El Salvador, officially the Republic of El Salvador, is a country in Central America. It is bordered on the northeast by Honduras, on the northwest by Guatemala, and on the south by the Pacific Ocean. El Salvador’s capital and largest city is San Salvador. El Salvador’s population in 2024 was estimated to be 6 million.
The economy of El Salvador has historically been dominated by agriculture, beginning with the Spanish taking control of the indigenous cacao crop in the 16th century, with production centred in Izalco, along with balsam from the ranges of La Libertad and Ahuachapán. This was followed by a boom in use of the indigo plant in the 19th century, mainly for its use as a dye. Thereafter the focus shifted to coffee, which by the early 20th century accounted for 90% of export earnings. El Salvador has since reduced its dependence on coffee and embarked on diversifying its economy by opening up trade and financial links and expanding the manufacturing sector. The colón, the currency of El Salvador since 1892, was replaced by the United States dollar in 2001. As of 2019, Salvadoran economics gifted them the lowest level of income inequality out of nearby countries. Among 77 countries included in a 2021 study, El Salvador had one of the least complex economies for doing business.
The Human Rights Measurement Initiativefinds that El Salvador is fulfilling 89.6% of what it should be fulfilling for the right to health based on its level of income. When looking at the right to health with respect to children, El Salvador achieves 98.3% of what is expected based on its current income. In regards to the right to health amongst the adult population, the country achieves only 82.9% of what is expected based on the nation’s level of income. El Salvador falls into the “fair” category when evaluating the right to reproductive health because the nation is fulfilling 87.6% of what the nation is expected to achieve based on the resources (income) it has available.
There are now 30 public hospitals in El Salvador, plus various primary care facilities and 27 basic health care systems. Before 2009 a “voluntary” donation was demanded to access a public hospital or clinic. Clinics staffed by Community Health Teams have been established in the rural areas. Although services are supposed to be a free, a shortage of funds means that people may have to pay for supplies Emergency services are very basic. The private health sector offers care in medical facilities concentrated in urban areas.
Leadership by the head nurse/unit manager in facilitating the implementation of Infant and Family Centered Care (IFCDC) is often unrecognized. The key role of the head nurse/unit manager in promoting IFCDC and creating a NIDCAP Training Center within the neonatal intensive care unit at the University Hospital of Ghent, Belgium, serves as an example of significant practice change. Instead of taking a theoretical model of change as a starting point, concrete personal experiences and roles that are incorporated into daily practice are described. The aim is to provide insight into how leadership, entrepreneurship, and connection significantly contribute to successful implementation, and to inspire managers facing similar processes.
A description of the evolution of the role of the head nurse from clinical expert to an inspiring, facilitating, and strategic manager includes grounding in clinical skills that lead to an understanding of the necessity of implementing IFCDC. Expansion of the leadership role includes believing in one’s own team, actively giving employees opportunities to build and share expertise, and developing a culture of shared leadership and evidence-based working. The use of care consultants, working groups, and internal study days strengthened both expertise and team solidarity.
A focus on the importance of the head nurse’s entrepreneurial leadership complements clinical expertise and team leadership. Despite budgetary pressure, gaining insight into financial flows, using workload measurement tools, and developing an appropriate financing model enabled continued investment in training and innovation. Strategic alignment with the hospital’s mission, vision, and quality models increased support among senior management.
The head nurse’s role in connecting and communicating is highlighted as crucial for sustainable change management. Transparent communication, multidisciplinary involvement, and attention to pitfalls and concerns proved essential to embed IFCDC and NIDCAP principles into daily healthcare practice and create a shared sense of ownership and pride.
Background When preparing and developing a large project, such as a startup, any practice change involving developmentally supportive, family-centered care can be framed with objectives, project plans drawn, and theoretical frameworks developed from the literature. However, the role of the head nurse/unit manager does not include managing theoretical change processes; rather, it involves using concrete examples to demonstrate how implementation can work in a particular NICU. The theory can be used, often post hoc, to get insight into why a project is or is not implemented in practice.
The intent of the description of the head nurse’s/unit manager’s development and resulting role is to provide a narrative of what worked. The descriptions and strategies included are intended as inspiration for those facing similar implementation projects.
Knowledge background of the nurse manager
In the past, the ‘better nurses’ often rose to managerial positions. The person who was the most handy and who had the most clinical knowledge was often appointed as head nurse. However, it has become increasingly clear that the role has expanded to include many other competencies.
Inspirational role of a nurse manager
As a head nurse, it is first and foremost important to believe in the strength of your own team. Your own employees should be given maximum opportunities to develop their expertise, and in turn, they should share it within the team. A manager primarily facilitates nurses’ growth, embraces the knowledge they develop, and ensures it is shared with colleagues.
In the Ghent NICU, work is conducted across many domains (ventilation, breastfeeding, pain, transport, skin and wound care, resuscitation, developmental care, vascular topics, etc.). The head nurse/unit manager, recognizing the importance of work groups that address clinical care, grants a part-time exemption for a nursing consultant in each care domain. Their role is to follow and document the work group processes and provide training to colleagues, intra- and extramural. The resulting work on the specific care domains is supported not only by the nursing consultant but also by several team ambassadors. In this way, multiple contact persons for various topics are created, and opportunities are offered to different team members. Recognition of evidence-based, high-performance care then spreads within the broader organization.
Every two years, a symposium for nurses and midwives is developed and offered with significant support from the head nurse/unit manager. These educational programs provide a connection and collaboration towards a common goal within the various care domains of neonatal care. It is a moment to ‘shine’ as a team and to share the evidence we have acquired with others. This ‘study day’ can be seen as an example of the department’s dynamic culture, which pursues clinical excellence.
As a unit manager, inspiring is essential to education. For example, looking for relevant topics together and cross-pollinating ideas with each work group is an example of how to provide inspiration. Additionally, providing inspiration is essential for stimulating employee growth on your team. It is an opportunity both to optimize care quality and for nurses individually to grow and rise above themselves. If a manager is not afraid to step outside of their comfort zone, it can lower the threshold for employees to do the same.
Entrepreneurial and innovative role of the nurse manager
Inspiring and facilitating staff are important, but achieving financial freedom and earning the trust of senior management are necessary. In a context where resources are increasingly scarce and priorities are increasingly focused on direct business results, the role of a head nurse/unit manager as an entrepreneur and innovator is not an obvious choice. However, it is essential to the success of any initiative.
Financing as an entrepreneurial skill.
Financial autonomy to generate and control income is a key component of the entrepreneurial role of the head nurse/unit manager. To realize this new cultural shift in how a head nurse/unit manager’s role is perceived, an individualized, well-thought-out financial plan that generates income (e.g., by organizing symposia and offering training to external partners) is essential. In turn, generating income makes it possible, for example, to send colleagues to international conferences and training courses. It is therefore also the task of a head nurse, as the department’s budget holder, to identify, see, and take advantage of financial opportunities.
It is important to have insight into the NICU’s financial flows relative to the entire organization. Very often, people complain about deficiencies, which is nothing new and is probably a sore point in every organization. A head nurse/unit manager should try to get a handle on the income and expenses of their department. Demonstrating financial control often ensures that senior management has the confidence to start working with the NICU entrepreneurially. For example, the Ghent NICU, together with the other Flemish NICUs, successfully validated a neonatal measurement instrument and used it to document nurses’ workload on a daily basis (WANNNT). The outcome data, along with income from fees and historical hospitalization data for our service, enabled us to predict our unit’s budget. Working solely with post-factum data means the head nurse/unit manager is less able to respond quickly to a rapidly evolving context.
Innovation as an entrepreneurial skill.
An important aspect of the entrepreneurial role is innovation. Head nurses are expected to actively explore innovative solutions and consider opportunities to optimize patient care. Undoubtedly, these opportunities present themselves in every organization.
Neonatal care has undergone many developments in recent decades. NIDCAP and IFCDC are receiving increasing attention. It leads, among other things, to better neonatal outcomes, shorter length of stay, fewer complications, and less stress for parents. Sharing the most recent literature on this subject with the hospital’s management and higher management while also emphasizing the financial benefits to the hospital can help free up budgets more easily.
Implementing NIDCAP and IFCDC comes with a significant price tag. When hospitals are under financial pressure, they often quickly reduce non-primary assignments, including training. It is important to demonstrate that the investment in developmental care is profitable in the long term, not only through patient and family outcomes but also by showing the sustainability of quality of care and staff retention. In addition to having self-acquired resources to continue investing in your team’s education and training, it ensures a successful start to greater innovation in implementing NIDCAP training and IFCDC standards of care.
Policy implementation role of the nurse manager
Within the hospital, the mission and vision are periodically adjusted. The individual units and services are asked to align their departmental objectives with the hospital’s policy. Keywords of the Ghent University Hospital policy are excellent—daring, people oriented, and efficient. It does not take much imagination to see that the core IFCDC and NIDCAP values are reflected in these key words in hospital policies. The head nurse/unit manager of the NICU must translate the link between the hospital and the developmental care values using concrete examples from clinical practice and present it to the hospital’s higher management.
Each hospital also works around and with an international quality model. The NICU at University Hospital Ghent also strives to meet, as far as possible, the highest standards set by the European Standards of Neonatal Care. Working with 2 different models is not always efficient. As a service, embedding the Neonatal Standards of Care is done as much as possible within the various care domains with the hospital’s quality model as the goal. On the one hand, this ensures working on quality in a broad sense, as expected by the hospital, and avoiding ‘quality fatigue’ by working with parallel models. It is also an opportunity to demonstrate in practice how to translate the hospital’s keywords and the organization’s central vision into our daily policies.
Connecting the role of the nurse manager
The head nurse serves as a connector within change management, linking vision and practice. In a care context that is constantly evolving, the head nurse helps translate changes into reality for the nursing team. This translation is best made in collaboration with stakeholders from the developmental care team, in concrete terms. The multidisciplinary working group on development-oriented care includes NIDCAP professionals who serve as guides. In this way, a bottom-up culture of co-ownership for important projects is cultivated.
Clear and empathetic communication is essential here. A space for dialogue is created; active listening to questions and concerns is employed; and assurance is provided that employees feel heard and involved.
In this way, a team-oriented culture, in which cooperation and interprofessional respect are central, is promoted. In the past, NIDCAP and a developmental care emphasis were often seen as the work of a small number of passionate nurses. A multidisciplinary approach, in which doctors, psychologists and, for example, care consultants are closely involved, provides much more support for this process and increases the likelihood of success.
Finally, the head nurse/unit manager acts as a role model in the change process. By showing a willingness to change, flexibility, and a constructive attitude, you give the team direction and trust. In this way, the head nurse not only becomes an initiator of change but also a catalyst that connects and strengthens people to achieve these sustainable improvements together.
Communicative role of the nurse manager
The head nurse also plays a central role in communicating key changes. This role goes beyond merely passing on information; it includes actively connecting people, their expectations, and their goals. A head nurse is at the crossroads between the nursing team, the medical staff, and senior management, ensuring that those three worlds are anchored together.
Within the team, creating clarity and trust is a priority, and open communication is crucial. In addition, a culture of dialogue is emphasized in which team members, together, are encouraged to help shape the policy on developmental care. Congruence in thinking and acting is essential here. The manager must ensure that the team’s vision translates into daily operations in direct patient care: in other words, “make sure that you DO what you SAY”.
At the same time, the head nurse is an important communication partner with senior management. Frequent, open, and honest feedback to management about the current state of the change process creates a long-term atmosphere of trust between management and the team. In doing so, the possibility of identifying any additional needs (e.g., additional staff needs) is embedded. SAYING what you DO is therefore not an empty illusion here.
To achieve this, it is also an undeniable asset if senior management wants to delve into the content of the developmental and family centered care project to a certain extent. The presence of a board member during a feedback session with the Ghent NICU staff made it easier to continue the discussion. In this way, co-ownership of the change project is supported at the higher management level.
As in any organization, organizational change sometimes occurs at the senior management level. Every change and new situation should be proactively used to invite new board members to share the unit’s vision and to explain projects within the long-term vision of both the organization and the unit. This approach can ensure that a lot of additional context information is less necessary for specific and/or new questions related to the project.
Pitfalls
Does everything always go perfectly? Not at all. Not everyone is immediately open to change: why would anyone suddenly change something that they have been doing in a certain way for 20 years? Familiar questions are • “Is there sufficient evidence for changes to this protocol?” • “Do all those adjustments cost too much money?” • “Is that profitable?” communication is crucial. In addition, a culture of dialogue is emphasized in which team members, together, are encouraged to help shape the policy on developmental care. Congruence in thinking and acting is essential here. The manager must ensure that the team’s vision translates into daily operations in direct patient care: in other words, “make sure that you DO what you SAY”. At the same time, the head nurse is an important communication partner with senior management. Frequent, open, and honest feedback to management about the current state of the change process creates a long-term atmosphere of trust between management and the team. In doing so, the possibility of identifying any additional needs (e.g., additional staff needs) is embedded. SAYING what you DO is therefore not an empty illusion here. To achieve this, it is also an undeniable asset if senior management wants to delve into the content of the developmental and family centered care project to a certain extent. The presence of a board member during a feedback session with the Ghent NICU staff made it easier to continue the discussion. In this way, co-ownership of the change project is supported at the higher management level. As in any organization, organizational change sometimes occurs at the senior management level. Every change and new situation should be proactively used to invite new board members to share the unit’s vision and to explain projects within the long-term vision of both the organization and the unit. This approach can ensure that a lot of additional context information is less necessary for specific and/or new questions related to the project. Pitfalls Does everything always go perfectly? Not at all. Not everyone is immediately open to change: why would anyone suddenly change something that they have been doing in a certain way for 20 years? Familiar questions are • “Is there sufficient evidence for changes to this protocol?” • “Do all those adjustments cost too much money?” • “Is that profitable?” • “Is that really a priority now?” • “Are we not shifting the focus too much to education and training, to project work, which jeopardizes our clinical work in direct patient care?” • “As a care provider, will I still be able to take my holidays with all those different assignments?”
Thus, we can continue with similar questions for a while.
These are all recognizable concerns in departmental change processes—concerns that can and will come from both the team and senior management and concerns to which head nurses cannot always give an immediate, satisfactory answer. Nevertheless, it is important to stick to basic ideas and evidence, asking the question: “Why and for whom are we doing all this?” which will often help with forward movement. It will be important to stay transparent with the team—even during personal uncertainties— show vulnerability, and, above all, continue to ensure a safe climate in which employees can share their concerns. Working step by step so that the effort remains manageable for everyone and not forgetting to celebrate the team’s successes when reaching milestones are essential to avoiding missteps. In this way, it creates a joint sense of pride with the developmental and family-centered care implementation story, in which even the care for each other as care providers within the team must continue to receive necessary attention.
Summary
Successful implementation of a complex and intensive change process, such as the start-up of a NICU-wide infant- and family centered developmental care program and a NIDCAP Training Center, is not merely the result of a theoretically based project plan but above all of thoughtful and committed leadership in practice. The role of a head nurse/unit manager in this effort is multifaceted: entrepreneurial, innovative, inspiring, facilitating, strategic, connecting, and communicative.
By starting with trust in the team’s expertise and growth opportunities, a culture is created that centralizes shared leadership, multidisciplinary collaboration, and evidence-based care. Consciously investing in training, stimulating internal nursing consultancy, and making expertise visible within and outside the department not only strengthens the quality of care but also increases employee involvement and pride. Entrepreneurial leadership within a healthcare context that is increasingly under financial pressure appears to work. Insight into budgets, the use of financial opportunities, and the substantiation of investments with both clinical and economic arguments have proven necessary to make such a change process possible.
Sustainable change can only succeed if it is strategically embedded in the broader mission, vision, and quality structures of the organization. Alignment with hospital-wide policy objectives increased support and prevented fragmentation or ‘quality fatigue.’ Crucial here is the head nurse’s role as a link between the unit and the hospital’s management, where transparent communication strengthens trust on both sides.
Finally, the change process is inevitably accompanied by uncertainties, resistance, and pitfalls. By leaving room for concerns, working step by step, and celebrating successes, a safe learning climate can be created in which change is not experienced as a threat but, hopefully, as joint growth. In this way, the head nurse not only becomes a manager of change but also a driving force behind sustainable, people-oriented care.
New parents Nicole and Joe welcomed identical twins Ava and Amelie, who were born premature at just 26 weeks at Birmingham Women’s Hospital, and were cared for on the Neonatal Intensive Care Unit (NICU) for over 11 weeks before they were well enough to go home.
Nicole, who lived in Lichfield at the time, was seen at the hospital’s Fetal Medicine Department when they noticed at her 16-week scan one of the twins was growing significantly smaller than the other.
She recalled: “It was my first pregnancy, and we found out we were having twins at six weeks and the pregnancy was going smoothly.
“They noticed at a scan one of the twins was growing significantly smaller, so we were referred to the Fetal Medicine team.”
The Fetal Medicine department discovered the twins had Selective Intrauterine Growth Restriction ( sIUGR ), a condition that can occur in identical twin pregnancies where one twin is growth restricted due to an absent or reversed flow from the umbilical cord.
Nicole added: “We’d never heard of the condition before, and it was really scary knowing something was potentially wrong.
“It was all due to where they’d ended up connecting to the placenta. The bigger twin was plugged in at a larger part so was getting plenty of nutrition, but the smaller twin was plugged into the tail end of the placenta, meaning she wasn’t getting enough nutrition and was so much smaller.
“We didn’t know what this would mean for them, but everyone was so kind and reassuring and explained things in a way we could understand.”
Nicole was scanned twice a week to closely monitor the smaller twin’s growth, until Nicole was 26 weeks pregnant and was admitted overnight for daily monitoring.
She said: “Her heart rate kept dropping low on the monitor, and we were starting to get concerned and thinking about having to deliver them early.
“It kept dropping and taking longer to come back up, and one of the consultants who looked after us said that it was time for them to come out now.
Ava and Amelie arrived prematurely at 26 weeks and 4 days, weighing just 2.2 and 1.9 pounds.
Nicole said: “I was able to see both girls after they were born before they went straight down to the NICU, where they were both intubated for 24 hours before progressing onto oxygen.
“Joe went down with them, and once I’d recovered, they took me to see them, and they looked so tiny and fragile.
“Amelie, the smaller twin, kept getting blood in her feeding tube, so had to be nil by mouth due to the risk of infection. She had a much harder ride to start with, but she kept fighting.”
Both twins started to get stronger with the help of oxygen and feeding tubes, however, when Ava was six weeks old, she developed Necrotising Enterocolitis (NEC) which, an infection which can affect premature babies and is a condition where the bowel becomes inflamed and damaged.
Nicole recalled: “Something hadn’t been quite right with her tummy the day before, but then we got a phone call at home to say she’d taken a turn for the worse.
“It was horrible hearing the phone ring in the middle of the night knowing it was probably about the girls, but knowing we weren’t with them.
“They were both so strong and were real fighters all the way throughout.”
During their stay at the NICU, Nicole and Joe visited every day, arriving first thing in the morning and staying until last thing at night. They also received counselling on the unit and were part of the family group that had been set up for parents to share their journey.
Nicole commented: “Nothing can prepare you for a stay on the NICU.
“While we were there, we lived in our own little bubble and we didn’t talk to family or friends much because it was hard to explain how it feels, and you don’t know what’s going to happen next.
“The team were really supportive, and they helped us be as hands-on as possible with their care, and the family group was really helpful too. It was nice to be able to talk to other parents who knew how it felt and were going through the exact same thing too.
“Walking away from your babies every night was just horrible, so to finally leave with them was a huge relief.
“When we went home, they both still had a feeding tube, but the team were brilliant in giving us training so we could do it ourselves at home. Both tubes ended up being removed the next day as they were doing so well breastfeeding.”
The twins are now over two years old and are thriving at home after their difficult start to life.
Nicole added: “They’ve got such different personalities now, but they’re both very cheeky little girls.
“Ava especially loves animals and trips to the farm, and they both love singing and dancing around the house.
“They both absolutely adore their younger sister and they’re so gentle and kind with her.
“We’re so thankful for everyone at the Women’s Hospital for looking after our girls, they’re both so strong and such fighters and we couldn’t be prouder of how far they’ve come already.
“Shireen Meher looked after us from our time in fetal medicine all the way to the delivery, and she was had such a positive impact on our journey.”
The neonatal intensive care unit (NICU) relies on a multidisciplinary team of advanced practice providers (APPs), including neonatal nurse practitioners (NNPs) and physician assistants. With the Accreditation Council for Graduate Medical Education residency rotation reductions taking effect in July 2025, the demand for NNPs to fill clinical coverage gaps will increase. Anticipated changes in federal reimbursement and Medicaid services and National Institutes of Health pose financial challenges for Children’s Hospitals.
Evidence Acquisition:
This review examines the current state of the NICU APP workforce with special emphasis on NNPs, including historical trends, educational requirements, and the impact of regulatory changes. Data were gathered from surveys completed by national professional organizations, published literature in PubMed, and expert communication.
Results:
Despite their critical role and increased demand, APPs including NNPs face challenges, such as burnout, staffing deficits, reimbursement, and a decline in the number of NNP graduates by 20% since 2022. Neonatal nurse practitioner recruitment is hindered by the lengthy onboarding process and high costs. The integration of physician assistants, hospitalists, and non-NNPs as possible solutions to fill the NNP shortage gap presents challenges, such as lack of training opportunities and managing patients outside their scope of practice.
Implications for Practice and Research:
Addressing workforce shortage requires strategies, including tuition-supported programs, recruiting registered nurses to become NNPs, developing mentorship programs, and increasing NNP preceptors. Further research is needed to evaluate the effectiveness of these strategies and to explore additional solutions for sustaining the NNP workforce.
Introducing Preemies Hub: A New Global Resource for Preemie Families, Built with You in Mind
For every preemie warrior and every parent who has stood beside an incubator, the journey into the NICU often begins without warning. It can feel overwhelming—filled with medical language, uncertainty, and the urgent need to make sense of what is happening to your baby. In those moments, access to clear, trustworthy, and relatable information is not just helpful—it is essential. That is why we are so excited to introduce Preemies Hub, an innovative new platform developed in partnership with Our Kids Health, designed to support families navigating the realities of premature birth.
Preemies Hub was created with a deep understanding that not all families experience the NICU in the same way. For many, challenges are compounded by language barriers, cultural differences, and limited access to reliable, evidence-based information. This platform addresses those gaps by providing translated, adapted, and culturally responsive health information specifically designed for parents across equity-deserving communities. Every piece of content has been developed with respect for different values, beliefs, and ways of communicating—ensuring that families can not only access information, but truly connect with it.
So why does this matter? Because caring for a premature baby is already one of the most emotionally and physically demanding experiences a family can face. Misconceptions about prematurity, lack of preparation for an unexpected early delivery, and difficulty navigating medical information can make that journey even harder. Preemies Hub helps change that. It empowers parents with knowledge they can trust, presented in a way that is clear, compassionate, and accessible—so families can feel more confident, informed, and supported in advocating for their child.
The platform offers a wide range of topics relevant to the NICU journey and beyond, along with resources available in multiple languages including Punjabi, Ukrainian, Tamil, Spanish, Mandarin, Inuktitut, Cantonese, Filipino, Arabic, and more. It also intentionally centers diverse communities, including Black families, ensuring that representation and inclusivity are not afterthoughts—but foundational to the resource itself. For providers, this means having a trusted tool to share with families. For parents, it means finally seeing information that reflects your language, your culture, and your experience.
At Neonatal Womb Warriors, we believe that every family deserves access to information that meets them where they are. Preemies Hub is more than just a resource—it is a step toward equity in neonatal care, a bridge between knowledge and community, and a reminder that no preemie journey should be navigated alone. 💙
The quality of health in Cambodia is rising along with its growing economy. The public health care system has a high priority from the Cambodian government and with international help and assistance, Cambodia has seen some major and continuous improvements in the health profile of its population since the 1980s, with a steadily rising life expectancy.
A health reform of Cambodia in the 1990s, successfully improved the health of the population in Cambodia, placing Cambodia on a track to achieve the Millennium Development Goal targets set forth by the United Nations. One such example is the Cambodian Health Equity Fund, largely financed by the country itself, created in 2000 to increase access to free health care to around 3 million poor people. The Fund, which pays for traveling expense and even daily allowance for anyone accompanying a patient, has resulted in increasing health care seeking among Cambodians who otherwise could not afford any kind of medical care. As a result of the reform, mortality rates significantly dropped. Similarly, life expectancy at birth in 2010 was 62.5 years, a 1.6 folds increase from 1980.
GLOBAL PRETERM BIRTH RATES – Cambodia
Estimated # of preterm births: 10.5 per 100 live births
Cambodia’s sustained progress in improving maternal, newborn and child health
20 February 2025
At the beginning of the 2000’s, Cambodia faced alarming maternal, newborn and child health indicators. The maternal mortality ratio stood at 437 per 100 000 live births, while newborn and child mortality rate accounted for 37 and 124 per 1000 live births respectively. Limited infrastructure, a shortage of skilled birth attendants and financial constraints hindered progress. To tackle these challenges, the Cambodian government, with support from WHO and key partners, embarked on a transformative journey to strengthen maternal and newborn health services and ensure equitable access to quality care.
Today, skilled birth attendance is near universal, with 98.7% of births attended by trained health professionals and 97.5% of women giving birth in a health facility. Between 2014 and 2021-2022, neonatal and under-five mortality rates declined by 54%, from 18 to 8 and from 35 to 16 per 1000 live births respectively, far exceeding the global average reduction of 14% during 2015-2022. Cambodia achieved its Sustainable Development Goal targets for reducing neonatal and under-five mortality eight years ahead of schedule.
Strengthening health systems
Cambodia’s investments in health systems and workforce capacity have been instrumental in driving progress. Midwifery training programmes have equipped health workers with essential skills to provide safe, high-quality care, including routine antenatal care, essential intrapartum care, postnatal care, and management of childbirth complications. Deployment strategies have ensured that even remote health centres are staffed with skilled birth attendants.
To incentivize facility-based deliveries, the government introduced a delivery incentive programme for health teams in 2007 and launched cash transfer programmes for pregnant women and infants from poor families in 2019, targeting the critical first 1000 days of life. These initiatives encourage families to seek comprehensive antenatal and postnatal care, ensuring access to a full package of essential health services. Financial mechanisms such as health equity funds, cash transfers and fee exemptions have alleviated economic barriers, making institutional care more accessible to vulnerable populations.
Improvements in water, sanitation and hygiene infrastructure have also contributed significantly to better health outcomes. An integrated routine primary health care delivery system has been established across provinces and districts, ensuring that essential services effectively reach communities. Health promotion and behaviour change campaigns have played a vital role in encouraging exclusive breastfeeding and antenatal care-seeking behaviours.
Strong leadership and strategic framework
A key milestone in Cambodia’s progress has been the strong leadership of the Ministry of Health, which has provided clear strategies for advancing maternal and newborn health. Two main coordination platforms — the Sub-Technical Working Group for Maternal and Child Health and the Early Essential Newborn Care (EENC) Coordination Committee — were established and have convened regularly to align efforts within the Ministry and with health partners.
With technical support from WHO and funding from the Korea Foundation for International Healthcare (KOFIH), the EENC Coordination Committee plays a crucial role in harmonizing national and sub-national efforts, monitoring progress through regular reviews, mobilizing resources to scale up EENC practices, and ensuring consistency in care delivery while addressing service gaps.
Recognizing the need for a strategic and systematic approach to newborn care, the committee led the development and adoption of the Five-Year Action Plan for Newborn Care (2016–2020). The plan emphasizes scaling up EENC and institutionalizing evidence-based practices, integrating key life-saving and cost-effective interventions — such as routine immediate care for all newborns under “The First Embrace” approach, as well as measures to prevent and care for small or sick newborns.
By 2023, EENC coaching was implemented in 89.4% of health facilities (1187 out of 1328), surpassing the 80% target. Kangaroo Mother Care for preterm and low birthweight infants has been scaled up to two national hospitals and ten provincial and district referral hospitals, while a national protocol for EENC in Caesarean sections, introduced in 2019, has standardized care nationwide.
“Maternal, newborn and child health are essential components of investing in human capital. Providing quality care for mothers and newborns brings immense benefits — not just for families, but for entire communities and economies. Cambodia’s coordinated approach to maternal and child health serves as an inspiring model for the region and globally. It demonstrates what can be achieved with strong national leadership, dedicated health workers and sustained partnerships,”stated Dr Marianna Trias, WHO Representative to Cambodia.
Remaining challenges
Despite significant achievements and high coverage of antenatal care and facility-based deliveries by trained health personnel, challenges persist. While maternal mortality has declined, it remains high at 154 deaths per 100 000 live births, primarily due to haemorrhage and pregnancy-induced hypertension — both preventable causes. Greater efforts are needed to get on track to achieve the 2030 target of 70 deaths per 100 000 live births. Similarly, child malnutrition continues to impact long-term productivity, with 22% of children under five stunted and 10% wasted for over a decade.
Disparities between urban and rural areas and gaps in facility capacity to provide quality essential services require targeted attention. Addressing unmet family planning needs and expanding adolescent-friendly services are crucial, particularly as rural adolescent girls aged 15–19 experience significantly higher birth rates than their urban peers.
The way forward
Moving forward, further reducing maternal and neonatal mortality requires a stronger focus on enhancing the quality of care. Building on significant improvements in coverage, efforts should prioritize improving the quality of basic routine care during antenatal and intrapartum periods, including emergency obstetric care, alongside establishing robust referral systems for cases requiring higher-level care. Achieving this will require both the strengthening of quality improvement mechanisms with enhanced monitoring and the implementation of targeted improvement actions.
The Fast-Track Initiative Roadmap for the Reduction of Maternal and Newborn Mortality (2025–2030) aims to accelerate progress by scaling up interventions, sustaining quality care and addressing service delivery gaps. To support its implementation, WHO will assist in developing a comprehensive country action plan and support the Coordination Committee for Strengthening Quality of Care and Wellbeing of Women, Maternal, Newborn and Child Health to ensure effective coordination and execution.
Bringing clean water to where life begins: a neonatologist’s story from Ukraine
12 June 2025
These are the words of Galina Dmytrova, a neonatologist at Chuhuiv Central Hospital in the Kharkiv region of Ukraine. To her patients, the support Galina and her colleagues provide make a difference between life and death.
“They are already under enormous stress because of the war and now we are facing water shortages again. Before the war, you’d turn on the tap and not think twice. But now, under daily shelling, the electricity goes out, and with it, the water too,” says Galina.
5 water stations set up across Kharkiv city and the wider region in Ukraine continue to allow hospitals to provide essential care despite the war. Among them is Chuhuiv Central Hospital. The stations were installed in 2025 by WHO with funding from the European Union and in partnership with Ukraine’s Ministry of Health.
For communities regularly affected by attacks that disrupt electricity and water supply, this support ensures access to clean, safe water for both patients and health workers, which is critical in maternity wards, where hygiene and continuity of care are vital.
“In our hospital, thanks to WHO and the European Commission, we now have a water treatment system. I’m deeply grateful. It’s hard to explain the importance – especially for mothers and their babies. Many people actually can’t believe women are still giving birth under such harsh conditions. But they are, and I truly admire them,” Galina adds.
Those are our babies
In 2024, some 179 children were born in the Chuhuiv Central Hospital in the Kharkiv region. This year, the birth rate is similar; in the first 3 months of 2025, hospital staff oversaw more than 45 births.
“That’s our maternity ward, our babies, around 15 every month – even while the war goes on,” Galina tells us.
The certainty and assurance that care is available, that there is a hospital nearby, gives people hope. A functioning hospital is a reminder that life goes on. The opposite is also true; when health facilities are damaged or attacked in conflict, it not only deprives communities of access to health care. It also deprives them of hope.
“When the war started, I was new to Chuhuiv. I didn’t know the area that well. One night, a woman in labour came very late and explained they’d been looking for a boat. The bridge to her village had been destroyed – so, to get here, they had to cross the river. But they did it, because they knew here was a hospital that could help,” says Galina.
Fortifying our commitment to pediatric academic medicine during turbulent times
Academic Medicine, with its tripartite mission to advance medical science, cultivate the next generation of healthcare professionals, and provide exceptional clinical care, offers unparalleled opportunities to shape the future of evidence-based healthcare delivery and inform health policy. Biomedical innovation developed through collaboration between academic medicine and public health can improve health at the individual and population health levels including mapping disease trends and improving treatment outcomes. According to the Association of American Medical Colleges (AAMC) economic impact report published in 2022, every one dollar spent by the AAMC member medical schools and teaching hospitals contributes $1.62 to the United States economy. Unfortunately, medical schools and teaching hospitals continue to face reductions in government funding for research and education support and have faced decades of under-reimbursement for publicly insured care, often delivered in these systems which also serve as safety net health care systems across the country.
The National Institutes of Health (NIH) revealed that the nation’s supply of physicians engaging in research continues to decline, with increased competition for decreasing available federal funding. Pediatric research is disproportionately impacted by gaps in funding, directly impacting the scientific innovation aimed at improving child health outcomes. As advanced technology such as artificial intelligence (AI) balanced with rapidly evolving scientific discoveries offer novel and dynamic clinical approaches to care, these persistent funding gaps often lead to pediatric care falling behind adult care delivery. With an estimated 646,000 researchers supported by federal grants, 48% of whom are students and trainees, the cross-cutting dependence and impact of federal funding on research and education is undeniable. Therefore, to mitigate further impact in pediatric academic medicine, continued promotion of NIH-funded pediatric research must leverage the understanding that return on the investment continues over the lifespan of the growing child to adult.
In the article by Arnaez and colleagues, Dr. Garcia-Alix is celebrated for his longitudinal contributions and global reach in academic medicine, specifically in field of Neonatal Neurology. By understanding that at least 30% of neonates admitted to Neonatal Intensive Care Units (NICUs) present with neurological pathology or other conditions impacting brain development, he recognized the importance of studying neuroprotective factors that impact these children’s morbidity. For Dr. Garcia-Alix, this area of interest sparked a career long passion. His dedication was evident, while advancing and supporting academic education and mentorship of his learners, generously investing time and role modeling for further generations. With the appreciation of the life-course model for his neuro-neonatal patients, Dr. Garcia-Alix, translated the overarching goal of improvement of functional outcomes by creating Brain-Aware Care, a family-centered, multidisciplinary approach targeting protecting an infant’s developing brain at the earliest stages. He recognized and appreciated that neuro-neonatal care delivery differs requires a comprehensive, multidisciplinary, family-centered approach tracking continuity of care as a baby grows, as is the continued research to understand how to develop appropriate care guidelines and protocols for developing, growing and thriving children. Dr. Garcia-Alix dedication and contributions as a physician scientist and educator with global impact on generations of patients in the field Neonatal Neurology is a testament of the longitudinal investment and support required to achieve the return on investment in child health outcomes in pediatric academic medicine.
Fiscal pressure on the future of pediatric academic medicine
The goal of pediatric academic medicine is to continue to develop and support clinician scientists like Dr. Garcia-Alix throughout their careers, who are committed to innovation, clinical care, and education. However, the fiscal pressure on pediatric academic medicine for the past several years, balancing under-reimbursed Medicaid clinical activity, rising labor costs, inadequate availability of pediatric extramural funding, and insufficient graduate medical education funding, is leaving teaching hospitals and partnered medical schools to find novel ways to advance this pediatric academic mission. Institutional-level investment in clinician scientists (e.g., 3 year contracts where early career faculty have time to successfully compete for a career development grant) are less feasible as financial pressure mount from funds flow models in Children’s Hospitals. Similarly, competition for institutional (e.g., KL2) and external (e.g., K23) grants are increasing as paylines are decreasing. With recent changes in administration policy, opportunities for first-generation scientists and those underrepresented in biomedical research (e.g., diversity supplements, MOSAIC award) are now unavailable. Protecting NIH funding, particularly money appropriated to child health research, is essential to promote the mission of pediatric academic medicine. Moreover, given diminishing availability of federal extramural funding, reviewing alternative, non-traditional academic sources of funding mechanisms for research including private industry, venture capital or foundation funding will be necessary to explore to uphold the tripartite mission of our pediatric academic mission.
In addition to research challenges, pediatric residency training programs are in jeopardy. Since the annual budget for graduate medical education is supported through the Congressional appropriations processes, strategic consideration of alternative platforms of support for retention, learner mentorship, and workforce pipelines are critical to ensure continued access to care for our pediatric population. Mentors can be instrumental at different stages of learners, from guiding students in explicit academic knowledge, to implicit knowledge of professionalism, ethics and the art of medicine.9 Retention of faculty is critical during times of economic stressors in academic medicine and leaning on mentorship and sponsorship as a key strategy, especially given pay inequity between pediatric and adult academic clinicians. Finally, evaluation of the economics of health professions education (HPE), is critical with ongoing cost-constrained academic medicine environments, especially with graduate medical education funding at risk.
Call to action for the health of our nation’s children
We need to reinforce and double-down on our commitment to the pediatric academic medicine mission-centered goal in improving the health and well-being our children and youth through investments in advancing science, cultivating our next generation of pediatric learners and improving clinical care for our pediatric patients. With several decades of Medicaid under-reimbursement, challenging degradation of federal pediatric extramural funding compared with adult funding, and even greater disparities in pediatric workforce shortages, families are facing a stark reality in worsening access to pediatric healthcare which will only grow in the upcoming years due to Medicaid cuts. We must continue to educate legislators and government officials that children require the same level of extramural funding (if not greater), in efforts to evolve even greater investment on return investment over the life-course trajectory. We must advocate for reimbursement parity greater than Medicare, especially understanding the discrepancy between Medicaid enrollment and Medicaid expenditure on children, being roughly 50% and 20%, respectively. Finally, we must educate that pediatric academic medicine, with its medical schools and teaching hospitals, contribute to the economy and health of the United States.
Call to action
Support the Bipartisan Legislation H.R. 3890 (Sewell, Fitpatrick)- Resident Physician Shortage Reduction Act of 2025- Educate your local legislators on the importance of Pediatric Education workforce pipeline and its’ impact on access to care, especially in rural communities
Continuing to unequivocally advocate for Children’s Hospitals Graduate Medical Education (CHGME), and budget appropriation within the annual Labor Health and Human Services Appropriations Process for the House and Senate Committees
Support NIH funding increases for Pediatric Research funding, which will increase and parity (and increase) for pediatric extramural funding for research to improve the evidence-based decision-making, and uphold trust with patients, families and society
Continue to educate our legislators about the life-course model in child health, and the return on investment, with the reality that for every $1 investing in early intervention, there is a return on investment from $1.26 to $17.07 for every child invested in the United States.
Finally, ensure that with the rapid advancing in technology, including artificial intelligence (AI), gaps do not arise regarding access to therapeutic tools between pediatric and adult populations in healthcare.
Background: Perinatal loss is a profoundly complex form of grief, often linked to heightened risk of prolonged bereavement and adverse mental health outcomes. Perinatal grief rooms-private, supportive spaces within healthcare settings-aim to help families process their loss, spend time with their baby, and create meaningful memories in a respectful environment. While bereavement care has received growing attention, the role of the physical environment in supporting grief remains underexplored.
Objective: To synthesize current evidence on how dedicated physical spaces can support individuals and families after perinatal loss, and to identify priorities for research, design standards, and interdisciplinary collaboration.
