El Salvador, officially the Republic of El Salvador, is a country in Central America. It is bordered on the northeast by Honduras, on the northwest by Guatemala, and on the south by the Pacific Ocean. El Salvador’s capital and largest city is San Salvador. El Salvador’s population in 2024 was estimated to be 6 million.
The economy of El Salvador has historically been dominated by agriculture, beginning with the Spanish taking control of the indigenous cacao crop in the 16th century, with production centred in Izalco, along with balsam from the ranges of La Libertad and Ahuachapán. This was followed by a boom in use of the indigo plant in the 19th century, mainly for its use as a dye. Thereafter the focus shifted to coffee, which by the early 20th century accounted for 90% of export earnings. El Salvador has since reduced its dependence on coffee and embarked on diversifying its economy by opening up trade and financial links and expanding the manufacturing sector. The colón, the currency of El Salvador since 1892, was replaced by the United States dollar in 2001. As of 2019, Salvadoran economics gifted them the lowest level of income inequality out of nearby countries. Among 77 countries included in a 2021 study, El Salvador had one of the least complex economies for doing business.
The Human Rights Measurement Initiativefinds that El Salvador is fulfilling 89.6% of what it should be fulfilling for the right to health based on its level of income. When looking at the right to health with respect to children, El Salvador achieves 98.3% of what is expected based on its current income. In regards to the right to health amongst the adult population, the country achieves only 82.9% of what is expected based on the nation’s level of income. El Salvador falls into the “fair” category when evaluating the right to reproductive health because the nation is fulfilling 87.6% of what the nation is expected to achieve based on the resources (income) it has available.
There are now 30 public hospitals in El Salvador, plus various primary care facilities and 27 basic health care systems. Before 2009 a “voluntary” donation was demanded to access a public hospital or clinic. Clinics staffed by Community Health Teams have been established in the rural areas. Although services are supposed to be a free, a shortage of funds means that people may have to pay for supplies Emergency services are very basic. The private health sector offers care in medical facilities concentrated in urban areas.
Source: https://en.wikipedia.org/wiki/El_Salvador
- GLOBAL PRETERM BIRTH RATES – El Salvador
- Estimated # of preterm births: 7.78 per 100 live births
- (Global Average: 10.6)
- Source- https://worldpopulationreview.com/country-rankings/preterm-birth-rates-by-country

COMMUNITY

Source:https://doi.org/10.63682/jns.v14i31S.8739



HEALTHCARE PARTNERS
Overview
Leadership by the head nurse/unit manager in facilitating the implementation of Infant and Family Centered Care (IFCDC) is often unrecognized. The key role of the head nurse/unit manager in promoting IFCDC and creating a NIDCAP Training Center within the neonatal intensive care unit at the University Hospital of Ghent, Belgium, serves as an example of significant practice change. Instead of taking a theoretical model of change as a starting point, concrete personal experiences and roles that are incorporated into daily practice are described. The aim is to provide insight into how leadership, entrepreneurship, and connection significantly contribute to successful implementation, and to inspire managers facing similar processes.
A description of the evolution of the role of the head nurse from clinical expert to an inspiring, facilitating, and strategic manager includes grounding in clinical skills that lead to an understanding of the necessity of implementing IFCDC. Expansion of the leadership role includes believing in one’s own team, actively giving employees opportunities to build and share expertise, and developing a culture of shared leadership and evidence-based working. The use of care consultants, working groups, and internal study days strengthened both expertise and team solidarity.
A focus on the importance of the head nurse’s entrepreneurial leadership complements clinical expertise and team leadership. Despite budgetary pressure, gaining insight into financial flows, using workload measurement tools, and developing an appropriate financing model enabled continued investment in training and innovation. Strategic alignment with the hospital’s mission, vision, and quality models increased support among senior management.
