially from domestic sources, is still low and inadequate for many countries to meet the universal health coverage and ensure health security.
“The numbers of Africans who have left the continent in search of greener pastures in other parts of the world are staggering. It is a matter that needs to be addressed as a top priority for African governments and indeed all those who wish to see a shift in the historical as well as current trends,” said Honourable Dr Kalumbi Shangula, Minister of Health and Social Services of Namibia.
The charter launched today brought together the health workforce investment efforts of all stakeholders, including national governments, the private health sector, civil society, external financing institutions and development partners in Africa.
“By investing in the health workforce, we not only address the challenges within the sector but also generate dividends in education, employment and gender equality,” said Dr Matshidiso Moeti, WHO Regional Director for Africa. “These investments will contribute to our sustained efforts in attracting more resources and improving the quality of our health workforce.”
Investing in the health workforce will have positive spin-offs in the form of decent jobs, particularly for women and youth who often face barriers to employment. By providing opportunities for education, training and career progression, the Charter will immensely contribute to the economic empowerment of these demographics and fundamentally support inclusive economic growth.
Additionally, health labour force investment also brings multiple returns for health and economies, increasing life expectancy and job creation, while accelerating countries towards the achievement of the Sustainable Development Goals and universal health coverage.
For every US$1 invested in health and sustaining the jobs of health workers, the potential return is as much as US$9. It has also been demonstrated that half of all economic growth globally over the past decade resulted from improvements in health, and that for every added year of life expectancy, the economic growth rate is boosted by 4%.
“Studies show that investments in the health sector yield substantial economic returns, estimating a nine-to-one return on investment. The new narrative that we are promoting is to transform the health sector to move from liability to an asset for the economy of our countries,” said Dr Jean Kaseya, Director-General of the Africa Centre for Disease Control and Prevention.
The Africa Health Workforce Investment Charter was inaugurated in Namibia during the Health Workforce Investment Forum being held from 6 to 8 May 2024. Efforts will continue to be made to engage multisectoral stakeholders and partners on their experiences and achievements, and mobilize commitments, partnerships and investments to deliver on the principles and actions enshrined in the investment charter.

NEW CAMERA IN ST.CHARLES NICU HELPS PREVENT INFANT BLINDNESS
May 05, 2024
St. Charles’ Neonatal Intensive Care Unit has a new tool to help prevent blindness in premature infants, thanks to $85,000 in funding from St. Charles Foundation. The new retinal camera now in use allows caregivers to take high quality images of babies’ eyes, giving ophthalmologists the ability to detect early warning signs and recommend treatment for infants before the disease progresses, possibly leading to blindness.
“We feel very fortunate to have this new tool, and the improved monitoring and quality of care for our patients. It is exciting for St. Charles to have the newest technology and the best equipment to support our community,” said Dr. Patrick Lewallen, NICU medical director. “We are grateful to the Foundation for helping raise the level of care our infants are receiving that is ultimately reducing the risks that premature babies have visual difficulties related to prematurity.”
Infants who are born premature are vulnerable to a number of health concerns – including eye disease and blindness. This is caused by a condition called retinopathy of prematurity. Infants born before 30 weeks’ gestation or weighing less than 3 pounds need to be scheduled for regular eye exams following birth. Until 2024, those exams at the St. Charles NICU were not that dissimilar from a regular eye exam: a pediatric ophthalmologist would shine a light into the eye and provide a written description of what was observed.
But starting this year, caregivers in the NICU are using a state-of-the-art retinal camera to observe and record the condition of the eye, thanks to donors who gave to the St. Charles Foundation’s General Fund. The camera takes highly detailed photos of the retina so they can be closely examined and compared to images over time. Early detection is key for this condition, as it is very treatable.
Pediatric Ophthalmologist Dr. John Davis works at the Oregon Health & Science University Casey Eye Institute’s Bend clinic and visits the NICU at St. Charles at least once a week to evaluate premature babies meeting criteria for this special monitoring. OHSU’s Bend clinic utilizes a similar retinal camera to the one used in the NICU. This allows for easy collaboration between the two organizations to compare images and best support patients as they transition from NICU to an outpatient setting.
When infants are born, blood vessels in their eyes have not fully developed, explained Davis. It takes between 36-40 weeks for infants to completely develop these blood vessels, and in premature infants, sometimes they never fully develop, which can lead to visual impairment and blindness.
Catching it early is critical as there are ways of treating it through the injection of a medication or laser procedure.
“The majority of patients who are screened do not need treatment, but for those that do, this is a critical tool to preserve vision,” said Davis.
The retinal camera is an example of new technology that is funded through St. Charles Foundation to give caregivers access to the best tools possible to treat patients.
“This is an example of how the Foundation can elevate our care for patients from good to excellent,” said Jenny O’Bryan, Executive Director for the Foundation, about why this project was funded. “Our goal is to raise funds that ultimately elevate the care we are able to provide for people in Central Oregon.”
https://www.stcharleshealthcare.org/news/new-camera-st-charles-nicu-helps-prevent-infant-blindness
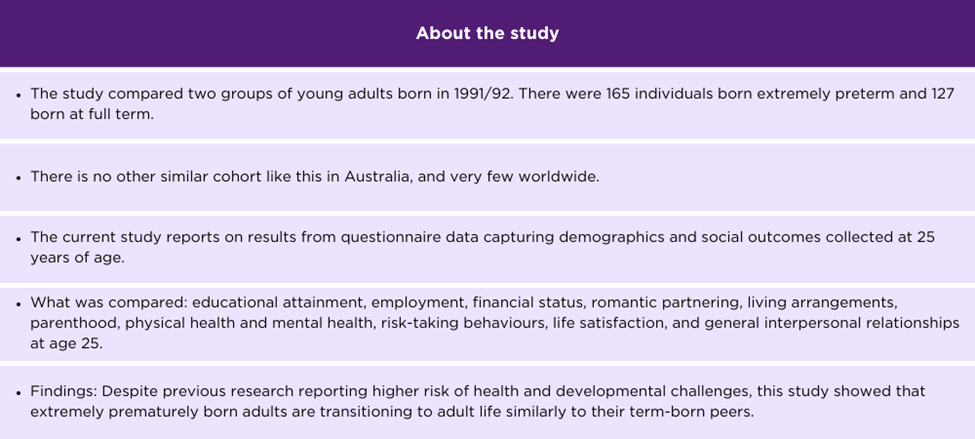
New guidelines to improve the long-term care of preterm babies are expected to result in better health outcomes for babies and parents.
Experts say the strategies will address gaps and minimise growth, health and developmental problems.
Published 26 June 2024 7:32am Presented by Omoh Bello