Methods: A narrative review was conducted in accordance with PRISMA-ScR guidelines. Literature searches were performed across PubMed, PsycINFO, Medline (OVID), Embase, ScienceDirect, SCOPUS, SciELO, and Google Scholar using terms, such as “perinatal grief rooms”, “bereavement rooms”, “angel suites”, “butterfly suites”, “snowdrop suites”, “cloud rooms”, “designated units for perinatal loss”, and “birthing + bereavement suites”. The review examined (1) the current role of physical spaces in the perinatal loss experience, and (2) how their availability and design may influence grief outcomes.
Results: Of the 17 articles meeting inclusion criteria, only 4 (24%) referenced bereavement rooms, and just 3 (18%) noted the need for formal protocols-without offering concrete examples. No studies evaluated implementation, design standards, or measurable impact on grief, mental health, or family well-being. This lack of empirical evidence and standardized guidance underscores a critical gap that limits integration of therapeutic environments into perinatal bereavement care.
Conclusion: Despite increasing recognition of the importance of bereavement care, dedicated grief rooms remain under-researched and inconsistently implemented. Advancing this field will require rigorously designed studies, development of design standards, and collaborative partnerships among healthcare providers, researchers, policymakers, and design experts to ensure equitable access to therapeutic spaces for grieving families.
Harnessing the power of a multidisciplinary team carries vast potential for effectiveness and problem-solving—while achieving high-performance with diversely skilled stakeholders requires adroit management.
The Center for Innovative Leadership (CIL) exists to support and accelerate the production of new research on leadership in today’s dynamic, complex organizations and bring research to life through engaging student experiences and powerful industry partnerships.
Summary: In healthcare it is common practice for multidisciplinary teams to be involved in efforts to improve the quality and safety of patient care. The perioperative period, which encompasses the time before, during, and after a surgical operation, is a prime target for multidisciplinary improvement efforts because of the diversity of professional roles and care delivery settings involved. Failure to achieve improvement targets in this context is often attributed to lack of resources or resistance to change.
A recent study counters this view, suggesting failure is more likely to be due to the way the multidisciplinary improvement team is led and how well it collaborates. Successful improvement projects depend on effective leadership—from designing the team, communicating a shared vision, planning the project, through to creating a collaborative approach to getting work done, and a structured training and feedback process.
A new study distils existing literature and gathers expert opinions on leadership and high-performing teams to offer practical guidance on those factors and behaviors relevant to the delivery of perioperative improvement projects, but also to leading multidisciplinary teams outside of healthcare.
High-performing healthcare services continually seek to improve patient experience and outcomes. One key area of focus for improved performance has been the perioperative period—the time leading up to, during, and after surgery. Unfortunately, perioperative improvement teams often fail to achieve their goals and when this happens the blame is often ascribed to resistance to change or lack of resources.
A recent study highlights that another important – yet overlooked – reason why t improvement projects fail is because of the way multidisciplinary improvement teams are designed, how they are led, and how the multidisciplinary teamwork is managed.
The study, from Christina Yuan and Michael Rosen, Faculty Affiliates at the Center for Innovative Leadership at Johns Hopkins Carey Business School, in collaboration with Tasnuva Liu, Benjamin Eidman, Della M. Lin, and Elizabeth Wick, contends that taking time to pre-plan and continually reflect on how team leadership behaviors are enacted is the best way to ensure team success—yet this is often overlooked.
The researchers surveyed a range of thought leaders and team leaders with deep-rooted experience in perioperative work to discover the leadership behaviors and practices considered to be most relevant to planning and implementing perioperative improvement initiatives.
Based on their findings the researchers recommend the following six key areas leaders should consider when designing and leading teams to deliver perioperative improvement projects—recommendations that carry implications for the management of multidisciplinary and cross-functional teams in a wider context too:
Design and Define
It is important to clearly define the aims of the mission, and to choose a team that includes all stakeholders and the right mix of skills and roles—allowing flexibility and ensuring that roles are not too rigidly defined. It is also wise to include those who are skeptical about improvements, as well as those who are more receptive, so as to understand the scope of the challenge ahead and ideally to bring skeptics on board.
Manage
Leaders should create an environment where collaboration is prioritized and fine-tuned. Through discussion, establish effective processes for getting work done and delegating tasks. With agreement leaders should identify challenging but realistic goals for the team. They should monitor and report on progress and help the team recover from any small set-backs.
Sustain
An environment of psychological safety should be created, where team members feel they have a voice and their opinions are acknowledged. Leaders should communicate regularly to everyone to show how the project is progressing and to build a collective understanding of what is being achieved and what more might be done. This should be framed as a positive way to learn from successes and failures as opposed to seeking compliance.
Train and Feedback
Listening, asking good questions, and soliciting feedback are essential leadership behaviors. In a multidisciplinary team it is important everyone participates and is heard, including less vocal team members. This interaction can be the basis for providing skills training and promoting continuous learning—appreciating that failures can be opportunities for learning.
Manage Team Boundaries
It is a leader’s role to clarify the boundaries between the core project team and other groups and departments, as well as to be a liaison with these entities. It is vital to obtain senior leadership buy-in at the outset of the project and to maintain this throughout with regular reporting on progress, successes, and any potential barriers. Messages should be brief and individualized to address each senior leader’s particular concerns.
Manage Organizational Context
Aligning the team’s efforts with organizational needs is key. Here an important factor is for senior leaders to ensure access to data the team needs to make decisions and do their work. Removing barriers to data sources and providing the team with opportunities to ask senior leaders questions and get information as needed is also the leader’s responsibility.
In a busy healthcare setting, where the delivery of a perioperative improvement project will be one of many priorities for the members of the assigned multidisciplinary team, above all team leadership must be clear and precise. It must ensure all members of the team understand their roles, feel free to participate fully, and are empowered to achieve to the best of their abilities. There are innumerable management theories and practices that might be suggested to accomplish this.
The value of Yuan and Rosen’s study is that it helps to distil the essence of what is really required for effective team leadership in this context.
Recent research provides new insights into significant brain and behavioral changes in the baby’s first six months after birth, laying a foundation for later physical, cognitive, and social development. Preparation in utero leads to infant behavioral responses that ensure survival, and the caregiving environment provides safety and protection during these early months. Brain development accelerates, and regulation of biophysiology is demonstrated in respiratory, cardiovascular, and gastrointestinal systems, as well as in behavior.
Newborns and young infants often exhibit behaviors that signal caregivers to provide protective and nurturing responses. Caregivers, usually the baby’s parents, typically respond to the baby’s signaling. Mutual reinforcement of behavior leads to the dyad becoming adapted and regulated in early infancy. Mismatches in the baby’s explicit behavioral signaling and/or challenges in the caregiver’s reading and/or responding to the baby’s behavior in these early formative months can affect later social, emotional, and cognitive development.
Signaling behavior:
Signaling behaviors such as crying, vocalizations, alertness, and face scanning prompt interaction with others. Crying signals distress and is likely to promote immediate caregiver response. Facial expressions, such as smiling, brow knitting, and pouting, often elicit an emotional response from the baby’s caregiver. The resulting dyadic exchanges promote ongoing social interaction. As brain development proceeds at a rapid pace, the transition from reflexive to volitional behaviors typically occurs around 2-4 months. These more intentional behaviors lead to more sophisticated behavioral repertoires and social bids.
The responsive caregiving environment and mutual interaction between caregivers and their baby during this time contribute to the development of increasingly regulated behavior. Caregivers of newborn and very young infants need support to understand babies’ available signaling behaviors, as these behaviors have a significant impact not only on early caregiving relationships but also on brain development.
Signaling behavior of hospitalized babies:
Early-born or sick newborns are at a disadvantage in the development of signaling behavior. Their experience as a fetus and during delivery can interfere with the development of or overwhelm effective behavioral communication. Early-born babies have not had experiences during the last weeks of their fetal life that contribute to more organized behavioral responses. Their reflexes may be weak or hard to elicit, arousal and visual regard may be limited, and physiologic instability may affect responsiveness. Necessary medical support may also overwhelm their meager energy and/or fail to recognize their efforts to signal.
In addition to early birth and/or medical concerns, the caregiving environment in intensive care is vastly different from the “expected” one for a more typically developing baby and can thus affect foundational brain and behavioral development. It is well known that long-term effects on brain development, social/emotional, and cognitive development in babies hospitalized at birth are recognized as less than optimal. Early birth, medical issues, and hospitalization can interfere not only with a baby’s ability to provide clear signals but also with caregivers’ ability to interpret them.
Intensive care professionals are typically trained in medical assessment and intervention, which until recently have not included behavioral assessment. Berry Brazelton was a pediatrician who took the lead in understanding the behavioral repertoire of newborn babies. Heidelise Als, one of his protégés, extended that understanding to babies born early. She developed the Newborn Individualized Developmental Care and Assessment Program (NIDCAP) and emphasized observing and interpreting babies’ behavior. Based on those assessments, caregiving recommendations are developed to help the baby achieve regulated behavior and thus achieve their own developmental goals. Since her early work, most NICUs now incorporate identification of at least some behavioral signals and implement strategies to support babies’ development.
IFCDC standards provide a foundation for supporting signaling behavior:
At the center of the IFCDC standards concept model is an emphasis on the baby as an interactor in their relationship with their primary caregiver, typically the mother. Woven into each of the other principles is the understanding that the baby influences how they are cared for both by family members and by intensive care professionals. The model implies that the baby’s individualized interaction with the environment of care influences their physical, social, emotional, and cognitive development.
Each of the six evidence-based areas of developmental care emphasizes the importance of understanding the baby’s behavioral communication to fashion an individualized approach to their caregiving experience. Additionally, each of the six areas includes an emphasis on supporting the baby’s primary caregivers, typically the parents, to observe, interpret, and respond to the baby’s behavioral signals. Early-born and medically fragile babies’ signals can be challenging to interpret. Professional staff must have a thorough understanding of the baby’s signaling behavior to provide individualized caregiving and support parents in knowing how best to care for their baby.
The continuum after discharge:
The continuum after discharge: Leaving intensive care marks a transition into early infancy and involves a multitude of brain and behavioral changes. During these foundational months, rapid brain development is reflected in significant behavioral changes. As noted above, reflexes become modified into volitional events, and signaling behaviors become dependent on the baby’s environment of care. As the medically fragile or early-born baby becomes more physiologically and behaviorally regulated, their signaling becomes more socially responsive.
The primary caregiver, on the other hand, may still be affected by the intensive care experience and be hesitant to interact with their previously fragile baby vigorously. It is postulated that as the baby becomes clearer in their communication, more intentional, and ready to interact, the parent can be less responsive to their bids.
Although targeted interventions for caregivers in their early relationships with their baby begin in the NICU, they must be continued after discharge, as behavioral changes in the first months are rapid, and it is often difficult to understand how best to respond.
Caregivers’ understanding of their baby’s signaling behavior as it changes over time must be supported and reinforced by knowledgeable professionals for at least the first six months of the baby’s corrected age, and sometimes longer, depending on the baby’s adaptation during this period. As brain and behavior, as well as parenting skills, are still developing, individualized dyadic care should be provided early and frequently after discharge and should continue for at least six months.
Conclusion:
The continuum of brain and behavior development from the fetal to the newborn to the early infancy period evolves in the context of the baby’s environment of care. The behavior the baby uses to signal their need for caregiving changes dramatically over the first six months, and caregiving responses that regulate the baby’s behavior lay the foundation for later physical, cognitive, and social emotional development. Babies born preterm or medically fragile are typically less effective in their signaling behavior. Due to the altered environment in which they develop and the myriad factors that influence their parents’ responsiveness to their behavior, they and their parents need supportive measures to assess, interpret, and provide support for early development. The current IFCDC standards incorporate supportive strategies into both the concept model and the evidence-based practice areas. Because brain and behavior are particularly vulnerable during the first six months, there is a need not only to understand and respond to their behavior in intensive care but also to continue this understanding and response after discharge for at least the first six months.
Breastfeeding a premature baby requires special care, patience, and close monitoring—especially during the transition from tube or bottle feeding to the breast. In this hospital-based guide, a healthcare professional demonstrates how to safely breastfeed a growing preterm infant while ensuring adequate milk intake.
This video explains how pre- and post-feeding weight checks are used to accurately measure how much milk a premature baby consumes. You’ll learn correct breastfeeding positions, how to maintain proper body alignment, and how to achieve a deep, effective latch. The guide also helps parents distinguish between nutritive sucking and comfort sucking, recognize early signs of fatigue or stress, and follow essential safety protocols such as monitoring breathing patterns and proper burping techniques.
Ideal for parents of premature babies and NICU families, this video supports confident, safe breastfeeding during a critical stage of infant development.
INNOVATIONS
“In the 1960s, when the first NICUs opened, premature infants had a 95% chance of dying. Today, they have a 95% chance of survival” – Dr. Rahul K. Parikh, a pediatrician from California, published in August 2012 in the New York Times . This incredible shift in survival can be considered a great example of the conquest of modern neonatal medicine. Among many technological advancements, the ability to continuously monitor vital signs such as heart rate and respiratory rate, was followed by closed loop body temperature (T) control, blood pressure assessment, and finally by continuous and non-invasive monitoring of oxygen saturation. Monitoring of these vital signs was paramount for the assessment of well-being and detection of pathophysiological states in tiny patients, allowing for adjustments or initiation of treatments or interventions that are lifesaving.
There is no question that neonatal technology has advanced tremendously over the last 60 years and parents have become very approving of this. In the book From Surviving to Thriving, Fabiana Bacchini, the mother of a twin baby boy born at 27 weeks, wrote: “I was able to watch in happiness and gratitude, all the technology that exists to keep these tiny beings alive.” Later, it also became clear that, despite the important role of technology, it can also cause fear and anxiety for parents. Fabiana mentioned that the first time she entered the NICU “I did not see a baby, I saw wires, monitors and a breathing machine” .
Indeed, current technology for vital signs monitoring uses several skin sensors connected to the bedside monitors by wires and cables. In most patients, raw signals, average values and trends of heart rate, respiratory rate, temperature, and oxygen saturation are continuously displayed. However, this system carries some challenges for patients, parents, and healthcare professionals (HCP) as the multiple wires can tangle around the infant body, restrict the patient’s movement, and cause discomfort or pressure sore. Hence, regular care involves frequent removal, reapplication, and readjustments of the sensors, which may harm the fragile neonatal skin, cause pain, and/or interrupt resting or sleeping. For parents, not much information is available on what are their perspectives on these vital signs monitoring systems. Some small surveys have reported that the presence of multiple wires and cables can cause intimidation and additional stress, acting as a barrier to skin-to-skin contact for fear of disconnecting the sensors or wires, or interfering with regular monitoring . This technology may also increase HCP’s workload as wires and cables may touch contaminated surfaces or become soiled with urine, blood or stools, increasing the risks of nosocomial infections. Consequently, nurses must constantly inspect, sanitize, reposition, or replace components of the system.
Is a Wireless NICU Possible?
Neonatal intensive care units manage a diversity of health problems with variable degrees of severity and patient maturation. To develop a wireless system that can be used during the first days of life in a 400 g extremely preterm infant born at 22–23 weeks of gestation and a 4-kilo term infant born with perinatal asphyxia is a real challenge. Furthermore, there are some more stable infants that are just feeding and growing, or infants with chronic problems that require prolonged hospitalizations. Noticeably, the needs of these populations are different, creating challenges for the development of new vital signs monitoring systems. As an example, an extremely preterm infant in the first days of life spends most of the time quiet, sleeping inside the incubator, and has very sensitive skin that can easily be damaged by skin adhesives and sensors. In these cases, non-contact technologies may play a very important role, at least for the monitoring of heart rate and respiratory rate. This is not the case with more stable and mature infants that are active, and where parents can constantly hold and promote kangaroo care (KC). Therefore, the adoption of new monitoring technologies needs to consider those different needs, be very familiar with the technology advantages and limitations, and develop protocols and proper training for all healthcare providers involved.
Is a Wireless NICU Desirable?
Although wired vital sign monitors are the standard, they are frequently cited as obstacles to key aspects of family-integrated care and routine clinical practice. Wireless vital sign monitoring technologies are increasingly being explored as a potential solution to these issues. However, there is limited research available which quantitatively or qualitatively examines how key NICU stakeholders such as parents and HCPs, perceive the current monitoring system and these wireless innovations.
The small number of existing studies have highlighted that the wires and sensors used in current systems interfere with skin-to-skin contact and KC, limit parents’ ability to hold or touch their infants, and contribute to a highly technical environment that many find overwhelming. Survey and interview studies consistently show that parents perceive the wires as intimidating and as contributing to their anxiety . HCPs also express widespread concerns with the current systems, especially regarding the physical clutter created by wires, challenges with positioning and handling of infants, risk of pressure sores from adhesives, and the frequency of false alarms .
These concerns have led to growing interest in wireless monitoring as a possible solution. While research on parent and HCP in this area is very limited, all existing studies show optimism toward the adoption of wireless technology. Parents have generally responded positively, citing benefits such as reduced anxiety, possible easier interaction with their infant, improved KC, and enhanced infant comfort. However, there are some apprehensions related to signal reliability, sensor size and appearance, battery duration, and potential risks such as radiation exposure . Similarly, HCPs have voiced strong support for wireless monitoring, highlighting its potential to reduce handling difficulties, decrease false alarms, and improve comfort for both infants and families . Importantly, they also emphasize areas of concern, including reliability, safety related to radiation, and costs . In particular, the absence of economic feasibility studies is a significant gap in the current literature.
Overall, the available evidence indicates that wireless monitoring is a promising advancement, with support from key stakeholder groups in the NICU. The shift away from wired systems could improve key aspects of neonatal care, particularly KC and parental engagement, while also addressing some of the frustrations voiced by HCPs. However, to address these challenges, and ensure new technologies will be adopted by NICU staff and parents, concerns around reliability, safety, and cost must be addressed through careful user-centered design, and rigorous research including clinical evaluation. Future research should prioritize that wireless systems not only meet regulatory and clinical standards but are also feasible and acceptable for daily use in the NICU.
What Wireless Technology for Neonatal Vital Signs Monitoring Is Available or Emerging?
Non-Contact
A large number of small studies have investigated the use of non-contact vital sign monitoring in the NICU. Most studies used a single-device system and monitored respiratory or heart rate using offline analysis. The following technologies have been tested: red, green, blue cameras, infrared cameras, monochrome cameras, depth cameras, and radar, primarily for respiratory rate and heart rate monitoring . Non-contact sensors are typically placed at the head or foot of the infant’s incubator or crib. In some cases, the sensor cannot collect data through the plexiglass and may require either an open incubator or a small opening to maintain a clear line of sight. Depending on the technology and algorithms used, a defined Region of Interest within the sensor’s visual field may be designated for vital sign extraction.
These studies generally featured small sample sizes and short recording durations of <1 h . Nearly all exclusively focused on accuracy by comparing novel non-contact methods to a reference measurement using the Bland-Altman method. Analyses of heart rate and respiratory rate using this method revealed low bias and moderately acceptable 95% limits of agreement. Feasibility outcomes were rarely explored and measured using metrics such as the amount of usable data or processing times. No studies explored outcomes related to safety, although this can be expected as these monitoring methods pose no threat to the fragile neonatal skin.
While these technologies show promising preliminary results, several concerns remain. First, feasibility concerns remain as most devices rely on an uninterrupted clear view of the infant. How it would perform in situations where the infant is moving, clothed, or receiving care needs to be better clarified. Additionally, a systematic review of non-contact technologies applied the QUADAS-2 assessment and revealed several areas of concerns regarding risk of bias and applicability due to lack of clear inclusion and exclusion criteria and small sample sizes . Furthermore, many studies lacked key basic descriptors of the population, such as age and weight, making it difficult to ensure a representative range of NICU patients such as those requiring respiratory support or in incubators were included in the research. Additionally, some studies provided incomplete descriptions of reference measurements, only naming them as “standard” or “routine” monitoring, limiting the ability to determine the risk of bias. Unfortunately, most non-contact studies lack a conflict-of interest statement.
Ultimately, non-contact technologies may represent an appealing monitoring solution for some of the most vulnerable infants in the NICU, such as extremely premature infants with extremely fragile skin. This research area is rapidly growing as non-contact studies often utilize commercially available cameras and present low research risks for patients. However, concerns regarding the ability to perform reliably for prolonged periods in a real NICU environment and across a range of patients require further exploration and validation.
Wireless Wearables
Studies focusing on wearable devices provide slightly more detailed information regarding participant selection criteria and larger sample sizes. Emerging classes of wireless sensors in the form of soft, flexible, skin-like (“epidermal”) platforms have the potential to redefine practices for monitoring in the NICU, with additional possibilities for use in the home. Recent work at Northwestern University shows that a pair of devices of this type, each of which gently and non-invasively adheres to the fragile skin of a premature neonate, is capable of capturing complete, clinical grade vital signs information without any wires or cables . These devices include distributed flexible electronic components with stretchable interconnects; all embedded in strategic layouts within medical-grade silicone encapsulating structures. The designs optimize for conformal interfaces to the skin at relevant anatomical locations. In pilot studies on patients in NICU settings, these technologies achieved high accuracy and fidelity similar to those of traditional wired monitors. Extensions enabled by additional sensors allow for precise measurements of body sounds, relevant to cardiac and respiratory monitoring, with additional capabilities in tracking gastrointestinal activity . Specifically, high-bandwidth microphones and accelerometers yield seismocardiograms, lung sounds, bowel motility, and even the spectral and temporal features of crying and other forms of vocalization. In this way, these advanced technologies can not only capture vital signs and physiological signals but also an array of important biophysical metrics of health status, beyond those addressed with conventional NICU hardware.
Commercial translation is also gaining momentum. As an example, Sibel Health (Sibel Health, USA) has secured successive FDA 510(k) clearances since 2021 for its ANNE® One sensor platform, a pair of chest and foot patches to continuously monitor heart rate, respiratory rate, skin and core temperatures, oxygen saturation and biomarkers. It is also noteworthy that ANNE One® is currently under investigation in NICU at Montreal Children’s Hospital with the aim of create a wireless NICU. Meanwhile, other emerging technologies, focusing on more specific modalities, include Bambi Belt (Bambi Medical, the Netherlands) and Boppli® (PyrAmes, USA) for monitoring ECG/EMG and blood pressure, respectively.
Collectively, efforts with wireless technologies signal a paradigm shift to transform neonatal care with fewer risks and burdens, and to improve clinical workflow and patient safety. With continued refinement and real-world validation, wireless multimodal sensors are poised to enhance monitoring precision, promote a patient-centric environment, and ultimately give our most vulnerable patients a gentler start to life . With that, a wireless NICU became a much closer to reality than just fiction.
Vaginal cervical cerclage and progesterone are established treatments for prevention of pregnancy loss and prematurity. There is limited data to assess the effect of these treatments in combination. The objective of this study was to investigate the association between progesterone and no progesterone treatment on pregnancy outcomes in women at high risk of preterm birth who had received a vaginal cervical cerclage.
Methods and findings
This is a secondary post-hoc analysis of women recruited to the C-STICH randomised controlled trial, which recruited in 75 obstetric units in the UK between 2015 and 2021. In the C-STICH trial, women with a singleton pregnancy, receiving a vaginal cervical cerclage due to a history of pregnancy loss or premature birth, or if indicated by ultrasound, were randomised to cerclage with braided or monofilament suture, with a primary outcome of pregnancy loss, defined as miscarriage, stillbirth, or neonatal death in the first week of life. In this secondary analysis, the primary outcome was pregnancy loss, defined as miscarriage and perinatal mortality, including any stillbirth or neonatal death in the first week of life. Secondary maternal outcomes included miscarriage and previable neonatal death; stillbirth; gestational age at delivery; preterm pre labour rupture of membranes, and sepsis. Secondary neonatal outcomes included early/late neonatal death and sepsis. For each outcome, regression models were fitted adjusting for prespecified prognostic variables.
From the 2,048 women recruited to C-STICH, 1943 (95%) women had a vaginal cerclage placed and available progesterone data. Of these, 834 (43%) women received progesterone and 1,109 (57%) did not receive progesterone. In women with primary outcome data available, in our predefined analysis pregnancy loss occurred in 49 (5.9%) of 832 women who received progesterone and 91 (8.3%) of 1,103 women who did not receive progesterone (adjusted* risk ratio 0.70 (95% confidence interval (CI) [0.50, 0.99]); adjusted risk difference −0.02 (95% CI [−0.04, −0.001], *adjusted for indication, obstetric history, surgical technique, and maternal age). Further exploratory analysis excluding women who had termination of pregnancy for foetal anomaly demonstrated a nonsignificant reduction in the risk of pregnancy loss. Key limitations of this study include a non-randomized trial design and unknown confounding relating to variation in progesterone use.
Conclusion
In women with a vaginal cervical cerclage and concomitant progesterone there appears to be an association with a reduced risk of pregnancy loss. This combination therapy may be an important opportunity to further reduce the risk of pregnancy loss in this high-risk cohort.
Stronger Together: Building Friendship, Community, and Courage as Neonatal Womb Warriors
Building friendships is one of the most powerful ways we grow as Neonatal Womb Warriors. As preemie survivors, we begin life in a world of uncertainty, strength, and resilience that most people never experience. That journey can sometimes feel isolating—but it doesn’t have to be. When we build friendships with peers, colleagues, and our broader community, we create spaces where our stories are understood, our challenges are validated, and our victories are celebrated. These connections remind us that we are not alone—we are part of a network of survivors, supporters, and advocates who stand together.
Friendship also teaches us how to trust again—trust in others, and trust in ourselves. Many preemie survivors grow up navigating medical complexities, transitions, and moments of vulnerability. Through friendships, we learn how to communicate our needs, listen to others, and build mutual support systems. Whether it’s a colleague who understands the importance of flexibility, a friend who encourages us during a difficult moment, or a mentor who helps us see our potential, these relationships become pillars of strength. They help transform survival into thriving.
Stepping outside of our comfort zone is often where the most meaningful connections begin. It can feel intimidating to introduce yourself, to join a new group, or to share your story—but courage lives in those small steps. For Neonatal Womb Warriors, getting out of our comfort zone is not just about social growth; it’s about reclaiming our voice and our place in the world. Each time we reach out, collaborate, or say yes to a new opportunity, we expand what is possible for ourselves and for others who may be watching and learning from our example.
At its heart, friendship is teamwork. It is showing up for one another, lifting each other up, and building something stronger together than we could alone. As a community of preemie survivors, families, clinicians, and advocates, we are all part of a shared mission: to help every warrior survive, grow, and thrive. When we lean into friendship and community, we build not only support systems, but movements of compassion, advocacy, and hope. And that is the true strength of a Neonatal Womb Warrior.
Belize’s abundance of terrestrial and marine plants and animals and its diversity of ecosystems, including extensive coral reefs, give it a key place in the globally significant Mesoamerican Biological Corridor. It is considered a Central American and Caribbean nation with strong ties to both the American and Caribbean regions.
It has an area of 22,970 square kilometres (8,867 sq mi) and a population of 397,483 (2022). Its mainland is about 290 km (180 mi) long and 110 km (68 mi) wide. It is the least populated and least densely populated country in Central America. Its population growth rate of 1.87% per year (2018 estimate) is the second-highest in the region and one of the highest in the Western Hemisphere. Its capital is Belmopan, and its largest city is the namesake city of Belize City. The country has a diverse society composed of various cultures and languages. It is the only Central American country where English is the official language. Belizean Creole and Spanish are widely spoken, followed by the Mayan languages and Garifuna. Over half the population is multilingual due to the diverse linguistic backgrounds of the population. It is known for its September Celebrations and punta music.
Healthcare in Belize is provided through both public and private healthcare systems. The Ministry of Health (MoH) is the government agency responsible for overseeing the entire health sector and is also the largest provider of public health services in Belize. The MoH offers affordable care to a majority of Belizeans with a strong focus on providing quality healthcare through a range of public programs and institutions.
In contrast to the public health sector, the private health sector provides care to a smaller portion of the population. However, similar to the public sector, private health services are offered at a relatively low cost with a shared emphasis on quality of care and quality improvement.
The Human Rights Measurement Initiative[3] finds that Belize is fulfilling 83.0% of what it should be fulfilling for the right to health based on its level of income. When looking at the right to health with respect to children, Belize achieves 99.1% of what is expected based on its current income. In regards to the right to health amongst the adult population, the country achieves only 86.6% of what is expected based on the nation’s level of income. Belize falls into the “very bad” category when evaluating the right to reproductive health because the nation is fulfilling only 63.2% of what the nation is expected to achieve based on the resources (income) it has available.
Longest continuously running study on preterm birth that has followed research participants for more than 35 years published in JAMAURI College of Nursing Professor Amy D’Agata’s study shows that the effects of preterm birth can linger throughout an individual’s lifetime, necessitating the inclusion of birth history in adult health records.
KINGSTON, R.I. — August 4, 2025 — The stress preterm infants experience at birth can carry on throughout a lifetime and cause negative health impacts later in life, necessitating the routine inclusion of birth history in medical records and the development of clinical guidelines for adults born preterm, the longest continuously running study of individuals born preterm in the United States has shown.
University of Rhode Island College of Nursing Professor Amy D’Agata is continuing the work that began in the 1980s with a group of babies born preterm at Women & Infants Hospital. Involving 215 people born 35 years ago—including a control group of full-term babies, and preterm babies born at 22 to 36 weeks—the study tracks the successes and difficulties preterm babies continue to face into adulthood, and compares them to the group of participants born full term. The project has so far garnered more than $10 million in research grant funding.
D’Agata, who took over as principal researcher after the retirement of Professor Emeritus Mary Sullivan, has published the most recent results in the Journal of the American Medical Association. The published paper focuses physiological and psychological health outcomes that D’Agata and her team of researchers have identified as the study participants approach 40 years old. Those born preterm have shown a higher risk of high blood pressure, high cholesterol, increased abdominal fat, and low bone density. Psychologically, the group tends to internalize problems, often resulting in increased levels of depression and anxiety.
“Preterm birth is not just a neonatal issue. It, in fact, is a lifelong condition,” D’Agata said the study shows. “For individuals who have medical complications early in life, we are now seeing an increased risk of different chronic health issues later in life. We are now realizing that there is a very strong link between what happens to you early in life and later health outcomes.”
The study offers important takeaways for health-care clinicians, who are not always aware a patient was born preterm because birth history is not commonly included in adult medical records. D’Agata’s study is showing the need to include the information, and to develop adult screening guidelines for individuals who have a history of preterm birth. The work is also helping people who have been impacted by preterm birth understand that their birth history should be included in their medical records and should be considered in the context of their overall health.
“In this country, millions of people born preterm have grown into adulthood and are now seeing clinicians across primary care and various specialties, yet providers rarely ask about birth history,” D’Agata said. “We are urging that birth history be included as a standard question on every adult intake form. Health cannot be fully optimized if we overlook such a critical assessment piece.
Understanding an individual’s birth history, alongside growing research identifying increased health risks for those born preterm and the development of targeted clinical guidelines, will advance health equity for survivors of early birth. We believe a paradigm shift is needed in health care that recognizes preterm birth as a chronic condition requiring lifelong monitoring and support.”
While the study’s most recent results were just published in JAMA Network Open in July, D’Agata is already looking toward the next set of findings. Continuing to work with fellow URI professor Justin Parent, D’Agata is examining epigenetic age acceleration among individuals born preterm. Understanding any differences in epigenetic aging that may exist between preterm and full-term born adults may be another approach to understanding long-term health.
In the heart of the Cuban capital, the Dr. Cosme Ordoñez Carceller Teaching Polyclinic stands as a testament to the nation’s unique approach to healthcare: universal, free of charge, accessible, regionalized, community-centered, and deeply rooted in preventive medicine. Unlike the profit-driven models that dominate much of the world, Cuba’s system prioritizes equitable access, public health education, and early intervention.
At the core of this approach is a commitment to health promotion through education, disease prevention through habit management, and the integration of medical care and rehabilitation. By emphasizing proactive healthcare rather than reactive treatment, the system ensures that communities receive continuous, comprehensive support to maintain overall well-being.
During a recent visit to the Dr. Cosme Ordoñez Carceller Teaching Polyclinic in Havana, the staff detailed how the system was developed and how it ensures that no Cuban, regardless of income, is left without medical care.
The structure of Cuba’s healthcare system
Cuba’s National Health System operates as a hierarchical, state-run model designed to ensure seamless coordination of care. At the top, the National Assembly oversees the Ministry of Public Health, which sets national policies and directs specialized health institutes that tackle broader public health concerns.
Below the Ministry, provincial governments, answering directly to the Assembly, oversee provincial health departments, which manage larger hospitals and specialized medical facilities. These provincial bodies, in turn, delegate responsibilities to municipal governments, which run the municipal health departments and smaller hospitals that serve local populations. At the community level, municipal health departments manage Cuba’s extensive polyclinic network, the cornerstone of the country’s healthcare system. These polyclinics not only provide specialized care, diagnostics, and emergency services, but they also coordinate closely with family doctor-and-nurse teams, who serve as the first point of contact for Cuban citizens.
These frontline providers play a crucial role beyond immediate treatment, emphasizing preventive care, home visits, and alternative therapies such as nutrition counseling, acupuncture, and plant-based medicine. Despite supply shortages exacerbated by US sanctions, this integrated, top-down approach ensures that resources are distributed efficiently, maintaining consistent healthcare access nationwide.
Founded in 1974, the Dr. Ordoñez Carceller Polyclinic serves approximately 13,000 residents, offering care in medical specialties such as cardiology, orthopedics, fertility consultations, and genetic testing. The clinic is named after Dr. Cosme Ordoñez Carceller (1927–2019), an epidemiologist and pioneer of Community Medicine, who championed the polyclinic model that emerged in the 1960s and 1970s. He played a key role in training young physicians in comprehensive general medicine and launched innovative programs like the Grandparents’ Circles, a senior care initiative so effective that it was replicated nationwide.
Cuba’s system prioritizes equitable access, public health education, and early intervention. The country’s healthcare approach is rooted in promoting health through education, preventing disease by managing habits, and ensuring comprehensive medical care and rehabilitation. Unlike the fragmented, for-profit US healthcare model, Cuba’s integrated, community-based approach ensures better health outcomes and higher patient satisfaction. At polyclinics like Ordoñez Carceller, primary care is not just about treating illness but about education, prevention, and holistic well-being. This commitment to accessible, people-centered medicine reflects Cuba’s broader philosophy: that healthcare is not a privilege, but a fundamental human right.
Cuba’s healthcare achievements: A global leader in public health
Despite enduring over six decades of economic embargo, Cuba has achieved remarkable public health milestones. The following list highlights key accomplishments of both the Ordoñez Carceller Polyclinic and the Cuban healthcare system as a whole:
AIDS: Cuba identified HIV in 1983 and quickly set up a system to track and treat it. By 2014, it eliminated mother-to-child transmission of HIV and syphilis, a milestone the US has yet to reach.
COVID: Cuba developed two COVID vaccines, kept infections low, and even sent vaccines abroad.
Diabetes: The nation has developed an effective medication that treats diabetic ulcers (skin wounds that result from poor blood sugar control)
Alzheimer’s research: Cuba developed a drug that may help reverse Alzheimer’s effects
Maternal-fetal medicine: 99% of Cuban children are vaccinated, and the country has a lower infant mortality rate than the US
Nutrition: While obesity is not an issue in Cuba, malnutrition is an increasing concern due to shortages caused by the US embargo
Home health Doctors make house calls to care for the elderly and new mothers.
Profit vs. public health: How medical education and healthcare delivery differ in Cuba and the US
The paths to becoming a doctor in Cuba and the United States could not be more different. In the US, medical students take on crippling debt, often exceeding USD 200,000, before ever treating a patient. The pressure to repay loans steers many toward high-paying specialties, leaving primary care and rural communities underserved. The system is structured around financial incentives rather than public need, reinforcing the idea that medicine is a business first, a service second.
Cuba takes the opposite approach. Medical education is fully state-funded, allowing students to focus on patient care instead of profit. Training begins immediately after secondary school, with students placed in community clinics early in their careers. By the time they specialize, they have already served in primary care settings, ensuring that the system produces physicians committed to public health, not private wealth.
A focus on prevention, not just treatment
Cuba’s prevention-first model stands in stark contrast to the reactive nature of US healthcare. While American medicine often prioritizes treatment over lifestyle interventions, Cuban doctors routinely incorporate nutrition, exercise, and disease prevention strategies into care plans. The country’s polyclinic system ensures patients receive consistent, community-based healthcare rather than navigating a fragmented, for-profit system that often leaves them behind.
The US blockade: An unjust barrier to health
The US embargo continues to hinder Cuba’s healthcare system by restricting access to essential medicines, medical equipment, and scientific research. Pharmaceutical and shipping companies, fearing US penalties, avoid business with Cuba—leading to severe shortages of everything from aspirin to cancer treatments.
Even medical journals and online resources are blocked due to US restrictions, forcing Cuban researchers to work under constraints that most Western physicians never encounter.
Yet, rather than succumbing to these barriers, Cuba has turned to self-sufficiency, investing in biotechnology, vaccine development, and herbal medicine research to compensate for limited imports. If freed from economic sanctions, Cuba’s contributions to global healthcare innovation could expand exponentially.
For decades, Cuba has exported medical expertise worldwide, sending doctors to disaster-stricken and underserved regions. These global medical brigades have provided care to millions, particularly in Latin America, Africa, and the Caribbean. Yet, rather than supporting these humanitarian efforts, Washington has sought to dismantle them. In February 2025, the US expanded sanctions on Cuba’s international medical program, further restricting its ability to send doctors abroad. The move reflects a deeper failure to understand Cuba’s model of solidarity-driven healthcare, a stark contrast to the US system, where medicine is often dictated by profit rather than public service.
It is within this profit-driven framework that Cuba’s medical missions are misunderstood, labeled as “forced labor” by those who cannot imagine doctors choosing service over salary. The very idea of healthcare as a human right, rather than a commodity, challenges the US worldview, leading to efforts to discredit and sanction those who practice it differently.
What could be if the embargo were lifted
Cuba’s healthcare system is a model of resilience and innovation, but its full potential remains hindered by decades of US sanctions. If given access to global resources and technology, Cuban researchers could expand medical advancements in infectious diseases, chronic illness treatment, and disaster response. For now, Cuban doctors continue their work—undaunted by external pressures, committed to the principle that healthcare is a right, not a privilege.
People’s Health Dispatch is a fortnightly bulletin published by the People’s Health Movement and Peoples Dispatch. Renée L. Quarterman, MD, FACS, is a surgical breast specialist. She is the director of Delaware Breast Care, a part of US Oncology.
Quality improvement (QI) initiatives have become essential to advancing patient outcomes in the neonatal intensive care unit (NICU), where high acuity and complex care are the norms. NICU nurses are uniquely positioned to find inefficiencies, propose practical solutions, and drive meaningful change. However, despite the growing emphasis on QI in nursing practice, well-intentioned projects fall short due to avoidable missteps in the planning and execution phases.
The following guide can be utilized by NICU nurses to navigate through common pitfalls in QI research and offers evidence-based strategies to overcome them. By focusing on foundational principles and real-world examples, this guide supports nurses in conducting impactful, sustainable QI work that enhances neonatal outcomes and team collaboration.