The head nurse’s role in connecting and communicating is highlighted as crucial for sustainable change management. Transparent communication, multidisciplinary involvement, and attention to pitfalls and concerns proved essential to embed IFCDC and NIDCAP principles into daily healthcare practice and create a shared sense of ownership and pride.
Background When preparing and developing a large project, such as a startup, any practice change involving developmentally supportive, family-centered care can be framed with objectives, project plans drawn, and theoretical frameworks developed from the literature. However, the role of the head nurse/unit manager does not include managing theoretical change processes; rather, it involves using concrete examples to demonstrate how implementation can work in a particular NICU. The theory can be used, often post hoc, to get insight into why a project is or is not implemented in practice.
The intent of the description of the head nurse’s/unit manager’s development and resulting role is to provide a narrative of what worked. The descriptions and strategies included are intended as inspiration for those facing similar implementation projects.
Knowledge background of the nurse manager
In the past, the ‘better nurses’ often rose to managerial positions. The person who was the most handy and who had the most clinical knowledge was often appointed as head nurse. However, it has become increasingly clear that the role has expanded to include many other competencies.
Inspirational role of a nurse manager
As a head nurse, it is first and foremost important to believe in the strength of your own team. Your own employees should be given maximum opportunities to develop their expertise, and in turn, they should share it within the team. A manager primarily facilitates nurses’ growth, embraces the knowledge they develop, and ensures it is shared with colleagues.
In the Ghent NICU, work is conducted across many domains (ventilation, breastfeeding, pain, transport, skin and wound care, resuscitation, developmental care, vascular topics, etc.). The head nurse/unit manager, recognizing the importance of work groups that address clinical care, grants a part-time exemption for a nursing consultant in each care domain. Their role is to follow and document the work group processes and provide training to colleagues, intra- and extramural. The resulting work on the specific care domains is supported not only by the nursing consultant but also by several team ambassadors. In this way, multiple contact persons for various topics are created, and opportunities are offered to different team members. Recognition of evidence-based, high-performance care then spreads within the broader organization.
Every two years, a symposium for nurses and midwives is developed and offered with significant support from the head nurse/unit manager. These educational programs provide a connection and collaboration towards a common goal within the various care domains of neonatal care. It is a moment to ‘shine’ as a team and to share the evidence we have acquired with others. This ‘study day’ can be seen as an example of the department’s dynamic culture, which pursues clinical excellence.
As a unit manager, inspiring is essential to education. For example, looking for relevant topics together and cross-pollinating ideas with each work group is an example of how to provide inspiration. Additionally, providing inspiration is essential for stimulating employee growth on your team. It is an opportunity both to optimize care quality and for nurses individually to grow and rise above themselves. If a manager is not afraid to step outside of their comfort zone, it can lower the threshold for employees to do the same.
Entrepreneurial and innovative role of the nurse manager
Inspiring and facilitating staff are important, but achieving financial freedom and earning the trust of senior management are necessary. In a context where resources are increasingly scarce and priorities are increasingly focused on direct business results, the role of a head nurse/unit manager as an entrepreneur and innovator is not an obvious choice. However, it is essential to the success of any initiative.
Financing as an entrepreneurial skill.
Financial autonomy to generate and control income is a key component of the entrepreneurial role of the head nurse/unit manager. To realize this new cultural shift in how a head nurse/unit manager’s role is perceived, an individualized, well-thought-out financial plan that generates income (e.g., by organizing symposia and offering training to external partners) is essential. In turn, generating income makes it possible, for example, to send colleagues to international conferences and training courses. It is therefore also the task of a head nurse, as the department’s budget holder, to identify, see, and take advantage of financial opportunities.
It is important to have insight into the NICU’s financial flows relative to the entire organization. Very often, people complain about deficiencies, which is nothing new and is probably a sore point in every organization. A head nurse/unit manager should try to get a handle on the income and expenses of their department. Demonstrating financial control often ensures that senior management has the confidence to start working with the NICU entrepreneurially. For example, the Ghent NICU, together with the other Flemish NICUs, successfully validated a neonatal measurement instrument and used it to document nurses’ workload on a daily basis (WANNNT). The outcome data, along with income from fees and historical hospitalization data for our service, enabled us to predict our unit’s budget. Working solely with post-factum data means the head nurse/unit manager is less able to respond quickly to a rapidly evolving context.