It has been eight years since Emma Byers had her twins. They were born very preterm which means before 32 weeks gestation. She says the experience came with a lot of postpartum anxieties and pressures.
“It was very sudden, and it was quite a shock. I didn’t see my boys until the following day. When I arrived, I was really overwhelmed by the medical intervention that my boys needed to help them in these very, very early stages of their life. And both of them needed really significant help and intervention with their breathing. That was the main concern for them because they were born so early and spontaneously so there was no ability to get any interventions and steroids to help their lungs. They both had a lot of trouble and had to learn, I suppose, how to breathe”
This is the case for many Australian preterm families with over 3,500 babies born very prematurely in Australia each year.
Approximately 60 per cent experience difficulties and are at higher risk of growth, health, and developmental problems than full-term babies.
Although not all babies will encounter these issues, many parents are concerned about the long-term health outcomes for their children.
A team lead by Murdoch Children’s Research Institute [[MCRI]] has developed the first national guidelines to improve the long-term health outcomes of these infants.
Professor Jeanie Cheong is the Group Leader for the Victorian Infant Brain Studies at the M-C-R-I.
“The purpose of the guidelines is to provide a framework, an evidence based framework, to guide health professionals and also to inform families themselves about what areas of health and development are important. And also at what ages ideally, the children should be seen. And it is very important that you know, any problems with growth or health or development is detected early in childhood. So that resources and interventions can be put in place to help the children improve their outcomes. And optimise you know their potential. “
The National Health and Medical Research Council of Australia has adopted the guidelines – covering children from the moment they leave the hospital until they reach six years of age.
The guidelines will address care gaps by directing every family with a very preterm infant to a coordinated, multidisciplinary team to ensure health risks are detected and treated early.
Sarah Kirby, who had her son Teddy at 26 weeks, says he weighed 719 grams and could almost fit in her hand.
Ms Kirby, whose son is now a healthy 14-month-old, believes the process of having a preterm baby can be overwhelming, and the establishment of national guidelines is a relief.
“It’s a lot, and I’m just so glad that there’s going to be a standard guideline that are going to be in place now so that all the parents after us can just have like, even just walk out of the hospital feeling like they’ve got something to support them. Because you do spend a lot of time in NICU [[Neonatal Intensive Care U nit]]. So to have someone there to say, Okay, this is the check-ups that we’re going to do, when we’re going to be able to find out you know, what’s going on, what’s your baby if there’s anything wrong fairly quickly, because this is standard across the board. You can’t get much further than that can ya? Like I know that it’ll keep getting better but at the moment, to have that is just incredible.”
Ms. Byers says structured support is important also for the mental health of families of very preterm babies.
“Everybody was very well aware that I needed to support as much as the boys did. I felt like the emotional help and support that I got was amazing, but then when I came home, there just sort of seemed to be a disconnect with the mental health services to help me process everything that was going on. I think it would have been great to have been linked in with those prior to the boys being discharged from hospital. But once I did, I really did find that the supports were there. It just took a little bit of a disconnect to get to that.”
Professor Cheong says services vary considerably across Australia.
She says follow-up care needs to be tailored to each child and initiated by each hospital’s Neonatal Intensive Care Unit [[NICU]] team.
Professor Cheong says the guidelines will significantly improve survival rates for babies.
“Children who are born very preterm do have follow up after they leave the hospital intensive care. However, this is not uniform throughout the country. And depending on where you live and the availability of resources, there is a great disparity of follow up. So these guidelines once again provide best practice recommendations. So that health services and families can advocate for the best care possible within the resources that we have.”
The guidelines will be reviewed in five years and updated with any additional evidence-based recommendations.
Professor John Newnham, chair of the Australian Preterm Birth Prevention Alliance says the body is working on safely lowering the rate of early birth across Australia.
“Improving the care for babies born very preterm is very important. But we in Australia now have a program running to prevent preterm birth in the first place and the signs are that it’s being effective.”

Fally Ipupa – Afsana (Clip Officiel)

19,585,780 views Aug 25, 2023
‘Formule 7’, triple album Rumba toujours disponible : https://FallyIpupa.lnk.to/formule7AY


DRC offers free maternity care to cut death rate among mothers and babies
Healthcare workers say clinics are being overwhelmed by women seeking help, amid lack of staff and facilities to back programme