Common Pitfalls in QI Research
Lack of Clear Problem Definition
A common pitfall in QI efforts is the failure to define the problem thoroughly. Without a precise understanding of the issue, teams may invest critical time and resources into solutions that do not address the root cause.
For instance, a unit may notice an uptick in central line-associated bloodstream infections (CLABSIs) and immediately implement new sterile techniques without investigating the underlying variables. Was the increase related to staffing changes, procedural drift, or equipment issues? Without a clear problem definition, interventions risk being misaligned or ineffective.
Strategy: Use structured problem-identification tools—such as root cause analysis (like the Five Whys) or fishbone diagrams—to uncover deeper system issues. Frame the problem in a way that is specific, data-informed, and agreed upon by stakeholders. A clearly defined problem becomes the foundation for targeted and measurable interventions.
Neglecting Stakeholder Involvement
Successful QI initiatives require input and collaboration across disciplines. A common misstep occurs when projects are developed in isolation, often without input from those who will implement or be affected by the change. This can lead to resistance, logistical challenges, or unintended consequences.
For example, consider a QI team aiming to improve feeding initiation times by adjusting nursing workflows. If respiratory therapists or neonatal physicians are not consulted, the new protocol might inadvertently clash with intubation or stabilization practices, resulting in delays rather than improvements.
Strategy: Identify all stakeholders early in the project, including nurses, physicians, respiratory therapists, pharmacists, and families, when appropriate. Conduct stakeholder analyses and engage representatives in project design and testing phases. Inclusive collaboration fosters ownership, smoother implementation, and more sustainable outcomes (Institute for Healthcare Improvement, n.d.).
Poorly Defined Metrics
Without clearly defined, relevant, and measurable outcomes, a QI initiative’s impact is difficult to assess. Broad or vague goals such as “improve thermoregulation” fail to provide direction or an evaluation method.
Strategy: Use SMART goals—Specific, Measurable, Achievable, Relevant, and Time-bound—to guide metric development. For instance, instead of aiming to “reduce hypothermia,” a SMART goal might be: “Increase the percentage of newborns with normothermic admission temperatures (36.5°C–37.5°C) from 65% to 90% over six months.” Tools and resources are available to learn how to develop clear metrics, help track progress, guide adjustments, and communicate results to the team and leadership (Agency for Healthcare Research and Quality, 2020).
Inadequate Data Collection Planning
Even well-designed projects can falter without a strong plan for data collection. Inconsistent, incomplete, or biased data limit the ability to draw valid conclusions and make informed decisions.
Strategy: Design a standardized data collection process before the intervention begins. Identify what data are needed, who will collect data, how often, and how data will be stored and analyzed. Use validated tools where possible and use the electronic health record (EHR) system to reduce manual workload and increase reliability. Pilot test the data collection process to identify issues before scaling up.
Failure to Pilot Interventions
Another frequent misstep is implementing large-scale changes without first evaluating them in a controlled way. Skipping the pilot phase can lead to disruptions in care, staff confusion, or overlooked safety concerns.
Strategy: Use Plan-Do-Study-Act (PDSA) cycles to test changes on a small scale. For instance, a new bedside handoff tool can be trialed with one team for over a week before expanding unit wide. Piloting helps refine interventions, identify barriers early, and build staff confidence.
Lack of Sustainability Planning
Often, improvement is easier to achieve than sustain. QI initiatives can experience initial success but not maintain gains over time due to a lack of follow-up, ownership, or integration into routine practice.
Strategy: Plan for sustainability from the outset. Embed new practices into policies, electronic systems, and training programs. Assign champions to monitor compliance, provide feedback, and adapt as needed. Ongoing measurement and leadership support are critical to prevent regression.
Not Sharing or Publishing Results
When results are not shared beyond the unit, valuable insights and lessons are lost. This limits the potential for broader impact and professional growth.
Strategy: Disseminate findings through presentations, newsletters, or professional journals. Even small projects can inspire similar efforts elsewhere and contribute to the collective advancement of neonatal care. Sharing also strengthens the culture of learning and improvement.
Better QI Creates Lasting Change
Quality improvement is a powerful tool NICU nurses use to enhance care and outcomes. By avoiding common pitfalls—such as unclear problem definitions, poor metric planning, and lack of sustainability—nurses can lead effective and lasting change. Through structured planning, collaborative engagement, and thoughtful execution, every QI effort becomes an opportunity for growth and better care for our most vulnerable patients. (Institute for Healthcare Improvement, n.d.).
Ghosting is one of those terms that seem out of place in medicine, borrowed from social media and dating culture. However, the phenomenon itself is alive and well in our clinical ecosystems. In fact, medicine may be one of the most fertile environments for it. How else can someone remain deeply involved, wholly committed, ever-present in the work, yet increasingly pushed to the side, rendered peripheral to decisions they once shaped?
In the professional world, ghosting is less dramatic and more insidious. It is not someone vanishing; it is colleagues stepping around them. It is conversations that slip behind closed doors. It is the rise of intermediaries and buffers. It is the subtle but unmistakable shift from direct speech to third-person references. It is the choice to go around rather than through.
It is ostracizing, but with a veneer of civility. It is quiet exclusion disguised as efficiency.
And yes, it does not feel very good. For many, the experience intensifies with seniority. The more seasoned someone becomes, the more they know, the more institutional memory they carry, the more perspective they bring; the easier it becomes for others to rationalize keeping them out of the loop. People frame it as respect, as courtesy, as a desire not to “burden” them. Nevertheless, the line between courtesy and dismissal is thin and often crossed.
Technology, ironically, amplifies the problem. Zoom, Teams, and the creeping normalization of AI presence create new pathways for invisibility. What once required the discomfort of face-to-face avoidance now happens silently. Disengagement becomes frictionless. They can be physically present on a screen and still be utterly alone in the room. When they realize they are the only one who showed up in person, while everyone else has delegated their attendance to an AI proxy, they feel the ghostliness in full.
Ghosting rarely begins with an attack. It begins with a narrative.
“They’re too busy for this.”
“They have so much on their plate already.”
“They’re so senior; we shouldn’t bother them with this.”
“They don’t need feedback—they’re above the evaluators.”
What begins as deference quietly morphs into distance. And distance, unchecked, hardens into exclusion. Soon, the storyline shifts:
“They’re not involved.”
“They didn’t attend the last meeting.”
“They never weigh in anymore.”
What remains unsaid and often unnoticed is that no one invited them, no one asked for their opinion, and no one created space for them to be part of the process.
Decisions move forward. Processes evolve. Incentives and priorities shift. Meanwhile, the ghosted clinician continues to do their work, unaware that the landscape is changing around them in ways that diminish their role, complicate their tasks, or diminish their influence. When they finally recognize that something fundamental has shifted, it is often too late to re-enter the conversation.
What does this feel like? It feels exactly like being a ghost.
The film The Sixth Sense offers a powerful metaphor. (Spoiler Alert) Bruce Willis’s character, after suffering a fatal gunshot wound, continues living as though nothing has changed. He goes to work, he engages in therapy, and he attempts to connect with his wife. However, something is off. People drift away. His wife is distant. Rooms feel colder. It is only through his sessions with a child who can “see dead people” that he finally confronts the truth: he is no longer part of the living world, no longer part of the relationships he believes himself to be nurturing.
Professionally, the comparison is not perfect, but it is evocative. In medicine, the “ghosts” have not died. They walk our halls. They mentor trainees. They contribute to scholarship. They carry decades of clinical experience. They built the foundations upon which our teams now stand.
Nevertheless, they are treated as if they no longer inhabit the same professional world as everyone else.
Ghosting in medicine is not just a social slight; it is a cultural wound. It erodes respect. It weakens teams. It destroys continuity. It discards institutional memory. It creates unnecessary rifts between generations of clinicians. It deprives trainees of mentorship. It can turn accomplished physicians into isolated figures who continue to serve, but without the acknowledgment or inclusion that sustains service.
Most dangerously, ghosting perpetuates the illusion that this is normal. That it is natural. That it is simply the denouement of a career.
But it does not have to be.
In an era where burnout is widespread, where talent is scarce, and where the wisdom of experience is more valuable than ever, ghosting is a luxury medicine cannot afford. Inclusion is not just good manners: it is good practice. It strengthens teams, enhances decision-making, and honors the very people who paved the way.
So the next time you see a colleague who seems peripheral, someone once central, now slowly fading from the edges of the conversation—pause before stepping around them. Invite them in. Ask their opinion. Keep them part of the fabric of the work. The difference between belonging and ghosthood may hinge on the smallest acts of acknowledgment, the simplest acts of inclusion. Because the ghost you see before you today is not a relic to be ignored; they are a reflection, a warning, of what any one of us might become.
At well-baby visits, your baby’s provider checks your baby’s health and development and gives your baby vaccinations to protect them from diseases.
If your baby has a medical condition, they may need ongoing care from different healthcare providers.
If you think your baby is sick, call their provider. If you think it’s an emergency, call 911.
If your baby needs medicine or medical equipment at home, learn how to give or use it correctly before your baby leaves the NICU.
When does your baby need to see their healthcare provider?
Your baby will get several checkups (well-baby visits) with their provider during their first year. At each visit, talk to their provider to make sure your baby’s developing in a healthy way. Are they rolling over, sitting up, crawling, and walking when they should? These skills are called developmental milestones. You may need to remind the provider that your baby spent time in the neonatal intensive care unit (NICU), because this may affect when they reach the milestones.
Take your baby’s medical file to your first visit with your baby’s provider. This file includes their discharge summary and other information from the hospital. The provider needs to know what happened during and after your baby’s birth. Hospital staff may send the summary directly to the provider.
If your baby has a medical condition, such as a birth defect, they may need ongoing care from different healthcare providers. Find a way to keep track of your baby’s medical appointments. This may be on a calendar in your kitchen or on your phone with an alert to remind you. Decide if it’s easier to schedule a few appointments on the same day or spread them out over different days.
Ask your providers to keep your baby’s main provider up to date about all visits and treatments. This helps make sure that all members of your baby’s healthcare team have the same information.
Keep your own record of any checkups, tests, and treatments your baby has had. When your doctor makes a change to your baby’s care or medication, make sure this is also shared with your baby’s in-home nursing care agency and equipment company if you use these services.
What should you do if your baby gets sick?
All babies get sick from time to time. But babies who were in the NICU are more likely than other babies to get infections. Watch for signs that your baby may be sick so you can get medical help right away. You should call your baby’s healthcare provider if your baby:
Looks blue around the nose, lips, or on the skin, or is paler than usual
Refuses to eat or doesn’t eat enough
Throws up (which is more serious than spitting up or reflux)
Has less than five wet diapers in a 24-hour period, or has diarrhea for more than a day
Has a large or hard belly that they have not had before
Has a temperature higher than 100.4 F or lower than 97 F (using a rectal thermometer)
Has apnea or trouble breathing. Apnea is when the baby stops breathing for 15 seconds or more.
You know your baby best. If you think something is wrong, call their provider, call 911, or take your baby to the emergency room.
How do vaccinations help protect your baby?
All babies, including those who spend time in the NICU, need vaccinations to help protect them from serious diseases. Some babies start getting these shots while they’re in the NICU. Check with your baby’s provider about when they need their vaccinations. Keep a record of your baby’s vaccinations in your medical file for them.
If you have other children, they need their vaccinations, too. This helps keep them from passing infections to the baby. During flu season, everyone in the family, including parents, should get a flu shot. Any adult who may have contact with your baby also needs a Tdap vaccination. This vaccination helps protect against tetanus, diphtheria, and pertussis (whooping cough). If you didn’t receive your Tdap vaccine during pregnancy, you can get it after you’ve given birth. To create a safe space for your baby, it is important for everyone who will be in contact with your baby to receive their vaccinations.
How can you protect your baby from respiratory syncytial virus (RSV)?
RSV is a common virus. It affects almost all children before they reach age 2. Most of the time, it causes a slight cold. But for preterm babies (born before 37 weeks of pregnancy), this virus can be more serious. Babies born preterm or who have heart or lung problems may benefit from a medicine to keep them from getting RSV. Ask your baby’s healthcare provider if your baby got this medicine in the NICU or if they should get it now that they’re at home.
What do you need to know about giving your baby medicine?
Some babies go home from the NICU still taking medicines. Learn how to give your baby their medicine before they leave the hospital. Write down all the directions. If you have questions or are worried about giving your baby medicine, tell the nurse or other NICU staff. They can show you exactly what to do so you feel comfortable and confident about giving your baby medicine.
When giving your baby medicine, make sure you know:
Where you can get the prescription filled (at a grocery store, drug store, or pharmacy). A prescription is an order for medicine given by a healthcare provider.
How much medicine to give, how often to give it, and when to stop giving it
If you can give it before, during, or after feedings
If the medicine needs to be refrigerated, prepared, or mixed
What to do if you miss a dose
If your baby needs more than one medicine, if you can give them together at the same time
You also need to know:
What position your baby should be in to take the medicine
What to do if your baby spits up or vomits the medicine
If there are side effects from the medicine and what to do if your baby has them
To track your baby’s different medicines and when to give them, use a chart. Ask the nurse to help you make the chart.
How can you manage your baby’s medical equipment at home?
If your baby has medical equipment at home, this can feel like a lot to manage. Staying organized and planning ahead can help. Keep a list of your baby’s equipment and medical supplies, including order numbers, size, and quantity. The equipment company can give you a checklist. Be sure to re-order supplies with enough time, as shipments can sometimes be delayed. Always be prepared when you leave the house, make sure you have your baby’s supplies even when you’re just going to the park.
If the equipment uses electricity:
Share information about your baby’s medical condition with your local fire department and emergency or first responders so they know what to expect in case they’re called to your home for an emergency. Invite them to come to your home to meet you and your baby.
Contact your utility companies to let them know your baby’s healthcare needs. They may have a priority list for repairing power outages or plowing snow.
Make a plan for if the power goes out. Have back-up batteries and know how long they will last.
Anxiety is another word for feeling worried or scared. It’s normal for children and teens to feel anxious sometimes, like before a big test at school or talking in front of a group of people. But if your child’s anxiety gets in the way of normal activities, such as sleeping alone at night, playing outside or going to school, they may need extra support.
The good news is that there are things you can do to help prevent your child from feeling anxious and help them handle worries when they happen. Talk with your pediatrician to discuss strategies and tips that can help.
What are some common signs of anxiety in children?
If your child is feeling anxious, they may not be able to tell you. Your child may feel bad or sick without knowing why, or you may notice they seem restless or tired.
Feeling as if their heart is racing
Sweating or blushing
Shaking or feeling sick to their stomach
Feeling very cold or hot
Trouble paying attention or sitting still
Touching the crotch area (for young boys)
How can I help my child manage anxiety at home?
These tips are helpful for all children, but they can be especially helpful for children with anxiety. Parenting is a busy job, so use your judgment about which tips make the most sense for your family.
Connect with your child
Set aside one-on-one time every day without TV or other media. Even just 10 minutes each day can make a big difference. Try gardening or taking care of houseplants, drawing or going for a bike ride.
Praise your child and make them feel good about themselves. For example, “You did a great job on that homework assignment!” or “Thank you for helping me with the laundry. I’m so lucky to have your help.”
Find out what’s worrying your child, because stress can make them feel anxious. Things such as being bullied at school, divorce, or a death in the family can make a child feel anxious. Your child may need extra help to handle issues such as these.
Help your child learn to manage fears
When your child is calm, start a conversation about things they can do to manage fears and worries when they happen. For example, let them know that they can
Practice deep breathing and muscle relaxation.
Use positive self-talk (for example, “I can try this” instead of “I can’t do this”).
Think of a safe place, such as their bedroom or favorite place outdoors.
Gradually facing fears. Consider gradually exposing your child to feared objects or activities.
Praise and reward brave behavior: the goal is to cope, not avoid.
Get active! Encourage your child to be active for at least an hour every day. This activity can include playing outside, joining a sports team or an activity at the YMCA, biking or walking to school, or dancing at home to favorite music.
Eat healthy. Eat healthy meals every day, including fruits and vegetables, whole grains, and protein foods. Remember to eat breakfast!
Get plenty of sleep. School-aged children need 9 to 12 hours of sleep every night, and teens need 8 to 10 hours.
Build a family media planto set healthy guidelines around entertainment screen time. Avoid scary or violent TV shows, video games, and movies.
Set up family routines. Follow a regular schedule for playtime, mealtime, and bedtime. Knowing what to expect can help your child feel safe and secure.
How can I help my child manage school anxiety?
Children may find it hard to focus on or even go to school when they’re feeling worried. If your child is having trouble in school, try these ways to help.
Gently but firmly tell your child why it’s important to go to school.
Talk with your child’s teachers and the guidance counselor about what to do if your child asks to go home from school early.
If you think your child may be upset by family stress or pressure to do well in school, let them know they are doing a good job and you’re proud of them.
Help your child set realistic goals for school. If they set goals that are too hard to meet, they may feel worse about themselves.
Remind your child that they can take steps to control their worries. For example, they can think about what to do ahead of time to handle a stressful situation.
Reward your child’s brave behaviors at school. Spending time doing fun activities with a parent is a very powerful reward.
Remember, you know your child best.
Whether it’s at school or the doctor’s office, you are your child’s biggest advocate. Don’t hesitate to speak up on behalf of your child.
When do I need to go back to the doctor?
If your child’s anxiety doesn’t go away or gets worse, get back in touch with the doctor. You and the doctor can make a plan to try new approaches or strategies with your child.
It’s especially important to talk with your child’s doctor if:
Your child starts to experience other behavior problems, such as shyness.
Something scary happens in your child’s life that may make their anxiety worse, such as an injury or death in the family.
You suspect your child’s anxiety is affecting another medical condition (for example, if your child’s asthma gets worse with anxiety).
The doctor can also help you decide whether visiting a specialist may help. For example, a type of therapy called cognitive behavioral therapy can be helpful for children with anxiety.
Make time to care for yourself, too.
Parenting can be stressful. If you’re feeling overwhelmed, don’t be afraid to ask for support from family, close friends, social services, or your faith community. Children pick up on the stress and worries of adults, so getting support for yourself can help your child too.
The neonatal intensive care unit (NICU) is a special unit in the hospital for babies born preterm, very early, or who have some other serious medical condition. Most babies born very early will need special care after birth. This is done by or under the supervision of a neonatologist, a doctor with special training in the care and problems of newborns.
This article discusses the consultants and support staff who may be involved in the care of your infant depending on your infant’s specific medical needs.
Information
AUDIOLOGIST
An audiologist is trained to test a baby’s hearing and provide follow-up care to those with hearing problems. Most newborns have their hearing screened before leaving the hospital. Your health care providers will determine which hearing test is best. Hearing tests may also be done after leaving the hospital.
CARDIOLOGIST
A cardiologist is a doctor that has special training in the diagnosis and treatment of heart and blood vessel disease. Pediatric cardiologists are trained to deal with newborn heart problems. The cardiologist may examine the baby, order tests, and read test results. Tests to diagnose heart conditions may include:
If the structure of the heart is not normal due to a birth defect, a cardiologist might work with a cardiovascular surgeon to perform surgery on the heart.
CARDIOVASCULAR SURGEON
A cardiovascular (heart) surgeon is a doctor who has special training in doing surgery to correct or treat defects of the heart. Pediatric cardiovascular surgeons are trained to deal with newborn heart problems.
Sometimes, surgery can correct a heart problem. Other times, complete correction is not possible and surgery is done just to make the heart work as well as possible. The surgeon will work closely with the cardiologist to care for the baby before and after surgery.
DERMATOLOGIST
A dermatologist is a doctor who has special training in diseases and conditions of the skin, hair, and nails. Such a doctor might be asked to look at a rash or skin lesion on a baby in the hospital. In some cases, the dermatologist might take a sample of the skin, called a biopsy. The dermatologist might also work with the pathologist to read the biopsy results.
DEVELOPMENTAL PEDIATRICIAN
A developmental pediatrician is a doctor who has been specially trained to diagnose and care for infants who have trouble doing what other children of their age can do. This type of doctor often evaluates babies who have already gone home from the NICU and will order or perform developmental tests. The doctor can also help you find resources near your home that provide therapies to help infants and children in meeting development milestones. Developmental pediatricians work closely with nurse practitioners, occupational therapists, physical therapists, and sometimes neurologists.
DIETITIAN
A dietitian has special training in nutritional support (feeding). This type of provider may also specialize in pediatric (children’s) nutritional care. Dietitians help determine if your baby is getting enough nutrients, and may recommend some choices of nutrition that can be given through the blood or a feeding tube.
ENDOCRINOLOGIST
A pediatric endocrinologist is a doctor with special training in the diagnosis and treatment of infants with hormone problems. Endocrinologists might be asked to see babies who have problems with the level of salt or sugar in the body, or who have problems with the development of certain glands and sexual organs.
GASTROENTEROLOGIST
A pediatric gastroenterologist is a doctor with special training in the diagnosis and treatment of infants with problems of the digestive system (stomach and intestines) and liver. This type of doctor might be asked to see a baby who has digestive or liver problems. Tests, such as x-rays, liver function tests, or abdominal ultrasounds, might be done.
GENETICIST
A geneticist is a doctor with special training in the diagnosis and treatment of infants with congenital (inherited) conditions, including chromosomal issues or syndromes. Tests, such as chromosome analysis, metabolic studies, and ultrasounds, may be done.
HEMATOLOGIST-ONCOLOGIST
A pediatric hematologist-oncologist is a doctor with special training in the diagnosis and treatment of children with blood disorders and types of cancer. This type of doctor might be asked to see a baby for bleeding problems due to low platelets or other clotting factors. Tests, such as a complete blood count (CBC) or clotting studies, might be ordered.
INFECTIOUS DISEASE SPECIALIST
An infectious disease specialist is a doctor with special training in the diagnosis and treatment of infections. They might be asked to see a baby that develops unusual or serious infections. Infections in babies can include blood infections or infections of the brain and spinal cord.
MATERNAL-FETAL MEDICINE SPECIALIST
A maternal-fetal medicine doctor (perinatologist) is an obstetrician with special training in the care of high-risk pregnant women. High-risk means there is an increased chance for problems. This type of doctor can care for women who have premature labor, multiple gestations (twins or more), high blood pressure, or diabetes.
NEONATAL NURSE PRACTITIONER (NNP)
Neonatal nurse practitioners (NNP) are advanced practice nurses with extra experience in the care of newborn infants in addition to completing master’s or doctoral level educational programs. The NNP works along with a neonatologist to diagnose and treat health problems in babies in the NICU. The NNP also performs procedures to help diagnose and manage certain conditions.
NEPHROLOGIST
A pediatric nephrologist is a doctor with special training in diagnosing and treating children who have problems with the kidneys and urinary system. This type of doctor might be asked to see a baby who has problems in the development of the kidneys or to help care for a baby whose kidneys do not work properly. If a baby needs kidney surgery, the nephrologist will work with a surgeon or urologist
.NEUROLOGIST
A pediatric neurologist is a doctor with special training in the diagnosis and treatment of children with disorders of the brain, nerves, and muscles. This type of doctor might be asked to see a baby who has seizures or bleeding in the brain. If the infant needs surgery for a problem in the brain or spinal cord, the neurologist might work with a neurosurgeon.
NEUROSURGEON
A pediatric neurosurgeon is a doctor trained as a surgeon who operates on children’s brains and spinal cords. This type of doctor might be asked to see a baby who has problems, such as spina bifida, skull fracture, or hydrocephalus.
OBSTETRICIAN
An obstetrician is a doctor with special training in taking care of pregnant women. This type of doctor might also assist women who are trying to get pregnant and follow women with medical conditions, such as diabetes or decreased fetal growth.
OPHTHALMOLOGIST
A pediatric ophthalmologist is a doctor with special training in diagnosing and treating eye problems in children. This type of doctor might be asked to see a baby who has birth defects of the eye.
An ophthalmologist will look at the inside of the baby’s eye to diagnose retinopathy of prematurity. In some cases, this type of doctor might perform laser or other corrective surgery on the eyes.
ORTHOPEDIC SURGEON
A pediatric orthopedic surgeon is a doctor with special training in the diagnosis and treatment of children who have conditions involving their bones. This type of doctor might be asked to see a baby who has birth defects of the arms or legs, hip dislocation (dysplasia), or fractures of the bones. To see the bones, orthopedic surgeons might order ultrasounds or x-rays. If needed, they can perform surgery or place casts.
OSTOMY NURSE
An ostomy nurse is a nurse with special training in the care of skin wounds and openings in the belly area through which the end of the intestine or the collecting system of the kidney stick out. Such an opening is called an ostomy. Ostomies are the result of surgery needed to treat many intestinal problems, such as necrotizing enterocolitis. In some cases, ostomy nurses are consulted to help care for complicated wounds.
OTOLARYNGOLOGIST/EAR NOSE THROAT (ENT) SPECIALIST
A pediatric otolaryngologist is also called a pediatric ear, nose, and throat (ENT) specialist. This is a doctor with special training in the diagnosis and treatment of children with problems with the ear, nose, throat, and airways. This type of doctor might be asked to see a baby who has problems with breathing or a blockage of the nose.
Occupational and physical therapists (OT/PT) are professionals with advanced training in working with infants with developmental needs. This work includes neurobehavioral assessments (postural tone, reflexes, movement patterns, and responses to handling). In addition, the OT/PT professionals will help determine a baby’s nipple-feeding readiness and oral-motor skills. Speech therapists will also help with feeding skills in some centers. These types of providers might also be asked to provide family education and support.
PATHOLOGIST
A pathologist is a doctor with special training in lab testing and examination of body tissues. They supervise the lab where many medical tests are performed. They also examine tissues under the microscope that are obtained during a surgery or an autopsy.
PEDIATRICIAN
A pediatrician is a doctor with special training in the care of infants and children. This type of doctor might be asked to see a baby in the NICU, but is usually the primary care provider for a healthy newborn. A pediatrician also provides primary care for most babies after they leave the NICU.
PHLEBOTOMIST
A phlebotomist is a specially trained professional who takes your blood. This type of provider may take the blood from a vein or a baby’s heel.
PULMONOLOGIST
A pediatric pulmonologist is a doctor with special training in diagnosing and treating children with respiratory (breathing) conditions. Even though the neonatologist cares for many infants with respiratory problems, the pulmonologist might be asked to see or to help care for babies who have unusual conditions of the lung.
RADIOLOGIST
A radiologist is a doctor with special training in obtaining and reading x-rays and other imaging tests, such as barium enemas and ultrasounds. Pediatric radiologists have extra training in imaging for children.
Social workers are professionals with special education and training to determine the psychosocial, emotional, and financial needs of families. They help families find and coordinate resources in the hospital and community that will help to meet their needs. Social workers also help with discharge planning.
UROLOGIST
A pediatric urologist is a doctor with special training in diagnosing and treating conditions involving the urinary system in children. This type of doctor might be asked to see a baby with conditions such as hydronephrosis or hypospadias. With some conditions, they will work closely with a nephrologist.
X-RAY TECHNICIAN
An x-ray technician is trained in taking x-rays. X-rays can be of the chest, stomach, or pelvis. Sometimes, solutions are used to make body parts easier to see, as with barium enemas. X-rays of bones are also commonly performed on babies for a variety of reasons.
Pediatric surgical conditions are a significant source of morbidity and mortality in low- and middle-income countries (LMICs), where children with surgically treatable conditions lack access to care owing to an insufficient number of pediatric surgeons, poor and limited training, and financial barriers. There is a growing shift from charitable missions to capacity-strengthening projects, which strengthen the skills and resources of communities. The objective of this study was to synthesize the literature to identify capacity-strengthening projects, their methods and outcomes, and their limitations and barriers.
METHODS
MEDLINE, EMBASE, Cochrane, and Web of Science were searched until May 5, 2023. Eligibility criteria were as follows: (1) inclusion of pediatric surgery patients; (2) designation as capacity-strengthening interventions; (3) outcomes of improved access defined through Lancet Commission on Global Surgery Indicators; and (4) designation as an LMIC defined by the World Bank. Two independent reviewers conducted screening and extraction.
RESULTS
A total of 80 studies met inclusion criteria. Interventions were implemented in 69 LMICs and used 19 different methods of capacity strengthening. Common capacity-strengthening methods included the following: international surgical visits, training programs, partnerships, mobile clinics and camps, infrastructure enhancements, and telemedicine. Common methods used included the following: training of local providers, continuous contact between both countries after the visit was completed, improved access for rural families, and economic support for low-income families. A total of 1 357 077 pediatric surgeries were performed through these interventions. Limitations included the fact that only peer-reviewed studies were included. Included studies were mainly case series or small observational studies with qualitative data.
CONCLUSIONS
This review identifies methods to implement capacity-strengthening interventions in LMICs, including their successes and barriers. Future research should report ethical concerns and quantitative outcomes to determine effectiveness.
Neonates and infants are commonly referred to as “therapeutic orphans” due to the overall scarcity of therapeutic interventions that have been developed and tailored to their needs and specific characteristics. This is well known by care providers and researchers active in this field, but is perhaps less on the radar of authorities, funding bodies or the broader public. There is significant health inequity when comparing newborns to other age populations in terms of specific drug and device development and therapeutics. In addition there are health inequities in the provision of neonatal care globally which require special attention in terms of improvement.
Bronchopulmonary dysplasia, neonatal seizures, poor growth, necrotizing enterocolitis (NEC) and short bowel, hypoxic-ischemic encephalopathy, retinopathy of prematurity (ROP), neonatal infections and sepsis hereby serve as a non-exhaustive list of “orphan conditions” in need of more equity, through adequately and urgently funded research and improvement.
The good news is that there have been increased efforts, in recent years, by researchers and regulatory bodies to focus on the provision of drugs, devices, and treatment modalities tailored for neonatal use, while further advocacy remains an obvious need . This brings perspective and explains the initiative taken to organize a focused research topic on what is on the horizon as well as recent advances.
Overview of the topics covered
We targeted emerging or new aspects related to monitoring, diagnostics and therapeutics in neonatal care for the current research topic. Fortunately, this research topic was perceived as very relevant by the research community, as 135 authors expressed their interest as contributors, resulting in 20 accepted papers. This serves as a signal of the importance to continue to work on this topic.
Post-hoc, and in a somewhat arbitrary way (because of overlap in these subcategories) these papers were subdivided by the editors into different subcategories, with focus on (1, 5 papers) perinatal biomarkers in blood and urine and how these relate to or predict outcomes, (2, 6 papers) adaptations of existing and newly emerging equipment in neonatal units, (3, 3 papers) needed advances in pharmacotherapy, (4, 3 papers) machine learning or deep learning applications in neonatal care, and finally, (5, 3 papers) underreported aspects of contemporary NICU care, with a focus on the holistic nature of care for the infant and the family.
Perinatal biomarkers in blood and urine and how these relate to or predict outcomes
Two papers focused on biomarkers related to gestational diabetes, with reflections and data on maternal and neonatal outcomes. Postnatal maternal levels of glycated albumin and hemoglobin A1c in mothers of large-for-gestational-age (LGA) informed us of the relevance of accurate diagnosis during pregnancy. This is because postpartum women without diagnosis during pregnancy had higher glycated albumin values, associated with LGA and associated complications (Železnik et al.). Interestingly and related to this paper, Yin et al. reported on a untargeted metabolomics study in women with gestational diabetes, with the recommendation of a maternal serum metabolite panel to forecast neonatal adverse outcomes (hypoglycemia and macrosomia) (Yin et al.).
Other papers focused on the use of vitamin D, acid-base and biomarkers associated with fetal growth restriction with impaired neurodevelopmental outcome. In a cohort of 217 preterm neonates, a multivariate regression analysis identified antenatal steroids as protective, and lower birth weight, duration of ventilation, sepsis and the serum 25-(OH)D vitamin as risk factors to develop ROP (Yin et al.). Musco et al. reported on a systematic review on blood biomarkers indicating risks of adverse neurodevelopmental outcome in fetal growth restricted infants (Musco et al.). While the authors retrieved some data on neuron specific enolase and S100B, the overall conclusions reflect a call for further research. Finally, an association between lactate levels in umbilical cord blood and cerebral oxygenation in preterm neonates was studied as a secondary outcome analysis (Dusleag et al.). In non-asphyxiated preterm neonates with respiratory support, lactate levels were negatively associated with cerebral and arterial oxygenation. In term neonates without respiratory support, no associations were observed.
Adaptations of existing and newly emerging equipment in our units
In a review on emerging innovations in neonatal monitoring, Krbec et al. concluded that there is an urgent, still unmet need to develop wireless, non- or minimal-contact, non-adhesive technology, capable to integrate multiple signals in a single platform, tailored to neonates (Krbec et al.). Related to this call of action, Svoboda et al. reported on their pilot experience with contactless assessment of heart rate, applying imaging photoplethysmography (Svoboda et al.). Rectal and axillary temperature monitoring on admission were compared in a cohort of preterm (n = 80, <32 weeks gestational age) by Halabi et al., reporting that rectal measurement was likely more reliable in the event of hypothermia (Halabi et al.). Ultrasound-guided measurement of anterior cerebral artery resistive index in the first week of life in 739 preterm neonates (<35 weeks) was not associated with subsequent co-morbidities on admission or during neonatal stay (asphyxia, sepsis, NEC) (Singh Gill et al.). A case series of neurally adjusted ventilatory assist to rescue pulmonary interstitial emphysema in 5 extremely low birth weight infants illustrated the potential value of this ventilatory equipment and strategy and need for further study (Chen et al.). Finally, van Rens et al. compared a conventional to a modified Seldinger technique (a dedicated micro-insertion kit) for peripherally inserted central catheter (PICC) placement, illustrating the relevance of developing “low risk, high benefit” type of medical devices, adapted to the specific needs of neonates (van Rens et al.).
Advances needed in pharmacotherapy
The currently available medicines and dosing regimens in neonatal care are limited and there is an urgent need for improvement in this domain. This was illustrated by articles on sepsis, septic shock and steroids. Inequity in provision of neonatal care across the globe ought to be a major focus of improvement. Gezahegn et al. described the outcome in neonates admitted with sepsis in Harar (Ethiopia). Low white blood cell count, desaturation, preterm birth, absence of prenatal maternal care, and chorioamnionitis were important risk factors for sepsis-related mortality (Gezahegn et al.). Addressing these prognostic factors hold the promise to act as levelers to improve outcomes. A pilot study compared noradrenaline and adrenaline as first line vasopressor for fluid-refractory sepsis shock (Garegrat et al.). Both interventions were comparable to resolve the septic shock, while the overall mortality (13/42, 30%) remained significant, highlighting the need for better diagnostic and therapeutic options. Finally, in a systematic review, outcome of postnatal systemic corticosteroids (hydrocortisone to dexamethasone) were compared as reported in randomized controlled trials (Boscarino et al.). The authors concluded that dexamethasone appeared to be somewhat more effective than hydrocortisone in improving respiratory outcomes, but with inconclusive but relevant concerns on the uncertainties on long-term neurodevelopmental outcome, again highlighting the need for better therapies for prevention and management of chronic lung disease of prematurity.
Machine learning or deep learning applications in neonatal care
Artificial intelligence is a rapidly advancing area with fast evolving clinical applications in healthcare, including in the NICU (6). It is no surprise that the current research topic also contains papers illustrating its relevance to improve our practices and outcomes. Two papers hereby focused on NEC, and a 3rd paper on prediction of significant patent ductus arteriosus (PDA). In a mini-review, Cuna et al. reports on the various pathophysiological processes underlying NEC endotypes, and how artificial intelligence holds the promise to influence further understanding and management (Cuna et al.). An approach to enhance surgical decision making in NEC is illustrated by Wu et al. Based on x-rays from 263 neonates diagnosed with NEC (94 surgical cases), a binary diagnostic tool was trained and validated, with Resnet18 as approach applied (Wu et al.). For PDA, an ultrasound-based assessment of ductus arteriosus intimal thickness in the first 24 h after birth was applied in 105 preterm neonates. A prediction model for closure on day 7 included birth weight, mechanical ventilation, left ventricular end-diastolic diameter, and PDA intimal thickness (Hu et al.). Such models can be considered to better target future study, integrated in a precision medicine approach. Use of AI and big data have the potential to significantly improve our understanding of neonatal conditions and also support neonatal researchers in asking better research questions.
Underreported aspects of contemporary NICU care, holistic care
As part of this research topic, we also accepted papers reporting on the use of music on pain management, on multisensory stimulation to improve maternal milk volume production, and parents’ experiences related to congenital cardiac surgery. All these 3 papers reflect the need for holistic care and to further integrate the perspectives of (former) patients and parents into neonatal practice.
In a systematic review, Ou et al. demonstrated that music is an effective intervention to relief procedural pain (e.g., Premature Infant Pain Profile score) in preterm neonates, as it reduced some markers of stress, and improved blood oxygen saturation (Ou et al.). Multisensory stimulation (audiovisual, or audiovisual + olfactory) compared to a control setting improved maternal milk volume production, with evidence of positive effects of both interventions, even more pronounced if both interventions are combined (Cuya et al.). Finally, a quantitative analysis of parent’s experiences with neonates admitted to NICU with a congenital heart disease reinformed us on the importance of actively focusing on parental experiences of care (Catapano et al.).
From advances in neonatal care to implementation In our opinion, this research topic nicely illustrates the diversity in ongoing clinical research activities, that all hold the promise to improve our clinical management practices, with the overarching aim to improve neonatal outcomes. There is an urgent need to focus on the current health inequities in the provision of care to neonates (3). The trend towards a “neuro” dedicated NICU care is an illustration on how relevant progress may occur. This progress is based on improved neuromonitoring techniques (7), improved management and precision medicine in the field of anti-epileptic drugs (8), and integrating families as partners in neonatal neuro-critical care and similar improvement programs (9). The good news is that we are already experiencing a shift in the right direction. The neonatal community and all other relevant stakeholders need to work better together to improve the pace and scale of this improvement.
Despite the widespread use of pain rating scales in neonatal care worldwide, a new Cochrane review shows that current tools for assessing pain in newborns are based on very low quality evidence. According to the review, none of the pain rating scales in use today are methodologically reliable enough to measure pain.
The Cochrane analysis, which included 79 studies involving over 7,000 infants across 26 countries, evaluated 27 different clinical rating scales. The findings reveal significant limitations in the reliability and clinical usefulness of all currently available tools, raising concerns about whether healthcare professionals can accurately measure pain in this extremely vulnerable population.
“We were truly hoping that one pain scale would be stronger than another, but instead we found that all of them are poorly developed. This is an issue that also affects Swedish clinical practice and research. For example, a recent publication out of KI found that 25 percent of Swedish infants were assessed without using a rating scale at all, which was already shocking, and now we can confirm that the remaining 75 percent of the infants were assessed with rating scales that are now known to not be methodologically sound enough to measure pain. So, this unfortunately means that medical professionals cannot be sure whether they are measuring pain at all.” says Emma Persad, Phd student at the Department of Women’s and Children’s Health, Karolinska Institutet.
Yet, from this uncertainty comes a call to action. The researchers hope these findings will spark a global collaborative effort, led by Swedish experts, to develop a new, robust, and evidence-based pain assessment scale for newborns. Such a tool could greatly improve neonatal care worldwide and further establish Sweden as a leader in the field of neonatology.
According to the article “this involves developing better rating scales or physiological techniques to measure pain”.