Innovation as an entrepreneurial skill.
An important aspect of the entrepreneurial role is innovation. Head nurses are expected to actively explore innovative solutions and consider opportunities to optimize patient care. Undoubtedly, these opportunities present themselves in every organization.
Neonatal care has undergone many developments in recent decades. NIDCAP and IFCDC are receiving increasing attention. It leads, among other things, to better neonatal outcomes, shorter length of stay, fewer complications, and less stress for parents. Sharing the most recent literature on this subject with the hospital’s management and higher management while also emphasizing the financial benefits to the hospital can help free up budgets more easily.
Implementing NIDCAP and IFCDC comes with a significant price tag. When hospitals are under financial pressure, they often quickly reduce non-primary assignments, including training. It is important to demonstrate that the investment in developmental care is profitable in the long term, not only through patient and family outcomes but also by showing the sustainability of quality of care and staff retention. In addition to having self-acquired resources to continue investing in your team’s education and training, it ensures a successful start to greater innovation in implementing NIDCAP training and IFCDC standards of care.
Policy implementation role of the nurse manager
Within the hospital, the mission and vision are periodically adjusted. The individual units and services are asked to align their departmental objectives with the hospital’s policy. Keywords of the Ghent University Hospital policy are excellent—daring, people oriented, and efficient. It does not take much imagination to see that the core IFCDC and NIDCAP values are reflected in these key words in hospital policies. The head nurse/unit manager of the NICU must translate the link between the hospital and the developmental care values using concrete examples from clinical practice and present it to the hospital’s higher management.
Each hospital also works around and with an international quality model. The NICU at University Hospital Ghent also strives to meet, as far as possible, the highest standards set by the European Standards of Neonatal Care. Working with 2 different models is not always efficient. As a service, embedding the Neonatal Standards of Care is done as much as possible within the various care domains with the hospital’s quality model as the goal. On the one hand, this ensures working on quality in a broad sense, as expected by the hospital, and avoiding ‘quality fatigue’ by working with parallel models. It is also an opportunity to demonstrate in practice how to translate the hospital’s keywords and the organization’s central vision into our daily policies.
Connecting the role of the nurse manager
The head nurse serves as a connector within change management, linking vision and practice. In a care context that is constantly evolving, the head nurse helps translate changes into reality for the nursing team. This translation is best made in collaboration with stakeholders from the developmental care team, in concrete terms. The multidisciplinary working group on development-oriented care includes NIDCAP professionals who serve as guides. In this way, a bottom-up culture of co-ownership for important projects is cultivated.
Clear and empathetic communication is essential here. A space for dialogue is created; active listening to questions and concerns is employed; and assurance is provided that employees feel heard and involved.
In this way, a team-oriented culture, in which cooperation and interprofessional respect are central, is promoted. In the past, NIDCAP and a developmental care emphasis were often seen as the work of a small number of passionate nurses. A multidisciplinary approach, in which doctors, psychologists and, for example, care consultants are closely involved, provides much more support for this process and increases the likelihood of success.
Finally, the head nurse/unit manager acts as a role model in the change process. By showing a willingness to change, flexibility, and a constructive attitude, you give the team direction and trust. In this way, the head nurse not only becomes an initiator of change but also a catalyst that connects and strengthens people to achieve these sustainable improvements together.
Communicative role of the nurse manager
The head nurse also plays a central role in communicating key changes. This role goes beyond merely passing on information; it includes actively connecting people, their expectations, and their goals. A head nurse is at the crossroads between the nursing team, the medical staff, and senior management, ensuring that those three worlds are anchored together.