Patrice Citera – Mon 6 Nov 2023
Pregnant women across the Democratic Republic of the Congo are to be offered free healthcare in an effort to cut the country’s high rates of maternal and neonatal deaths.
Women in 13 out of 26 regions in the country will, by the end of the year, be entitled to free services during pregnancy and for one month after childbirth. Babies will receive free healthcare for their first 28 days under the scheme, which the government plans to extend to the rest of DRC – although there is no timetable for that yet.
However, health workers have raised concerns that hospitals and medical centres are ill-equipped to cope with any increased demand on services. Some told the Guardian there were not enough staff, facilities or equipment to successfully introduce the $113m (£93m) programme, which is supported by the World Bank.
The rollout of the programme comes amid nationwide strikes by nurses, midwives, technicians and hospital administrative staff, who are calling for higher pay and better conditions.
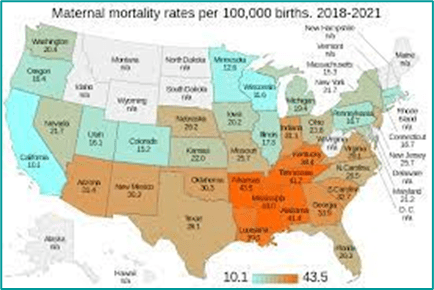
Congo has one of the highest number of maternal and neonatal deaths in the world. Latest figures record the maternal morality ratio at 547 deaths for every 100,000 live births, and its neonatal rate – the number of babies dying before 28 days of life – at 27 per 1,000 live births. The numbers are a long way from UN targets to reduce maternal and neonatal deaths to fewer than 70 deaths per 100,000 and 12 per 1,000, respectively, by 2030.
The minister of public health, Roger Kamba Mulamba, said the programme would free women from a “prison sentence”.
He said: “Mothers today get healthcare without fear when they are pregnant. Babies today do not die because they have no access to antibiotics. Mothers today do not die because they cannot afford to pay for a caesarean delivery.”
General examinations in public health centres can cost about 27,000 Congolese francs (£8), while ultrasounds can cost 60,000 francs. C-sections cost about 524,000 francs. According to the World Bank, more than 60% of Congolese live on less than $2.15 (5,600 francs) a day.
DRC has no universal health coverage, and most people cannot afford what limited care there is. Hospitals are known to detain patients until they have paid medical bills in full. Some new mothers have been forced to stay for weeks in overstretched facilities while relatives search for solutions.
The scheme was initially launched in the capital, Kinshasa, in September, but is now being rolled out to more of the country, including in eastern DRC, which has been blighted by years of conflict. The health ministry said it is spending $42m on the scheme, which is the first part of a $200m programme for prenatal, maternal and neonatal care. It said it was using radio, television to inform women about the free services.
Dr Simplice Kibatatu, from Kinkole general hospital on the outskirts of Kinshasa, said he welcomed the programme, but added that his health centre had been overwhelmed by the number of women seeking care.
“We moved from 30 women to about 65 women delivering each month,” he said. “Pregnant women were arriving at around 10am. Now that it [care] is free, they are turning up early, at around 8am, waiting for a consultation.”
Claudel Diakileke, a technician at the maternity centre in Barumbu, a district of Kinshasa, called the pilot scheme a fiasco. He said there were not enough doctors or trained midwives to meet the demand, and that the government had not provided health centres with more equipment or medicines.
The country has an estimated 9,500 doctors and 73,000 nurses to serve a population of about 95 million. It has one midwife for every 20,000 people.
He added that some women were concerned about the quality of care they would receive. “They say, ‘we always see that anything free is not good’,” he said.
Diakileke criticised the government for not consulting the healthcare workforce or community liaison workers, “who play the role to sensitise the population” before introducing the scheme. Community workers are “the ones who build trust with pregnant women, that tell them if you join the scheme you’ll get good care”.
Nenete Asuka, who owns a restaurant in Kinshasa, said she had yet to benefit from the scheme. She had to pay for a recent ultrasound and examinations at the Barumbu centre. “They said free delivery, but, when I come here I [had to] pay,” said Asuka, who is six months pregnant.
Filo Biancumpa, a dressmaker, who is also six months pregnant, is happy about the scheme, but said: “I never knew the free birth delivery was under way. Whenever I’m coming here [to the health centre], I find they [health workers] are on strike. There is no way to speak to female health workers who counsel pregnant women.”

HEALTHCARE PARTNERS

Breaking the Cycle of Nursing Chaos
The Need to Address the Nursing ShortageBreaking