““This is precisely what we are hoping to do. Through convening the global community we hope these findings and the outcome become a global collaborative effort, driven by Swedish researchers, to finally develop a pain rating scale that is robust and evidence-informed (and will hopefully be properly adapted and translated for use worldwide). We hope that Sweden’s role in neonatology can further be solidified through this work,” says Emma Persad.
Dr. Michael Copass, M.D.—a Harborview Emergency Medicine physician instrumental in the early development and later leadership of the Medic One paramedic training program, helping expand it beyond cardiac care—worked alongside Dr. Leonard Cobb and Seattle Fire Chief Gordon Vickery to shape what would become one of the world’s most respected emergency medical systems. When the original grant funding for the Medic One program ended unexpectedly, the community rallied in extraordinary ways: bake sales, marathons, neighborhood drives, even children donating their birthday money. Their efforts raised nearly $200,000, inspiring the creation of the Medic One Foundation in 1974 to ensure this lifesaving work would never fade. Since that time, more than $35 million has been invested in Medica One’s training, equipment, and research, contributing to lifesaving outcomes on a daily basis.
Years later, that legacy still lives and breathes inside the halls of Harborview Medical Center. As a student assistant with the University of Washington School of Medicine and the UW surgical residency program, I had the privilege of witnessing something quite extraordinary. Each week, an Emeritus physician would return to the hospital—not for recognition or ceremony, but simply to sit down for lunch and vibrant conversation.
Those gatherings were never formal lectures. They were living, breathing exchanges of wisdom — stories from the early days of emergency medicine, thoughtful clinical reflections, and gentle reminders that compassion matters just as much as technical skill. Students, interns, residents, fellows, and senior attendings all pulled up chairs. Hierarchies faded. Curiosity filled the room. Medicine, in its truest form, felt like a shared calling.
It was in those moments that I truly understood the impact Emeritus physicians have on the medical community. They often carry history, perspective, humility — and they give it away freely. Their mentorship strengthens not just clinical practice, but the heart of healthcare itself. The legacy of Medic One isn’t only found in ambulances and survival rates — it is also found in conversations around cafeteria tables, where knowledge is passed from one generation to the next.
And as we continue to advocate for fragile newborns and medically complex children, that lesson stays with me: when compassion, community, courage, and teaching come together, the ripple effect is immeasurable — and hope continues forward.
Sierra Leone, officially the Republic of Sierra Leone, is a country on the southwest coast of West Africa. It is bordered to the southeast by Liberia and by Guinea to the north. Sierra Leone’s land area is 73,252 km2 (28,283 sq mi). It has a tropical climate and environments ranging from savannas to rainforests. As of the 2023 census, Sierra Leone has a population of 8,460,512. Freetown is its capital and largest city.
Available healthcare and health status in Sierra Leone is rated very poorly. Globally, infant and maternal mortality rates remain among the highest. The major causes of illness within the country are preventable with modern technology and medical advances. Most deaths within the country are attributed to nutritional deficiencies, lack of access to clean water, pneumonia, diarrheal diseases, anemia, malaria, tuberculosis and HIV/AIDS.
Healthcare in Sierra Leone is generally charged for and is provided by a mixture of government, private and non-governmental organizations (NGOs). There are over 100 NGOs operating in the health care sector in Sierra Leone. The Ministry of Health and Sanitation is responsible for organizing health care and after the end of the civil war the ministry changed to a decentralized structure of health provision to try to increase its coverage.
Sierra Leonean Innovator and CEO of Women in Energy-SL Margaret Yainkain Mansaray became the first Sierra Leonean to be listed among Innovators competing for the Africa Prize for Engineering Innovation 2023. An award organized annually by the Royal Academy of Engineering UK (The United Kingdom’s national academy of engineering).
Mansaray, who is the only female rising to compete against 14 other innovators from ten countries across Africa was recognized for her invention of a Smart Green Stove. The smart green stove is a fast and efficient non-electric cooking device she designed to reduce greenhouse gas emissions and health risks that greatly affect women and girls in Africa.
The stove burns briquettes made from recycled local materials such as coconut and jelly shells which are usually discarded. The insulator absorbs most of the heat and makes the stove nearly smokeless, reducing the harmful soot which would otherwise be released into the environment.
“My team and I are working tirelessly to uplift women and girls by addressing time and energy poverty. I’ve always been the only woman in a room full of men, and so one of my aims is to educate women and girls, specifically on the role engineering can play in improving their lives.”, Mansaray said.
The Africa Prize for Engineering Innovation was launched in 2014 by the Royal Academy of Engineering. An award for ambitious African innovators creating local and scalable solutions to pan-African and international challenges. The innovations shortlisted in 2023 tackle challenges approaching the UN’s Sustainable Development Goals, including clean water and sanitation, sustainable cities and communities, clean energy, good health and well-being, and quality education.
According to the Royal Academy of Engineering, Innovators shortlisted for the Africa Prize will benefit from a special package of support including business incubation, mentoring, fundraising and communications. The package will also include access to the Academy’s global network of high-profile and highly experienced engineers and business experts in the UK and Africa. Four finalists will be chosen to direct their innovations and business plans to Africa Prize judges at an event in Accra, Ghana, on July 6th, 2023. The winner will have a take-home of £25,000, and three runners-up will win £10,000 each. An additional One-to-Watch award of £5,000 will be given to the most promising entrepreneur from the remaining shortlist.
Mansaray took to her Facebook handle and expressed her joy as she took pride in being that this is the first time Sierra Leone has been shortlisted for the Royal Academy Africa prize. She emphasized that her achievement is a win for the country and especially for vulnerable girls and women.
“I am happy to share that for the first time Sierra Leone has been shortlisted in the Royal academy Africa prize and I am the only female among 10 African countries.”, Mansaray wrote.
The song “Waterloo” is amazing! We discovered it through a promotion by Jakey Jake and instantly fell in love. This talented artist, known as Papi J, deserves to be signed to a record label. In this song, Papi J describes his hometown, Waterloo—a place known for its cassava bread, fried fish, and hardworking community.
Long, yet concise and comprehensive, this article is abundant in its research, collaboration, big-picture perspective, and applicability. Well worth the read!
Recommendations of the Iberoamerican Society of Neonatology (SIBEN®) for “Transdisciplinary and Humanized care for the Newborn and the Family”: XIV SIBEN CLINICAL CONSENSUS (English Version)
Jorge Pleitez Navarrete, MD, Carmen Dávila-Aliaga, MD, Lordes Lemus-Varela, MD, María Teresa Montes Bueno MT, Cristian Muñoz, MD, Augusto Sola, MD, Sergio Golombek, MD, and participants of the XIV SIBEN Clinical Consensus of the Iberoamerican Society of Neonatology (SIBEN)
Abstract: A cultural change in Iberoamerican neonatal hospitalization units is imperative to guarantee respect for the rights of newborns and their families during hospitalization, with equity at different levels of care, without differences based on geographic areas or socioeconomic level. It is essential to train and improve the competencies of the health team, from managers to healthcare professionals, to provide transdisciplinary and humanized care (CTH) for newborns and their families. There is sufficient evidence that CTH positively impacts the outcomes of newborns and their families when their families are involved in the care of their hospitalized babies.
This paper summarizes the results of the XIV SIBEN® Clinical Consensus on “Transdisciplinary and humanized care for newborns and their families,” in which 50 SIBEN® members, neonatologists, and nursing graduates from 14 Iberoamerican countries actively participated during 2023, before, during and after the face-to-face meeting held in Mar de Plata, Argentina in November 2023. This article answers questions based on the best available evidence and describes recommendations of clinical significance for truly providing transdisciplinary and humanized care (CTH).
Introduction:
In the 19th century, infant deaths were considered part of the natural order 1. In 1802, the first pediatric hospital, L’Hôpital des Enfants Malades, was founded in Paris, which promoted breastfeeding and the emotional needs of children.
Neonatology emerged in the 20th century owing to technological advances that increased neonatal survival but with reduced parental involvement. Research, such as the “Citizens’ Committee for Children of New York City” and the “Platt Report” in the United Kingdom, influenced the acceptance of parental presence in hospitals, demonstrating that their presence did not increase infection rates. Spitz coined the term “hospitalism” to describe the adverse effects of prolonged hospital confinement . In the 1980s, the family-centered model of neonatal care was introduced, demonstrating its effectiveness in caring for premature infants.
In 1984, the European Parliament approved the Charter of Patients’ Rights. In 1986, it adopted the European Charter for Hospitalized Children, which recognized 23 rights, including the right to be accompanied by their parents or primary caregivers for as long as possible. This charter was adopted by international organizations such as the WHO and UNICEF. Western countries began to ease visitation restrictions on parents as early as 1990.
Not all neonatology units in Ibero-America had adequate conditions to implement CTH by 2016. A study by the Ibero-American Society of Neonatology (SIBEN®) revealed that 63% of the units offered space for mothers to stay with their infants (27% overnight), and in 60% of cases, there were time restrictions for parental visits. This demonstrates the need for a cultural change in Ibero-American NICUs to guarantee respect for the rights of neonates and their families during hospitalization.
Concept and principles of transdisciplinary humanized care (CTH) for newborns and families
In recent years, different denominations have incorporated families into the care of hospitalized newborns. We consider that this care is provided by many disciplines to the newborn (NB) and its family in an integrated, simultaneous, non-hierarchical, organized manner, according to the needs of the newborn and, above all, in a humanized way; therefore, SIBEN calls this model of care “Transdisciplinary Humanized Care (CTH) for the newborn and its family.”
With a comprehensive approach, the CTH for the NB and its family emphasizes family participation, respect for their needs, and transparent communication . These interventions reduce neonatal stress, favor their development, reinforce the family’s caregiver role, and improve family bonding and quality of care.
The fundamental principles of CTH are respect, honoring families’ diversity, flexibility, exchange of information, no medical terminology, participation and decision-making, collaboration between the patient, family, and health care providers, and family empowerment to discover their strengths.
Levels of Intervention of CTH for the Newborn and Family :
• First level: Support parents through psychoeducational, communication, and environmental interventions to help them cope with hospitalization and prepare them for the newborn’s follow-up.
• Second level: Interventions provided by the parents focused on improving the development and recovery of the newborn, with psychological and physical benefits for parents who received education from the clinical team.
• Third level: Collaborative care models, where parents are fully involved in newborn care.
Elements of CTH (12)
According to the currently available scientific evidence, we agree with the following elements:
• Recognition of the family as an important and indispensable part of the care of hospitalized neonates
• Constant participation of the family in decision-making, as well as the procedures carried out
• Facilitate family/professional collaboration at all levels of care.
• Communication and exchange of information by health personnel at all times with the family.
• Recognition of family diversity, including ethnicity, socioeconomic, educational, racial, geographic,
etc., thus avoiding value judgments.
• Incorporate models that contribute to parents’ learning regarding the care of their children through courses and educational programs.
• Unrestricted access at all times and the family can always be involved in the care of their child
• Creation of family support networks.
• Recognize the family’s strengths, feelings, emotions, concerns, and ability to help and contribute,thus validating them as an important, fundamental, and indispensable part of the NB’s care.
• Facilitate the parents’ stay as much as possible by providing a comfortable space for them to be close to their child for as long as possible.
In 2011, the book Neonatal Care, Discovering the Life of a Sick Newborn by Sola, A introduces and emphasizes the concept that: “parents are not visitors” and that there should not be limited hours for a mother to be with her baby who is in the neonatal intensive care unit (NICU).
Changes, benefits, and tools for performing CTH:
* promote the newborn’s neurological and physical development
* humanize care
* reduce stress
* improve health
* improve adherence to treatment
* facilitate breastfeeding
* optimize discharge care and transition to home care
* increase the quality of care
* increase parental satisfaction
The following are some essential strategies to achieve this objective:
1. Information and awareness-raising: Promote the benefits of BFHC through programs aimed at medical teams, families, and public policymakers.
2. Staff training: Implementation of workshops, courses, and internships to train staff in CTH.
3. Involve parents from the beginning: Encourage their presence and participation in medical procedures and daily care to strengthen bonding.
4. Empower parents: Provide them with tools and training so that they can actively participate in making decisions about their babies’ health.
5. Adapt physical spaces: Design areas that allow parents to stay close to their children.
6. Ongoing emotional support: Offer psychological support programs to help families manage stress and emotional difficulties.
7. Planning and evaluation: Ensure gradual implementation with constant adjustments and collaboration of professionals, parents, and the community to achieve more humane and effective care.
Some tools to promote parental involvement in neonatal care include:
a) Welcome Kit: This kit contains educational information on neonatal care, educational resources,and guidance for parental involvement.
b) Skin-to-skin contact: improves thermal stability, facilitates breastfeeding, and reduces stress in parents and infants (7,18)
c) Care diary: Parents record the baby’s daily activities, such as feeding, diaper changes, and procedures, which allows them to feel more engaged in their care and evaluate their progress as caregivers.
d) Medical rounds participation program: Parents can discuss the baby’s condition and treatment, ask questions, and express concerns.
e) Training classes and workshops: Educational resources on neonatal care and child development are provided.
f) Mobile applications and online platforms: Allow parents to access up-to-date information on their baby’s condition, schedule visits, and communicate with medical staff.
g) Support groups and counseling: Facilitate mutual support among parents, share experiences, and get involved in their child’s care.
Difficulties or obstacles in the CTH process:
Including the family in the care of the hospitalized neonate is a humanized and recommended practice, although it is not always implemented in all neonatal units. Some professionals consider that the presence of parents is not necessary, arguing that they may generate anxiety, not be prepared for invasive procedures, or that the physical space is insufficient. In addition, lack of knowledge about family-centered care and institutional regulatory barriers negatively affect the care of the infant and family.
Skin to skin contact: Skin-to-skin contact (SSC) has ancestral origins in different cultures and times, and it is a common practice between mothers and their healthy or sick babies. In protocolized form, it began in the 1970s in Bogota, Colombia; the maternal body heat allowed it to stabilize physiologically and provide comfort and security to neonates. Since 1990, the success of this practice has spread, and it has been adopted in several countries as a neonatal care option.
SSC is beneficial for both term and preterm newborns, and it is applied immediately after delivery, during the first hour of postnatal life, during hospitalization, and even at home. It is associated with decreased maternal postpartum depressive symptoms, improved perspective on motherhood, and intrinsic and extrinsic gratification, especially being able to care for her baby. Lower maternal salivary cortisol levels have been reported at one week and one month postpartum.
In addition, recent studies have shown a significant prolongation of breastfeeding at six months (5.08 months vs. 2.05 months). Other findings highlight additional benefits, such as increased weight gain of the NB, reduction of hospitalization time, strengthening of the mother-child bond, and contribution to the overall development of the NB.
CTH and the advantages of breastfeeding
CTH includes the concept of 24-hour “open-door units” where fathers are encouraged to be present during breastfeeding and participate in feeding, either directly from the breast or by expressed milk. This approach promotes bonding, analgesia, neurodevelopment, milk production, and breastfeeding.
CTH and family satisfaction:
Parents of hospitalized NBs may experience acute or posttraumatic stress, affecting their physical, psychological, and social health, as well as their relationship with their children. Parents’ confidence increases when they know how to act and the impact of their actions on their infant’s health.
When CTHs are established, the family is recognized as a permanent reference in the child’s life, even during hospitalization. Family members become involved in the care, take an early part in it, and participate in decision-making regarding their child, promoting the parent-child bond .
The most important dimensions of neonatal care for parents are safety, care, communication,information, education, environment, monitoring, pain management, and participation .
SIBEN® recommends:
1. Change the paradigm and improve the communication skills of healthcare personnel to meet the family’s needs regarding the illness, treatment, and recovery of the neonate.
2. Encourage empathy, accessibility, and confidentiality in communication with families, increasing their participation in decisions about care and treatment. In addition, family functioning is considered to be crucial support during the newborn’s hospitalization.
3. Apply CTH from the admission of the newborn, integrating the family as active and competent caregivers of their child.
Family satisfaction helps in dealing with grief.
The NICU neonatal health team focuses on preserving the newborn’s life through therapeutic interventions . When parents face the loss of an infant, the grief they experience requires compassionate accompaniment by multidisciplinary teams that pay attention to psychological, emotional, and spiritual aspects of the family and offer empathy and respect for the parents to mitigate their pain .
Infrastructure to Implement CTH for the Newborn and Family
The World Health Organization (WHO) recommendation of 24-hour parental presence in the NICU has motivated the construction of neonatal units with private rooms, encouraging these indications. The implementation and use of private rooms in the NICU as a recommendation dates back to approximately 1990.
Impact and Advantages of private rooms for the newborn.
• Reduction of infections. Decreases the spread of nosocomial infections and makes the isolation of patients colonized by potentially pathogenic microorganisms possible.
• Increased weight gain. Preterm infants who remained in private rooms with their parents in the short term had a higher rate of weight gain during hospitalization.
• Less pain, with fewer procedures and lower pain scores in infants in private rooms compared to infants in shared rooms.
• Better neurobehavioral outcomes. Infants in private rooms had significantly less physiological stress, hypertonicity, and lethargy.
• Lower noise levels. In the shared NICU model, 20 decibels were found to be 20 decibels higher.
• Fewer days of hospitalization. More infants were discharged early.
• Increased breastfeeding. 90% achieved breastfeeding in private rooms compared to only 66% is shared.
• Fewer episodes of apnea. In the group stratified on the PEMR (Physician’s Estimate of Mortality Risk) scale, there was a 57% decrease in total apnea events in preterm infants.
• Reduction in direct cost.
• Reduction in illumination. Neonates admitted in open and private NICU rooms at Sanford Children’s Hospital in Sioux Falls, USA, were compared, and a reduction in illumination was shown: 48.4 lux and only 6.4 lux in private rooms (p < 0.05), with longer sleep time in neonates.
• Post-discharge: fewer consultations and hospitalizations. Comparing two groups of preterm infants it was found that they had lower rates of rehospitalization and requests for medical care at discharge.
• Higher cognitive scores. At an 18-month follow-up, Bayley III cognitive language and motor scores were compared in private and shared rooms in preterm infants under 30 weeks of gestational age. Infants with high maternal involvement in both NICUs had improved cognitive scores.
Disadvantages and risks of private rooms
The optimal types and frequencies of stimulation for very preterm brain development are unknown. Still, the isolation of these infants in relatively dark and quiet private rooms may be going in the wrong direction. However, auditory stimulation, such as parental voices, is considered positive in the NICU environment, being associated with better motor and language outcomes. Therefore, the need for greater parental permanence and involvement in the single-family room is emphasized, as otherwise, this aspect may be considered a disadvantage.
NICU nurses are at greater risk of fatigue, anxiety, and depression than nurses in general wards. Burnout in neonatal nurses continues to be a problem.
Is family presence during neonatal resuscitation or other invasive procedures advisable? ANSWER: YES. Parents or family members should be welcome to be present during an inpatient procedure and should not be asked to leave the room if they wish to be there.
SIBEN® Position. There is no scientific evidence to justify separating parents from critically ill NBs or those requiring advanced cardiopulmonary resuscitation. On the contrary, numerous studies report the beneficial effects on the parents, family, and even their approach concerning the care received. They always respect the parents’ decision to participate and are accompanied by health personnel who explain the situation and what they are seeing.
It is advisable, after the presence of the parents during the resuscitation, to carry out a joint analysis with their presence, to provide feedback to explain the procedures performed, to clarify their doubts, and also to consider their observations and concerns to improve the quality of the procedures performed in our units.
A philosophical concept to be taken into account is the following, which establishes a position in this regard: “Thus, from Anthropology, it can be noted that throughout the history of mankind, women have sought assistance at the time of childbirth, while the rest of mammals do it alone. It is considered that this is due to the complexity implied by the bipedestation, the pelvic cavity, and the human cephalic perimeter.”
Recommendations to implement transdisciplinary care in Neonatal Units:
• The importance of names: the name of the NB and his/ her parents. Knowing and referring to the mother, father, and newborn by name is essential. Never call or refer to the newborn as: “the baby in incubator number such and such”.
The art of communication. The importance of listening and making yourself understood.
Use simple and straightforward language to ensure that what has been expressed has been understood, especially when listening to the family’s concerns and encouraging them to ask questions and express emotions. Respect the family’s cultural and religious beliefs and customs.
We are part of the same team—”Parents Are Not Visitors” The importance of encouraging, facilitating, and accompanying the participation of the mother and family. Encourage skin-to-skin contact.
We should also consider the participation of the newborn’s brothers or sisters, grandfathers and grandmothers, or other designated persons, with the authorization of their mothers and/or fathers.
Interpreting beyond words. The importance of feelings and mental health support. Health care professionals should identify situations where the mother expresses fatigue, anguish, hopelessness, sadness, frustration, depression, crying, etc.
They are not alone. The importance of the peer support network and parent associations (such as FAMISIBEN)
In 2021, SIBEN®, with the FAMISIBEN working group, drafted recommendations for parents of neonates in the NICU. These recommendations are available in digital format on its website, https://sites.google.com/siben.net/famisiben/, free of charge for family members, caregivers, health professionals, and the general public.
Common questions for implementing CTH in the NICU:
Should the pacifier be banned? Answer: NO. Why? Non-nutritive sucking (NNS) is an integral part of infant developmental physiology. Based on the available evidence, the “SIBEN Mini Clinical Consensus / 2021” authors recommend initiating stimulation with a pacifier (NNS) at 28-29 weeks gestational age. Centers that “prohibit or forbid” the use of pacifiers, teats, or whatever it is referred to should review this restriction and know that this is not baby-friendly but quite the opposite.
Should the mother be made to feel welcome for 1440 minutes each day? Answer: YES “Parents are not visitors.” CTH for the family promotes stress reduction for the parents and a more positive relationship between the parents and the newborn.
Can the mother stay 24 hours a day in the hospital where the NICU is located? Answer: YES. We should encourage the mother or father to stay close to the baby even in the NICU; mothers and fathers in single family nurseries care more for their baby, including skin-to-skin contact compared to mothers in the open NICU, improving infant growth and neurodevelopmental outcomes.
d. Is there a minimum or maximum length of stay for at least one parent in the NICU? Answer: NO. There is evidence that the separation of hospitalized patients alters the dynamics of parental care and affects all family group members.
e. Will the family member (mother, father, or whoever the mother indicates) be able to participate in NICU care? Answer: YES. Family involvement is a key element in all infants’ physical, cognitive and psychosocial development, including those in the NICU.
f. What are the benefits of performing a blood sampling, vaccine placement, peripheral vein cannulation, or other pain-generating procedure with the infant nestled, held, and sucking? The SIBEN® Clinical Consensus on the diagnostic and therapeutic approach to pain and stress in the newborn recommends non-nutritive sucking when performing procedures that cause mild to moderate pain. Breastfeeding is considered the first choice treatment because of its safety, ease of administration, and availability, in addition to its multiple benefits, which have been extensively studied both nutritionally and immunologically.
What is the role of the “schools for parents” in the CTH for the newborn and the family? The schools are a training space for parents whose roles are as follows:
1. To allow conscious and active participation of parents in neonatal care.
2. Teach parents about the child’s physiological states, biorhythms, and adaptation mechanisms.
3. To offer knowledge for post-discharge care of the newborn.
4. To instruct on the benefits of breastfeeding and newborn feeding.
5. To teach and promote skin-to-skin contact.
6. Teach parents about hygiene, care, and medication administration.
7. To teach warning signs, infection prevention, and infant cardiopulmonary resuscitation.
8. Provide tools to work on psychomotor development stimulation, forms of stimulation, and
expected emotions of the newborn in different circumstances to ensure adequate growth and
development of children.
h. What key actions are indispensable and essential for CTH to exist?
1. First and foremost, a paradigm shift is necessary, associated with a theoretical/practical
educational plan for all personnel, providing them with specific tools and skills to promote
change.
2. Achieving the multidisciplinary participation of all neonatology staff without dissonant or
opposing voices (“everyone cooperates”).
3. It must be recognized that discussing this type of neonatal care is not enough since
implementing CTH in action requires facing and overcoming many challenges in different areas.
4. Modify the environment: It is essential to have areas, offices, and spaces for private conversations
with parents and family.
5. Partnering with health care administrators and financiers in the task
i. In the NICU of an institution certified as “mother and child friendly,” is CTH practiced for the care of the newborn and its family? In many NICUs, even in many hospitals certified as “mother friendly”, mothers are still separated from their babies, and there is little or no space for mothers, and a chair or bed is not always provided next to the newborn’s incubator.
Key points from SIBEN® about CTHs in the NICU:
• The brain’s structural plasticity is in response to maternal auditory stimulation.
• The quality of experience significantly influences the brain and the function and structure of the
developing central nervous system
• The presence of the family in neonatal care has beneficial effects, including improved bonding of
the NB with the family and improved quality of care.
• It should be emphasized that “parents are not visitors.”
• Smooth transition from the hospital environment to the home: no rush and no pressure. Ideally,
this occurs during pre-hospitalization, especially in prolonged hospitalizations of more than three
weeks.
• Setting concrete, everyday actions and deeds (not just words or documents) into practice, such as
those discussed in this manuscript, is very useful in achieving the best results.
• Periodically carry out critical and continuous self-evaluation of the neonatal team.
International cooperation and solidarity are essential in tackling global challenges, including efforts to ensure the effective realization of the right to health for all nations.
As proclaimed by the United Nations, promoting international cooperation and solidarity is a duty of States.
In this context, we express our profound appreciation, gratitude, and recognition to Cuban health professionals who have provided—and continue to provide—their services in multiple nations.
Since 2019, and with even greater intensity now, a dishonest campaign has been unleashed to discredit Cuba’s international medical cooperation, exert pressure on recipient governments, and deprive populations of essential healthcare services.
No one with a basic sense of honesty can doubt that this is an attack on multilateralism, a manipulation for political purposes, and a continuation of aggression and hostility against Cuba.
Access to healthcare is a human right, and millions of people cannot be deprived of this inalienable right for political reasons.
Attempts to delegitimize Cuban medical cooperation overlook the fact that the shortage of health professionals is a pressing issue worldwide, whose solution demands greater international cooperation and solidarity, not unfounded attacks.
Cuba has devoted considerable efforts and resources to health care and today has one of the highest ratios of doctors per capita in the world, enabling it to make a significant contribution to global health.
Cuban international medical cooperation has made it possible to provide high-quality health care to millions of people around the world.
Over the past 60 years, more than 605,000 Cuban health collaborators have completed missions in 165 nations.
Their feats are notable in the fight against Ebola in Africa, blindness in Latin America and the Caribbean, cholera in Haiti, and the COVID-19 pandemic. Numerous brigades from the Cuban International Contingent of Doctors Specialized in Disasters and Major Epidemics ‘Henry Reeve’ have carried out humanitarian work in many nations.
Cuban professionals and technicians participating in these programs do so exclusively upon the express request of the concerned countries, offering their expertise and services freely and voluntarily.
Many of them work in remote rural areas to save lives, even at the risk of losing their own. They provide care to all patients without distinction, refraining from getting involved in internal political affairs and strictly respecting the laws and customs of the countries where they work.
Additionally, Cuba has provided free medical training to 43,000 healthcare professionals from 120 nations. In numerous countries, medical faculties have been established with Cuban professors.
It is imperative to defend and recognize the valuable contributions of thousands of Cuban health professionals who, through immense personal sacrifice, continue to offer their cooperation.
Neither discrediting campaigns nor the devastating effects of the intensified economic, commercial, and financial blockade have succeeded in preventing Cuba from continuing to save lives and share its limited resources with other nations in need.
Cuban medical cooperation will remain a symbol of hope, dedication, humanity, and solidarity.
***The Non-Aligned Movement is a forum of 120 countries that are not formally aligned with or against any major power bloc, and dedicated to representing the interests and aspirations of developing countries. It was established in 1961.
Report identifies 7 of the most pressing industry trends that will shape the months and years ahead
ProgenyHealth, LLC, a recognized national leader in Maternity and NICU Care Management, today announced the release of its 2025 key trends and insights report, “Steep Challenges & Uneven Progress.” This year’s highly anticipated annual report identifies critical areas within maternal and infant health to watch in the year ahead, for health plans, hospitals, and healthcare providers.
The state of maternal and infant health in America remains precarious. By now, the sobering data has become all too familiar – The United States’ mortality rate is the highest of all high-income nations. Tragically, as many as 80% of maternal deaths, many of which occur in the first 42 days after giving birth, are preventable.
“While many challenges exist, there is continued hope on the horizon, as an increasing volume of healthcare-focused experts strategize to turn this situation around—and as new trends emerge to offer fresh opportunities and solutions,” said Linda Genen, Chief Medical Officer, ProgenyHealth. “These shifts promise to upend the present state of maternal and infant health, setting the nation on a new and better path forward.”
Key findings and predictions of the 2025 trends report include:
Maternal Decision-Making Will Take Center Stage. The concept of self-determination in the birthing process is being taken more seriously by medical institutions that are piloting programs to create dedicated care teams to listen to, work with and support those going through the birthing process. Research continues to show that providing women with a more empowered birthing experience pays dividends down the road.
Neonatology Will Continue to Advance the Viability of Micro Preemies. Until recently, very few infants born before 26 weeks were likely to survive. Today, many infants born as early as 22 weeks are not only surviving but thriving due to medical advancements. These extraordinary advancements have entirely improved the outlook for those born too young and too early.
Payers Will Increase Focus on Postpartum Support for Women. Between 2017 and 2019, nearly 30% of pregnancy-related deaths happened in the six weeks to 12 months after women gave birth, CDC data shows. Notably, many of these deaths were tied directly to mental health issues, which tend to go both undetected and untreated in the postpartum period. It is estimated that 50% of all postpartum depression cases go undiagnosed.
Amid Rising Costs, Employers Will Demand Alternatives to Standard Insurance Products. Since total birth costs are one of the top cost categories for health coverage, employers will likely begin to focus on proactive managed care partnerships to provide additional support during this complex period.
Increased Birth Anomalies Will Require More Complex Care. Congenital anomalies are among the chief causes of infant mortality, and as births increase across the nation—particularly in states with reproductive health restrictions in place—these anomalies are expected to climb. Children born with such anomalies may require surgical intervention, ongoing physical or occupational therapy, long-term educational support, or an array of assistive devices—needs that may evolve and last for life.
Whole Genome Sequencing Will Become a Game-Changer for Newborn Care. Rapid Whole Genome Sequencing (rWGS) testing for newborns may soon address this widespread genetic disorder blind spots. This genetic test can be used to identify and diagnose numerous conditions, including developmental delays, seizure disorders, conditions that affect hearing, vision, and immune deficiencies. rWGS is faster and more accurate than other genetic testing and considers a person’s full DNA sequence. While rWGS remains unavailable to many families, that situation is likely to change in the years ahead.
The Rate of Home Births Will Keep Rising – as Will Insurers’ Potential Role in Covering Them. Given the growing number of home births, some states are now exploring ways in which supporting this birth choice—and making it safer and more routinized, with intervention available in case of emergency—may help to combat certain aspects of the maternal health crisis
Newborn Health Resources: Trainings and Tools for Improving Newborn Health in Humanitarian Settings
In 2018, the Global Health Cluster lead by the World Health Organization (WHO) conducted a capacity survey of Global Health Cluster partners to capture information on partners’ self-assessment of their technical, operational, and coordination capacities. The results showed that most international and national partners reported a lack of capacity and expertise to provide maternal and newborn health (MNH) services. Less than half reported an ability to provide Basic Emergency Obstetric and Neonatal Care (BEmONC) and Comprehensive Emergency Obstetric and Neonatal Care (CEmONC) at primary and secondary level respectively, and only 42% of the international partners and 50% of the national partners reported providing Essential Newborn Care (ENC).
To accelerate newborn health services in humanitarian settings, recent global interagency efforts have led to the development of the 2018 Inter-Agency Working Group on Reproductive Health in Crises (IAWG)-endorsed Newborn Health in Humanitarian Settings: Field Guide (NBFG); the Newborn Care Supply Kits for Humanitarian Settings; and a Roadmap to Accelerate Progress for Newborn Heath in Humanitarian Settings: 2020–2024.
In addition, these resource cards were developed to facilitate capacity building of humanitarian stakeholders. To build these cards, a consultant conducted a mapping of key maternal and newborn health trainings across the development and humanitarian sectors using a methodology that included a desk review of existing trainings, stakeholder interviews, and a short online survey delivered to Health Cluster Coordinators. The findings of the mapping exercise were presented and discussed at an experts meeting organized by Laerdal Global Health, Maternity Foundation, and Save the Children in Stavanger, Norway in 2019.
Overall, the mapping identified a great variety of existing training programs, mainly for clinical health care providers, on all aspects of newborn care and at all levels of care provision. Existing trainings for program managers were somewhat scarce, and access to available tools and guidelines could be improved.
Thus, we have packaged these resource tools as a quick pocket reference to aid program managers and implementers in humanitarian and fragile settings with identifying and accessing the most relevant trainings, tools, implementation guidance, and clinical guidance
The transfusion of platelets and fresh frozen plasma (FFP) to critically ill neonates in neonatal intensive care units (NICUs) is a common intervention, yet it is still widely performed without adhering to international guidelines. The guidance itself on the therapeutic management of neonatal coagulation disorders is generally limited due to the absence of strong indications for treatment and is mainly aimed at the prevention of major hemorrhagic events such as intraventricular hemorrhage (IVH) in premature neonates. Historically, the underrepresentation of neonates in clinical studies related to transfusion medicine had led to significant gaps in our knowledge regarding the best transfusion practices in this vulnerable group and to a wide variability in policies among different neonatal units, often based on local experience or guidance designed for older children or adults, and possibly increasing the risk of inappropriate or ineffective interventions. Platelet transfusion and, particularly, FFP administration have been linked to potentially fatal complications in neonates and thus any decision needs to be carefully balanced and requires a thorough consideration of multiple factors in the neonatal population. Despite recent advances toward more restrictive practices, platelet and FFP transfusions are still subject to wide variability in practices.
This review examines the existing literature on platelet and FFP transfusions and on the management of massive hemorrhage in neonates, provides a summary of evidence-based guidelines on these topics, and highlights current developments and areas for ongoing and future research with the aim of improving clinical practices.
Connecting with your premature infant in the Neonatal Intensive Care Unit (NICU) may seem overwhelming and complicated. It can be a unique and challenging experience since it involves the emotional well-being of the parents and the development of the baby.
However, with the proper knowledge, resources, and support, bonding with your preemie may be a lovely and joyful experience. With the appropriate guidance and techniques, these may foster a closer relationship with your infant in its new surroundings.
Every baby and every situation is unique. Be patient with yourself and your baby as you navigate the NICU. Understand preemies’ distinct needs and the most significant ways to help them. This article will delve into everything you need to know about bonding with your premature baby in the NICU.
Understanding Preterm Development: How It Helps With Bonding
Preterm and full-term newborns have a developmental trajectory, even if preterm babies grow at a different rate. Premature infants, or preemies, as they’re fondly called, have a distinct development.
A clear understanding of preterm development is critical to the bonding process between parents and their preemies—a great way to get closer to your baby. You can still establish a connection with your preemie while in the NICU by being aware of their developmental milestones.
Parents must understand their unique requirements and developmental stages to effectively care for and support them. Some of these characteristics include:
Small Body, Thin and Delicate Skin
Overall, premature babies have significantly low birth weight; hence, their physical size is relatively small. Additionally, they have thin and delicate skin. These unique features require special care in handling and bathing them.
Sensitivity to Touch
Premature babies learn about the world mainly through touch. More importantly, a sense of touch is the key for parents to bond with them. However, they’re more sensitive to touch than full-term babies, so providing a gentle and comforting touch is critical.
Vulnerability to Overstimulation
Light and noise are two stimuli that easily overwhelm premature babies. It’s best to create a calm and quiet environment that makes them feel more secure and facilitates bonding.
Delayed Bone and Muscle Development
As advised by medical experts, involve your premature infant in gentle exercises and motions to help support their development and create opportunities for bonding.
Premature babies may have delayed physical development, including muscle and bone development. Late preterm babies, born between 34 and 36 weeks, may have fully developed organs but still have changes happening in their brains.
Premature babies born earlier than 28 weeks and babies born with an extremely low birth weight of less than 1 kg have the highest chance of developing problems.
Potential for Neurodevelopmental Challenges
Premature babies may experience long-term effects on their cognitive and neurological development, including learning disabilities, attention-deficit/hyperactivity disorder (ADHD), and difficulties with executive functioning.
Parents must be aware of these developmental challenges; hence, bonding and interaction with their baby should consider these disabilities.
Needs Specialized Care
Premature babies in the NICU require specialized medical care, which makes it challenging for parents to bond with them. However, being involved in their care, such as participating in diaper changes or helping with feeding, can still contribute to their bonding success.
Potential for Longer Hospital Stays
Premature babies need to stay in the hospital for an extended period, which can be emotionally challenging for parents. Finding ways to stay connected and involved with their care can help maintain the bond during this time.
Understanding these unique characteristics helps parents bond with their premature babies. By being aware of their baby’s needs and sensitivities, parents can provide a comforting and supportive environment that promotes bonding and development.
Bonding with Your Premature Baby in the NICU
Managing the difficulties and uncertainties of having a preemie could be complex. You need to focus on developing a strong bond, even while in the NICU. By prioritizing this bond, you provide your baby with love and encouragement despite hardship.
Maintaining a deep bond with your baby through care and engagement is essential for their development and general well-being throughout their stay in the NICU. Premature infants who receive loving care are more likely to experience favorable developmental outcomes.
Remember that every baby and family’s situation is unique, so it’s important to tailor your approach based on the specific needs and guidelines provided by the NICU staff
There are many ways to develop a bond with your baby. Here are some tips to consider:
1. Spend quality time.
Find time to visit your baby regularly at the NICU and make the most of the time you have together. Even if your baby is sleeping or connected to monitors, your presence creates a sense of familiarity and constant support.
Your presence alone provides a long-term positive impact on your baby’s development and gives you confidence as a parent too. Spending time with your baby is such an important part of bonding in the NICU.
2. Learn your baby’s cues.
With your regular visits to your preemie, you take time to learn your baby’s cues. Get involved in their care, especially on how to make your baby comfortable at all times. You may ask the NICU staff for guidance on how to interact with your baby.
3. Kangaroo care.
Also known as skin-to-skin contact, kangaroo care is highly encouraged and affords numerous benefits to premature babies. This involves holding the baby against your bare chest with only a diaper on for an extended period.
Hold your baby against your chest so they can hear your heart beating. For a premature baby, such moments are crucial for physical and emotional bonding.
This skin-to-skin contact helps regulate the baby’s temperature, heart rate, and oxygen levels, promotes breastfeeding and breathing, and reduces stress for both the parent and baby. It also promotes weight gain and digestion. All these benefits foster bonding with your preemie.
4. Gentle touch.
Premature babies are sensitive to touch due to their underdeveloped nervous system. Use a light and gentle touch to stroke your baby’s skin, hands, and feet. This tactile stimulation helps promote relaxation and bonding—a soothing effect that helps establish a connection with the parent.
These comforting touches provide reassurance and make the baby feel loved and secure. Your care team will guide you to feel comfortable while touching your baby. They will guide you in specific ways that your baby will be looking for and can tolerate.
Some NICU infants can be held right away, while others may need an alternative approach. Once their condition is stable, massage can also help them relax. They will feel calm, cared for, and supported. You could hold your baby’s hand or stroke their head, for example.