Within the team, creating clarity and trust is a priority, and open communication is crucial. In addition, a culture of dialogue is emphasized in which team members, together, are encouraged to help shape the policy on developmental care. Congruence in thinking and acting is essential here. The manager must ensure that the team’s vision translates into daily operations in direct patient care: in other words, “make sure that you DO what you SAY”.
At the same time, the head nurse is an important communication partner with senior management. Frequent, open, and honest feedback to management about the current state of the change process creates a long-term atmosphere of trust between management and the team. In doing so, the possibility of identifying any additional needs (e.g., additional staff needs) is embedded. SAYING what you DO is therefore not an empty illusion here.
To achieve this, it is also an undeniable asset if senior management wants to delve into the content of the developmental and family centered care project to a certain extent. The presence of a board member during a feedback session with the Ghent NICU staff made it easier to continue the discussion. In this way, co-ownership of the change project is supported at the higher management level.
As in any organization, organizational change sometimes occurs at the senior management level. Every change and new situation should be proactively used to invite new board members to share the unit’s vision and to explain projects within the long-term vision of both the organization and the unit. This approach can ensure that a lot of additional context information is less necessary for specific and/or new questions related to the project.
Pitfalls
Does everything always go perfectly? Not at all. Not everyone is immediately open to change: why would anyone suddenly change something that they have been doing in a certain way for 20 years? Familiar questions are • “Is there sufficient evidence for changes to this protocol?” • “Do all those adjustments cost too much money?” • “Is that profitable?” communication is crucial. In addition, a culture of dialogue is emphasized in which team members, together, are encouraged to help shape the policy on developmental care. Congruence in thinking and acting is essential here. The manager must ensure that the team’s vision translates into daily operations in direct patient care: in other words, “make sure that you DO what you SAY”. At the same time, the head nurse is an important communication partner with senior management. Frequent, open, and honest feedback to management about the current state of the change process creates a long-term atmosphere of trust between management and the team. In doing so, the possibility of identifying any additional needs (e.g., additional staff needs) is embedded. SAYING what you DO is therefore not an empty illusion here. To achieve this, it is also an undeniable asset if senior management wants to delve into the content of the developmental and family centered care project to a certain extent. The presence of a board member during a feedback session with the Ghent NICU staff made it easier to continue the discussion. In this way, co-ownership of the change project is supported at the higher management level. As in any organization, organizational change sometimes occurs at the senior management level. Every change and new situation should be proactively used to invite new board members to share the unit’s vision and to explain projects within the long-term vision of both the organization and the unit. This approach can ensure that a lot of additional context information is less necessary for specific and/or new questions related to the project. Pitfalls Does everything always go perfectly? Not at all. Not everyone is immediately open to change: why would anyone suddenly change something that they have been doing in a certain way for 20 years? Familiar questions are • “Is there sufficient evidence for changes to this protocol?” • “Do all those adjustments cost too much money?” • “Is that profitable?” • “Is that really a priority now?” • “Are we not shifting the focus too much to education and training, to project work, which jeopardizes our clinical work in direct patient care?” • “As a care provider, will I still be able to take my holidays with all those different assignments?”
Thus, we can continue with similar questions for a while.
These are all recognizable concerns in departmental change processes—concerns that can and will come from both the team and senior management and concerns to which head nurses cannot always give an immediate, satisfactory answer. Nevertheless, it is important to stick to basic ideas and evidence, asking the question: “Why and for whom are we doing all this?” which will often help with forward movement. It will be important to stay transparent with the team—even during personal uncertainties— show vulnerability, and, above all, continue to ensure a safe climate in which employees can share their concerns. Working step by step so that the effort remains manageable for everyone and not forgetting to celebrate the team’s successes when reaching milestones are essential to avoiding missteps. In this way, it creates a joint sense of pride with the developmental and family-centered care implementation story, in which even the care for each other as care providers within the team must continue to receive necessary attention.