Bagwell, Gail A. DNP, APRN, CNS, FAAN; Cesario, Sandra K. PhD, RNC-OB, FAAN; Fraser, Debbie MN, NNP, CNeon(C), FCAN; Kenner, Carole PhD, RN, FAAN, FNAP, ANEF, IDFCOINN; Walker, Karen PhD, RGN, RSCN, MACN Advances in Neonatal Care 23(6):p 495-498, December 2023. | DOI: 10.1097/ANC.0000000000001126
Metrics
Across the globe the nursing workforce is in crisis mode leaving nurses and nursing in chaos. Numerous countries are reporting acute shortages of nurses resulting, in part, from dissatisfaction and burnout resulting in high turnover. This is not a local or national problem, it is a global crisis, even more pronounced in low- and middle-income countries, vulnerable settings, and rural and remote locations. Globally, the World Health Organization predicts that there will be a shortfall of 10 million healthcare workers by 2030. In the United States, the Health Resources and Services Administration is projecting a shortage of 78,610 full-time equivalent registered nurses in 2025.
While it is difficult to break down the nursing shortage by specialty areas, reports around the world suggest that neonatal nursing shortages are similar to those in other areas. For example, data from the 2019 National Neonatal Audit Program in the UK found that only 69% of neonatal nursing shifts were staffed at the level recommended by national guidelines and that only 44% of shifts met the requirements for specialist nurse staffing. The accompanying article from the Nursing Times goes on to suggest that the UK is “desperately short of nurses in the right numbers and expertise to meet national guidelines” and that the UK requires at least 605 additional nurses to meet the staffing standards. In Australia, The Sydney Morning Herald in 2022, reported “More staff needed for our smallest, sickest babies on neonatal wards.”
CONTRIBUTING FACTORS
The current nursing shortage is not a new phenomenon, but a constant issue that has ebbed and flowed for decades, affecting the profession of nursing not only in the United States but globally. Nursing shortages are harmful to our profession, as it leads to exhausted nurses providing inadequate patient care, which results in errors and compromises patient safety. Nurses working under these conditions become frustrated when they cannot provide high-quality care. Patients and families suffer. Nurses break the cycle by quitting—not just leaving the current workplace but too often, leaving the profession.
This shortage is different than in the past. It is a global crisis resulting from staffing patterns, lack of ability to influence decision-making, and inequitable pay. These are recurring problems that are worsened by the escalating incidence of both vertical and horizontal violence, which is leading to burnout and the resultant intention of many nurses to leave the profession. A healthcare workforce survey by the Vivian Group found that, in 2021, 40% of survey respondents were considering leaving the profession in the next 5 years. In 2022, that number had increased to 67%.
Hospital systems add to the problem by treating nurses as an expense and not a revenue generator, which was clearly evident during the COVID-19 pandemic. The COVID-19 pandemic exacerbated the situation by reminding nurses that a work–life balance is critical to one’s well-being and that nurses have many options outside traditional nursing. The images of frontline workers during the pandemic drew new students to the profession and at the same time scared others away.
The declining US high school student pool coupled with an aging faculty and decimated college budgets has decreased the capacity of many colleges to enroll enough nursing students to meet the growing nursing workforce needs. In fact, in 2021, the American Association of Colleges of Nursing reported that over 90,000 eligible applicants were turned away from undergraduate and graduate programs because of a shortage of faculty, clinical sites and preceptors, and a lack of funding.
CONSEQUENCES OF THE NURSING SHORTAGE
One of the concerning outcomes of this nursing shortage is the impact on quality care and the increase in error rates. Medication error rates in the United States are reported to occur at rates of 5.5 to 77.9 per 100 medication orders. Over 2 decades ago, in 1999 the Institute of Medicine report “To Err is Human” highlighted that patient safety and quality of care were compromised when health systems failed including staffing inadequacies. Since that time multiple research studies have demonstrated that medical errors increase with staffing shortages.
Similarly, research has demonstrated that staffing ratios also impact other iatrogenic complications including unplanned extubation rates and the rates of nosocomial infection.A study by Tubbs-Cooley and colleagues14 found a significant correlation between nursing workload and missed care in the neonatal intensive care unit. This was also highlighted in a systematic review by Imam et al. Missed care included things such as parent education and supporting parent involvement in the care and oral feeding of their infants, items that may affect parental confidence and nursing satisfaction.
SOLUTIONS
Strategies to address shortages of healthcare workers have varied across the globe. From attempts to increase the number of positions in medical and nursing programs to recruiting workers from other countries or even from one area of a country to another, there are concerns that these strategies will not be effective. Moral and ethical issues arise when countries attempt to address the nursing shortage by enticing nurses from other countries with incentives and relocation packages; this practice is now happening between states or provinces. One state in Australia offered $10,000 relocation funding and another $10,000 after 12 months; hospitals on state borders are suffering as staff leave to work an hour up the road with better pay and conditions. A similar trend is occurring with travel nursing where nurses are resigning from their unit positions to be employed by a travel nursing company at a much higher salary.
THE ROLE OF NURSING ORGANIZATIONS
One of the key factors identified as contributing to nurses’ burnout and intention to leave the profession is unsafe staffing levels.1 The American Nurses Association (ANA) represents the interests of more than 4 million registered nurses. In a June 2023 statement, the ANA addressed governmental agencies and other key stakeholders urging them to implement safe staffing standards that highlight a need for minimum nurse-to-patient ratios. The ANA is urging policymakers, healthcare leaders, and nursing organizations to develop staffing standards to safely meet the unique needs of the patient populations they serve.
The ANA is not only advocating, but seeking solutions, launching the Nurse Staffing Think Tank in 2022 in partnership with other leading organizations, which produced a series of actionable strategies that healthcare organizations could implement within 12 to 18 months. In May 2023, the Nurse Staffing Task Force identified another 65 proposed long-term recommendations designed to spur innovation, policy, and regulatory action, encourage new care models, and effectively support direct care nurses and nurse leaders.
The ANA continues to advocate on behalf of nurses, remain a collaborative partner, and to call on Congress to enact meaningful legislation and policies that improve nurse staffing and their work environments. The ANA provides nurses at all levels key resources to help inform advocacy as well as approaches to address the nurse staffing crisis.
In 2022, the Association of Women’s Health, Obstetric and Neonatal Nurses released a new document titled “Standards for Professional Registered Nurse Staffing for Perinatal Units” based on 3 decades of research. In addition to the rationale for staffing ratios, the standards also stress the importance of nurse well-being, which is critical to patient safety and the financial stability of healthcare organizations. Historically, in the United States, the fetus and newborn have not been a part of the equation in calculating patient acuity levels. However, these vulnerable patients require extensive amounts of nursing care to assure quality and safety. It is essential that the number of bassinets is included in the number of beds reported by hospitals and daily census reports reflect the currently invisible fetus and newborn.
THE ROLE OF NEONATAL NURSES IN REDUCING THE NURSING SHORTAGE
While nurses are quick to blame the administrators for the causes of the nursing shortage, as nurses we also have to take responsibility for the situation ourselves by taking a hard look in the mirror and asking ourselves how our individual actions might contribute to or help alleviate the nursing shortage. How many overtime shifts do you willingly take on for the money or because you do not want to leave your colleagues abandoned even though you are mentally, physically, and emotionally exhausted? Have you been the aggressor, or witnessed or experienced lateral violence? When witnessing or experiencing lateral violence, did you speak up or intervene to stop the situation, or just let it continue? Are you a member of your country’s national nurses association and/or specialty organization? Have you contacted your representatives to your local, state, federal governments to help create legislation to improve nurse–patient ratios? Have you ever discouraged a child, young adult, or adult from pursuing a nursing degree?
As nurses we cannot wait for someone else to fix our problem, we need to start fixing it ourselves. But with it being such a huge problem, it is overwhelming to think that just one person can make a difference. In the United States alone, there are over 4 million nurses and worldwide there are 28 million, which is a lot of voices to help make/demand a change in how we care for patients. Five specialty organizations that focus on neonatal nursing care have come together to raise our collective voices, to advocate for neonates, their families, and our nursing members. We believe that professional organizations must take a stand to speak out against violence in the workplace, bullying, unsafe staffing ratios, and advocate for patient safety and high-quality care. We recognize it is not always safe to speak out in your own organizations, so we encourage you to use your professional organizations to advocate on your behalf. So what are the actions you can take to advocate for yourself and your patients?
- Tell your story—to anyone who will listen, especially those who have the power to make a change. This puts nursing in the forefront and gives a face to the issues. The British Broadcasting Company StoryWorks has a series called “Caring with Courage” and they are recruiting for more stories—consider sharing your story! (https://www.bbc.com/storyworks)
- Develop and practice your elevator speech so that when you have a chance to speak to an administrator, political representatives, or others who can help make a change you are prepared! (https://careerservices.fas.harvard.edu/blog/2022/10/11/how-to-create-an-elevator-pitch-with-examples/)
- Take care of yourself—one cannot have a positive outlook on life and career choices if we do not make ourselves our number 1 priority. Eating healthy, exercising regularly, and getting at least 6-8 hours of sleep/day will go a long way to giving you a better perspective on life.
- Advocate for novel rostering practices; rotating rosters with no flexibility will not entice new nurses into the profession, or keep current staff. The current generation (rightly) want a work–life balance and want to be able to have holidays, attend events when they choose, and have stability in their work–life. Yet, we still have in many places, rostering practices that have been unchanged for 40 years!
- Lobby your politicians in regions with poorer conditions or lack of ratios.
- Belong to your national nursing organization and specialty organizations—together we can do more, but in order to do more we need members to join and participate! Our organizations have realized the power of being a collective group to help create change and while we vie for the same population of nurses, we have decided to come together to work on common issues to improve the life of all neonatal nurses and the patients/families we care for.
CONCLUSION
The chaos that we find our profession in affects each and every one of us, in every country in the world. Never before, have we faced such a crisis, but never before have there been so many of us, collectively, able to address this chaos. We are the largest healthcare profession in the world, and it is time we use our collective voice to demand change and acknowledge that every single one of us has a voice and that voice is important. We all have a role to play to ensure the sustainability of our profession and never ever should we hear when asked what we do “I am just a nurse.” For us, as neonatal nurses, we care for the tiniest, most vulnerable in our society and therefore hold the future of humanity in our hands.