5. Talk, sing, and read.
Premature babies benefit from hearing their parent’s voices. Even though they may seem too small to understand or respond to, talking, singing, and reading softly to them create a sense of familiarity and connection. It helps them recognize and connect with your voice, promoting bonding.
Engage in gentle conversation and sing lullabies. Your voice will become familiar to them, providing a sense of security. Your baby recognizes your voice from when they were inside the womb, so hearing it can be comforting and soothing—a source of bonding during the NICU stay.
6. Help with care tasks.
Discuss with the NICU staff if you could participate in your baby’s care routine as much as possible. Changing diapers, feeding if permitted, and bathing your baby enhance your bonding experience and help you feel more connected with your little one.
Other simple tasks could just be providing comfort through swaddling and positioning. These activities help establish a sense of parental responsibility that promotes bonding.
7. Create a sense of normalcy.
Despite a highly medicalized environment, try to create a sense of normalcy by personalizing the baby’s space. You can bring familiar items, such as a blanket or a small toy, to make the surroundings feel more like home.
8. Leave your scent.
Check with NICU staff to learn what cloth items are appropriate to place in your baby’s space. Sleep with that item or wear it all day tucked under your clothing, then place it in your baby’s space. In this way, you’re establishing a connection with your baby through your scent.
Sweet premature baby in an incubator with oxygen and unrecognizable mom caressing baby trying to calm him down
9. Take care of yourself.
Prioritize self-care during this challenging time, taking care of your physical and emotional well-being during this stressful period. Have a balanced diet, get enough rest, and engage in activities that give you joy and relaxation.
When you’re calm and well-rested, it positively impacts your interactions and connection with your baby.
10. Seek emotional support.
The NICU experience can be emotionally overwhelming and exhausting, especially for moms. It’s essential to seek support from your partner. Also, from healthcare professionals, therapists, family, friends, and support groups specific to parents of premature babies.
Sharing experiences and emotions can help cope with the challenges and strengthen the bond during this critical period. They can provide comfort, understanding, and guidance, which are essential for maintaining a healthy emotional state during this challenging time.
11. Seek support from NICU staff.
Ask the medical staff for guidance and support on ways to bond with your premature baby. They have experience working with families in similar situations and can offer valuable advice and resources.
12. Ask questions.
Don’t hesitate to ask questions or seek clarification from the medical team regarding your baby’s condition, progress, and care plan. Being well-informed helps alleviate anxiety and empowers you to initiate more meaningful interactions with your baby.
13. Celebrate milestones.
Premature babies often reach developmental milestones later than full-term babies. Celebrate each small achievement, such as gaining weight, moving to an open crib, or starting to breastfeed.
These milestones testify to your baby’s progress and strengthen the bond between you and your little one. Maintaining a positive outlook can help strengthen your bond and offer hope during the NICU journey.
Make Bonding Moments with Your Preemie at the NICU
Nothing is as unique as a parent’s and baby’s bond, despite the challenges. Even in the NICU, you can create lasting memories and form a connection that will grow as your baby grows. Understand your baby’s growth and foster a happy atmosphere with your preemie.
Bonding happens over time, and it’s built on everyday moments like smiling at your baby, touching them, using loving words, and responding to their needs. With the strategies outlined in this article, determine which technique works best for you and your baby.
While every baby is different, you may try various approaches. Enjoy every bonding moment. Your preterm baby may be physically small, but they’re strong and have a lifetime of love and opportunity ahead of them.
In late 2021, I was pregnant with twins, 2 little siblings for my son Rico. The pregnancy was very exciting, and we couldn’t wait to meet them. We wanted to do a gender reveal, but sadly we didn’t get the opportunity.
At 21 weeks, I had a scan which found that my cervix was open. I had to have an emergency cerclage on New Year’s Eve 2021, and was in hospital for 2 weeks.
A week after being sent home, my waters broke. I was 24 weeks pregnant at this point and very scared. I rushed back to hospital where they told me I would remain until the twins were born.
Giving birth
10 days later, after multiple scans, I went into labour. My beautiful twins were born at 25 + 6 weeks at 2:03am (Luna) and 2:36am (Luca).
Both babies were transferred to NICU to begin their fight.
At 4 days old, suddenly and unexpectedly, our baby boy Luca died. We had to wait 6 months for his postmortem results to find out why, which is when we were told he’d died of NEC. Our survivor Luna spent 87 days in NICU before coming home.
How I coped
The early days of grief I just shut myself away from people. I was at the hospital everyday with Luna and I just engrossed myself in caring for her. I had bereavement therapy which didn’t really help me, but what did help immensely was PTSD therapy.
I’ve also used the Facebook community to reach out to other people who have been through similar situations. I’ve made friends through those communities and we regularly message and support each other when things get tough.
Honouring Luca
We miss Luca every day. Having a surviving twin is such a complex mix of emotions – we feel happy and sad at the same time. We honour Luca daily and include him in our family.
We have a garden for him at home and in my parent’s garden. I also wear jewellery to remind me of him, and have lots of little ornaments around the house in his memory. On the twin’s birthday, we had a cake for both of them (pink and blue).
Every year, I try to do something for charity in his name. Last year I raised over a £1000 in a swimming challenge and this year I took part in Tommy’s Walk for Hope and managed to raise £400.
Advice for others
My advice to anyone who loses a twin baby would be:
Embrace the feelings of happiness and sadness. Losing a baby is something that no one should have to go through, but you’re a twin parent and your survivor will always be a twin.
Reach out to support through charities, and take counselling if you can. You will probably be suffering from some form of PTSD and working through that really helped me.
Led by trained PSI facilitators, our online NICU group is intended for parents of babies who are currently or formerly in the NICU. This peer support group is for those with babies up to two years old who experienced a NICU stay for any reason. Connecting with others who have experienced the uniquely stressful environment of a NICU will provide parents with understanding, as well as helpful tools and resources. Whether your baby is currently in the NICU or you have finally returned home, our NICU Postpartum Parents support group is here for you.
Note: This group is not for people processing the details and trauma of pregnancy and/or infant loss. Please join one of our Loss and Grief Support Groups for this important support.
PSI Support Groups
All of our groups are FREE and virtual. When registering for Sharewell for the first time, skip the unlimited offer on the payment page.
What to Expect
Our groups are 90 minutes (1.5 hours) in length. The first ~30 minutes is spent providing information, education, and establishing group guidelines. The next ~60 minutes is “talk time,” in which group members share and talk with each other. Group members must be present for the group guidelines before joining in the discussion or “talk time.”
Student and clinical observations are not allowed in our group spaces due to confidentiality and creating a safe space.
Cameras are required during introductions for the safety of all group members. Please make sure your technology allows you to turn on your camera at least briefly for this portion of the session.
The session will take place via Zoom (from the ShareWell website), so make sure your device is compatible with the Zoom app. This may require updating or downloading the Zoom app.
Student and clinical observations are not allowed in our group spaces due to confidentiality and creating a safe space.
Registration Information
PSI Support Groups are hosted on ShareWell and are split into different “wells.” Click on the registration link above to go to the Well, which includes support groups in each category.
When signing up for groups and making an account:
Skip the unlimited offer on the payment page (all of our groups are free!)
Access PSI support groups in each dedicated community
Reach out to groups@postpartum.net if you have any questions
In this new platform, we will no longer have a waitlist function. **We will allow up to 16 group members to enter the group, so please arrive on time to get a spot. Once we reach 16 members OR we have started talk time, the group space will be closed.
Sick or premature babies: tips for family and friends
Key points
Parents of sick or premature babies have a lot of stress in the early months of their babies’ lives.
Practical help and emotional support from friends and family can help parents cope.
It’s good to ask parents exactly how you can help.
Supporting parents of sick or premature babies
Parents of sick or premature babies go through a lot of emotional ups and downs in the early weeks and months of their babies’ lives.
When they get practical help and emotional support from family and friends, parents often cope a lot better with the experience. And when they’re managing well, they’re better able to look after their babies.
Here’s how you can help
Celebrate as you usually would when a baby is born
Offer congratulations, send a card or flowers, and ring the new parents. By celebrating the birth of their baby in this way, you’re helping them celebrate as well. Give a gift if this is what you’d usually do. Small gifts for the parents can help them feel nurtured too.
If you’re thinking of giving clothes for the baby, make sure they’re very easy to put on and take off – loose necklines and armholes are good. If the baby is premature, size 00000 clothes can also be useful, because many parents won’t have bought these smaller sizes. Baby clothes for later are wonderful too, because they help the parents think about the future, when their child is at home.
Another gift could be a voucher for hospital parking. Or you could give a voucher for a restaurant close to the hospital, so that parents can have a meal and some time together but not be far from their baby.
You might be able to contribute to or help the parents organise cultural or religious traditions or ceremonies to celebrate their baby’s birth.
2. Offer practical help
Parents will be visiting the hospital as often and for as long as they can for days, weeks or months to come. This means that everyday chores are hard to fit in or don’t get done, which can be stressful.
Here are helpful things you could offer to do:
Mow the lawn or walk the dog.
Prepare meals or do the weekly grocery shopping.
Take older siblings to preschool or school or look after the other children in the evening.
Give parents a lift to the hospital – parking and transport can be very expensive.
Set up a messaging group or social media page, so that parents can send updates to just one source.
3. Support parents in whatever way they need
It’s OK to ask parents what they need. Some parents want to shut themselves off and cope with the situation alone or with a few close friends and family. Respect their wishes, but also let them know that you’re thinking of them. You could try to offer help when they seem ready.
Some parents need a lot of people around for support. These parents might love having company at the hospital. You could offer to drive, have lunch or just sit with them. Some parents want to talk about things other than the baby. Parents’ needs can change as their baby grows and changes.
4. Stay in touch with parents
A text message, an email, a quick phone call or voice message, or even an old-fashioned card in the mail – these are simple ways to let parents know you’re thinking of them. They help parents feel supported and remembered.
Try to understand how stressed the parents are and avoid judging them if they forget a birthday, can’t get to a family gathering, or take less interest in what’s happening in your life. It’s not that they don’t care – it’s just that right now, all their energy and focus is on their baby.
5. Say positive things about the baby
You can show your support by saying positive things like ‘Your baby is growing fast already’, or ‘They’re strong just like you’.
Avoid talking about setbacks that might happen or challenges that the baby could face, unless the parents bring it up with you. Also avoid giving advice about the baby.
6. Don’t expect to cuddle the baby
Sick or premature babies are very sensitive to touch, noise, infection and other things in their environment, so cuddling or touching is often limited or not allowed. Parents can also be very protective of their babies.
You might not even be able to see the baby, because there are usually limits on the number of visitors allowed at one time. Often it’s only 2 visitors. Sometimes only family is allowed – often this is only the baby’s parents. Each hospital has its own set of rules. Instead, you could ask to see photos of the baby (if the parent feels up to sharing them) or have a coffee with the parents at the hospital café.
Don’t be surprised if you still can’t have a good cuddle when the baby goes home. Many babies are still easily overwhelmed and might need to be protected from too much handling and too many new people.
Parents are likely to have mixed and strong feelings about their sick or premature baby and their experiences of the birth or hospital. These might not surface for weeks, months or even years.
Be open, let them talk and avoid giving advice unless it’s asked for. Avoid comparing them with other parents who’ve had a hard time. If you listen more than talk and follow the lead of the baby’s parents, you’re more likely to be helpful.
8. Keep offering help after the baby comes home
Parents might be tied to the house for some weeks once the baby comes home. Having someone organise shopping or preschool and school runs can really help.
Premature babies, or “preemies,” are born before 37 weeks gestation.
Hailey Petersburg was born at 24 weeks and five days.
Considered a “micro-preemie” and weighing just one pound and seven ounces, Hailey had a 40% chance of survival and a long road ahead of her in the Neonatal Intensive Care Unit (NICU). She spent 133 days in the NICU, where she underwent multiple surgeries and was treated for anaemia of prematurity. “Every day was a rollercoaster,” said Hailey’s mother and Leidos Data Scientist Allison Petersburg. “She was in a critical stage where her condition changed so rapidly every day.”
Before Hailey even reached what would have been full-term at 40 weeks, she received almost two dozen transfusions, which were crucial to her treatment plan.
Hailey’s tiny body was working as hard as it could, often enduring bradycardic events where her heart was beating too slow. Her medical team provided blood and platelet transfusions to help carry oxygen throughout her body; their impact was immediate, improving Hailey’s health and significantly increasing her vital signs.
In the United States, someone is in need of blood or platelets every two seconds. For many months, Hailey was one of those people. She received blood or platelet transfusions almost daily in the first weeks of her life, decreasing over time as she grew stronger each day. “Throughout the NICU experience of being in day-to-day survival mode, the gift of blood was a vital stability for Hailey,” said Allison.
Blood and platelets can’t be manufactured and must be donated. They also have an expiration date, so there is always a need for more blood donors. Since the beginning of the COVID-19 pandemic, the American Red Cross has seen a decline in blood donations, resulting in a national blood crisis. Between blood, platelets, and plasma, “nearly 16 million blood components are transfused each year in the United States.”
“Whenever Hailey had a transfusion, she would immediately begin breathing better, her heart rate was stable. As she received blood, the bradycardic and oxygen desaturation events decreased and all her vital signs improved,” said Allison. “They were lifesaving.”
After almost four and a half months in the hospital, Hailey Petersburg was ready to go home. Fast forward five years, and now Hailey is a recent preschool graduate, who, according to her mother, “is doing absolutely amazing.”
She’s an active soccer player, swimmer, and dancer, as well as an avid Disney princess fan, currently infatuated with Jasmine from Aladdin. Allison thinks Hailey intuitively knows how hard she had to fight soon after she was born, citing her joie de vivre, “she’s just the happiest little girl.”
Hailey is an example of why it’s so imperative to donate blood if you’re able. With nearly 30,000 units of blood needed each day, the Red Cross is continually in need of donors and one pint of blood can save up to three lives.
Even during a global pandemic, Leidos remained committed to diminishing the national blood crisis, collecting more than 311 units over the past two years. Since 2016, we’ve hosted 23 blood drives at our Global Headquarters in Reston, VA, thanks to 674 donors. Other offices, including our Columbia, MD, and San Diego, CA, locations regularly host blood drives, as well as one of our subsidiaries, QTC. The Columbia Leidos office has collected 125 units of blood since 2017.
Not only is donating blood so important, but the process is very quick, only taking about 20 minutes for the physical donation. For perspective, if just 1% more of all Americans donated, blood shortages “would disappear for the foreseeable future.”
“It was clear that the donated blood Hailey received in her transfusions saved her life,” said Allison. “I don’t know if my daughter would be with us today if not for blood donors.”
Schedule an appointment to donate blood today – and save a life.
The still predominant siloed, vertical structure of academia, health care systems, funding institutions/mechanisms, and public health organizations around the world pose an important challenge to tackle complex societal and health challenges for people, animals, and ecosystems. Understanding and acknowledging the delicate interdependence between ecosystem, human, and animal health is needed to design and implement comprehensive and holistic health strategies, beyond just human health. Infectious diseases with a zoonotic component have caused widespread human suffering in recent decades, with increased interactions between human and animal populations making people ever more vulnerable to new infections, given the rapidly and constantly changing global ecosystem. Additionally, socio-cultural, political, and economic factors impact the ability of systems to better prevent, detect, and respond to public health challenges at the human, animal, and environmental interface. This complex landscape applies to non-communicable diseases as well, requiring multisectoral approaches well beyond the traditional, narrow biomedical model. Hence, a wholesale shift is needed in how we approach public health. Instead of equating public health only with human health, we need to recognize what it truly is: the inter-related health of the world’s people, animals, and the environments we all share.
The complete interdependence between human, animal, and ecosystem health has been long recognized within Indigenous communities; however, the emergence and rapid expansion of the fields and practice of both One Health (OH) and Planetary Health (PLH) are recent developments in the right direction [1]. While the OH approach has been advocated for mostly in the context of addressing global threats related to zoonotic diseases and antimicrobial resistance, this approach is also relevant for several major public health challenges including pollution management, the environmental/agricultural component of food safety, food security, and nutrition. For example, the OH approach may lead to ecologically sustainable dietary patterns impacting the prevention and management of chronic conditions, such as cardiovascular disease.
The OH/PLH approaches have experienced considerable growth and expansion in academia, and within governmental and non-governmental organizations (NGOs)—with greater traction occurring in the past decade . While OH and PLH are highly complementary approaches based on transdisciplinary, multisectoral, and system-based approaches to health, challenges remain when translating ideas into policy and practice. “Overall, One Health and Planetary Health provide an opportunity to build a stronger research community to collectively address pressing public and global health issues in a truly integrated way”.
In March 2023, the Quadripartite organizations: the Food and Agriculture Organization of the United Nations (FAO), United Nations Environment Programme (UNEP), World Health Organization (WHO), and World Organisation for Animal Health (WOAH), issued an unprecedented call for enhanced global action to use the OH approach to “achieve together what no one sector can achieve alone”, emphasizing the need to translate the OH approach into policy action. Additionally, the Quadripartite institutions, in December 2023, published the One Health Joint Plan of Action with recommendations to implement OH approaches at national levels. Similar movements are occurring within the PLH space. For example, a National Planetary Health Action Plan (NPHAP) is being developed in Malaysia “to mainstream planetary health in all national policies and plans through a holistic and whole-of-nation approach”. Having endorsements from national and international organizations are important; however, there are still elements lacking when considering the implementation of OH/PLH to ensure human, animal, and ecosystem health.
What is next? Local community leadership and involvement is needed to build upon progress to date at the global level. To tackle complex public health challenges, a “bottom-up” approach is needed that complements global and national efforts. An emphasis on local, practical, and feasible solutions are also needed to address complex problems, while engaging local stakeholders and affected communities. A key aspect, however, of implementing OH and PLH approaches into public health strategies is to account for the socio-cultural, religious, and economic factors among local and rural communities. This is especially important when working with those most marginalized, such as Indigenous and rural communities, who are often already closely and directly attached to having strong connections with the ecosystem they inhabit.
Scientific, biomedical, and health knowledge is necessary, but not sufficient alone. Successful public health interventions that work at the human-animal-ecosystem interface require the broad and committed collaboration of members from all levels of society. A coordinated, multisectoral approach that involves animal health and public health authorities, health practitioners, physicians, veterinarians, environmental workers, politicians, researchers, experts in social, cultural, and communication issues, as well as economists, farming and agricultural groups, and local communities is necessary. Importantly, bold and courageous political leadership is essential to co-lead while securing public support for health policy decisions and implementation [5]. It is key to develop a OH/PLH “business case” (e.g. cost-benefit analysis), with governments enabling, facilitating, and supporting implementation processes both financially and within appropriate legal frameworks. This will ensure the recognition for not only the importance of economic benefits derived from reducing a specific health issue, but also for assessing the broader public health and societal benefits and impacts.
While OH and PLH offer a rational systems approach for safeguarding health in an interconnected world, to secure its benefits, public health must do what humans, animals, and plants have always done—evolve!
Globally, the management of low-risk pregnancies by midwives often leads to a more natural childbirth process, which enhances physical and psychological outcomes for mothers and their babies. Midwives implement various models of maternal care in practice. This study investigates and compares maternal and neonatal outcomes associated with midwifery-led care versus routine midwifery care in private hospitals in Iran.
Methods
This retrospective cohort study was conducted in Iran in 2022. The study population consisted of two groups including 387 women in the Routine Care Group (RCG) and 397 women in the Private Care Group (PCG). Participants were selected through continuous sampling in accordance with the inclusion criteria. The two groups were compared in terms of some maternal and neonatal outcomes. The research data collection tool was a researcher-made checklist with variables adjusted according to the ‘Iman’ system of the Iran Ministry of Health. Based on this tool, the data were extracted from the mentioned system and analyzed with SPSS software.
Findings
The results indicated no significant difference between the two groups in terms of the type of delivery (p = 0.999), the use of forceps or vacuum (P = 0.5) and transferring the mother to the operating room (OR) or the intensive care unit (ICU) immediately after delivery (P = 0.744). However, there was a statistically significant difference between the two groups in terms of labor pain control (P < 0.001), induction of labor (P < 0.001), and the use of episiotomy (P < 0.001). Regarding neonatal outcomes, there was no statistically significant difference between the two groups in relation to the average infant weight (P = 0.46), Apgar score (P = 0.75), need for resuscitation (P = 0.999), skin-to-skin contact (P = 0.626), initiation of breastfeeding (P = 0.241) and admission to the neonatal intensive care units (NICU) (P = 0.66).
Conclusion
Given the positive impact of private care on key maternal outcomes, it is recommended that health policymakers create the conditions necessary for establishing a continuous midwifery care model in both governmental and private hospitals. Besides, more quantitative, qualitative, and especially mixed methods research should be conducted to explore the challenges and facilitators of this model across various settings.
Children born before 37 weeks of gestation have a considerably increased risk of dying before they reach the age of five. Predicting the risk of preterm birth (PTB) and hence implementing preventive strategies is complicated by the heterogeneity of the condition, the many unknown mechanisms involved, and the lack of reliable predictive tools.
Now, however, researchers have been able to show that blood cell-free RNA (cfRNA) signatures can predict PTB over four months before delivery date. The research was presented at the annual conference of the European Society of Human Genetics.
Dr. Wen-Jing Wang, an associate researcher at BGI Research in Shenzhen, China, together with team leader Professor Chemming Xu from the Obstetrics and Gynecology Hospital of Fudan University, Shanghai, China, and colleagues analyzed blood plasma samples from 851 pregnancies (299 PTB cases and 552 controls) at about 16 weeks gestation to identify cfRNA markers associated with spontaneous PTB, and found significant alterations in cfRNA between PTB and birth at term.
The study included both preterm births with intact membranes and premature rupture of membranes (when the waters break before labor starts), with fewer than 3% having a prior preterm birth.
“Being able to detect these predictive signals over four months suggests early biological priming for PTB, far earlier than current clinical recognition,” she says. “This extended window could revolutionize prevention strategies.”
Annually, about 13.4 million newborns worldwide are delivered prematurely, accounting for approximately one in 10 of all live births. Nearly one million of these preterm infants die each year, and PTB remains the primary cause of mortality in children under five.
Because children born preterm have immature organs that are not yet prepared for life outside the womb, it means that they will have a far higher risk of complications than those born at term. This can lead to a range of health issues such as respiratory problems, jaundice, feeding difficulties, and infections.
Long-term health problems for these children include cerebral palsy, epilepsy, and blindness, and impose substantial emotional and financial burdens on families.
“Practically, our method uses the same blood draw timing as routine Non-Invasive Prenatal Testing (NIPT), enabling dual testing. Current cfRNA sequencing costs are similar to NIPT pricing, but future optimization using targeted qRT-PCR panels could reduce expenses significantly. This creates a potential route to both monitoring patients at high risk and for wider population-level screening,” says Dr. Wang.
Before this diagnostic technique can be used more widely, the researchers say that standardized protocols for sample handling need to be developed, given RNA’s instability compared with DNA.
Prediction algorithms need to be developed in diverse population studies, and the causes of different PTB subtypes explored to be able to guide targeted interventions. The team is pursuing these goals and seeking to collaborate with other institutions in order to accelerate the use of their findings in clinical practice.
Chair of the conference, Professor Alexandre Reymond, said, “Advances in sequencing and analysis technologies are now offering many new diagnostic possibilities. This is a fascinating example of the use of sequencing readouts to evaluate risk, rather than assessing genetic background to assess predisposition.”
Saving Tiny Lives: The Critical Need for Blood and Platelet Donations for Preemie Babies Undergoing Surgery
Premature infants, especially those born before 32 weeks of gestation, often face life-threatening challenges that require surgical intervention. These delicate babies are at heightened risk for bleeding complications due to their underdeveloped organs and fragile blood vessels. In fact, studies indicate that platelet transfusions are administered to 5.8%–53.0% of neonates with a gestational age at birth below 32 weeks, underscoring the critical need for these life-saving donations.
When it comes to blood versus platelets, it’s essential to understand the differences. Blood transfusions typically involve the whole blood or red blood cells, which help provide oxygen to the body’s tissues. For preemie babies, blood transfusions are often required to address anemia, a condition where the body doesn’t have enough red blood cells to carry sufficient oxygen. Platelet transfusions, on the other hand, are crucial for babies who are at risk of bleeding or have low platelet counts, which are essential for blood clotting. While blood transfusions address oxygen needs, platelet transfusions play a vital role in preventing severe hemorrhaging in these tiny patients.
The impact of blood and platelet transfusions on preemie babies cannot be overstated. For instance, a study involving neonatal surgeries revealed that 14% of neonates received perioperative red blood cell transfusions. Among those transfused, 30-day mortality rates were significantly higher, and they also experienced increased rates of complications such as wound dehiscence, mechanical ventilation beyond 48 hours, cardiac arrest, and septic shock. Platelet transfusions, however, are often the key to minimizing bleeding risks during surgeries and promoting recovery in fragile babies.
Recognizing the importance of these donations, I recently contributed by donating platelets to support children undergoing cardiac surgery. This experience highlighted the profound difference that blood and platelet donations make in the lives of critically ill children. Each donation has the potential to save lives and improve outcomes for these vulnerable patients. If you’re considering how you can make a tangible impact, donating blood or platelets is a powerful way to help. Your donation could be the one that gives a tiny baby the chance to grow, thrive, and lead a healthy life. To learn more about how you can donate and make a difference, visit your national blood donation agency’s website. Your generosity can be the lifeline these babies desperately need.
Surf’s up in Sierra Leone
Sierra Leone’s beaches and waves make them attractive for surfers. But the country has just one surf club. It tries to get boys and girls off the streets and into the water, despite equipment and personnel being in short supply. Sierra Leone is still infamous for its civil war and poverty. But it’s also incredibly beautiful. Enjoy the breathtaking views from Bureh Beach — a perfect spot for surfing.
Singapore has a generally efficient healthcare system, even though health expenditures are relatively low for developed countries. The World Health Organisation ranks Singapore’s healthcare system as 6th overall in the world in its World Health Report. Singapore has had the lowest infant mortality rates in the world for the past two decades. In 2019, Singaporeans had the longest life expectancy of any country at 84.8 years. Women can expect to live an average of 87.6 years with 75.8 years in good health. The averages are lower for men.[479] Singapore is ranked 1st on the Global Food Security Index.
Financial Considerations: Medical professionals often face significant student loan debt, which can impact career choices and personal life decisions.
Technological Integration: The integration of technology like telemedicine and electronic health records is transforming how doctors provide care and stay updated with medical advancements.
Communication In Medicine: Effective communication skills significantly enhance doctor-patient relationships and improve treatment outcomes, emphasizing their importance alongside medical knowledge.
In the fast-paced and ever-evolving world of medicine, doctors and residents commit to a lifelong calling. These dedicated individuals spend countless hours honing their expertise, driven by a deep commitment to patient care and medical excellence. While the white coat and stethoscope symbolize readiness and a passion for their practice, the reality of their journey is far more complex, filled with challenges and responsibilities that often play a crucial role in shaping their careers and the care they provide.
This article goes beyond common perceptions, revealing ten surprising facts about doctors and residents that highlight the depth and complexity of their roles. Whether you’re a medical student preparing for the road ahead, an educator nurturing future providers, or a healthcare professional seeking deeper insight, these realities offer a fresh perspective on the field.
Understanding these intricacies fosters greater appreciation, resilience, and professional growth, ensuring that the next generation of physicians is equipped not only with medical knowledge but also with the tools to thrive in both their careers and personal well-being.
Fact 1: Many Doctors Face Student Loan Debt Long Into Their Careers
Becoming a doctor is one of the most rewarding professions, but the financial burden is significant. Many physicians graduate with over $200,000 in student loan debt, impacting career choices and personal milestones. Here are ways that student loan debt can impact medical professionals:
Influences Specialty Decisions: Some choose higher-paying fields over passion-driven specialties.
Delays Major Life Events: Homeownership, marriage, and family planning may be postponed until studies are completed.
Requires Strategic Financial Planning: Understanding repayment options and budgeting is crucial.
Fact 2: Doctors Must Continually Update Their Knowledge
Medicine evolves rapidly, requiring lifelong learning to provide optimal patient care. Continuing education ensures physicians stay updated on the latest research, treatments, and technologies. Here are some reasons why:
USMLE And CME Requirements: Ongoing exams and certifications keep doctors current.
Medical Advancements: New treatments, AI tools, and clinical protocols evolve constantly.
Efficient Learning Strategies: Consistent review of clinical content allows doctors to maintain their medical mastery and mitigate skill decline.
Fact 3: Technology Is Transforming How Doctors Practice Medicine
Technology is revolutionizing healthcare for the better and improving efficiency. Below are some ways technology is changing the healthcare game:
Electronic Medical Records (EMRs): Digitally store and organize patient health information, improving accessibility, documentation accuracy, and care coordination.
Telemedicine: Expands access to remote and underserved populations.
AI And Automation: Enhances diagnostics, workflows, and patient care.
Fact 4: Many Doctors Pursue Research Alongside Clinical Practice
For many doctors, the desire to discover new medical knowledge is as strong as the calling to patient care. Many doctors balance clinical work and medical research to push the field forward.
Medical research:
Advances Evidence-Based Medicine: Research findings shape treatment protocols.
Improves Patient Outcomes: Clinical trials lead to breakthrough therapies.
Strengthens Analytical Skills: Evaluating data sharpens clinical decision-making.
Fact 5: Communication Skills Are As Important As Medical Knowledge
Beyond expertise, strong communication enhances patient trust and treatment outcomes by ensuring clarity, collaboration, and understanding. Below are some communication skills that medical professionals should value:
Clear Explanations: Helps patients make informed decisions.
Interdisciplinary Teamwork: Ensures seamless care coordination.
Active Listening: Strengthens doctor-patient relationships.
Fact 6: The Number Of Female Physicians Is On The Rise
In recent years, the medical field has witnessed a transformative shift as the number of female physicians steadily increases. Women now make up over 50% of U.S. medical school students, creating a more inclusive healthcare environment.
This change not only reflects broader societal advancements but also heralds a new era where diverse perspectives lead to more comprehensive patient care. Here are a few reasons why this trend is a positive force in the medical community:
Enhancing Patient Perspectives: Women in medicine improve representation and inclusivity.
Expanding Leadership Roles: More female doctors are entering executive positions.
Shaping Mentorship And Education: An increasing number of programs support future generations of female physicians.
As more women enter the field, efforts to support career advancement, mentorship, and leadership opportunities continue to grow. These changes contribute to a more balanced healthcare workforce, ensuring that medical education and patient care reflect the diverse needs of the communities they serve.
Fact 7: Residents Are Both Students And Employees
Residents face a tough battle, as they are expected to balance learning with employment. The responsibilities of patient care, combined with a deep, unyielding commitment to mastering the breadth and depth of medical knowledge, create a unique dynamic.
Residents deal with:
Hands-On Experience: Residents manage cases under supervision, participate in medical procedures, and deliver expert care in high-stakes environments.
Long Hours And High Stress: Demanding schedules prepare residents for independent practice.
Balancing Education And Work: Requires strategic planning and smart time management to stay sharp.
At the heart of every successful treatment plan lies a strong doctor-patient relationship. This dynamic significantly impacts treatment outcomes, as trust and communication form its foundation. Here’s why this bond is essential to a positive healthcare experience:
Empathy Improves Patient Engagement: Positive experiences with doctors encourage patients to follow treatment plans accordingly.
Communication Enhances Understanding: Simplified explanations of medical conditions and solutions lead to informed decisions.
Trust Strengthens Compliance: Patients are more likely to return for follow-ups and engage in routine check-ups when they trust their healthcare provider.
Developing effective communication and interpersonal skills allows physicians to foster meaningful connections with their patients. When patients feel understood and respected, they are more likely to adhere to medical advice and treatment plans, ultimately leading to improved health outcomes.
Fact 9: Wellness Programs Are Becoming More Common In Medical Training
The rumors are true: Becoming a doctor is an incredibly long and arduous process. Thankfully, in recent years, wellness programs have been developed to support students and residents with healthy coping mechanisms. These initiatives, including the ones listed below, are a testament to the growing recognition of the demanding pressures faced by medical students and residents and their impact on mental health and overall well-being.
Mental Health Support: Resources such as counseling help prevent burnout.
Work-Life Balance Strategies: Encouraging self-care and mindfulness.
Peer Support Networks: Strengthening community and resilience.
Fact 10: Global Health Opportunities Are Available To Doctors And Residents
Joining global health initiatives allows medical professionals to see firsthand the different healthcare challenges that occur worldwide. This experience can be pivotal in developing resilience and adaptability, skills that are crucial in any medical setting. For residents, these opportunities can be eye-opening, offering real-world applications of their clinical skills in diverse environments. Here’s why global opportunities can be beneficial for the careers of doctors and residents:
Exposure To Diverse Medical Environments: Broadens clinical expertise and adaptability to different clinical settings.
Develops Problem-Solving Skills: Teaches current and aspiring healthcare providers how to work with resource-limited care strategies.
Strengthens Public Health Impact: Contributes to underserved communities worldwide.
These opportunities enrich one’s medical expertise and broaden perspectives on health disparities, resource management, and cultural sensitivity.
Final Thoughts
The road to becoming a doctor is filled with challenges, sacrifices, and unexpected realities, yet it remains one of the most enriching careers. Understanding these crucial facts about doctors fosters greater empathy and appreciation for those dedicated to medicine. While the path is demanding, each step brings the opportunity to grow, refine skills, and make a meaningful impact on patient care.
By embracing a structured and comprehensive approach to medical education, future providers can develop true mastery. Investing in both clinical knowledge and personal well-being ensures not only success in training but also longevity and fulfillment in practice. Whether you’re a medical student, resident, or educator, every effort you make strengthens your ability to provide exceptional, compassionate care, shaping the future of healthcare for the better.
REALLY IN LOVE Written by: Benjamin Kheng Produced by: Benjamin Kheng, Evan Low Performed by: Benjamin Kheng Mixed & Mastered by: Charlie Kurata Spatial Audio Master by: Luke Nicholas Foo
Team from KKH, SGH aims to develop screening tool to identify women at risk of premature births
SINGAPORE – Her son weighed just 700g when he was born at 24 weeks after she spent the two weeks prior in hospital due to vaginal bleeding and cervix dilation.
Ms So Bee Leng’s son, Ethan Ang, was born in 2017 with multiple disabilities stemming from his extreme prematurity. At seven days old, he underwent his first major surgery when his intestines were operated on.
For the next five years, he underwent four more major operations, which included implanting a cochlear hearing device, laser eye surgery to help with his vision and placing a feeding device through his belly to the stomach.
It is currently a challenge to identify mothers at risk of giving birth to premature babies as the only gauge is when mothers have had previous preterm births, like Ms So, said Professor Teoh Tiong Ghee, director of maternal and child global health and care transformation at KK Women’s and Children’s Hospital (KKH).
To proactively reduce and prevent prematurity, a 10-member team of doctors specialising in newborn care and high-risk pregnancies from KKH and Singapore General Hospital (SGH) will start work on a new Preterm Pregnancy Prevention Programme in October.
The team aims to create a national database of all preterm pregnancies to identify risk factors, and then use this information to develop a screening prediction tool that can accurately assess the risk of preterm pregnancies.
A baby born before 37 full weeks of pregnancy is considered to have been born preterm or prematurely. A preterm baby’s organs may not be fully developed.
A full-term pregnancy typically lasts about 40 weeks, and babies’ birth weights typically range from 2.5kg to 4.5kg.
Globally, 13.4 million babies – 10 per cent of all births – are born prematurely each year and one million die from preterm complications.
Prematurity is the leading cause of death for children under five.
In 2023, 8.2 per cent of births in Singapore were premature, slightly lower than the 8.8 per cent recorded in 2014.
Recalling the dilemma she faced when told she might deliver early and her baby would develop health complications, Ms So, 38, said: “I was given the choice to either terminate the pregnancy or continue with bed rest in the hospital until I gave birth.
“After weighing the pros and cons, and discussing with my husband, we decided to carry on and accept whatever may come in the future.”
When she conceived again in 2023, her doctor told her she was at risk of another premature delivery. She was referred to the Preterm Birth Clinic at KKH’s Stork Centre, where she was closely monitored.
She underwent a procedure to stitch her cervix – the birth canal opening – when she was 12 weeks along, paving the way for the full-term birth of her daughter, Alysha Ang, at 38 weeks.
Called a cervical cerclage, the procedure is done to help the cervix hold a pregnancy in the womb to prevent preterm birth.
Dr Ilka Tan, a senior consultant at KKH’s department of maternal foetal medicine who oversaw Ms So’s care during her second pregnancy, said that infants are able to survive outside the uterus at 24 weeks.
She added that though there are rare cases of infants surviving when born at 22 or 23 weeks, the “outcome is still not very good” for these babies.
Acknowledging that there have been reports from around the world of some babies born around 22 weeks who have survived, she said: “Those are single anecdotal cases, but it’s not the norm.”
If diagnosed through screening and predictive tests early, mothers who are at risk of preterm births can undergo various treatments to help them bring the pregnancy to term, Dr Tan said.
These include taking the hormone progesterone and getting a cervical cerclage.
The Preterm Pregnancy Prevention Programme will use information collated to study common characteristics among women who deliver prematurely. This in turn can be used to develop a prediction tool to identify expectant mothers who are at risk of preterm births early, so that preventive measures can be taken.
“What we’re trying to do is to get all these demographics, and use biomarkers from blood and cervical length measurements, to try to predict each woman’s personalised risk so as to target with specific therapy,” said Prof Teoh.
The programme is funded by a $500,000 grant from Far East Organization.
Besides the child potentially suffering long-term health consequences and an increased risk of disability and developmental delays, the parents and the rest of the family experience long-term stress too, Prof Teoh noted.
“Some have to stop work to look after the kid. So not only does it have a psychological impact on the family, it’s got a big financial impact as well,” he added.
Dr Tan also leads the Preterm Birth Clinic at KKH that provides specialised care for women who may have a higher risk of having premature babies.
The clinic began operations in July 2021 and had 100 patients that year. In 2024, 402 patients were referred to the clinic from January to September.
Ms. So said she received personalised care and attention at the Preterm Birth Clinic to help her carry her second child to term.
“I was seen by the same doctor – it wasn’t random. So I felt well-looked after and relieved. I was assured that there was a plan to help me, and that was important.”
Skin-to-skin cuddling with a parent has lasting cognitive benefits for premature babies, according to a new Stanford Medicine study. Preemies who received more skin-to-skin contact, also known as kangaroo care, while hospitalized as newborns were less likely to be developmentally delayed at 1 year of age, the study found.
The research, which was published online July 11 in The Journal of Pediatrics, showed that even small increases in the amount of skin-to-skin time made a measurable difference in the babies’ neurologic development during their first year.
“It’s interesting and exciting that it doesn’t take much to really improve babies’ outcomes,” said the study’s senior author, Katherine Travis, Ph.D., who was an assistant professor at Stanford Medicine when the study was conducted and is now an assistant professor at Weill Cornell Medical School and Burke Neurological Institute.
The study’s first author is Molly Lazarus, a clinical research coordinator in pediatrics previously at Stanford Medicine and now at Weill Cornell Medical School.
The intervention is simple: With the baby only in a diaper, a parent holds the baby on their chest, next to their skin. But because hospitalized preemies are small and fragile, and often hooked to lots of tubes and wires, holding the baby can seem complicated. Parents may need help from their baby’s medical team to get set up. That work is worth it, the study showed.