Summary
Successful implementation of a complex and intensive change process, such as the start-up of a NICU-wide infant- and family centered developmental care program and a NIDCAP Training Center, is not merely the result of a theoretically based project plan but above all of thoughtful and committed leadership in practice. The role of a head nurse/unit manager in this effort is multifaceted: entrepreneurial, innovative, inspiring, facilitating, strategic, connecting, and communicative.
By starting with trust in the team’s expertise and growth opportunities, a culture is created that centralizes shared leadership, multidisciplinary collaboration, and evidence-based care. Consciously investing in training, stimulating internal nursing consultancy, and making expertise visible within and outside the department not only strengthens the quality of care but also increases employee involvement and pride. Entrepreneurial leadership within a healthcare context that is increasingly under financial pressure appears to work. Insight into budgets, the use of financial opportunities, and the substantiation of investments with both clinical and economic arguments have proven necessary to make such a change process possible.
Sustainable change can only succeed if it is strategically embedded in the broader mission, vision, and quality structures of the organization. Alignment with hospital-wide policy objectives increased support and prevented fragmentation or ‘quality fatigue.’ Crucial here is the head nurse’s role as a link between the unit and the hospital’s management, where transparent communication strengthens trust on both sides.
Finally, the change process is inevitably accompanied by uncertainties, resistance, and pitfalls. By leaving room for concerns, working step by step, and celebrating successes, a safe learning climate can be created in which change is not experienced as a threat but, hopefully, as joint growth. In this way, the head nurse not only becomes a manager of change but also a driving force behind sustainable, people-oriented care.
Source:https://neonatologytoday.net/newsletters/nt-feb26.pdf


PREEMIE FAMILY PARTNERS


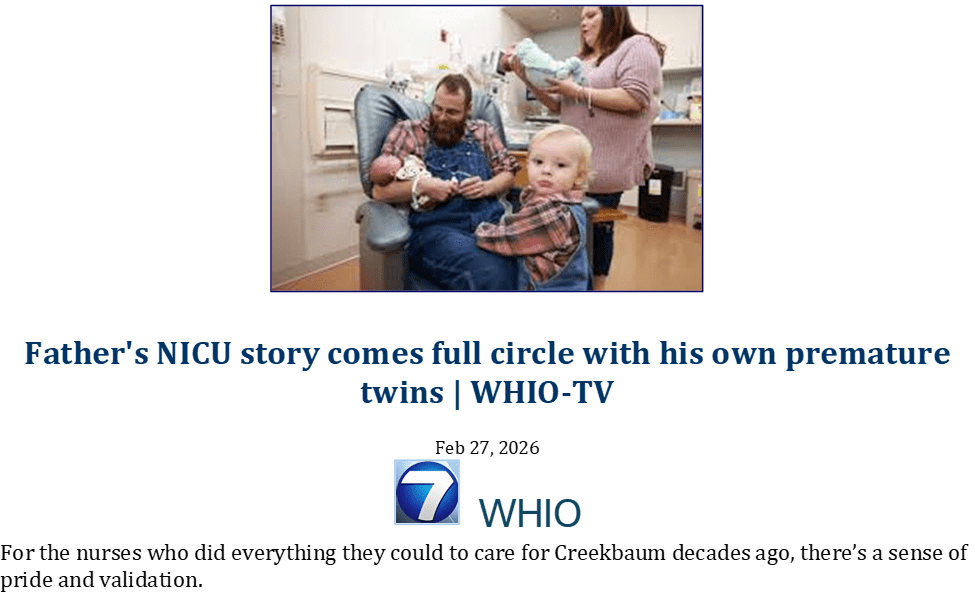
New parents Nicole and Joe welcomed identical twins Ava and Amelie, who were born premature at just 26 weeks at Birmingham Women’s Hospital, and were cared for on the Neonatal Intensive Care Unit (NICU) for over 11 weeks before they were well enough to go home.
Nicole, who lived in Lichfield at the time, was seen at the hospital’s Fetal Medicine Department when they noticed at her 16-week scan one of the twins was growing significantly smaller than the other.