How midwives support women during childbirth | Monash University

Aug 30, 2020
A midwife offers support and care to women during their pregnancy, labour and birth. Join our lecturers Kym and Joy as they go through a simulation of the birthing process, with one of our Bachelor of Nursing and Midwifery students. Our nursing and midwifery labs on campus are set-up to look just like the hospital environment, helping preparing our students before entering the wards.


Excerpts from the National Bereavement Midwives and Neonatal Nurses Forum hosted by Fieldfisher
May 2, 2024
Fieldfisher was delighted to host the 4Louis National Bereavement Midwives and Neonatal Nurses Forum in London. We recognise how invaluable such events are to encourage information sharing, collaboration, experience, providing support and promoting patient safety. The Forum was expertly led by Jane Scott MBE and Alex Mancini. It was a privilege to have been asked to speak at the event alongside other key speakers including Ruth May, Chief Nursing Officer NHS England, Kate Brintworth, Chief Midwifery Officer NHS England and Edile Murdoch, Consultant Neonatologist and Chair of the Maternity and Neonatologist Outcomes Group NHS England.


PREEMIE FAMILY PARTNERS

New animation series to support parents of premature infants
27 February 2024

Professor Caroline Hartley, Principal Investigator, and Dr Marianne van der Vaart Postdoctoral Researcher, in the Paediatric Neuroimaging Group at the Department of Paediatrics, have today launched a series of animations aimed at improving parental understanding of brain development in premature infants, and the effect it has on breathing and apnoeas (the cessation of breathing).

The series, called My Baby’s Brain, has been developed to support parents of premature babies, enabling them to understand why premature babies have apnoeas, the treatment they receive, and the equipment that is used.
My Baby’s Brain is a free, online resource that was created in collaboration with parents of premature babies alongside SSNAP (Supporting sick newborn and their parents), a charity based in the Newborn Care Unit at the John Radcliffe Hospital in Oxford.
Lauren Young, mother to Georgie, (age 7 and born at 40 weeks) and to Rosie (age 3 and born at 24 weeks), and also part of the Family Care Team at SSNAP, was part of the parent group that led to the creation of the series. She had a “traumatic, exhausting and long hospital stay of nearly 6 months” following the birth of her youngest daughter, and proactively wanted to help neonatal research and development.
She said: “In my role with the Family Care Team for SSNAP I see so many parents trying to navigate all the information they receive from the medical teams. I feel strongly that anything helping parents to process the information, feel more comfortable with their surroundings and the care that their child is receiving, can go a really long way to helping them on the journey.”
“These animations will be so helpful to parents and families with premature babies. They will help them to understand the reasons their baby is needing the care they receive and give a very clear picture of equipment used, as well as a soft introduction to language and terminology they may hear along their journey. My Baby’s Brain will help parents feel more in touch with their babies’ care and help them to build confidence in the neonatal setting.”
Professor Hartley said: “In the UK, 1 in 13 babies is born prematurely. Apnoea of prematurity is a common problem in neonatal care, affecting around 50 percent of premature infants. Apnoeas are well-managed by the clinical team but can be worrying for parents. These animations have been put together with parents in mind, to give parents of premature babies a better understanding of how their baby’s brain is developing, how apnoea is linked to the immaturity of a premature infant’s brain, and the techniques researchers use to investigate brain development. Working together so closely with SSNAP and parents on this project has been extremely rewarding and enjoyable and has greatly enriched the animations which we hope will be a valuable resource for parents.”
Martin Realey, Charity Lead for SSNAP, said: “We are delighted to be able to support the creation of My Baby’s Brain which will be an indispensable tool to all parents to premature infants on neonatal units here in the John Radcliffe Hospital, and across the country. They have been made with parents in mind to ensure the information is accessible and easy-to-understand. The videos can be accessed using QR codes making them available on mobile devices, allowing parents to choose a time that best suits them to watch and process the information: This could be cotside with their baby, in the quiet of their home, or even sharing them with other family members. Viewers are also able to choose from bite-sized clips or longer videos which helps manage what can be an exhausting time of processing so much new information.”
My Baby’s Brain was funded by the Wellcome Trust Enriching Engagement programme, an initiative created to support researchers’ public engagement outreach. This series is the public engagement activity of Professor Hartley’s core research project into the relationship between apnoeas and brain development in premature infants.
Professor Hartley is a Sir Henry Dale Fellow at the Department of Paediatrics.
https://www.paediatrics.ox.ac.uk/news/new-animation-series-to-support-parents-of-premature-infants
Breathe, Baby, Breathe!
Neonatal Intensive Care, Prematurity, and Complicated Pregnancies Annie Janvier- Professor of Paediatrics and Clinical Ethics at the University of Montreal, and a Neonatologist, clinical ethicist and researcher at CHU Sainte-Justin. https://doi.org/10.3138/9781487519261
About this book
These interwoven stories and articles provide essential insights into the medical world of premature birth, and into what happens to these babies and their families when things don’t go as planned.
“Annie Janvier has written the best book by far about prematurity for parents and health care providers. As a neonatologist, bioethicist, and mother of an extremely preterm infant, her voice is unique, and we should all listen to her wise and eloquent words. Her intensely honest account of giving birth to Violette at 24 weeks’ gestation and her subsequent experiences as a mother in the NICU is quite remarkable. This amazing book is written from Annie’s heart but also from her brain and her gut.” Nicolas Krawiecki, MD, Professor Emeritus of Pediatrics, Emory University: “Breathe, Baby, Breathe! is a book about resignation, resilience, and transformation.” Lainie Ross, Professor of Clinical Medical Ethics and Pediatrician, University of Chicago: “Breathe, Baby, Breathe! is incredibly honest, and there are times when you are brought to tears. Dr. Janvier not only discusses what it is like to be the mother of a premature baby, but its impact on her own sense of self-worth and the challenges to her family.”
https://www.degruyter.com/document/doi/10.3138/9781487519261/html#overview