“It didn’t matter if the baby was from a high- or low-income family; the effects we found were the same. And it didn’t matter if the baby was sicker or less sick—both responded to this treatment,” Travis said.
Neurological complications are challenging
Over the last 50 years, preemies’ survival rates have improved dramatically thanks to better treatments for many of the complications of prematurity, which is defined as being born at least three weeks early. For instance, neonatologists have developed effective approaches to help preemies breathe, even with immature lungs, while in the neonatal intensive care unit.
But premature birth still leaves babies at risk for long-term neurodevelopmental problems, including developmental delays and learning disabilities. Doctors and families have long hoped for treatments they could use during the newborn period to prevent such challenges.
“Ultimately, we want our patients to be healthy kids who can achieve the same milestones as if they didn’t come to the NICU,” said study co-author Melissa Scala, MD, clinical professor of pediatrics. Scala is a neonatologist who cares for preemies at Lucile Packard Children’s Hospital Stanford.
“Our finding legitimizes skin-to-skin care as a vital intervention in the neonatal intensive care unit to support our goal of getting that child out of the hospital, able to learn and develop,” Scala said.
Skin-to-skin care was first used in low-income countries to boost babies’ survival, where it is often used for healthy infants born after full-term pregnancies. In rural or impoverished areas, it is an essential way to keep newborns warm, promote parent-child bonding and facilitate the start of breastfeeding.
It’s been slower to catch on in the United States, especially for premature babies, who generally receive high-tech intensive care. But a growing body of research suggests that the practice has benefits for preemies’ brains, possibly because it could offer some of the same developmental inputs they would have received if they had not been born early.
More skin-to-skin was better
The research team reviewed medical records for infants who were born very prematurely, meaning at least eight weeks early, and were cared for at Lucile Packard Children’s Hospital Stanford between May 1, 2018, and June 15, 2022. Nurses in the hospital’s NICU had begun making notes in patients’ medical charts about developmental care practices, including the amount of time parents held babies skin-to-skin, shortly before the study began.
The study included 181 preemies who did not have genetic or congenital conditions known to affect neurodevelopment and who had received follow-up evaluations after they left the NICU. All very premature babies are eligible for care through California’s High Risk Infant Follow-Up program until age 3. The program provides developmental testing and connects families to appropriate therapists if their children have developmental delays.
The study used records from follow-up evaluations that the babies received at 6 and 12 months’ adjusted age, meaning their ages were corrected to account for how early they were born.
The evaluation included measures of visual-motor problem solving in standard tasks (such as dropping a cube into a cup) and expressive and receptive language skills (such as turning to see where the sound of a bell is coming from).
In addition to accounting for infants’ gestational age (how early they were born), the outcomes were adjusted for families’ socioeconomic status and for four common complications of prematurity: bronchopulmonary dysplasia, a breathing complication; brain hemorrhage, or bleeding; sepsis, an infection of the bloodstream; and necrotizing enterocolitis, an intestinal condition.
The infants in the study were born, on average, at about 28 weeks’ gestation, or about 12 weeks before their due dates. They stayed in the hospital for an average of about two and a half months.
Babies in the study averaged about 17 minutes a day of skin-to-skin care, usually in sessions lasting more than an hour but occurring less than two days per week. Seven percent of families did not do any skin-to-skin care, and 8% did more than 50 minutes per day.
Small increases in the amount of skin-to-skin care were linked to large differences in 12-month neurodevelopmental scores. An average of 20 minutes more per day of skin-to-skin care was associated with a 10-point increase on the scoring scale used for neurodevelopment. Similar to an IQ test, the scale has an average of 100 points; a score of 70 or less suggests significant developmental delays.
The frequency and duration of skin-to-skin contact predicted 12-month cognitive scores even after controlling for possible confounding factors, including the infant’s gestational age and medical complications, and the family’s socioeconomic status and frequency with which they visited the NICU.
How does it work?
Although the study was not set up to explore how skin-to-skin care benefits babies’ brains, the researchers have some educated guesses.
“We think of the womb as our benchmark for preterm babies. In utero, a fetus is physically contained, listening to the maternal heartbeat, hearing Mom’s voice, probably hearing her digest her sandwich,” Scala said. “In the NICU, they’re not next to anybody, and they hear the fan in the incubator; it’s a very different environment. Skin-to-skin care is probably the closest we can get to mimicking the womb.”
Parents can also benefit from skin-to-skin care, and this in turn may benefit their newborns, the research team said.
“The environment of the NICU is very stressful for parents and babies, and skin-to-skin care may buffer that,” Travis said, noting that it is not unusual for parents with a very tiny, sick baby to develop post-traumatic stress disorder.
In addition, many preemies are not developmentally ready to breastfeed, and skin-to-skin care can provide an alternate way to promote bonding between parents and babies.
The researchers hope their findings will motivate medical teams to help parents provide skin-to-skin care in NICUs across the country and will encourage parents by showing them the long-term benefits of this simple but important technique.
Packard Children’s recently expanded its infant developmental care program by hiring neurodevelopmental nurse practitioners, more physical and occupational therapists, a psychologist, and child life and music therapy experts for their NICU and intermediate care nurseries. The expanded team can make customized developmental care plans for high-risk infants.
Scala hopes other hospitals will follow suit.
“I would love for people to see this as part of the medical plan, not just something nice we’re doing, but to be really intentional about it,” Scala said. “Our findings underscore the value of having parents on the intensive care unit, doing this important part of infant care.”
Imagine giving birth at 22 weeks—facing the uncertainty, the emotional rollercoaster, and the challenges of an 8-month NICU stay. For Asma, this journey was life-changing, but it also ignited her passion for advocacy, helping other parents navigate the NICU experience with confidence and strength. Join us as Asma shares: ✅ Her raw & real experience as a NICU mom to baby Cylia Maria ✅ The emotional & logistical challenges of a long NICU stay ✅ The transition home—what she wishes she knew ✅ How sharing her story has fueled her passion for advocacy & parent empowerment ✅ Guidance for parents: questions to ask & how to take an active role in their baby’s care.
It can be very stressful having a baby in the NICU. During this time, it is helpful to include siblings as much as possible; to explain in simple terms what is happening with your new baby; to reassure them that they have not caused the baby to be early, sick, or small; and to remind them that they are not the source of your current worries. Most of all, you should reserve special time just for them, and remind them daily of your constant and unconditional love. More than ever, they need to feel secure, valued, safe, and loved by you and others.
Platypus Media is proud to offer a number of NICU sibling support resources. We hope these will be meaningful and useful for families experiencing the difficulty of having a child in the NICU.
The Come Home Soon coloring book series (available for baby boys and girls, in both English and Spanish) will help you guide your children to an understanding of why their baby sister or brother is in the NICU, and what they can do to help.
Rich and Creamy for Our Preemie, by Naomi Bar-Yam, ACSW, Ph.D., available in English and in Spanish, is a coloring book about how the NICU, milk banks, and families work together to help preemies.
Here is a list of other NICU sibling support resources:
Hand to Hold sibling support webpage (www.HandToHold.org) offers sample activity pages and NICU video tour.
No Bigger than My Teddy Bearby Valerie Pankow describes the NICU experience through the eyes of a new big brother.
My Brother is a Preemie/My Sister is a Preemie:A Children’s Guide to the NICU Experienceby Abraham R. Chuzzlewit & Dr. Jos. A. Vitterito II gives a child-friendly introduction to the NICU.
The Invisible Stringby Patrice Karst reassures children that even when loved ones are apart, they are always in each other’s hearts.
Keep reading for a list of organizations that help preemie families…
Different Dream serves as a gathering place for parents with special needs children.
Hand to Hold provides resources and support to parents of preemies, babies with special health care needs and new parents who have lost a baby.
Human Milk Banking Association of North American provides information and resources on donor milk banking for parents and health care providers. It also sets safety guidelines for all non-profit mothers’ milk banks in North America.
Kangaroo Mother Care promotes skin-to-skin contact, a universally available and biologically sound method of care for all newborns, and preemies in particular.
La Leche League International is a mother-to-mother breastfeeding support organization. They are a source of information and firsthand accounts related to providing preterm babies with breastmilk.
Managing the Neonatal Intensive Care Unit is an article from the Loyola University of New Orleans’ online nursing resource center. A great resource for students, professionals, and even parents of babies in the NICU.
March of Dimes (MOD) has a wealth of information about the NICU. They support an online community especially for NICU families. March of Dimes NICU Family Support programs operate in many NICUs. (Also available in Spanish.)
NICU Parent Support Site provides information, resources, and encouragement to reassure and support NICU parents.
Prematurity strives to support preemie parents by providing information on prematurity and preemie care.
Preemie Parent Alliance(PPA) represents a number of organizations that help support the parents of preemies and strives to improve the quality of the care they provide.
Preemie World brings together parents and professionals in the NICU. They strive to educate and help make the transition to home easier for everyone.
Ronald McDonald House serves as a home away from home for families with children receiving medical treatment. Families can do laundry, eat freshly cooked meals, sleep in private rooms, and gain/give support with other families.
Supplemental Security Income (SSI) and Medicaid Programs provide financial assistance for NICU medical expenses. Eligibility for assistance is determined by a baby’s birth weight rather than an income. You must apply for these programs shortly after your baby is born. Ask your social worker or care manager for assistance.
WIC (Women, Infants, and Children) provides nutritious foods to supplement diets, information on healthy eating, and referrals to health care for women, infants, and children up to 5 years. Even if you have been denied Medicaid due to financial reasons, you might still qualify for WIC.
Fetal heart rate (FHR) patterns are a critical tool for assessing a baby’s well-being during pregnancy and labor. Nurses must understand how to interpret these patterns to ensure safe care. Here are the key takeaways:
Baseline FHR: Normal range is 110-160 bpm. Below 110 bpm (bradycardia) or above 160 bpm (tachycardia) may signal distress.
Nurses must act quickly on abnormal patterns by repositioning the mother, administering oxygen, or preparing for emergency delivery. Accurate monitoring, documentation, and clinical judgment are essential for ensuring the safety of both mother and baby.
The moonlighter had just returned with our dinners when the code alarm sounded. Almost simultaneously, our pagers went off “Code infant 3312.” We all knew who it was. The 23-week gestation, two-day-old baby had coded earlier in the afternoon and had been doing poorly since. Oxygen saturations were in the low 80s despite maximal support, and blood pressures were marginal on dopamine, dobutamine, and epinephrine drips. Upon entering the room, we found the infant with saturations in the 40s and a heart rate in the 50s. We quickly assumed our positions around the warmer. The resident began chest compressions, the respiratory therapist hand bagged, the fellow at the head of the bed assessed the airway and ordered fluid pushes and medications, the bedside nurse administered the medications, and I, the attending physician, oversaw it all. The nursing staff also rapidly began their roles, one opening the crash cart and drawing up drugs, another charting, and multiple others observing and ready to assist if needed.
We quickly fell into our all-too-familiar routine, counting “one, two, three” for chest compressions, followed by “breath.” Over and over again. “Ten mils normal saline,” said the fellow, followed by “epi, point 0 five” every five minutes. The intern took over the chest compressions after about 10 minutes, but the cadence remained the same. Blood was bubbling up the endotracheal tube, indicating the presence of a pulmonary hemorrhage. A nurse was dispatched to retrieve emergency-release blood from the blood bank. The saturation and heart rate were steadily falling.
The mother was literally rolling on the floor, wailing, “Save my baby! Save my baby!” over and over again.
Despite several rounds of fluids and epinephrine plus a push of the blood, the baby continued to deteriorate. I knelt beside the mother, put my hand on her shoulder, and asked her to listen. She immediately stopped her wailing and looked me in the eye. I told her that her baby was dying, that we were going to stop CPR as it was not working, and that her baby’s brain had been irreversibly damaged. She nodded in agreement.
“Stop,” I said. The scene instantly shifted from the hustle and bustle of a code to a stony silence pierced only by the sobs of the mother whom the nurses had assisted into a recliner chair. The monitor was turned off, the ventilator and lines were disconnected, syringes and other debris were removed from the bed, and the baby was wrapped in a blanket and placed in mom’s arms. The nurses began their familiar postmortem care routine. The fellow auscultated the baby’s chest and confirmed the death.
We returned to the workroom and ate Chinese takeout. I had cashew shrimp. I conducted a debrief during our meal, asking everyone how they felt. The intern was visibly shaken, with a tear trickling down her cheek. It was July, and this was the first death of a patient in her charge since she had become a real doctor. “His life slipped through my hands when you told me to stop,” she said. One of the upper-level female residents hugged her as she sobbed for a while before regaining her composure and resumed picking at her food.
For myself and the fellow, this death was one of many, but each death is new all over again and is a fresh reminder of our human frailty.
Few outside our world would understand a situation like this. We were eating while a baby had just died and a mother was grieving. For her, life had just changed forever. For us, we had to nourish ourselves to have the strength to continue caring for the living. Nothing taught in medical school can prepare one for these moments. They must be experienced first-hand, processed, and reflected upon. Doing so is what gives us the strength to move forward.
4 actions health leaders must take to show doctors they are valued
It takes more than words to show gratitude to physicians. These concrete steps can help doctors feel valued and protect against burnout.
Physician Health – By Georgia Garvey, Contributing News Writer Mar 18, 2025
Good health care leaders realize that physicians need more than free food and thank yous to thrive. Well-meaning expressions of appreciation that do not address the root cause of burnout or stress cannot alleviate physicians’ stress or stave off burnout the way that truly feeling valued can.
But it takes more than knowledge to change a work environment—it takes concrete action.
“Many leaders know the importance of teamwork and communication,” said Jill Jin, MD, MPH, an internist and senior physician adviser for professional satisfaction and practice sustainability at the AMA. “But where they kind of struggle is, how do you actually support the individual at a level that is meaningful for them?”
Dr. Jin discussed “muffin rage,” a phrase that came about as a result of a 2021 Los Angeles Times op-ed by Jillian Horton, MD, when she—deep in the throes of work-related burnout and distress—happened upon a “resident appreciation” event handing out muffins.
“Muffin rage is what we feel when there is a vast chasm between our actual needs and what another person or an institution thinks we need,” Dr. Horton wrote.
Dr. Jin spoke alongside Jane Fogg, MD, MPH, physician director of organizational transformation for the AMA, in a recent webinar on how health care organizations can make doctors feel valued, which highlighted an AMA STEPS Forward® playbook on the topic.
During the event, Drs. Jin and Fogg touched on some of the ways that health systems, organizations and leaders can take actions that will make physicians feel valued in a way that avoids muffin rage, a crucial effort with implications for physician well-being, burnout and even the quality of patient care.
In fact, physician turnover can cost organizations anywhere from $500,000 to $1 million or more for every physician who leaves.
“Aside from it being the humane thing to do, there is also a financial benefit—a business case—for investing in your people,” Dr. Jin said.
For those looking to lessen the load on physicians, a key avenue to pursue is helping them understand the crucial role they play in their organization. Dr. Jin pointed out that research shows feeling valued correlates strongly with lower burnout rates, mentioning a 2022 study published in JAMA Health Forum that found physicians who felt valued had a 37% burnout rate, compared with 69% for those who did not.
As the leader in physician well-being, the AMA is reducing physician burnout by removing administrative burdens and providing real-world solutions to help doctors rediscover the Joy in Medicine™.
Help physicians know their worth
Once the importance of feeling valued as a key mitigator for physician burnout has been understood, Drs. Jin and Fogg said, the next step is determining what, exactly, helps physicians know and understand their worth in an organization.
Instead of superficial gestures like the one described in Dr. Horton’s piece, Dr. Jin said there are ways to effectively communicate gratitude to physicians. Those ways have much more to do with actions than with words.
Some key ways to show doctors they are valued, as described by Drs. Jin and Fogg, were to support:
Schedule flexibility and autonomy.
Paid time off (PTO).
Professional development.
Individual resilience and self-care.
Care during and after trauma.
Make work-life balance a priority
Often it can be difficult to justify costly changes aimed at improving physicians’ work conditions, said Dr. Fogg, but overwork and lack of autonomy in matters such as scheduling result in burnout, which is even more expensive.
“Productivity is a pressure that we often feel because of falling revenues across the health care landscape,” she said. “With pressure to fill our schedules, we can lose valuable time for our continuity patients. This tension between being productive and being available to our own patients often lies in how we design and manage our schedules.”
The key, Dr. Fogg said, is giving doctors the ability to “co-design the scheduling processes with their operational team. Make sure you partner with operational leaders to have a physician voice in designing the optimal schedule system for patient access, continuity, and work life balance.”
PTO is another area of concern for organizations looking to create a culture of value, Dr. Jin said.
Health care leaders can be role models in taking time off themselves, and organizations can proactively block off vacations, celebrate time off and resist the impulse to praise working while out of the office. Physicians’ responsibilities should also be fully covered when they’re on vacation, and compensation models and appointment schedules should take PTO into account.
Support the physician as a person
To show a physician that they are more than just a cog in the machine, their professional development must be supported, recognizing their individual aspirations and passions beyond the clinical practice of medicine.
“Feeling valued means the people around you—your supervisor in particular—know who you are, what excites you and what makes you passionate” outside the confines of the clinic or hospital corridor, Dr. Fogg said. “Asking physicians about their long-term goals and offering opportunities to get involved in a variety of activities outside of clinical practice can create a stronger sense of feeling valued. Some opportunities for growth include teaching, research, process improvement initiatives, leadership, community engagement and more.
And, said Dr. Jin, while “self-care” is not a replacement for—and should not be the major focus of—systemic efforts to reduce burnout, organizations can support an individual’s resilience by helping physicians set boundaries, prioritize tasks and limit their distractions. Leadership also should provide resources for and support physicians in self-care, promote collegiality and create spaces for breaks.
Additionally, the credentialling process should remove questions about mental health care so they don’t discourage physicians from seeking care if needed.
“Burnout is not a sign of mental illness, but there is a lot of overlap that happens when we are severely distressed by the way in which we’re practicing and what we’re witnessing in our practices,” she said.
For more information on this and other topics, explore the AMA STEPS Forward open-access toolkits and playbooks, which offer innovative strategies that allow physicians and their staff to thrive in the new health care environment. These resources can help you prevent burnout, create the organizational foundation for joy in medicine and improve practice efficiency.
Combat physician burnout
Event: American Conference on Physician Health (ACPH) Sept. 11-13, 2025, focusing on steps organizations can take to improve physician well-being
CME: How health systems can reduce physician burnout
Calculate: See the cost of physician burnout to your organization
Video: Latest trends in physician burnout by specialty
Question Do individuals born preterm have a higher risk of short-term and long-term mortality compared with those born at term?
Findings In this cohort study of 4 998 560 births, individuals born preterm had a higher risk of mortality from birth to age 36 years, with the highest risk observed from birth through early childhood. The risk of mortality varied by gestational age at birth and was more pronounced at lower gestational ages.
Meaning The findings of this study suggest that preterm birth is associated with increased risk of death from infancy to adulthood.
Abstract
Importance Preterm birth (PTB) is a leading cause of neonatal mortality. However, evidence on mortality beyond the neonatal period is limited, especially in North America.
Objective To examine associations of PTB with all-cause and cause-specific mortality from birth through 23 to 36 years of age.
Design, Setting, and Participants This population-based matched cohort study of live births in Canada included individuals born between January 1, 1983, and December 31, 1996, and followed up until December 31, 2019. Data were analyzed from June 1, 2023, to April 30, 2024.
Exposure PTBs, between 24 and 37 weeks’ gestation (with gestational age [GA]-specific subcategories of 24 to 27 weeks, 28 to 31 weeks, 32 to 33 weeks, and 34 to 36 weeks) compared with term births (37-41 weeks’ gestation).
Main Outcomes and Measures All-cause mortality and cause-specific mortality were the main outcomes. Risk differences (RDs) and risk ratios (RRs) were estimated for all-cause mortality using log-binomial regressions and hazard ratios were estimated for cause-specific mortality using Cox proportional hazards regression models (censoring individuals who died from other causes) within prespecified age intervals (ages 0-11 months and ages 1-5, 6-12, 13-17, 18-28, and 29-36 years). Observed confounding was accounted for using coarsened exact matching on baseline characteristics.
Results Of 4 998 560 births (54.2% male), 6.9% were born preterm (with GA-specific subcategories of 0.3% born at 24-27 weeks, 0.6% at 28-31 weeks, 0.8% at 32-33 weeks, and 5.1% at 34-36 weeks). During a median of 29 years of follow-up, 72 662 individuals died (14 312 born preterm and 58 350 at term). PTB was associated with an increased risk of death in all age intervals, with the highest RDs and RRs from birth through infancy (ages 0-11 months) (RD, 2.29% [95% CI, 2.23%-2.35%]; RR, 11.61 [95% CI, 11.09-12.15]) and in early childhood (ages 1-5 years) (RD, 0.34% [95% CI, 0.31%-0.36%]; RR, 2.79 [95% CI, 2.61-2.98]) and the lowest RDs and RRs among those between ages 18 and 28 years (RD, 0.07% [95% CI, 0.04%-0.10%]; RR, 1.13 [95% CI, 1.07-1.19]). We identified increased risks of mortality associated with several causes, including respiratory, circulatory, and digestive system disorders; nervous system, endocrine, and infectious diseases; cancers; congenital malformations; and conditions originating in the perinatal period. No associations were found for external causes of deaths. Associations by GA categories suggested lower risks with higher GA.
Conclusions and Relevance The findings of this population-based matched cohort study suggest that individuals born preterm were at an increased risk of death from birth until their third and fourth decades of life, with higher risks as GA decreased. Some of these associations may have been partly due to underlying health determinants that affected PTB and mortality. These findings suggest that PTB should be recognized as a risk factor for mortality and could inform preventive strategies.
1Department of Neonatology, University Hospitals Dorset NHS Foundation Trust, Dorset, United Kingdom
2Department of Development and Regeneration, KU Leuven, Leuven, Belgium
3Department of Pharmaceutical and Pharmacological Sciences, KU Leuven, Leuven, Belgium
4Department of Hospital Pharmacy, Erasmus MC, Rotterdam, Netherlands
Introduction
Neonates and infants are commonly referred to as “therapeutic orphans” due to the overall scarcity of therapeutic interventions that have been developed and tailored to their needs and specific characteristics (1, 2). This is well known by care providers and researchers active in this field, but is perhaps less on the radar of authorities, funding bodies or the broader public. There is significant health inequity when comparing newborns to other age populations in terms of specific drug and device development and therapeutics (1, 2). In addition there are health inequities in the provision of neonatal care globally which require special attention in terms of improvement (3).
Bronchopulmonary dysplasia, neonatal seizures, poor growth, necrotizing enterocolitis (NEC) and short bowel, hypoxic-ischemic encephalopathy, retinopathy of prematurity (ROP), neonatal infections and sepsis hereby serve as a non-exhaustive list of “orphan conditions” in need of more equity, through adequately and urgently funded research and improvement.
The good news is that there have been increased efforts, in recent years, by researchers and regulatory bodies to focus on the provision of drugs, devices, and treatment modalities tailored for neonatal use, while further advocacy remains an obvious need (2, 4, 5). This brings perspective and explains the initiative taken to organize a focused research topic on what is on the horizon as well as recent advances.
Overview of the topics covered
We targeted emerging or new aspects related to monitoring, diagnostics and therapeutics in neonatal care for the current research topic. Fortunately, this research topic was perceived as very relevant by the research community, as 135 authors expressed their interest as contributors, resulting in 20 accepted papers. This serves as a signal of the importance to continue to work on this topic.
Post-hoc, and in a somewhat arbitrary way (because of overlap in these subcategories) these papers were subdivided by the editors into different subcategories, with focus on (1, 5 papers) perinatal biomarkers in blood and urine and how these relate to or predict outcomes, (2, 6 papers) adaptations of existing and newly emerging equipment in neonatal units, (3, 3 papers) needed advances in pharmacotherapy, (4, 3 papers) machine learning or deep learning applications in neonatal care, and finally, (5, 3 papers) underreported aspects of contemporary NICU care, with a focus on the holistic nature of care for the infant and the family.
Perinatal biomarkers in blood and urine and how these relate to or predict outcomes
Two papers focused on biomarkers related to gestational diabetes, with reflections and data on maternal and neonatal outcomes. Postnatal maternal levels of glycated albumin and hemoglobin A1c in mothers of large-for-gestational-age (LGA) informed us of the relevance of accurate diagnosis during pregnancy. This is because postpartum women without diagnosis during pregnancy had higher glycated albumin values, associated with LGA and associated complications (Železnik et al.). Interestingly and related to this paper, Yin et al. reported on a untargeted metabolomics study in women with gestational diabetes, with the recommendation of a maternal serum metabolite panel to forecast neonatal adverse outcomes (hypoglycemia and macrosomia) (Yin et al.).
Other papers focused on the use of vitamin D, acid-base and biomarkers associated with fetal growth restriction with impaired neurodevelopmental outcome. In a cohort of 217 preterm neonates, a multivariate regression analysis identified antenatal steroids as protective, and lower birth weight, duration of ventilation, sepsis and the serum 25-(OH)D vitamin as risk factors to develop ROP (Yin et al.). Musco et al. reported on a systematic review on blood biomarkers indicating risks of adverse neurodevelopmental outcome in fetal growth restricted infants (Musco et al.). While the authors retrieved some data on neuron specific enolase and S100B, the overall conclusions reflect a call for further research. Finally, an association between lactate levels in umbilical cord blood and cerebral oxygenation in preterm neonates was studied as a secondary outcome analysis (Dusleag et al.). In non-asphyxiated preterm neonates with respiratory support, lactate levels were negatively associated with cerebral and arterial oxygenation. In term neonates without respiratory support, no associations were observed.
Adaptations of existing and newly emerging equipment in our units
In a review on emerging innovations in neonatal monitoring, Krbec et al. concluded that there is an urgent, still unmet need to develop wireless, non- or minimal-contact, non-adhesive technology, capable to integrate multiple signals in a single platform, tailored to neonates (Krbec et al.). Related to this call of action, Svoboda et al. reported on their pilot experience with contactless assessment of heart rate, applying imaging photoplethysmography (Svoboda et al.). Rectal and axillary temperature monitoring on admission were compared in a cohort of preterm (n = 80, <32 weeks gestational age) by Halabi et al., reporting that rectal measurement was likely more reliable in the event of hypothermia (Halabi et al.). Ultrasound-guided measurement of anterior cerebral artery resistive index in the first week of life in 739 preterm neonates (<35 weeks) was not associated with subsequent co-morbidities on admission or during neonatal stay (asphyxia, sepsis, NEC) (Singh Gill et al.). A case series of neurally adjusted ventilatory assist to rescue pulmonary interstitial emphysema in 5 extremely low birth weight infants illustrated the potential value of this ventilatory equipment and strategy and need for further study (Chen et al.). Finally, van Rens et al. compared a conventional to a modified Seldinger technique (a dedicated micro-insertion kit) for peripherally inserted central catheter (PICC) placement, illustrating the relevance of developing “low risk, high benefit” type of medical devices, adapted to the specific needs of neonates (van Rens et al.).
Advances needed in pharmacotherapy
The currently available medicines and dosing regimens in neonatal care are limited and there is an urgent need for improvement in this domain. This was illustrated by articles on sepsis, septic shock and steroids. Inequity in provision of neonatal care across the globe ought to be a major focus of improvement. Gezahegn et al. described the outcome in neonates admitted with sepsis in Harar (Ethiopia). Low white blood cell count, desaturation, preterm birth, absence of prenatal maternal care, and chorioamnionitis were important risk factors for sepsis-related mortality (Gezahegn et al.). Addressing these prognostic factors hold the promise to act as levelers to improve outcomes. A pilot study compared noradrenaline and adrenaline as first line vasopressor for fluid-refractory sepsis shock (Garegrat et al.). Both interventions were comparable to resolve the septic shock, while the overall mortality (13/42, 30%) remained significant, highlighting the need for better diagnostic and therapeutic options. Finally, in a systematic review, outcome of postnatal systemic corticosteroids (hydrocortisone to dexamethasone) were compared as reported in randomized controlled trials (Boscarino et al.). The authors concluded that dexamethasone appeared to be somewhat more effective than hydrocortisone in improving respiratory outcomes, but with inconclusive but relevant concerns on the uncertainties on long-term neurodevelopmental outcome, again highlighting the need for better therapies for prevention and management of chronic lung disease of prematurity.
Machine learning or deep learning applications in neonatal care
Artificial intelligence is a rapidly advancing area with fast evolving clinical applications in healthcare, including in the NICU (6). It is no surprise that the current research topic also contains papers illustrating its relevance to improve our practices and outcomes. Two papers hereby focused on NEC, and a 3rd paper on prediction of significant patent ductus arteriosus (PDA). In a mini-review, Cuna et al. reports on the various pathophysiological processes underlying NEC endotypes, and how artificial intelligence holds the promise to influence further understanding and management (Cuna et al.). An approach to enhance surgical decision making in NEC is illustrated by Wu et al. Based on x-rays from 263 neonates diagnosed with NEC (94 surgical cases), a binary diagnostic tool was trained and validated, with Resnet18 as approach applied (Wu et al.). For PDA, an ultrasound-based assessment of ductus arteriosus intimal thickness in the first 24 h after birth was applied in 105 preterm neonates. A prediction model for closure on day 7 included birth weight, mechanical ventilation, left ventricular end-diastolic diameter, and PDA intimal thickness (Hu et al.). Such models can be considered to better target future study, integrated in a precision medicine approach. Use of AI and big data have the potential to significantly improve our understanding of neonatal conditions and also support neonatal researchers in asking better research questions.
Underreported aspects of contemporary NICU care, holistic care
As part of this research topic, we also accepted papers reporting on the use of music on pain management, on multisensory stimulation to improve maternal milk volume production, and parents’ experiences related to congenital cardiac surgery. All these 3 papers reflect the need for holistic care and to further integrate the perspectives of (former) patients and parents into neonatal practice.
In a systematic review, Ou et al. demonstrated that music is an effective intervention to relief procedural pain (e.g., Premature Infant Pain Profile score) in preterm neonates, as it reduced some markers of stress, and improved blood oxygen saturation (Ou et al.). Multisensory stimulation (audiovisual, or audiovisual + olfactory) compared to a control setting improved maternal milk volume production, with evidence of positive effects of both interventions, even more pronounced if both interventions are combined (Cuya et al.). Finally, a quantitative analysis of parent’s experiences with neonates admitted to NICU with a congenital heart disease reinformed us on the importance of actively focusing on parental experiences of care (Catapano et al.).
From advances in neonatal care to implementation
In our opinion, this research topic nicely illustrates the diversity in ongoing clinical research activities, that all hold the promise to improve our clinical management practices, with the overarching aim to improve neonatal outcomes. There is an urgent need to focus on the current health inequities in the provision of care to neonates (3). The trend towards a “neuro” dedicated NICU care is an illustration on how relevant progress may occur. This progress is based on improved neuromonitoring techniques (7), improved management and precision medicine in the field of anti-epileptic drugs (8), and integrating families as partners in neonatal neuro-critical care and similar improvement programs (9). The good news is that we are already experiencing a shift in the right direction. The neonatal community and all other relevant stakeholders need to work better together to improve the pace and scale of this improvement.
Improvement Project to Reduce Uncontrolled Pain and Improve Staff Satisfaction
Sprecher, Alicia MD; Roeloffs, Kimberly NNP; Czarnecki, Michelle L. APN; Labovsky, Kristen MD; Kissell, Anna PharmD; Hornung, Genesee MSN, RN; Uhing, Michael MD Editor(s): Dudding, Katherine PhD, RN, RNC-NIC, CNE; Nist, Marliese D. PhD, RNC, Section Editors Advances in Neonatal Care 25(1):p 18-27, February 2025. | DOI: 10.1097/ANC.0000000000001234
Abstract
Background:
Postoperative pain management in the neonatal period is an area of high variability and a source of staff dissatisfaction. Pain management is a key component of high-quality care; however, pain assessment in infants is difficult and analgesics can negatively impact the developing brain.
Purpose:
We aimed to improve postoperative pain control for infants in our neonatal intensive care unit (NICU), limit variability in the approach to pain management, and increase staff satisfaction.
Methods:
This project was completed between April 2019 and March 2022 with sustainment tracked through December 2023. Interventions took place in a 70-bed level IV NICU using quality improvement methodology. Interventions included efforts aimed at improving pain assessment as well as development and implementation of a pain management guideline. Outcome measures included frequency of uncontrolled postoperative pain and measures of staff satisfaction. Process measures included compliance with pain assessment cadence and guideline recommendations. Opioid exposure within 24 hours of surgery was included as a balancing measure.
Results:
Pain management was assessed in 811 infants: 392 prior to guideline implementation, 273 during implementation, and 146 during sustainment period. Uncontrolled postoperative pain decreased from 26% pre-implementation to 18% post implementation and into the sustainment period. Staff satisfaction improved from 67% to 83%. These improvements were associated with decreased variability in postoperative pain management and a decrease in postoperative opioid exposure.
Implications for Practice and Research:
The use of a postoperative pain management guideline can improve pain control, decrease drug regimen variability, decrease opioid exposure, and increase staff satisfaction.
In Singapore, where skyscrapers rise and medicine meets innovation, a new kind of wellness journey is unfolding—one led by the smallest among us.
Our Womb Warriors who began life in the NICU are not just survivors—they are thrivers, growing through challenges and emerging with strength forged in the most fragile beginnings. Today, health and wellness for these preemie survivors extends far beyond the hospital walls. It means developmental follow-up, skin-to-skin care, nutrition support, and emotional well-being—not just survival, but quality of life.
Singapore’s approach is inspiring. With personalized risk assessments, neurodevelopmental care programs, and parent-empowering tools like kangaroo care, the wellness journey begins from day one. And studies now confirm what many NICU parents already knew in their hearts: the closeness, love, and presence of family are as powerful as any machine.
As our Warriors grow, their wellness becomes more than a checklist—it becomes a rhythm. Physical therapy. Play. Sensory exploration. Nourishment. Love. And for the parents walking beside them? Wellness looks like deep breaths, long walks, and the quiet courage to ask for help.
Whether your little one is a few months or a few years out of the NICU, this season is a reminder: wellness isn’t a destination—it’s a daily act of love.
Spring into Strength
Spring is a season of becoming—of blooming boldly, stretching softly toward the light, and waking up to what’s possible. For our Womb Warriors, it’s also a reminder that wellness is not about perfection—it’s about progress, presence, and power.
Whether you’re a preemie kid discovering new abilities, a teen navigating your story, or an adult survivor reclaiming your narrative, this season invites you to grow on your terms. Your early beginnings may have been fragile—but your spirit is anything but.
Health and wellness don’t have to look the same for everyone. What matters most is listening to your body, honoring your journey, and celebrating how far you’ve come.
🌸For Kids
Make movement magical—build obstacle courses, splash in puddles, or stretch like your favorite animal.
Explore foods that help you grow strong: yogurt parfaits, rainbow fruit plates, or protein-packed pancakes.
Practice deep breathing with bubbles or belly-breathing “dragon breaths.”
🌱For Teens
Journal your thoughts under a tree or start a mood-boosting playlist for mental clarity.
Try out yoga, trail walks, or a new sport—your strength isn’t defined by speed, but by showing up.
Fuel yourself with purpose: balanced snacks, hydration, and sleep that heals.
🌞For Adults
Redefine strength: maybe it’s finishing a workout, setting boundaries, or resting when you need to.
Revisit your NICU beginnings—use them to empower your healthcare choices and connect with your past.
Create a spring ritual: a morning stretch, a quiet walk, or a personal mantra. Wellness isn’t trendy—it’s transformative.
In Singapore, hospitals are leading the way in early screenings and personalized care to help preemies not just survive, but thrive. That same spirit of innovation and renewal lives in each of us.
So here’s to you—this spring, let’s grow wildly. Heal gently. Thrive loudly. Because once a Neonatal Womb Warrior, always a Warrior—and you are in full bloom.
The Path to Wellness | Alysha Aziz | TEDxHolyTrinitySchool
Wellness is a journey. In this insightful talk, learn about the PATH model: Perception, Analysis, Trial and Error, and Habits, as a framework for achieving personal well-being. This talk empowers audiences to embrace the process and find a path to a healthier, more fulfilling life. Hi everyone, I’m Alysha! I am a student in grade 11 and I’m one of the speakers for TEDEd’s Empowerment event. Having been part of the club since grade 9 and now as president, I’m really excited to share my talk with everyone! I’ll be talking about wellness and taking autonomy over your own mental health. I’m super excited that this is our first charitable event and can’t wait to see you all there!
10-minute guided meditation for kids 🧘 mindfulness for kids 🕊 Bye Bye Worry Balloons🎈 Worry-Free 💛
Relax, breathe, and feel calm with this simple meditation for kids. In this guided meditation for kids, we’ll say ‘bye-bye’ to worries and hello to happy thoughts. ☀️🎈
Would You Rather? Spring Edition! | Fun Fitness For Kids | This or That | Spring Workout | GoNoodle
Mr. Hassell’s Brain Breaks
Exercise your body and mind with this Spring themed brain break! In this fun and engaging workout video, we play a game of “Would You Rather” by picking our favorite Spring choices and performing exercises!! Perfect for a PE warmup, classroom brain break and at home workout!
Written by published children’s author, Jennifer Marino Walters, “Surprising Spring” tells the simple story of the beauty that Spring brings and its many flowering surprises.
Wave House Sentosa located on the sandy beaches of Sentosa is Asia’s only installation in an archipelago of global Wave Houses that stretches from Durban in South Africa, San Diego in California, Santiago in Chile, and Mallorca in Spain. Singapore has long been a crossroads for surfers seeking the perfect waves at beaches around Southeast Asia, however the island itself lacks the giant waves which surfers long for. With its opening, Wave House Sentosa puts Singapore on the global surfer destination map with its perfect and world famous 10′ FlowBarrel wave.
Slovakia, officially the Slovak Republic, is a landlocked country in Central Europe. It is bordered by Poland to the north, Ukraine to the east, Hungary to the south, Austria to the west, and the Czech Republic to the northwest. Slovakia’s mostly mountainous territory spans about 49,000 km (19,000 sq mi), hosting a population exceeding 5.4 million. The capital and largest city is Bratislava, while the second largest city is Košice.
Healthcare in Slovakia has features of the Bismarck, the Beveridge and the National health insurance systems. It has public health system paid largely from taxation. The cost of national health insurance is shared between the employees and the employers. The part of these taxes are paid by the employees as a deduction from theirs wages and the remaining part of these taxes is paid as compulsory contribution by employers. Sole traders pay the full amount of these taxes.
These taxes are managed by health insurance companies. Current healthcare system has 3 health insurance companies, namely Union (12,4%), Dôvera (32,4%) and Všeobecná zdravotná poisťovňa (55,2%)(market share). Všeobecná zdravotná poisťovňa is a state-run insurance company, the other two are private. These insurance companies have contracts with outpatient clinics, hospitals, rehabilitation centres, pharmacies, etc. Despite this, not everywhere and not always the insurance company covers the costs. The costs are not covered for all medicines, or the full price of them. Also, it is not covered dental treatment.
The government pays health insurance for children, students, pensioners, invalids, people performing activities for a church, religious or charitable community, etc.
CR’s experts say it’s much safer for children to wear their winter coat backward and on top of their car seat harness.