She recalled: “It was my first pregnancy, and we found out we were having twins at six weeks and the pregnancy was going smoothly.
“They noticed at a scan one of the twins was growing significantly smaller, so we were referred to the Fetal Medicine team.”
The Fetal Medicine department discovered the twins had Selective Intrauterine Growth Restriction ( sIUGR ), a condition that can occur in identical twin pregnancies where one twin is growth restricted due to an absent or reversed flow from the umbilical cord.
Nicole added: “We’d never heard of the condition before, and it was really scary knowing something was potentially wrong.
“It was all due to where they’d ended up connecting to the placenta. The bigger twin was plugged in at a larger part so was getting plenty of nutrition, but the smaller twin was plugged into the tail end of the placenta, meaning she wasn’t getting enough nutrition and was so much smaller.
“We didn’t know what this would mean for them, but everyone was so kind and reassuring and explained things in a way we could understand.”
Nicole was scanned twice a week to closely monitor the smaller twin’s growth, until Nicole was 26 weeks pregnant and was admitted overnight for daily monitoring.
She said: “Her heart rate kept dropping low on the monitor, and we were starting to get concerned and thinking about having to deliver them early.
“It kept dropping and taking longer to come back up, and one of the consultants who looked after us said that it was time for them to come out now.
Ava and Amelie arrived prematurely at 26 weeks and 4 days, weighing just 2.2 and 1.9 pounds.
Nicole said: “I was able to see both girls after they were born before they went straight down to the NICU, where they were both intubated for 24 hours before progressing onto oxygen.
“Joe went down with them, and once I’d recovered, they took me to see them, and they looked so tiny and fragile.
“Amelie, the smaller twin, kept getting blood in her feeding tube, so had to be nil by mouth due to the risk of infection. She had a much harder ride to start with, but she kept fighting.”
Both twins started to get stronger with the help of oxygen and feeding tubes, however, when Ava was six weeks old, she developed Necrotising Enterocolitis (NEC) which, an infection which can affect premature babies and is a condition where the bowel becomes inflamed and damaged.
Nicole recalled: “Something hadn’t been quite right with her tummy the day before, but then we got a phone call at home to say she’d taken a turn for the worse.
“It was horrible hearing the phone ring in the middle of the night knowing it was probably about the girls, but knowing we weren’t with them.
“They were both so strong and were real fighters all the way throughout.”
During their stay at the NICU, Nicole and Joe visited every day, arriving first thing in the morning and staying until last thing at night. They also received counselling on the unit and were part of the family group that had been set up for parents to share their journey.
Nicole commented: “Nothing can prepare you for a stay on the NICU.
“While we were there, we lived in our own little bubble and we didn’t talk to family or friends much because it was hard to explain how it feels, and you don’t know what’s going to happen next.
“The team were really supportive, and they helped us be as hands-on as possible with their care, and the family group was really helpful too. It was nice to be able to talk to other parents who knew how it felt and were going through the exact same thing too.
“Walking away from your babies every night was just horrible, so to finally leave with them was a huge relief.
“When we went home, they both still had a feeding tube, but the team were brilliant in giving us training so we could do it ourselves at home. Both tubes ended up being removed the next day as they were doing so well breastfeeding.”
The twins are now over two years old and are thriving at home after their difficult start to life.
Nicole added: “They’ve got such different personalities now, but they’re both very cheeky little girls.
“Ava especially loves animals and trips to the farm, and they both love singing and dancing around the house.
“They both absolutely adore their younger sister and they’re so gentle and kind with her.
“We’re so thankful for everyone at the Women’s Hospital for looking after our girls, they’re both so strong and such fighters and we couldn’t be prouder of how far they’ve come already.
“Shireen Meher looked after us from our time in fetal medicine all the way to the delivery, and she was had such a positive impact on our journey.”