A Day in the Life | Maternal Fetal Medicine Specialist Jane Martin, MD

Nov 3, 2022
Jane Martin, MD, shares what a typical day is like for her as a maternal fetal medicine specialist at Ochsner Baptist hospital in New Orleans, where she takes care of moms with medical complications during their pregnancy.


INNOVATIONS

Technology in the NICU

Wednesday, May 22, 2024 FROM THE BLOG
I recently came across an EETimes article by Ray Lumina that describes how electroforming can be used for medical products, especially for those that help save lives in the Neonatal Intensive Care Unit (NICU).
Electroforming is a preferred method for medical technology manufacturing, as it is highly versatile and can adhere to extremely precise specifications, complexity and surface finish. Electroformed optical components are created from plated metal, electro-deposited to provide a precision reproduction of a surface. Every component is an exact replication of the mandrel, making this an economically favorable manufacturing method.
Lumina writes that electroforming is ideal for the production of medical instruments because of its ability to create “high-volume, quality components with extreme accuracy and design complexity.”
An application that he cites is the use of electroforming to create:
…custom reflectors for newborn-baby warming devices. The warmers combine advanced technologies with innovative features to deliver state-of-the-art…The custom electroformed reflector simplified a complex design, ultimately reducing production time and increasing heat output with an improved gold plating that reflects a greater amount of energy.
Electroforming is not exactly a breakthrough technology. It’s been around for nearly two hundred years, and many of the products that use it are decidedly low-tech. Think jewelry.
But the article got me to think about more high-tech instruments and devices that are used in critical, life-saving settings like the NICU.
Children’s Hospital of Orange County had a good list of the “amazing technological advances found in our NICU.” Among the technology that CHOC deploys are a “monitoring system [which] uses near infrared light spectrometry to monitor brain and kidney function.” You’re probably familiar with CPAP machines because there are plenty of TV ads aimed at adults with sleep apnea who need continuous positive airway pressure. Well, there are tiny CPAP machines that work with tiny babies. Another lung-related technology is the high frequency oscillatory ventilator.
Sophisticated telemetry monitors newborns, in real time, for seizure activity, and provides physicians with real-time access to the data on their patients. There’s something wonderful called a “giraffe bed” which is “designed to minimize any unnecessary stimulation to our babies. The beds rotate 360°, can be lowered or elevated as needed, and slide out of the temperature-controlled microenvironment to make it easier to position the baby for all types of procedures without disturbing the infant.” And of paramount importance: the giraffe beds enable parents to touch their little ones.
Like CPAP, most of us have heard of extracorporeal membrane oxygenation (ECMO), given that this technique is used with some frequency to combat COVID. “With ECMO, blood from the baby’s vein is pumped through an artificial lung where oxygen is added and carbon dioxide is removed. The blood is then returned back to the baby.”
The NICU at Children’s of Orange County also uses bar code scanning to make sure that medications, tests, and treatments are for the right patient.
These technologies aren’t unique to CHOC, of course. Other children’s hospitals, and the NICU departments of more general-purpose hospitals, also use these and similar technologies.
Having so many life-saving high-tech devices in the NICU is wonderful. If you’ve had, or know someone who’s had, a preemie or a newborn with challenging health issues, you know how critical this technology can be to give these babies a fighting chance. But the more time these babies spend in the NICU, the more likely they are to come down with a hospital-borne infection. So the goal of the medical community is to reduce NICU admissions and the length of stay (LOS) for the babies who are admitted there. A recent NIH study shows that “equipping care managers with better technological tools can lead to significant improvements in neonatal health outcomes as indicated by a reduction in NICU admissions and NICU LOS.”
And to keep babies out of the NICU, telemedicine and remote monitoring are being increasingly deployed.
Another example of how technology is life-enhancing.
***Critical Link is a privately held US-based company that designs and manufactures embedded systems for electronic applications.
www.criticallink.com/2024/05/technology-in-the-nicu