“You better bundle that baby up or she’s going to catch a cold!” I knew before I turned around what was happening: The well-meaning lady in the grocery store parking lot wanted to know why my child didn’t have a coat on in her car seat, even though it was the middle of winter.
The reason? Because a bulky coat and a child car seat can be a dangerous combination. As a general rule, winter coats should not be worn underneath a car seat harness because that can leave the harness too loose to be effective in a crash.
Research priorities for preterm lung health research across the lifespan: a community priority setting partnership
Author affiliations – Naomi R Hemy1 Amber Bates1 Belinda Frank2 Anne McKenzie2 Shannon J Simpson1 3
Abstract
Background It is essential to embed patient and public perspectives into every stage of the research journey, including setting the future research agenda. The substantial gaps in our understanding of prematurity-associated lung disease presented a timely opportunity to determine the community’s research priorities.
Objective To conduct a priority setting partnership (PSP) to determine the top 10 research priorities for preterm lung health.
Design We undertook a modified James Lind Alliance methodology comprising three main stages: (1) an idea generating survey with open questions to ascertain the community’s most important ideas for future preterm lung health research, (2) prioritisation survey to distill the main themes into a shortlist of 20 and (3) consensus workshop where participants were tasked with ranking their final top 10. This PSP is reflective of the view of preterm-born individuals, parents of preterm children and healthcare professionals in an Australian healthcare setting.
Results We collated 144 submissions from the idea generating survey from which 27 prioritisation themes were developed. From the 150 prioritisation survey responses, the 20 themes receiving the most votes were taken to the consensus workshop. Participants identified the following top 10: (1) lifelong impacts; (2) interventions, treatments or supports; (3) ongoing lung health follow-up; (4) diagnostic tools, resources and education for primary healthcare providers; (5) resources to inform and empower families; (6) relationship to physical health and developmental issues; (7) preventing and/or treating lung infections; (8) additional supports, resources and research for minority groups; (9) impact on mental well-being; and (10) likelihood of asthma diagnosis.
Conclusion Priorities identified through the PSP will be invaluable in informing future research into prematurity-associated lung disease.
Following important research in neonatology / newborn medicine from around the world
I have written frequently about my concerns with “NDI” as an important measure of neonatal outcomes, indeed, it seems to be often thought of as if it were the only important measure. It has very often been included as part of a composite outcome measure “death or NDI”.
So why am I disturbed about the use of NDI as a primary outcome measure? NDI is itself already a composite measurement, including some indicator of delayed development (most commonly one of the various iterations of the Bayley Scales of Infant Development), some severity of motor disorder expected to be permanent, i.e. Cerebral Palsy, some severity of hearing loss, and some severity of visual impairment. It was a composite invented by neonatologists and follow up specialists as a way of trying to quantify the impacts of adverse cerebral impacts of prematurity. There are many problems with this, both in the actual importance of each component of NDI, and also in the permanence of the finding. For example, most infants with low scores on developmental screening tests at 2 years do not have intellectual impairment at follow up. In the follow up of the CAP trial, for example, only 18% of babies who had a low Bayley score at 18 months (version 2 MDI <70) actually had a low IQ at 5 years (WPSII <70). This is unlike CP, for which a diagnosis at 2 years is very accurate (not 100%, but appears to be about 95% PPV) as a predictor of long term motor dysfunction, but the severity of the problem can vary, especially after a diagnosis at 2 to 3 years, where about 1/3 of infants will change their classification on the GMFCS, either to a higher or a lower score. Visual and auditory impairments seem to be more permanent and invariable, but are a much smaller part of the NDI.
And, of course, combining NDI with death as part of a composite outcome implies that they are equally important, and means that an intervention which decreases death may not be found to be significant is there is an increase in low BSID scores in the survivors (for example).
Do parents of babies who are labelled as having NDI think that their infants are impaired? That is the question asked in a new publication from the follow up centres across Canada (Canadian Neonatal Follow-Up Network, CNFUN). Richter LL, et al. Parental and Medical Classification of Neurodevelopment in Children Born Preterm. Pediatrics. 2025. Over 1000 very preterm infants are involved in the study, and their parents were asked if they thought that their child had a developmental impairment when they attended a follow-up clinic appointment, but before they completed the standardised evaluation. They then had their evaluation and were classified as having no NDI or :
“to have a mild-moderate NDI if they had any 1 or more of the following: CP with GMFCS 1 or 2; Bayley-III motor, cognitive, or language composite scores 70 to 84; hearing loss without requirement for hearing devices or unilateral visual impairment. A child was considered to have a severe NDI if they had any 1 or more of the following: CP with GMFCS 3, 4, or 5; Bayley-III motor, cognitive or language composite scores <70; hearing aid or cochlear implant; or bilateral visual impairment.”
As this table shows, there was poor agreement between what the parents thought, and what the standardised evaluation stated. Most of the disagreements were parents considering their infants to not be impaired, or to be less impaired than the standard classification. There were 185 infants with “severe NDI” according to the definition above, only 23 parents thought their child was severely impaired, in contrast, among the 596 with no NDI, there were 11 parents who found their child to have severe impairment, and 104 thought they had mild-moderate impairment.
Some of the details of the analyses are quite interesting, for example, the small number of infants with serious CP, GMFCS 4 or 5, were mostly considered to have moderate or severe impairment by parents. The cognitive scores of infants who agreed that their infant, with CNFUN defined severe NDI, had at least moderate impairment were lower (median 70) than those who disagreed (median 80).
Many problems faced by families with ex-preterm infants are not captured by “NDI”. This is reflected, I think, by those parents who thought their child was impaired despite not satisfying CNFUN definitions, such infants were much more likely to be using technology at home, and more likely to have been referred for occupational therapy, or to see a psychologist or other therapist. Needing re-hospitalisation also made parent more likely to agree that their infant had an impairment.
Because we haven’t measured some of the things that impact families, such as behavioural disturbances, feeding problems, and sleep disruption, we really don’t know if they are affected by any of our NICU interventions. It wouldn’t surprise me if some interventions, ranging from postnatal steroids to skin-to-skin care or light cycling, might have major impacts on those outcomes. We just don’t know.
What should we do about findings such as these newly published data, and others from the Parents’ Voices project? Defining a single ‘yes or no’ outcome variable is the old-fashioned way of designing research and determining the benefit of an intervention. There are much better ways of comparing outcomes between groups, ways which can take into account the variety of outcomes, and the preferences of parents. It takes some extra work to define the kind of ordinal outcomes which reflect the values of parents and the relative importance of each component, but that is hugely preferable to using composite outcomes which implicitly value each component as being equivalent. Being dead, having a Bayley Cognitive composite of 69, having severe visual loss all qualify as “dead or severe NDI”, but the implications are enormously different.
In the future outcomes we measure should focus on how infants function, and should recognize that the answer to the question “how is your child doing?” is not a dichotomous choice.
Appropriate protein intake is crucial for growth and development in children born preterm. We assessed the effects of high (HP) versus low protein (LP) intake on neurodevelopment, growth, and biochemical anomalies in these children.
Methods
Randomised and quasi-randomised trials providing protein to children born preterm (<37 completed weeks of gestation) were searched following PRISMA guideline in three databases and four registers (PROSPERO registration CRD42022325659). Random-effects model was used for assessing the effects of HP (≥3.5 g/kg/d) vs. LP (<3.5 g/kg/d).
Results
Data from forty-four studies (n = 5338) showed HP might slightly reduce the chance of survival without neurodisability at ≥12 months (four studies, 1109 children, relative risk [RR] 0.95 [95% CI 0.90, 1.01]; P = 0.13; low certainty evidence) and might increase risk of cognitive impairment at toddler age (two studies; 436 children; RR 1.36 [0.89, 2.09]; P = 0.16; low certainty evidence). At discharge or 36 weeks, HP intake might result in higher weight and greater head circumference z-scores. HP intake probably increased the risk of hypophosphatemia, hypercalcemia, refeeding syndrome and high blood urea, but reduced risk of hyperglycaemia.
Conclusions
HP intake for children born preterm may be harmful for neonatal metabolism and later neurodisability and has few short-term benefits for growth.
Impact statement
Planned high protein intake after birth for infants born preterm might be harmful for survival, neurodisability and metabolism during infancy and did not improve growth after the neonatal period.
Protein intake ≥3.5 g/kg/d should not be recommended for children born preterm.
Conclusion (Full Study)
Planned high protein intake in the first weeks after preterm birth had few benefits and may be harmful for survival, neurodisability and biochemical abnormalities in neonatal care. However, there are few data beyond the toddler period and considerable unexplained heterogeneity. Longer-term follow-up and an individual participant data meta-analysis of existing trials, including data on total energy intake, would be helpful to clarify the effects of high protein intake for children born preterm.
Personalized communication with parents of children born at less than 25 weeks: Moving from doctor-driven to parent-personalized discussions
Marlyse F. Haward a, Antoine Payot bc, Chris Feudtner de, Annie Janvier bc
Abstract
Communication with parents is an essential component of neonatal care. For extremely preterm infants born at less than 25 weeks, this process is complicated by the substantial risk of mortality or major morbidity. For some babies with specific prognostic factors, the majority die. Although many of these deaths occur after admission to the intensive care unit, position statements have focused on communication during the prenatal consultation. This review takes a more comprehensive approach and covers personalized and parent-centered communication in the clinical setting during three distinct yet inter-related phases: the antenatal consultation, the neonatal intensive care hospitalization, and the dying process (when this happens). We advocate that a ‘one-size-fits-all’ communication model focused on standardizing information does not lead to partnerships. It is possible to standardize personalized approaches that recognize and adapt to parental heterogeneity. This can help clinicians and parents build effective partnerships of trust and affective support to engage in personalized decision-making. These practices begin with self-reflection on the part of the clinician and continue with practical frameworks and stepwise approaches supporting personalization and parent-centered communication.
Section snippets
Part 1: Antenatal consultation
Current recommendations for the antenatal consultation focus on equalizing knowledge imbalances by providing parents with physician-derived sets of information to facilitate rational, data-driven choices.14 These information sets span short and long-term morbidities, survival and mortality statistics determined by physicians, with little input from parents. Although recommendationssuggest exploring values, they fall short in acknowledging the ‘process’ of relationship building.
Part 2. Communication during the neonatal hospitalization
Parent-centered communications during neonatal hospitalizations follows similar concepts. This section will add how continuity of care and ‘good parenting beliefs’ can help manage uncertainty, hope, and realism. We will consider the case of Ms. Gladwell.
Part 3. Dealing with death: the importance of a stepwise approach
Generally, for babies born at less than 25 weeks, neonatal death occurs relatively early when the infant does not respond to interventions, often within the first 3 days of life for the most immature babies.84 Other babies die when respiratory support is removed after death is judged inevatable, or for quality of life concerns.15 For parents like Ms. Gladwell, when death is not immediate, time permits knowledge to be acquired and values to be clarified influencing how choices are interpreted.
Conclusion
Parents and families will live with these experiences for the rest of their lives. How they remember the communication process and care their infants received depends on their perceptions of the relationships built with clinicians and their ability to ‘justify’ what happened within the context of their values. Behaviors that make them feel disrespected or their infant not valued can leave lasting impressions, whereas trusting partnerships solidifies their roles as parents.
Here’s another video in our Journey Through Medicine series where we talk about what it was like for us to have a child while both completing our medical residencies. There’s never a perfect time to have a child during medical training, but here’s how we made it work. #medicalschool#residency#doctorcouple
Neuroprotective therapies in the NICU in preterm infants: present and future
Nature–Neonatal Neurocritical Care Series – 19 December 2023
Abstract
The survival of preterm infants has steadily improved thanks to advances in perinatal and neonatal intensive clinical care. The focus is now on finding ways to improve morbidities, especially neurological outcomes. Although antenatal steroids and magnesium for preterm infants have become routine therapies, studies have mainly demonstrated short-term benefits for antenatal steroid therapy but limited evidence for impact on long-term neurodevelopmental outcomes. Further advances in neuroprotective and neurorestorative therapies, improved neuromonitoring modalities to optimize recruitment in trials, and improved biomarkers to assess the response to treatment are essential. Among the most promising agents, multipotential stem cells, immunomodulation, and anti-inflammatory therapies can improve neural outcomes in preclinical studies and are the subject of considerable ongoing research. In the meantime, bundles of care protecting and nurturing the brain in the neonatal intensive care unit and beyond should be widely implemented in an effort to limit injury and promote neuroplasticity.
Impact
With improved survival of preterm infants due to improved antenatal and neonatal care, our focus must now be to improve long-term neurological and neurodevelopmental outcomes.
This review details the multifactorial pathogenesis of preterm brain injury and neuroprotective strategies in use at present, including antenatal care, seizure management and non-pharmacological NICU care.
We discuss treatment strategies that are being evaluated as potential interventions to improve the neurodevelopmental outcomes of infants born prematurely.
Compassionate Inquiry is a psychotherapeutic method developed by Dr. Gabor Maté that reveals what lies beneath the appearance we present to the world. Using Compassionate Inquiry, the therapist unveils the level of consciousness, mental climate, hidden assumptions, implicit memories and body states that form the real message that words both express and conceal.
PREEMIE FAMILY PARTNERS
Your friend or family has finally brought their preemie baby home from the NICU, and you’re excited to meet their little miracle, but unsure of how to approach the family altogether.
Don’t worry, as long as you stick to these simple do’s and don’ts written by a preemie mom, visiting a premature baby will be a happy and smooth time for everyone!
Do Listen to the Preemie Parents’ Conditions (and Comply)
Before visiting a premature baby, ask the parents if they are ready to receive visits in their home. And under which terms.
Don’t miss out!
You know the drill, if you want to be part of Preemie Mom Tip’s email list, subscribe below! You’ll receive weekly emails that will help you on your journey. We are preparing a new and improved FREE resource library, sign up and be the first to know once it’s ready!
Top of Form
It’s not uncommon that when we take our babies home, the doctors impose a no visit rule until we can complete the first vaccination schemes (which more often than not include at least three shots of the Synagis shot.) The complete process can take up to three months.
We didn’t allow almost any visit from friends or family until my son was around four months old (2 months old adjusted), some of our friends were understanding, and some weren’t.
We knew that we were doing what was best for our son, so we stuck to it!
If your friend says it’s OK to visit their baby, find out if they have any special request for your visit.
Some of the petitions may seem weird but know that they come from a very real place (the NICU), and visiting a premature baby during her first months is much like visiting babies in the NICU: short and strict.
Some parents may ask you to keep your cell phones at the entrance of the house (phones are full of germs), wash your hands for five minutes, visit straight from home, or tie your hair, take a shower just before visiting, or wear a surgical face mask. Whatever it is, by doing as they say you’ll help protect their baby and their peace of mind.
Do Bring Extra Clean Clothes for Interacting with the Preemie Baby
This is especially true if you are visiting a premature baby after being all day outside of your home.
The street is full of germs and contamination, and we preemie parents tend to develop a germ-vision.
By bringing freshly laundered clothes and changing into them as soon as you arrive at the house you are visiting you will show them that you are on their side, and support their every measure to keep their baby safe.
It is even more likely that they will let you hold the baby if you do this since she won’t be directly exposed to dirty clothes.
Do: Wash your Hands as Soon as you Enter, Wash your hands thoroughly.
Make sure you wash the space between your fingers, your palm, and the back of your hand.
Even so, many of us neglect this standard practice.
When a baby is in the NICU, the nurses teach us parents about the importance of hand-washing, the correct techniques to do so, the right moment to do it. We wash our hands so frequently that we get rashes most of the time (since the NICU soap is strong.)
It is second nature to us to wash our hands when visiting babies!
Having said all this, once our babies are bigger and stronger, we’ll be a bit laxer about this. After all, germs do help develop the immune system, we just don’t want to expose our miracles before they are ready for this!
Do Keep the Visit Short and Simple
There will be time for the lengthy visits that you may be dreaming about. In the months and years to come, you’ll be able to kiss and smooch the baby to your heart’s content, and stay during weekends, afternoons, and evenings!
But right now, the preemie family may be in need of some alone time. And though seeing you will surely help them, keep your visit under 30 minutes if possible.
Most breastfeeding moms need time adjusting to… well…breastfeeding, but this is especially the case of us preemie moms. We came from pumping our way in the NICU to actually breastfeeding a baby. That transition takes time to get used to.
Additionally, like all new parents, we are most likely to be sleep-deprived. Partly because our babies wake us up all night and partly because of the monitors beeping or ourselves waking up to check that the babies are doing fine.
Keeping a short visit is a long time investment in your relationship with NICU families.
Don’t Go if You’re Not Feeling Well
If your head hurts, your throat is sore or your nose itches, reprogram your visit.
Even if you are feeling well but visited someone who has had the flu within seven days before your visit you may be carrying the virus, so it’s also best to reprogram.
RSV and pulmonary infections are dangerous for preemies.
Ollie had simple flu when he was 12 months old and turned into pneumonia and bronchiolitis in less than 24 hours. We had to rush him to the ER because he wasn’t breathing. He was in the hospital on oxygen for ten days until he recovered. The younger the baby, the higher the risk of infection.
We limited our visits to non-flu visitors until Ollie was well over 8 months. And, we still ask everyone who may be sick to wear a facemask. We don’t overprotect our son, he goes to crowded places and has had the flu several times by now at 24 months. But we still don’t want to risk it by letting someone with the flu hold him without wearing a facemask.
Don’t Hold the Preemie Baby
Unless the parents ask you to hold their baby, don’t press them into it.
You’ll have plenty of opportunities. Just make them feel comfortable by knowing that you are OK just looking at the baby. If they are comfortable with you holding her, they will let you know.
Also, to keep on the safe side, avoid kissing the baby and holding her hands.
Don’t Compare their Preemie to any Other Baby
As preemie parents, the greatest joy in the world comes with sorrow.
We love our baby and wouldn’t change him for anyone else, nor would we want him to be any different. So we try not to compare our baby to anyone else’s. But, sometimes it is inevitable, and we internally cave in.
My son looked like a newborn during his first four months. He didn’t smile until he was eight months old and had to go through weekly Physical Therapy to move his hands and arms. He is healthy, bright, and has no significant delay. But when the children of my friends were smiling, walking, and talking, he wasn’t, and it’s human nature to worry and to compare them.
It gets even worse when people pity my boy or openly compare him to others. It feels as if they are undermining us as if they don’t know or don’t care about our background.
A few months ago a fellow mom who has a son two months younger than Ollie (but bigger and heavier), raved on and on about how small and fragile my Ollie was. She held him without my permission and said that she remembered the times when her son was smaller. She went as far as to congratulate me for being so chill and not overprotecting him. He was evidently so weak (to her eyes.) She seemed to be following an anti-manual for visiting a premature baby.
Needless to say, I despised every second we spent together, and I’ve never seen her again.
Don’t Talk about other Full-Time Pregnancies
Us moms also grieve about the weeks that we should have been heavily pregnant and weren’t.
Sometimes I see other moms complaining about their heavy wombs. Begging for their babies to come early so that they can stop being feeling uncomfortable. I understand that they don’t know what they are saying, but it hurts.
My son was born at 31 weeks, which means that I missed out on nine weeks of pregnancy. Some women dream about their pregnancies their whole lives. They imagine them picture perfect, so we miss what we didn’t have. And in some cases, what we’ll never have.
So it’s better to play it safe and stay clear of that topic.
That’s a Wrap
I’m sure you’ll love visiting a premature baby. Take it one step at a time and be patient with us preemie parents. We do want what’s best for our children, even if sometimes it is hard to express ourselves.
Most of all, you’ll see how powerful and miraculous a person can be, no matter how small!
Have you visited a preemie recently? Are you planning a preemie visit? Or, are you a preemie parent and would like people to know how to plan their visits? Tell us all about it in the comment section!
Empathy — the capacity to identify others’ needs and emotions, and to provide supportive care that meets those needs.
Our recent research shows that parents who express empathy toward their teenagers may give teens a head start in developing the skill themselves. In addition, adolescents who show empathy and support toward their friends are more likely to become supportive parents, which may foster empathy in their own offspring.
Starting in 1998, teens came to the university every year with their parents and closest friend, and a team of researchers recorded videos of their conversations. Researchers observed how much empathy the mother showed to her 13-year-old when her teen needed help with a problem. We measured empathy by rating how present and engaged mothers were in the conversation, whether they had an accurate understanding of their teen’s problem, and how much help and emotional support they offered.
Then, each year until teens were 19 years old, we observed whether teens showed those same types of empathic behaviors toward their close friends.
A decade later, when some of those same teens were starting to have children of their own, we surveyed them about their own parenting. We also asked them about their young children’s empathy. For example, parents rated how often their child “tries to understand how others feel” and “tries to comfort others.”
We found that the more empathic a mother was toward her teenager at age 13, the more empathic the teen was toward their close friends across the adolescent years. Among teens who later had kids themselves, the ones who had shown more empathy for close friends as adolescents became more supportive parents as adults. In turn, these parents’ supportive responses to their children’s distress were associated with reports of their young children’s empathy.
Why it matters
The ability to empathize with other people in adolescence is a critical skill for maintaining good relationships, resolving conflict, preventing violent crime and having good communication skills and more satisfying relationships as an adult.
Adults want teens to develop good social skills and moral character, but simply telling them to be kind doesn’t always work.
Our findings suggest that if parents hope to raise empathic teens, it may be helpful to give them firsthand experiences of being understood and supported.
But teens also need opportunities to practice and refine these skills with their peers. Adolescent friendships may be an essential “training ground” for teens to learn social skills such as empathy, how to respond effectively to other people’s suffering, and supportive caregiving abilities that they can put to use as parents. Our lab’s most recent paper presents some of the first evidence that having supportive teenage friendships matters for future parenting.
What’s next
We’re continuing to follow these participants to understand how their experiences with parents and peers during adolescence might play a role in how the next generation develops.
We’re also curious to understand what factors might interrupt intergenerational cycles of low empathy, aggression and harsh parenting. For example, it’s possible that having supportive friends could compensate for a lack of empathy experienced from one’s family.
While it’s true that you can’t choose your family, you can choose your friends. Empowering teens to choose friendships characterized by mutual understanding and support could have long-term ripple effects for the next generation.
*We checked to confirm these organizations are still active in February, 2025.There was only one resource we were unable to locate. We have also attached the website links!
12 Preemie Support Groups For New Parents, Because You Can’t Go It Alone
It really does take a village for preemie parents by Kinsey Gidick Nov.24, 2020
Only the parents of a premature baby can understand the emotional toll it takes to care for such a fragile child. That’s why finding a community of parents and caretakers who have been through similar circumstances is so important. Fortunately, there are many online resources for parents experiencing the challenge of navigating the NICU and raising a premature baby, from preemie support groups to virtual counseling sessions to even social media accounts.
While each is different, the focus is the same: to provide a space where preemie parents can bring their worries, wins, and concerns to each other and get help and feedback from those going through the same situations. 380,000 babies are born before 37 weeks gestation each year in the U.S. per March of Dimes — that’s 1 out of every 10 American babies. That’s a lot of babies receiving extensive medical intervention including respiratory support, invasive treatments, and extended Neonatal Intensive Care Unit stays. In many cases, these spaces are like lifelines for parents who are afraid of not only the unknown, but the known as well.
Rather than shoulder that burden alone, preemie support groups offer all kinds of resources from chat rooms to virtual mentors, podcasts to classes. It’s the kind of care one won’t often find in a clinic or hospital — ongoing assistance a preemie parent can turn to whether a child is 3 weeks or 3 years old.
1. A space for NICU transition support
Graham’s Foundation, a not-for-profit support group based in Ohio, was founded with a mission that no one should experience prematurity alone. To that end, the organization has a number of programs designed to help pre-term birth families including NICU transition to home care packages, preemie parent mentors who can be contacted 24/7, an app called MyPreemie, and many online forums for parents to engage with other preemie families. –https://www.grahamsfoundation.org/
2.A community of peers
Hand to Hold is an organization created to guide preemie families through the long journey from a NICU stay to home, as well as provide comfort and support in times of loss. To do so, the website maintains forums for its 63,000 online community members. But it’s not just for preemie families. There are also resources for NICU professionals including podcasts and an ambassador program of bedside support volunteers who visit NICUs and provide additional help. –https://handtohold.org/
3.A place for bereavement support
Bereavement support is something all too many families of premature babies need. And High Risk Hope is one place they can find it. The 501(c)3 believes that “there is no foot too small that it cannot leave an imprint on this world.” To do so, the Florida-based organization connects families with other organizations to provide ongoing grief support and counseling. –https://highriskhope.org/
4.One-on-one care
Support 4 NICU Parents Support 4 NICU Parents aims to improve psychosocial support for NICU parents and enhance training and support for NICU healthcare providers, ensuring families and babies thrive together. –https://www.pqcnc.org/node/13721
5.Parental Zoom chats
Tiny Miracles is a nonprofit charity based in Fairfield County, Connecticut, that is dedicated to helping families with premature babies. Like many premature baby groups, it offers all kinds of resources for families, but its most popular offerings are free weekly Zoom support chats that anyone can join. Held every Thursday at 8 p.m. EST, they’re a way for people to get to know other parents beyond a virtual chat room or forum.-https://www.projectsweetpeas.com/
6. Material support
Care packages, hospital events, peer-to-peer support, financial aid, educational materials, these are all the work of Project Sweet Peas. Families can reach out directly for all of the above and receive the care they need from this nonprofit. And for those who have simply been touched by a premature birth and want to give back, they can donate to Project Sweet Peas’ effort which has sent 23,126 NICU care packages to families and 4,909 bereavement boxes as well.-https://www.projectsweetpeas.com/
7.Facebook Preemie Page
Social media sites, like Facebook, are a natural home for support groups and the Parents of Preemies/Premature Babies is one of the biggest for this specific demographic. With 15.3K members, it’s a private group you must ask to join. It was started in 2007 when founder Heather Armstrong writes that she couldn’t find a similar support space. It invites members to discuss topics related to the raising of premature children but doesn’t allow fundraising, self-promotion, or requests for medical advice. It includes parents of preemies from around the world.-https://www.facebook.com/groups/2304668997
8. Helping hand from March of Dimes
Not every hospital has a March of Dimes NICU Family Support program, but it’s worth inquiring should a family find itself with a baby in the newborn intensive care unit. The nonprofit that’s committed to improving the health of mothers and babies organized its NICU Family Support program to provide families with essential materials during their child’s NICU stay. Those include things like “keepsake booklets for their NICU baby, a guide for parenting in the NICU, and a NICU guide” according to the organization’s website. For families with an infant having a shorter NICU stay, March of Dimes provides materials as well. There’s also a helpful app where families can explore their questions and concerns.-https://www.marchofdimes.org/find-support/compassbymarchofdimes
9.Support for babies less than 2 pounds
Premature babies are not a monolith. There are varying levels of prematurity and some of the most at-risk children are those born less than 2 pounds and before 27 weeks. That’s why the Micro Preemie Parents Facebook support page exists, to be there for parents of these special children. Only parents of so called “micro preemies” will be accepted to the private page. Once in, they can expect to be able to join conversations specific to this very unique experience with other parents and guardians who understand where they’re coming from. –https://www.facebook.com/groups/micropreemiemoms
10. A Space for Black Preemie Parents
Black Preemie Parents Community is a Facebook group just for Black parents to find “support, advice, share stories, or just vent as you go through your journey.” It’s a small group with less than 400 members providing those who join with an intimate circle of friends to reach out to during challenging times. –https://www.facebook.com/groups/blackpreemieparentscommunity
11. Where to go when they grow
The premature parenting journey doesn’t end when a child leaves the NICU. It’s a lifelong path and one that might find parents looking for support well into their child’s teens and twenties. For that there’s Parents of Older Preemies. Another Facebook group, this 1.5K member page is for “parents to share their stories of their preemie(s) and how far they have come in their lives in a caring and supportive environment. This group shares triumphs, setbacks, frustrations and positive advice to others that are on their continued “preemie journey.”-https://www.facebook.com/groups/276697059074997
12. Visual Support
Preemie baby support isn’t limited to Facebook and nonprofit organizations. Instagram has also become a network where people kind find kinship in navigating life with a preemie. For instance, preemiesupermoms is an Instagram page dedicated to prematurity awareness. The page posts images of premature babies along with inspiring quotes and stories
For families looking for someone to listen or a place to gather strength, these organizations are here to help. All families need to do is ask. –https://www.instagram.com/preemiesupermoms/
INNOVATIONS
EDITORIAL: What is new on the Horizon in Neonatology? Recent Advances in Monitoring, Diagnostics, and Therapeutics in Neonatal Care
Introduction
Neonates and infants are commonly referred to as “therapeutic orphans” due to the overall scarcity of therapeutic interventions that have been developed and tailored to their needs and specific characteristics . This is well known by care providers and researchers active in this field, but is perhaps less on the radar of authorities, funding bodies or the broader public. There is significant health inequity when comparing newborns to other age populations in terms of specific drug and device development and therapeutics . In addition there are health inequities in the provision of neonatal care globally which require special attention in terms of improvement .
Bronchopulmonary dysplasia, neonatal seizures, poor growth, necrotizing enterocolitis (NEC) and short bowel, hypoxic-ischemic encephalopathy, retinopathy of prematurity (ROP), neonatal infections and sepsis hereby serve as a non-exhaustive list of “orphan conditions” in need of more equity, through adequately and urgently funded research and improvement.
The good news is that there have been increased efforts, in recent years, by researchers and regulatory bodies to focus on the provision of drugs, devices, and treatment modalities tailored for neonatal use, while further advocacy remains an obvious need (2, 4, 5). This brings perspective and explains the initiative taken to organize a focused research topic on what is on the horizon as well as recent advances.
Overview of the topics covered
We targeted emerging or new aspects related to monitoring, diagnostics and therapeutics in neonatal care for the current research topic. Fortunately, this research topic was perceived as very relevant by the research community, as 135 authors expressed their interest as contributors, resulting in 20 accepted papers. This serves as a signal of the importance to continue to work on this topic.
Post-hoc, and in a somewhat arbitrary way (because of overlap in these subcategories) these papers were subdivided by the editors into different subcategories, with focus on (1, 5 papers) perinatal biomarkers in blood and urine and how these relate to or predict outcomes, (2, 6 papers) adaptations of existing and newly emerging equipment in neonatal units, (3, 3 papers) needed advances in pharmacotherapy, (4, 3 papers) machine learning or deep learning applications in neonatal care, and finally, (5, 3 papers) underreported aspects of contemporary NICU care, with a focus on the holistic nature of care for the infant and the family.
Perinatal biomarkers in blood and urine and how these relate to or predict outcomes
Two papers focused on biomarkers related to gestational diabetes, with reflections and data on maternal and neonatal outcomes. Postnatal maternal levels of glycated albumin and hemoglobin A1c in mothers of large-for-gestational-age (LGA) informed us of the relevance of accurate diagnosis during pregnancy. This is because postpartum women without diagnosis during pregnancy had higher glycated albumin values, associated with LGA and associated complications (Železnik et al.). Interestingly and related to this paper, Yin et al. reported on a untargeted metabolomics study in women with gestational diabetes, with the recommendation of a maternal serum metabolite panel to forecast neonatal adverse outcomes (hypoglycemia and macrosomia) (Yin et al.).
Other papers focused on the use of vitamin D, acid-base and biomarkers associated with fetal growth restriction with impaired neurodevelopmental outcome. In a cohort of 217 preterm neonates, a multivariate regression analysis identified antenatal steroids as protective, and lower birth weight, duration of ventilation, sepsis and the serum 25-(OH)D vitamin as risk factors to develop ROP (Yin et al.). Musco et al. reported on a systematic review on blood biomarkers indicating risks of adverse neurodevelopmental outcome in fetal growth restricted infants (Musco et al.). While the authors retrieved some data on neuron specific enolase and S100B, the overall conclusions reflect a call for further research. Finally, an association between lactate levels in umbilical cord blood and cerebral oxygenation in preterm neonates was studied as a secondary outcome analysis (Dusleag et al.). In non-asphyxiated preterm neonates with respiratory support, lactate levels were negatively associated with cerebral and arterial oxygenation. In term neonates without respiratory support, no associations were observed.
Adaptations of existing and newly emerging equipment in our units
In a review on emerging innovations in neonatal monitoring, Krbec et al. concluded that there is an urgent, still unmet need to develop wireless, non- or minimal-contact, non-adhesive technology, capable to integrate multiple signals in a single platform, tailored to neonates (Krbec et al.). Related to this call of action, Svoboda et al. reported on their pilot experience with contactless assessment of heart rate, applying imaging photoplethysmography (Svoboda et al.). Rectal and axillary temperature monitoring on admission were compared in a cohort of preterm (n = 80, <32 weeks gestational age) by Halabi et al., reporting that rectal measurement was likely more reliable in the event of hypothermia (Halabi et al.). Ultrasound-guided measurement of anterior cerebral artery resistive index in the first week of life in 739 preterm neonates (<35 weeks) was not associated with subsequent co-morbidities on admission or during neonatal stay (asphyxia, sepsis, NEC) (Singh Gill et al.). A case series of neurally adjusted ventilatory assist to rescue pulmonary interstitial emphysema in 5 extremely low birth weight infants illustrated the potential value of this ventilatory equipment and strategy and need for further study (Chen et al.). Finally, van Rens et al. compared a conventional to a modified Seldinger technique (a dedicated micro-insertion kit) for peripherally inserted central catheter (PICC) placement, illustrating the relevance of developing “low risk, high benefit” type of medical devices, adapted to the specific needs of neonates (van Rens et al.).
Advances needed in pharmacotherapy
The currently available medicines and dosing regimens in neonatal care are limited and there is an urgent need for improvement in this domain. This was illustrated by articles on sepsis, septic shock and steroids. Inequity in provision of neonatal care across the globe ought to be a major focus of improvement. Gezahegn et al. described the outcome in neonates admitted with sepsis in Harar (Ethiopia). Low white blood cell count, desaturation, preterm birth, absence of prenatal maternal care, and chorioamnionitis were important risk factors for sepsis-related mortality (Gezahegn et al.). Addressing these prognostic factors hold the promise to act as levelers to improve outcomes. A pilot study compared noradrenaline and adrenaline as first line vasopressor for fluid-refractory sepsis shock (Garegrat et al.). Both interventions were comparable to resolve the septic shock, while the overall mortality (13/42, 30%) remained significant, highlighting the need for better diagnostic and therapeutic options. Finally, in a systematic review, outcome of postnatal systemic corticosteroids (hydrocortisone to dexamethasone) were compared as reported in randomized controlled trials (Boscarino et al.). The authors concluded that dexamethasone appeared to be somewhat more effective than hydrocortisone in improving respiratory outcomes, but with inconclusive but relevant concerns on the uncertainties on long-term neurodevelopmental outcome, again highlighting the need for better therapies for prevention and management of chronic lung disease of prematurity.
Machine learning or deep learning applications in neonatal care
Artificial intelligence is a rapidly advancing area with fast evolving clinical applications in healthcare, including in the NICU (6). It is no surprise that the current research topic also contains papers illustrating its relevance to improve our practices and outcomes. Two papers hereby focused on NEC, and a 3rd paper on prediction of significant patent ductus arteriosus (PDA). In a mini-review, Cuna et al. reports on the various pathophysiological processes underlying NEC endotypes, and how artificial intelligence holds the promise to influence further understanding and management (Cuna et al.). An approach to enhance surgical decision making in NEC is illustrated by Wu et al. Based on x-rays from 263 neonates diagnosed with NEC (94 surgical cases), a binary diagnostic tool was trained and validated, with Resnet18 as approach applied (Wu et al.). For PDA, an ultrasound-based assessment of ductus arteriosus intimal thickness in the first 24 h after birth was applied in 105 preterm neonates. A prediction model for closure on day 7 included birth weight, mechanical ventilation, left ventricular end-diastolic diameter, and PDA intimal thickness (Hu et al.). Such models can be considered to better target future study, integrated in a precision medicine approach. Use of AI and big data have the potential to significantly improve our understanding of neonatal conditions and also support neonatal researchers in asking better research questions.
Underreported aspects of contemporary NICU care, holistic care
As part of this research topic, we also accepted papers reporting on the use of music on pain management, on multisensory stimulation to improve maternal milk volume production, and parents’ experiences related to congenital cardiac surgery. All these 3 papers reflect the need for holistic care and to further integrate the perspectives of (former) patients and parents into neonatal practice.
In a systematic review, Ou et al. demonstrated that music is an effective intervention to relief procedural pain (e.g., Premature Infant Pain Profile score) in preterm neonates, as it reduced some markers of stress, and improved blood oxygen saturation (Ou et al.). Multisensory stimulation (audiovisual, or audiovisual + olfactory) compared to a control setting improved maternal milk volume production, with evidence of positive effects of both interventions, even more pronounced if both interventions are combined (Cuya et al.). Finally, a quantitative analysis of parent’s experiences with neonates admitted to NICU with a congenital heart disease reinformed us on the importance of actively focusing on parental experiences of care (Catapano et al.).
From advances in neonatal care to implementation
In our opinion, this research topic nicely illustrates the diversity in ongoing clinical research activities, that all hold the promise to improve our clinical management practices, with the overarching aim to improve neonatal outcomes. There is an urgent need to focus on the current health inequities in the provision of care to neonates (3). The trend towards a “neuro” dedicated NICU care is an illustration on how relevant progress may occur. This progress is based on improved neuromonitoring techniques (7), improved management and precision medicine in the field of anti-epileptic drugs (8), and integrating families as partners in neonatal neuro-critical care and similar improvement programs (9). The good news is that we are already experiencing a shift in the right direction. The neonatal community and all other relevant stakeholders need to work better together to improve the pace and scale of this improvement.
The prenatal shunt, ductus arteriosus (DA), typically closes during the cardio-pulmonary transition at birth. We evaluated maternal and neonatal factors associated with delayed closure of DA in term-born neonates.
Method
We conducted a retrospective cohort study that included full-term neonates from the prospective observational Copenhagen Baby Heart cohort study. We assessed the association between maternal and neonatal factors and delayed ductal closure.
Results
We included 19,566 neonates, of whom 48% were female. Echocardiography was performed at a median age of 12 (IQR:9-15) and eight (IQR:2-13) days for neonates with no DA and an open DA, respectively. Associations with delayed ductal closure included maternal obesity adjusted risk ratio=2 (95%CI:1-3.8), maternal hypothyroidism during pregnancy aRR=2.02 (95%CI:1.2-3.4), low Apgar 2.6 (95%CI:1.2-6), high weight aRR=1.81(95%CI:1.2-2.6), and length at birth aRR=1.7(95%CI:1.1-2.6).
Conclusion:
The identified risk factors for delayed ductal closure in term-born neonates may help increase clinical attention and improve neonatal care.
UNICEF 2025 Global Outlook: Prospects for Children in 2025 – Building Resilient Systems for Children’s Futures
17 February 2025
Prospects for Children in 2025: Building Resilient Systems for Children’s Futures is the latest edition of Global Outlook, a series of reports produced each year by United Nations Children’s Fund (UNICEF) Innocenti – Global Office of Research and Foresight, which look at the key trends affecting children and young people over the following 12 months and beyond.
In this new report, new and intensifying crises for children – including climate change, conflict and economic instability – are shown to be closely interconnected.