Source:https://bwc.nhs.uk/news/identical-twins-now-thriving-after-being-born-premature-at-26-weeks-14305/


INNOVATIONS
Background:
The neonatal intensive care unit (NICU) relies on a multidisciplinary team of advanced practice providers (APPs), including neonatal nurse practitioners (NNPs) and physician assistants. With the Accreditation Council for Graduate Medical Education residency rotation reductions taking effect in July 2025, the demand for NNPs to fill clinical coverage gaps will increase. Anticipated changes in federal reimbursement and Medicaid services and National Institutes of Health pose financial challenges for Children’s Hospitals.
Evidence Acquisition:
This review examines the current state of the NICU APP workforce with special emphasis on NNPs, including historical trends, educational requirements, and the impact of regulatory changes. Data were gathered from surveys completed by national professional organizations, published literature in PubMed, and expert communication.
Results:
Despite their critical role and increased demand, APPs including NNPs face challenges, such as burnout, staffing deficits, reimbursement, and a decline in the number of NNP graduates by 20% since 2022. Neonatal nurse practitioner recruitment is hindered by the lengthy onboarding process and high costs. The integration of physician assistants, hospitalists, and non-NNPs as possible solutions to fill the NNP shortage gap presents challenges, such as lack of training opportunities and managing patients outside their scope of practice.
Implications for Practice and Research:
Addressing workforce shortage requires strategies, including tuition-supported programs, recruiting registered nurses to become NNPs, developing mentorship programs, and increasing NNP preceptors. Further research is needed to evaluate the effectiveness of these strategies and to explore additional solutions for sustaining the NNP workforce.




Introducing Preemies Hub: A New Global Resource for Preemie Families, Built with You in Mind
For every preemie warrior and every parent who has stood beside an incubator, the journey into the NICU often begins without warning. It can feel overwhelming—filled with medical language, uncertainty, and the urgent need to make sense of what is happening to your baby. In those moments, access to clear, trustworthy, and relatable information is not just helpful—it is essential. That is why we are so excited to introduce Preemies Hub, an innovative new platform developed in partnership with Our Kids Health, designed to support families navigating the realities of premature birth.
Preemies Hub was created with a deep understanding that not all families experience the NICU in the same way. For many, challenges are compounded by language barriers, cultural differences, and limited access to reliable, evidence-based information. This platform addresses those gaps by providing translated, adapted, and culturally responsive health information specifically designed for parents across equity-deserving communities. Every piece of content has been developed with respect for different values, beliefs, and ways of communicating—ensuring that families can not only access information, but truly connect with it.
So why does this matter? Because caring for a premature baby is already one of the most emotionally and physically demanding experiences a family can face. Misconceptions about prematurity, lack of preparation for an unexpected early delivery, and difficulty navigating medical information can make that journey even harder. Preemies Hub helps change that. It empowers parents with knowledge they can trust, presented in a way that is clear, compassionate, and accessible—so families can feel more confident, informed, and supported in advocating for their child.
The platform offers a wide range of topics relevant to the NICU journey and beyond, along with resources available in multiple languages including Punjabi, Ukrainian, Tamil, Spanish, Mandarin, Inuktitut, Cantonese, Filipino, Arabic, and more. It also intentionally centers diverse communities, including Black families, ensuring that representation and inclusivity are not afterthoughts—but foundational to the resource itself. For providers, this means having a trusted tool to share with families. For parents, it means finally seeing information that reflects your language, your culture, and your experience.
At Neonatal Womb Warriors, we believe that every family deserves access to information that meets them where they are. Preemies Hub is more than just a resource—it is a step toward equity in neonatal care, a bridge between knowledge and community, and a reminder that no preemie journey should be navigated alone. 💙
Preemies Hub: https://www.cpbf-fbpc.org/preemie-hub




Read Aloud: Ways to Make Friends by Jairo Buitrago | Stories with Star
Do you have any ideas for ways to make friends? Read along with Star as we learn some new and interesting ways to connect with others and yourself!