New tech lets Surrey NICU doctors monitor babies’ ‘most important organ’
By Simon Little & Janet Brown – Global News – Posted March 11, 2024
Staff at Surrey Memorial Hospital in British Columbia are celebrating the arrival of new technology that could help save the lives of some of their tiniest patients.
“The brain is the most important organ but the least monitored organ in the ICU, and this device will provide better brain monitoring,” pediatrician and neonatologist Dr. Samer Yousfi told Global News.
Yousfi was talking about near-infrared spectroscopy (NIRS) monitoring devices, four of which have been installed in the hospital’s neonatal intensive care unit (NICU), which treats premature and vulnerable newborns.
NIRS devices are not new in hospital settings, but technology has only recently advanced enough for them to be used on infant patients.
The machines can monitor how much blood is being used in the brain, or other organs, and now supplement existing equipment that monitors things like breathing, heart rate and other vital signs.
Yousfi said the tool allows doctors and nurses to better tailor their care for vulnerable infants by adding real-time information about what is happening with their brains to the other data they have about a baby’s condition.
“The brain is an important organ because it affects babies’ long-term development outcomes,” Yousfi said.
“If I have a scar in my lung, if I have an injury to my liver if I have an injury to my kidney, most likely I will recover. But if I have an injury to my brain I will have to live with it the rest of my life.”
Yousfi estimated that about one in eight infants in the NICU will need additional monitoring.
https://globalnews.ca/news/10351928/surrey-neonatal-brain-monitoring/

NIRS devices are not new in hospital settings, but technology has only recently advanced enough for them to be used on infant patients.
Staff at Surrey Memorial Hospital in British Columbia are celebrating the arrival of new technology that could help save the lives of some of their tiniest patients.
“The brain is the most important organ but the least monitored organ in the ICU, and this device will provide better brain monitoring,” pediatrician and neonatologist Dr. Samer Yousfi told Global News.
Yousfi was talking about near-infrared spectroscopy (NIRS) monitoring devices, four of which have been installed in the hospital’s neonatal intensive care unit (NICU), which treats premature and vulnerable newborns.
Behind the scenes of caring for B.C.’s youngest patients
NIRS devices are not new in hospital settings, but technology has only recently advanced enough for them to be used on infant patients.
The machines can monitor how much blood is being used in the brain, or other organs, and now supplement existing equipment that monitors things like breathing, heart rate and other vital signs.
The latest health and medical news emailed to you every Sunday.
Yousfi said the tool allows doctors and nurses to better tailor their care for vulnerable infants by adding real-time information about what is happening with their brains to the other data they have about a baby’s condition.
“The brain is an important organ because it affects babies’ long-term development outcomes,” Yousfi said.
“If I have a scar in my lung, if I have an injury to my liver if I have an injury to my kidney, most likely I will recover. But if I have an injury to my brain I will have to live with it the rest of my life.”
Yousfi estimated that about one in eight infants in the NICU will need additional monitoring.
Nurse educator Sonya Bal said an education campaign is now underway among NICU staff, as well as with parents.
“This is something they have not seen before, so we are really working on our parent education, explaining what it is, and they are very excited,” she said.
“(It gives us) a lot of confidence, we can monitor and interpret the data as it is coming hourly and make those informed decisions.”
Surrey Memorial’s NICU is among the first in B.C. to acquire the technology.
The hospital’s four new NIRS devices cost about $15,000 each, with funding through the Surrey Hospitals Foundation.
“We applied it on one of our babies just a few days ago, and after I explained this technology in two or three hours I was just passing by the room and I asked the nurse, ‘How is the brain doing?’” Yousfi said.
“Her answer was, ‘The brain is happy, it is using just the right amount of oxygen, not too much, not too little.’ She made my day. That’s how much the staff are excited.”
https://globalnews.ca/news/10351928/surrey-neonatal-brain-monitoring/

The Journey Toward Establishing Inpatient Care for Small and Sick Newborns in Ethiopia, India, Malawi, and Rwanda
Patricia S. Coffey,Kiersten Israel-Ballard,Laura Meyer,Kimberly Mansen,Nesibu Agonafir,Mitiku Bekere,Queen Dube,Gerard Kaberuka,Jayendra Kasar,Aishwarya Kharade,Sudhir Maknikar,Kelsang Choeki Namgyal,Alinane Linda Nyondo-Mipando,Stephen Rulisa,Bogale Worku,and Cyril Engmann
Documenting the journey to establish inpatient care for small and sick newborns in Ethiopia, India, Malawi, and Rwanda, the authors showcase the remarkable progress and share lessons with stakeholders in other countries who aim to do the same.
Key Findings
- Each country’s unique journey to establish inpatient care and roll out service delivery for small and sick newborns shows the diversity of actions and actors required to scale a new practice across different geographies:
- In Ethiopia, care was implemented in a stepwise expansion from a newborn care corner to community-based newborn care to neonatal intensive care units.
- In India, a model newborn care unit was an exemplar for national scale.
- In Malawi, a hub-and-spoke model used the introduction of continuous positive airway pressure as a grounding point.
- In Rwanda, integrated small and sick newborn care was initiated at the district level in the eastern region of the country, far from the capital city.
Key Implications
- National stakeholders should document country-level strategies and innovation related to the establishment of small and sick newborn care, thereby giving voice to lived country experience.
- Program managers can use the learnings from various countries to establish or strengthen small and sick newborn care service delivery.
ABSTRACT
Background:
Limited information is available about the approaches used and lessons learned from low- and middle-income countries that have implemented inpatient services for small and sick newborns. We developed descriptive case studies to compare the journeys to establish inpatient newborn care across Ethiopia, India, Malawi, and Rwanda.
Methods:
A total of 57 interviews with stakeholders in Ethiopia (n=12), India (n=12), Malawi (n=16), and Rwanda (n=17) informed the case studies. Our heuristic data analysis followed a deductive organizing framework approach. We informed our data analysis via targeted literature searches to uncover details related to key events. We used the NEST360 Theory of Change for facility-based care, which reflects the World Health Organization (WHO) Health Systems Framework as a starting point and added, as necessary, in an edit processing format until data saturation was achieved.
Findings:
Results highlight the strategies and innovation used to establish small and sick newborn care by health system building block and by country. We conducted a gap analysis of implementation of WHO Standards for Improving Facility-Based Care. The journeys to establish inpatient newborn care across the 4 countries are similar in terms of trajectory yet unique in their implementation. Unifying themes include leadership and governance at national level to consolidate and coordinate action to improve newborn quality of care, investment to build staff skills on data collection and use, and institutionalization of regular neonatal data reviews to identify gaps and propose relevant strategies.
Conclusion:
Efforts to establish and scale inpatient care for small and sick newborns in Ethiopia, India, Malawi, and Rwanda over the last decade have led to remarkable success. These country examples can inspire more nascent initiatives that other low- and middle-income countries may undertake. Documentation should give voice to lived country experience, not all of which is fully captured in existing, peer-reviewed published literature.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10461708/


Embracing the Journey: My Experience with Onychomycosis and Finding a Solution
Growing up with onychomycosis on my left foot toes, affectionately dubbed my “goblin foot,” was a challenging journey. Like some preterm infants, though rare, I have battled with onychomycosis since my time in the NICU. From an early age, this condition made me exceptionally self-conscious about my feet. Whether it was walking barefoot on the beach, surfing, or participating in yoga, the thought of exposing my toes was daunting. I avoided these activities free of heavily slathered-on nail polish to keep my condition hidden and always wore grip socks in yoga to feel more secure and less noticeable.
The hesitation to use prescribed medications was another layer of complexity. With a family history of kidney disease and my own health issues during the NICU, my mom and I were concerned about potential side effects on kidney health. We carefully weighed the risks and preferred to avoid traditional prescription treatments, which often led to trying various nail fungus ointments without any real success.
Recently, a friend introduced me to the world of “TikTok Dermatology,” recommending Vicks VapoRub as an alternative treatment. Skeptical but hopeful, I decided to give it a try. To my amazement, after just a couple of months, I noticed a dramatic transformation. My toes were finally looking healthier and were even ready for a normal pedicure process—a milestone I had missed out on as a teen and young woman due to my condition.Sharing this discovery is important to me, especially within the community of fellow preemie warriors who may face similar challenges. If you’re struggling with toenail fungus and traditional treatments haven’t worked for you you, I encourage you to consider this unconventional approach. Sometimes, the most unexpected solutions can bring the most significant changes.

WILL VICK’S VAPORUB KILL TOENAIL FUNGUS!?
Dr. Nick Campitelli
Sep 16, 2021 #toenailfungus #vicksvaporub #nailfungus
Does Vick’s Vaporub cure toenail fungus! Watch this video as Dr. Nick Campitelli answers the questions about Vick’s Vaporub and the treatment of toenail fungus!

What is pediatric onychomycosis?

Pediatric onychomycosis – Children’s Health
Fungal nail infections, or onychomycosis (on·y·cho·my·co·sis), are more common on the toenails than the fingernails.
Onychomycosis tends to run in families because of an inherited tendency, but not everyone is susceptible.
It is rare in children unless one or both parents are infected.
How is pediatric onychomycosis diagnosed?
Pediatric onychomycosis – Children’s HealthA dermatologist may take samples from the nail in order to properly identify and treat the problem.
A scraping of the nail is treated with a chemical called KOH which allows it to be examined under a microscope. Sometimes, the scrapings from under the nail can be used to culture the material to see what grows and identify it.
Other conditions such as nail psoriasis or allergic reactions to nail polish, hardeners, or acrylic nails may look like fungal infections, but they are not. These tests help make the proper diagnosis.
Fungal infection of the nails is also important in people who have other diseases such as diabetes, and those who have had their immune system suppressed. Patients who are HIV, have AIDS, cancer patients, particularly those taking anti-cancer medications, and transplant patients who are also taking drugs which suppress the immune system, should be treated to prevent future health problems.
How is pediatric onychomycosis treated?
Topical antifungal creams, lotions, gels, and lacquers may be used, however, it is difficult for them to penetrate the nail.
Oral medicines like itraconazole, terbinafine, and fluconazole are used, and may require monitoring with blood tests. These are usually avoided in patients with a history of liver problems such as hepatitis and are not given to pregnant or nursing women. These new internal treatments are very safe when monitored by the dermatologist. In general, toe and fingernail fungus usually requires pills except in very mild cases.
Debridement or removing the infected part of the nail may enhance the effectiveness of the treatment. Dissolving or surgically removing the nail if the nail is thick and deformed may be helpful in a few situations, and used only if the infection is very severe.
- Recurrence and prevention
- Keep toenails cut short so as to minimize trauma or injury.
- Wear shoes that fit properly and alternate shoes.
- Use an antifungal cream on the feet to prevent fungal infection of the foot (athlete’s foot).
- Use antifungal powder to control perspiration which may promote fungal infections of the feet.
- Treat nail fungus to avoid complications especially in diabetics and immunosuppressed people.
- Be certain of the correct diagnosis by seeing a dermatologist.
- Wash and dry the feet properly.
- Do not share clippers and files.
- Cleanse all foot instruments with alcohol.
- Avoid being barefoot in public facilities like locker rooms and pools.
- Never wear someone else’s shoes.
- Avoid wearing tennis shoes as regular shoes.
- Wear outside shoes for outside work.
- Use antifungal sprays and powders in the shoes weekly.
https://www.childrens.com/specialties-services/conditions/onychomycosis


SAMMIE THE SALMON
Kids underwater story / preemie baby story

Dec 15, 2020 #preemies #storytime
Sammie the Salmon by Debra Kline tells of Sammie a baby fish who was born to soon. He is very very small and his Mummy and Daddy worry. This amazing kids underwater story is a tale of love and letting your fears about your little ones go. Sammie goes from strength to strength and grows so big he becomes ” The biggest salmon the world has ever seen” This beautifully illustrated preemie baby story by Lynda Farrington Wilson hopes to inspire other families with their miracle babies.