For instance, climate change is disrupting the water cycle, leading to widespread water scarcity, threatening food production and livelihoods across the economy. This disruption poses direct and indirect risks to children, as it impacts the availability of safe water, food, and family income.
The report also notes that debt burdens are forcing governments to cut essential public services, including those related to water, sanitation, and hygiene. These challenges are compounded by a lack of investment in long-term development.
According to UNICEF, rising geopolitical tensions and competition among nations are hindering the implementation of solutions that will protect young people’s lives and build more resilient futures for them.
The report calls for resilient national systems that prioritize children’s health, education and wellbeing, and emphasizes the importance of including children’s rights in climate action.
Empathy and compassion is the foundation of the powerful bond we share as a community. It’s more than just understanding the struggles of others—it’s about truly connecting with their experiences and emotions. As we continue on our journey from the neonatal unit to where we are today, empathy strengthens our resilience and fosters a sense of unity. This connection gives us the strength to support one another, celebrate our victories, and face challenges together.
In the video you’re about to watch, we’ll dive deeper into how our shared experiences and collective empathy can empower us to not only overcome adversity but also to thrive. It highlights the importance of understanding and supporting each other, offering both comfort and encouragement in meaningful ways. Through storytelling and the exchange of our journeys, we create a community that is stronger, more resilient, and ready to face whatever challenges come our way.
I wanted to share this video because it perfectly encapsulates the power of empathy and how, together, we can elevate each other. It’s a reminder that even in difficult times, we are never alone—our shared experiences and collective strength can light the way forward.
Let’s continue to harness the power of empathy as we watch and reflect on the message in this video. Together, we are unstoppable.
What Is The Difference Between Empathy, Sympathy, and Compassion
The Power of Emotional Competency
Expert Reveals the Truth About Empathy, Sympathy and Compassion | Doug Noll
This video shows you the difference between empathy, sympathy, and compassion
• Sympathy is pity-based and is selfish
• Empathy is a learned skill
• Compassion is empathy with an impulse to relieve distress
This video is for our younger friends to help them understand empathy, which means caring about how others feel and being kind to them. Mark Ruffalo and Murray Monster from Sesame Street will show us what empathy is and give fun examples of how we can be kind and helpful to others. I wanted to share this video because it’s a great way for younger kids to learn how to show empathy and support for their friends and family. Let’s watch and see how we can all use empathy to make the world a kinder place! Enjoy watching!
Sesame Street – Empathy With Mark Ruffalo
This video is perfect for helping young students understand what empathy is. Murray Monster and Mark Ruffalo talk about what empathy means and go through several examples. Use this helpful video for introducing important social skills to your K-2 students!
Quiksilver & Roxy Czech and Slovak Surfing Championship 2022
Healthcare in Malaysia is under the purview of the Ministry of Health of the Government of Malaysia. Malaysia generally has an efficient and widespread system of health care, operating a two-tier health care system consisting of both a government-run public universal healthcare system along with private healthcare providers. Within the public universal healthcare system, specialist services are either free or have low user fees for procedures (however, appliances are fully self-funded out of pocket by the patient, even within the public healthcare system); as such the public healthcare system suffers from high demand, routine congestion, long wait lists, chronic widespread delays along with persistent shortages in healthcare personnel, medical equipment and healthcare supplies.
Therefore, private healthcare providers play a pivotal role in providing specialist consultants and general practitioner (GP) services to the Malaysian population; the private healthcare providers complements or supplants the public healthcare system in terms of availability, types of treatments provided and types of materials used.
Reducing neonatal deaths in premature infants in low- and middle-income countries is key to reducing global neonatal mortality. International neonatal networks, along with patient registries of premature infants, have contributed to improving the quality of neonatal care; however, the involvement of low-to-middle-income countries was limited. This project aims to form an international collaboration among neonatal networks in Asia (AsianNeo), including low-, middle- and high-income countries (or regions). Specifically, it aims to determine outcomes in sick newborn infants, especially very low birth weight (VLBW) infants or very preterm infants, with a view to improving the quality of care for such infants. Methods and analysis Currently, AsianNeo comprises nine neonatal networks from Indonesia, Japan, Malaysia, Philippines, Singapore, South Korea, Sri Lanka, Taiwan and Thailand. AsianNeo will undertake the following four studies: (1) institutional questionnaire surveys investigating neonatal intensive care unit resources and the clinical management of sick newborn infants, with a focus on VLBW infants (nine countries/regions); (2) a retrospective cohort study to describe and compare the outcomes of VLBW infants among Asian countries and regions (four countries/regions); (3) a prospective cohort study to develop the AsianNeo registry of VLBW infants (six countries/regions); and (4) implementation and evaluation of educational and quality improvement projects in AsianNeo countries and regions (nine countries/regions). Ethics and dissemination The study protocol was approved by the Research Ethics Board of the National Center for Child Health and Development, Tokyo, Japan (reference number 2020–244, 2022–156). The study findings will be disseminated through educational programmes, quality improvement activities, conference presentations and medical journal publications.
ABSTRACT
Introduction Reducing neonatal deaths in premature infants in low- and middle- income countries is key to reducing global neonatal mortality. International neonatal networks, along with patient registries of premature infants, have contributed to improving the quality of neonatal care; however, the involvement of low- to- middle- income countries was limited. This project aims to form an international collaboration among neonatal networks in Asia (AsianNeo), including low-, middle- and high- income countries (or regions). Specically, it aims to determine outcomes in sick newborn infants, especially very low birth weight (VLBW) infants or very preterm infants, with a view to improving the quality of care for such infants. Methods and analysis Currently, AsianNeo comprises nine neonatal networks from Indonesia, Japan, Malaysia, Philippines, Singapore, South Korea, Sri Lanka, Taiwan and Thailand. AsianNeo will undertake the following four studies: (1) institutional questionnaire surveys investigating neonatal intensive care unit resources and the clinical management of sick newborn infants, with a focus on VLBW infants (nine countries/regions); (2) a retrospective cohort study to describe and compare the outcomes of VLBW infants among Asian countries and regions (four countries/regions); (3) a prospective cohort study to develop the AsianNeo registry of VLBW infants (six countries/regions); and (4) implementation and evaluation of educational and quality improvement projects in AsianNeo countries and regions (nine countries/regions).Ethics and dissemination The study protocol was
approved by the Research Ethics Board of the National Center for Child Health and Development, Tokyo, Japan (reference number 2020–244, 2022–156). The study findings will be disseminated through educational programmes, quality improvement activities, conference presentations and medical journal publications.
A Critical Need For Breastmilk Collection Centres For High-risk Premature Babies
Authors: Wan Mazwati Wan Yusoff, International Islamic University Malaysia Mashitah Zainol Abidin
Abstract
Premature babies are very vulnerable and exposed to various life-threatening diseases. World Health Organization reported that many premature babies were saved from morbidity and mortality when they were fed with breastmilk starting from within the first hour after their birth. The rate of premature birth in Malaysia has increased exponentially since 2018—more than 20 percent premature births. Therefore, hospitals should have enough supplies of breastmilk to save the lives of the precious premature babies. However, only one hospital in Malaysia provides supplies of breastmilk on demand. This study employed philosophical method to argue for the establishment of breastmilk collection centre. It examined the concept of maqāṣid al-sharīʿah to justify the proposal of the establishment of breastmilk collection centres in hospitals throughout Malaysia to save the lives, intellects, and progenies of the at-risk premature babies. The primary issues resulting from breastmilk sharing according to Islamic perspective were examined and practical steps were proposed to rectify them. The steps involved obtaining signed consent from wet nurse and her husband; screening of wet nurse’s health and personality characteristics; screening of the breastmilk by the milk collection centre; obtaining signed consent from the premature baby’s parents; feeding breastmilk to the premature baby with the consent of witnesses; meeting between wet nurse and her family and the baby’s parents and family; and completing wet nursing document to be given to the newly formed milk kinship family.
Building Trusting Teams – A Pathway to Organizational Excellence
Rody Azar, MHA, RRT-NPS
Introduction:
Trust is an essential element of effective teamwork. It fosters an environment where team members feel safe communicating openly, sharing ideas, and collaborating towards common goals. Without trust, relationships become strained, communication breaks down, and organizational performance suffers. According to a study by Gallup, organizations with high employee engagement, which is closely related to trust, report 21% higher profitability (Gallup, 2020). This paper explores trust in teams, examining how it can be fostered and its profound impact on organizational success.
The Importance of Trust in Teams:
1. Enhanced Communication: Trust creates a safe space where team members can share their thoughts and feelings without fear of judgment. This openness leads to improved communication, enabling teams to function more effectively. When team members trust each other, they are more likely to engage in candid discussions, ask for feedback, and share constructive criticism. This process encourages continuous improvement and innovation.
2. Improved Collaboration: Teams characterized by trust collaborate more seamlessly. Trust encourages team members to share resources, support one another, and seek each other’s abilities. This collaborative spirit leads to better problem-solving and decision-making, as individuals are more willing to listen to diverse perspectives.
3. Increased Engagement: Trust enhances commitment and engagement within teams. Employees who feel trusted and valued are more likely to invest their time, energy, and creativity into their work. This higher level of engagement results in better performance and productivity, as engaged employees are motivated to achieve team goals.
4. Effective Conflict Resolution: Conflict is a natural occurrence in any team dynamic. However, team members are more likely to address conflicts directly and constructively in a trusting environment, allowing them to express their disagreements without fear of damaging relationships. This approach leads to more effective and quicker resolutions, which helps support a positive team atmosphere.
5. Greater Accountability: When trust exists within teams, members are more likely to hold themselves and each other accountable for their roles and responsibilities. Trusting teams create a culture of accountability where individuals take ownership of their work, leading to higher standards and better performance.
Characteristics of Trusting Teams:
Open Communication: Team members communicate transparently and honestly, fostering a culture of openness and inclusivity.
Mutual Respect: Trusting teams recognize and appreciate each other’s strengths, value
diversity, and promote an inclusive environment.
Shared Goals: All team members are aligned with common goals, reinforcing collaboration
and commitment.
Empathy and Support: Team members show care and understanding for one another,
creating a supportive atmosphere that encourages sharing and vulnerability.
Reliability: Trusting teams foster a sense of reliability, where members can depend on each
other to fulfill commitments and responsibilities.
Strategies for Building Trusting Teams:
Building trust is an ongoing process requiring intentional effort from leaders and team members. Below are strategies to cultivate trust in teams:
1. Lead by Example: Leaders play a crucial role in shaping team dynamics. By showing trustworthy behaviors, such as honesty, integrity, and accountability, leaders set the standard for others to follow. Vulnerability in leadership (e.g., admitting mistakes and seeking feedback) can also strengthen trust within the team.
2. Foster Open Communication: Encourage team members to openly share their thoughts, ideas, and feedback. Create an environment where communication is valued, and actively listen to team members. Regular check-ins, team meetings, and one-on-one discussions can help open dialogue and build trust.
3. Encourage Collaboration: Design opportunities for team collaboration across various projects. Creating diverse project teams allows members to collaborate, share knowledge, and build relationships. Activities such as brainstorming sessions or team-building exercises can strengthen interpersonal connections.
4. Recognition and Appreciation: Regularly acknowledge and celebrate the contributions of team members. Recognition fosters an environment of appreciation, reinforcing the value of individual efforts. Simple gestures such as expressing gratitude during meetings or highlighting achievements can significantly boost trust within the team.
5. Create a Safe Environment for Risk-Taking: Encourage team members to take thoughtful risks and innovate without fear of negative consequences. Providing autonomy and support for innovative ideas helps build trust, as team members feel empowered and valued for their contributions.
6. Establish Clear Roles and Expectations: Clarify the roles and responsibilities of each team member. When individuals understand their specific roles and expectations, it fosters accountability and reduces uncertainty. Clear roles create a sense of security, allowing team members to trust that everyone is working towards the same goals and can depend on one another to fulfill their responsibilities.
7. Promote Team-building Activities: Engaging in in-person or virtual team-building activities can significantly strengthen team members’ interpersonal relationships. These activities should encourage collaboration, promote understanding, and foster positive interactions outside of day-to-day work. Such experiences can help individuals develop personal connections, creating a more profound sense of trust.
8. Provide Opportunities for Professional Development: Encouraging continuous learning and professional growth shows team members that the organization values their development. Offering training, workshops, and mentorship opportunities improves individual skills and reinforces trust, as team members see that their organization is invested in their success.
9. Practice Transparency: Transparency is a key part of trust. Leaders should share relevant information about the organization’s goals, decision-making processes, and performance metrics with their teams. When team members are informed about what is happening within the organization, they feel more involved and valued, strengthening trust.
10. Encourage Feedback: Creating a culture where feedback is valued encourages trust among team members. Implementing regular feedback mechanisms—such as one-on-one check-ins and anonymous surveys—allows team members to express their thoughts and concerns. Moreover, showing that feedback is taken seriously and leads to action, reinforcing the notion that everyone’s input is valuable.
The Impact of Trusting Teams on Organizational Success:
The presence of trusting teams can lead to transformative outcomes in an organization:
1. Higher Performance and Productivity: Organizations with trusting teams have been shown to achieve higher performance levels. Trust enhances collaboration and reduces time spent on conflicts, resulting in teams completing projects more efficiently and effectively.
2. Improved Employee Well-being: A trusting environment improves employee morale and job satisfaction. Employees who feel trusted are less likely to experience stress and burnout, resulting in a healthier workforce with higher retention rates.
3. Greater Innovation: Trust allows teams to embrace creative solutions and explore innovative ideas without fear of failure. This environment fosters innovation as team members confidently share their insights and experiment with novel approaches to work.
4. Stronger Organizational Culture: A trust-based culture promotes a sense of belonging and shared purpose. Employees are more likely to feel aligned with the organization’s mission and values, which enhances overall engagement and loyalty.
5. Resilience to Change: Organizations characterized by trust navigate change effectively. Trusting teams adapt more readily to new initiatives and challenges as members communicate openly and support one another during transitions.
Conclusion:
Building trusting teams is not just a desirable outcome but essential for organizational success. Trust enhances communication, collaboration, and accountability while fostering a positive work environment. Organizations can cultivate a culture where teams thrive by implementing strategies that promote trust-building, such as leading by example, fostering open communication, and providing opportunities for development.
Leaders must recognize that trust is a pivotal part of team dynamics and should actively work to nurture it. The benefits of trusting teams extend beyond individual relationships; they affect organizational performance, employee satisfaction, and innovation. As organizations navigate complexities in the modern workplace, prioritizing trust will be paramount for achieving sustainable success.
By building trust within teams, organizations can strengthen their foundation and position themselves for future success. As shown throughout this paper, trusting teams are the cornerstone of an effective and resilient organizational culture.
SOS Préma” empowers healthcare providers with parental insights at 15th annual training days
Posted on 13 November 2024
10-11 October saw 340 healthcare professionals gather in France for SOS Préma’s 15th annual training days, a pivotal event offering an empathetic view into the realities faced by families of preterm infants.
Each year, “SOS Préma”, our valued partner in France, hosts training sessions to deepen the understanding of healthcare providers around the unique challenges encountered by preterm infants and their families. Established in 2011, these events now bring together hundreds of healthcare professionals, all committed to improving neonatal care. The 15th edition, held on 10 and 11 October, attracted over 340 participants, all united in their commitment to advancing care for these vulnerable newborns.
The event revolved around four main themes, each addressing key aspects of neonatal care:
Zero Separation: Couplet care from birth Promoting uninterrupted contact between newborns and parents from birth through hospitalisation, ensuring that critical family bonds are supported from the earliest moments.
Supporting late preterm babies Exploring breastfeeding and Kangaroo Mother Care as essential practices to help these infants grow and thrive, reinforcing the importance of holistic approaches.
Navigating difficult moments with Zero Separation Addressing challenging periods during hospitalisation and equipping professionals with strategies to provide consistent infant- and family-centred support.
Observing newborns with family involvement Encouraging healthcare providers to incorporate parents as essential members of the caregiving team, fostering a collaborative environment for a more comprehensive understanding of each infant’s needs.
SOS Préma’s Charter for the Hospitalised Newborn, a cornerstone of these discussions, continues to influence practices by promoting humane and inclusive neonatal care. Parental testimonials were central to the event, with families sharing their firsthand experiences, followed by scientific insights, ensuring that every healthcare professional gains practical tools and empathetic perspectives.
Global Health Education for Medical Students and Residents
Before you complete your family medicine residency or even finish medical school, there are ways that you can begin to nurture your interest in global health and prepare for service you may want to provide in the future. Here’s how to get started.
For Medical Students
Integrating Global Health into Your Medical Education
Seeking out as many global health-related opportunities as possible during your time in medical school can help you clarify your vision for working and serving globally, and cultivate relationships through which you may contribute and be mentored.
Opportunities you should consider include the following:
Develop knowledge, skills, and understanding that will prepare you to work effectively in a global context.
Participate in your medical school’s global health track (if available). Getting involved in a global health track during medical school is strongly recommended. A well-designed global health track provides necessary background information and skills. It can also facilitate networking, which is key to short-term international rotations, and help you find individual mentors who can help guide your decisions.
Participate in activities that focus on local underserved populations and/or global health (e.g., journal clubs, courses, electives, service projects, service-oriented student groups, research)
Volunteer for a not-for-credit experience serving an underserved population during your M1-M2 summer, or during a fall, spring, or holiday break
Do a research project or a scholarly/capstone project focused on a population outside of the United States or an underserved population in the United States
Advocate for the value and relevance of global health curriculum and experiences to your medical school. For example, you could provide the dean and the family medicine chair with information about the value of global health experiences and curriculum for your development as a physician and the school’s achievement of its mission.
Get involved in your medical school’s global health-related student interest group (if available)
Lead your Family Medicine Interest Group (FMIG)in serving a local underserved population; you might want to partner with other student groups to develop a sustainable program.
Engage with your medical school’s office/center/institute for global health (if available)
Build a foundation for long-term collaboration by developing relationships with people and organizations involved in global health; tap into your medical school’s existing partnerships and relationships, if available.
Aim for a longitudinal experience throughout medical school
Cultivate relationships with mentors who can guide your development of abilities and attributes you will need to pursue your interest in global health
Finding a Family Medicine Mentor in Global Health
Finding a mentor can be a huge help in navigating the many questions you’ll have as you become more aware of global health needs and opportunities. Here are some suggestions on finding a mentor for yourself.
Attend the American Academy of Family Physicians’ (AAFP’s) annual Global Health Summit. This conference is specifically designed to facilitate networking and is attended by experienced global health workers who have long-term involvement in specific cultures and countries.
Try personal networking. Ask colleagues, friends, and family members whether they know anyone who works in global health, and contact potential leads with emails and phone calls. The more connections you make, the greater your chances of identifying one or more physicians who would be an appropriate mentor.
Look for someone who is doing the type of global health work you would like to do or working in a region that interests you. Contact that person to share your background and aspirations.
Reach out to presenters at meetings or to authors of articles/books of interest. Ask for advice or offer to help someone with a project. People working in global health often find it rewarding to advise and work with those who are exploring an interest in global health.
For Residents
Preparing for Global Health During Family Medicine Residency
An accredited family medicine residency program provides ideal preparation for short- and long-term global health work. Family physicians are specifically trained to provide the care that is most needed in the developing world—care for patients of all ages that is comprehensive, continuous, integrated, community oriented, and team based. If you are seriously considering global health work, you should select a residency program that offers:
Support and guidance for interest in global health
A patient population that includes a variety of ethnicities, cultures, and languages so that you can become proficient in the use of translators and cultural interpreters
A robust global health track that provides additional training in tropical and poverty-related diseases, advanced procedural skills, and cultural competence; the opportunity to participate in global rotations; and a network of international contacts. Getting involved in a global health track during residency is strongly recommended.
Once you have started your family medicine residency, the following steps can help you prepare for global health work:
Develop competence in a team-based approach to medical care; attention to the whole family; preventive and community-oriented care; and provision of continuous care to a defined population
Develop specific interventional skills (e.g., procedures that are commonly performed at the primary care level in developing countries, such as repair of complex lacerations and interpretation of diagnostic ultrasound examination)
Find a faculty mentor or advisor who is involved in global health work and can help you prepare yourself and your family. A faculty mentor might also be able to help you use your global health experience to develop a scholarly presentation or paper.
Complete additional (e.g., fellowship-based) training in advanced obstetrics and gynecology (including c-section) or disaster relief. Although a fellowship is not essential for an effective contribution to global health, it can be helpful.
Family Medicine Residency Programs with International Rotations
The AAFP Center for Global Health Initiatives has compiled a director of family medicine residency programs that include international rotations. Search our free database to explore these programs.
Ways to Integrate Global Health into Your Residency Experience
Find your passion within global health.
If you want to make a lasting impact in a global health setting, it is important to find your niche within the vast array of family medicine global health opportunities. It may take time and several different experiences to discover and develop your passion. You may find that you are drawn to a certain country, culture, language area, or area of need (e.g., maternal and child health, social determinants of health, disaster relief, policy, noncommunicable diseases). Be open to the many types of experiences that are available. If possible, explore them before you are committed to long-term employment.
There may be faculty mentors in your residency program who have experience in certain areas of global health. The AAFP offers a directory of global health opportunities.
Attending conferences such as the AAFP Global Health Summit also will expose you to many different areas of interest within global health.
Form partnerships.
Once you find your passion, partnering with individuals and organizations that share your enthusiasm will further your interest and help you have a lasting, sustainable impact. Cultivate relationships by staying connected with particular organizations or international communities. If you travel, try to return to the same area so you can deepen your commitment to that population. Partnerships and connections will help you integrate global health fully into your career, and expand your capabilities in sustainable global health efforts.
Connect with others.
There is significant interest in global health among family medicine residents in the United States and abroad. The World Organization of Family Doctors (Wonca) Young Doctors’ Movements (YDMs) around the world connect passionate residents and young physicians in conversations about family medicine in global health.
The Polaris Movement for New and Future Family Physicians in North America is a YDM launced in 2014 that provides an international platform for medical students, residents, and new family physicians. Connect on their Facebook page.
Another initiative of the Wonca YDMs is Family Medicine 360°, an exchange program for family medicine residents during their elective months. These four-week exchanges allow participants to travel to a country of interest and experience primary health care delivery in that setting.
Consider completing a Master of Public Health (MPH) degree.
Proficiency in public health is becoming increasingly important in the global health arena, especially if you want to make lasting impact on prevention and social determinants of health. Some residency programs and fellowship programs pay for pursuit of an MPH while in training. Find out if your residency program is among them.
Explore fellowships in global health.
It is becoming easier to find residency programs that offer a family medicine global health fellowship; however, there are currently more global health fellowships in emergency medicine (EM) and internal medicine (IM) than in family medicine. If this is the case at your residency program, talk with the fellowship program to find out whether these fellowships can be adapted to family medicine.
Explore electives in global health.
Many residencies already have global health electives or tracks in place. If your residency does not offer these, consider creating your own global health elective in your area of interest. Most residency programs will accept your ideas for an elective, especially if you already have a relationship with the organization with which you will be working.
If you are unable to travel due to time or financial constraints, pursue or create electives locally that encompass global health ideals. Working with underserved or marginalized populations in your own community can create lasting positive changes. Remember, global health is not just international health; it includes efforts in your own backyard as well!
While the majority of neonatologists are women, women make up a far smaller proportion of neonatologists in leadership positions. A recent national survey led by Kristen Leeman, MD, in the Division of Newborn Medicine at Boston Children’s and Lindsay Johnston, MD, at Yale, finds that many female neonatologists face roadblocks to career development. They often miss out on speaking engagements, career guidance, additional training, networking opportunities, and above all, mentors.
To learn more about their needs, Leeman and her colleagues contacted nearly 4,000 female neonatologists from the AAP-affiliated Women in Neonatology group and a Facebook group for female neonatologists. They received 451 survey responses, revealing several additional challenges:
gender-based salary discrepancies, reported by 49 percent of respondents
delayed promotion (37 percent)
harassment by colleagues (31 percent), trainees (8 percent), staff (24 percent), and patient families (32 percent)
lack of an established mentor (61 percent).
Female neonatologists also tend to struggle more than their male counterparts with work/life balance issues, Leeman notes, making it hard to advance. “Women commented on child care stress and burnout,” she says. “The supports are not there at vulnerable times in their careers. It’s a leaky pipeline.”
Building a mentoring program for female neonatologists
Leeman and Johnston decided to address what they see as the key missing ingredient — mentors.
“Both of us have had the benefit of superb mentorship, which has been integral to our careers,” says Leeman. “We wanted to offer an opportunity for all women across the U.S. to have access to female role models to help mentor them through different elements of their careers.”
With colleagues across the country, they created the National Women in Neonatology Mentorship Program. Bringing together senior, mid-career, and junior neonatologists, the year-long pilot program, which concludes in August, has three goals:
to provide resources to facilitate career advancement and professional and personal satisfaction
to identify strategies to help female neonatologists gain appropriate compensation, promotions, and professional recognition
to foster a feeling of community.
In virtual and in-person meetings, the program’s 250-plus participants read and discuss materials, hear speakers, share their thoughts and experiences, network, offer mutual encouragement, and consult with mentors. The program has various subgroups, including groups for women practicing in community NICUs, groups for specific interests like global health or lab research, and groups for women from backgrounds that tend to be underrepresented in medicine.
Neonatology mentorship at Boston Children’s: Balancing medicine, research, and family
Patricia Davenport, MD, and Martha Sola-Visner, MD, neonatologists at Boston Children’s, illustrate the value of mentorship. As a junior faculty member, Davenport found herself juggling her clinical, research, and family responsibilities. In addition to caring for patients in the NICU, she joined Sola-Visner’s lab to conduct research on neonatal platelet transfusions. Sola-Visner quickly became a mentor.
“Martha’s mentorship has been crucial to me,” Davenport says. “She values her patients, her research, and her family. Holding those three things equally in your hands is really important. I had never done basic science before and needed a lot of mentoring, not just at the bench but also writing and presenting.”
Whether it’s an unfortunate patient outcome, an experiment that didn’t work, or a family emergency, Sola-Visner has been a vital support and sounding board. And the benefits of mentorship flow in both directions.
“I’m established now, and at this stage in my career, seeing other people progress and move forward is the most rewarding part of what I do,” says Sola-Visner. “Making sure that the people who I’ve mentored are succeeding becomes more and more important over time. I get great joy to see that.”
Davenport is also an enthusiastic participant in the national pilot mentorship program, where she is part of a subgroup on basic science.
“We talk about funding difficulties, how to organize a lab, wellness, how to care for yourself,” she says. “There’s a real sense of community across the nation. You’re always asking, ‘am I good enough?’ and it’s nice to hear other women having the same thoughts and feelings of ‘imposter syndrome.’ But we’re all doing good work.”
Key Points Original Investigation Public Health December 19, 2024
Question Is physical activity during pregnancy associated with preterm birth among women with gestational diabetes (GD)?
Findings In this cohort study of 1427 pregnant women with GD, accelerometer-derived moderate-to-vigorous intensity physical activity (MVPA) demonstrated an inverse association with preterm birth. The dose-response curve for MVPA in relation to the risk of preterm birth exhibited an L-shaped pattern, with a steady decline in preterm birth rate up to approximately 74 minutes per day.
Meaning These findings provide key evidence for the health benefits of MVPA during pregnancy and lay the foundation for establishing physical activity guidelines for pregnant women with GD.
Abstract
Importance Physical activity, as a modifiable factor, emerges as a primary intervention strategy for the prevention and management of gestational diabetes (GD). Among women with GD, the association of physical activity during pregnancy with preterm birth remains unclear.
Objective To examine the association of accelerometer-derived physical activity metrics and patterns with preterm birth among women with GD.
Design, Setting, and Participants This prospective cohort study recruited pregnant women with GD in Hangzhou, China, from August 2019 to August 2023 as part of the Westlake Precision Birth Cohort study. Statistical analysis was performed between August and November 2023.
Exposures Wearable accelerometer–derived physical activity metrics and patterns. Measurements of physical activity via wearable accelerometer were performed at a median (IQR) of 25.4 (24.6-26.6) weeks’ gestation.
Main Outcomes and Measures Preterm birth was determined through the examination of delivery records. Incident preterm birth was defined as the delivery of infants before completing 37 weeks of gestation.
Results Among the 1427 women meeting the inclusion criteria, the mean (SD) age was 31.3 (3.8) years, and there were 80 cases of preterm birth. An increase in moderate-to-vigorous intensity physical activity (MVPA) and the fraction of physical activity energy expenditure derived from MVPA exhibited an inverse association with preterm birth, with an odds ratio per 30 minutes of 0.64 (95% CI, 0.42-0.98) and an odds ratio per SD of 0.69 (95% CI, 0.55-0.88). In the dose-response analysis, there was a progressive decrease in the odds of preterm birth with increasing duration of MVPA per day, reaching a plateau at approximately 74 minutes per day. Furthermore, the findings indicated that active MVPA (MVPA ≥30 minutes per day), whether it was concentrated into a few days or followed a more regular pattern, had similar beneficial association with preterm birth.
Conclusions and Relevance In this prospective cohort study, MVPA during pregnancy exhibited an inverse association with preterm birth among women with GD. Concentrated physical activity was associated with similar benefits in reducing preterm birth risk as regular physical activity.
Two years ago, Adiah and Adrial Nadarajah defied the odds when they were born at just 22 weeks at Mount Sinai Hospital.
The twins, who share the Guinness World Records for the youngest and lightest premature babies born, recently celebrated their second birthday, and we caught up with the family to find out how they’re doing.
Things certainly are much different in the Nadarajah household these days. “The first year of their lives was spent constantly tending to their medical needs,” reflects Shakina. And today, as the twins’ mother puts it, the family is now in the phase of “full throttle toddler parenting.”
“In the first year, the twins didn’t have much recognition of each other, so it’s beautiful to see how close they are becoming,” says Shakina. “Adrial is very affectionate and is always trying to hug his sister. He has started saying a few words too.” Some of which include: banana, potato, purple, car and of course – mama and papa.
Adiah is “the bossy one,” calling all of the shots when it comes to play time. She loves reading books, and given that both of her parents play the piano, Adiah has been naturally drawn to it.
“She is mesmerized by the piano and enjoys watching us play on it, or playing it herself,” says Shakina. “That is how she spends quality time with her dad, Kevin.”
The younger twin, Adrial was on oxygen for a period of time following a re-hospitalization after their discharge from the NICU, but went off it shortly after the twins’ first birthday. And while checking oxygen tanks and figuring out wiring across the house were not what they envisioned for their first year of parenthood, these add to their unique story of parenthood and to the twins’ story of resilience.
The twins continue to attend standard follow up appointments at Mount Sinai Hospital’s neonatal follow-up clinic, which provides families with developmental assessments for their infant(s) who received care in the NICU, and also counselling for early intervention, depending on the needs of children. The detailed assessment of a baby’s growth, feeding and development includes movement patterns, speech, play skills and problem-solving abilities, and guides families in supporting activities to enhance their development to the full potential.
“Infants who spend an extended period of time in the NICU can face long-term challenges, which is why it is important to continuously monitor these children to identify any challenges they may face as early as possible,” says Dr. Prakesh Shah, Paediatrician-in-Chief at Sinai Health. “This allows us to proactively provide optimal support, planning and timely therapy referrals for families.”
The twins were referred to different specialists, including a speech therapist, physiotherapist and an occupational therapist, and continue to get support on an ongoing basis.
“This family is a living example of what hope can do,” says Dr. Shah. “The family continuously advocated for their babies and persevered and now the twins are two years old, defying many odds.”
Although so much has changed for the Nadarajah family over the past two years, Shakina shares that “not a single day goes by” that they don’t think about the Mount Sinai Hospital NICU.
“It holds such a special place in our hearts, and was where we spent the first half year of our babies’ lives. It was our everything – our whole world. And it was amazing to have the support we received from the hospital, especially in the first year.”
The first app of its kind to offer information SPECIFIC to the weekly growth and development of the premature baby.”
“A comprehensive guide for parents of premature babies that helps to reshape the NICU experience. Providing and educational and empowering platform to document, record, and celebrate their preemie’s story.”
“The Peekaboo ICU PREEMIE App is inspiring parents and making an impactful difference for NICU families.”
INNOVATIONS
Advancements in Neonatal Technology: What’s New in 2024?
Jun 29, 2024
The realm of neonatal care has always been a critical aspect of medical science. The delicate nature of newborns, especially preterm infants, necessitates constant innovation and improvement in technology.
As we advance through 2024, several groundbreaking developments are revolutionizing neonatal care, ensuring better survival rates and improved health outcomes for infants. In this blog, we will delve deeper into the significant advancements in neonatal technology that are shaping the landscape this year.
Neonatal Intensive Care Units (NICUs): Modern NICUs are increasingly integrating smart technology and artificial intelligence (AI) to enhance care delivery. In 2024, many hospitals have adopted AI-driven monitoring systems that continuously analyze vital signs and predict potential complications before they become critical.
The modern NICUs use machine learning algorithms to identify patterns that may be missed by human observation, providing early warnings for serious medical conditions. In fact, more seizures are recorded in real-time when the AI algorithms are applied.
Additionally, NICUs are now equipped with advanced incubators that offer more than just a controlled environment. These incubators come with integrated sensors that monitor temperature, humidity, oxygen levels, and even the infant’s movements. Real-time data from these sensors helps healthcare providers make immediate adjustments to optimize the infant’s environment, significantly reducing the risk of complications.
Telemedicine and Remote Monitoring: Telemedicine has become a crucial tool in neonatal care, particularly in remote or underserved areas. In 2024, advancements in telehealth technology allow for real-time video consultations between neonatologists and local healthcare providers.
Remote monitoring technology has also made significant strides. Wearable devices designed for neonates can now continuously track vital signs and other health metrics, transmitting data to healthcare providers instantly. These devices are minimally invasive, ensuring that they do not interfere with the infant’s comfort while providing critical health information.
Respiratory Support: Respiratory support is a cornerstone of neonatal care, especially for preterm infants whose lungs are not fully developed. In 2024, advancements in this area are particularly noteworthy.
The high-frequency ventilation and non-invasive procedures are two examples of innovations in the respiratory support systems that have been able to improve the prognosis for neonates suffering from respiratory distress syndrome. These developments also lower the likelihood of long-term problems by offering mild and efficient breathing assistance.
Furthermore, innovations in surfactant therapy, which helps to reduce the surface tension in the lungs and keep the airways open, are enhancing the survival rates and respiratory outcomes for preterm infants.
Personalized Medicine and Genomics: Personalized medicine is transforming neonatal care by customising treatments to the individual needs of each infant. Advances in genomic sequencing allow for the early identification of genetic disorders enabling targeted interventions.
In 2024, whole-genome sequencing is becoming more accessible and faster, allowing for timely diagnosis and treatment of congenital conditions. Pharmacogenomics, which studies how genes affect a person’s response to drugs, is also making its way into neonatal care.
Advanced Imaging Techniques: Imaging technology has seen remarkable improvements, providing clearer and more detailed views of neonatal anatomy and physiology. High-resolution screening devices such as CFM Olympic Brain Monitor specifically designed for neonates are now available, offering non-invasive ways to screen brain conditions.
In addition, there are other advanced imaging techniques help in early detection of issues such as brain injuries, congenital heart defects, and other critical conditions, allowing for prompt and appropriate interventions.
Parental Involvement and Support Technologies: A number of technologies have been introduced in 2024 to encourage parental involvement in neonatal care, in recognition of the vital role that parents play in this process.
Throughout their child’s time in the NICU, parents are offered resources to remain informed, involved, and supported. Furthermore, specially made wraps and clothes are making skin-to-skin contact—also referred to as Kangaroo care. These items enable parents to comfortably hold their infants while providing the essential medical supervision and assistance.
Summing It Up:
The advancements in neonatal technology in 2024 are profoundly transforming the care and outcomes for newborns, especially those born prematurely or with critical conditions.
As technology continues to evolve, the hope is that these advancements will become accessible to all, ensuring that every newborn receives the highest standard of care, regardless of their circumstances.
Despite healthcare improvements in Rwanda, newborn mortality remains high. This study assesses the impact of neonatal mentorship on enhancing nurses’ competencies within neonatal units, aiming to address this mortality concern and strengthen healthcare providers’ abilities.
Methods
The prospective cohort study included 25 health facilities supported by Ingobyi Activity in Rwanda, which were beneficiaries of a monthly mentorship program focusing on five critical neonatal competencies. These included adopt manipulation of neonatal equipment, effective management of small and sick newborns, stringent infection prevention and control (IPC), kangaroo mother care (KMC) implementation, and family-centered care provision. We employed an observation checklist to measure neonatal practice competencies, comparing practices at the time point of the baseline, at the 6th mentorship session, and finally at the 12th mentorship session.
Results
The program engaged 188 neonatal nurse mentees. Data analysis highlighted a substantial increase in overall neonatal practice competencies from a baseline of 42.7%–75.4% after 12 mentorship sessions. Specific competency enhancements included family-centered care (40.3%–70.3%), IPC (43.2%–84.2%), KMC (56.9%–73.3%), management of small and sick newborns (38.5%–77.6%), and manipulation of neonatal equipment (42.7%–75.4%).
Conclusions
This neonatal mentorship program was effective in enhancing nursing competencies, leading to significant improvements in neonatal care practices. Future work should evaluate the program’s cost-effectiveness and explore its potential to positively impact neonatal health outcomes, thus ensuring sustainable healthcare advancements.
We are delighted to present an editorial for the Special Issue ‘Advances in Healthcare for Neonates’. This Special Issue is a testament to the excellent quality of the eleven articles submitted in the short span of just one year, far exceeding our expectations. We are humbled by the commitment of the scientific community to pursue neonatal research across the globe, which bodes well for improvements in quality of life as newborns grow into children and adults.
The survival of extremely preterm infants in the past few decades is closely linked to the discovery of surfactants in the early 1990s. Advances in neonatal care, including parenteral nutrition, gentle ventilation, and infection control practices, have further contributed to the increasing survival of extremely low birth weight (ELBW) infants. The extensive use of continuous positive airway pressure (CPAP) and non-invasive ventilation (NIV) techniques is essential for the close monitoring of infants on NIV to ensure appropriate clinical decision-making. One such method is standardizing the weaning process when using non-invasive ventilatory support. Nussbaum et al. attempted to standardize the weaning of NIV using the Silverman–Andersen score (SAS). The study did not find any differences among the groups, highlighting the fact that various factors, including interrater reliability, influence weaning from NIV, thereby limiting the predictive value of the SAS. However, the study addresses an important knowledge gap in weaning infants on NIV off respiratory support.
Neonatal units have traditionally used chest X-ray for the diagnosis of respiratory disorders in neonates. However, more recently, lung ultrasound has emerged as a useful clinical tool at the bedside. Ismail et al. have demonstrated that imaging using lung ultrasound can not only be used as an alternative to chest X-ray, but also as a high-precision tool for diagnosing various respiratory diseases in neonates, such as respiratory distress syndrome, pneumonia, transient tachypnea of the newborn, meconium aspiration syndrome, pneumothorax, and atelectasis. Incorporating point-of care-ultrasound scanning in scientific studies and training programs would certainly enhance the existing clinical applications of ultrasound, thus helping to advance the care of neonates.
Despite advances in neonatal care leading to the increased survival of ELBW infants, premature infants are at an increased risk of adverse long-term neurodevelopmental outcomes, including cerebral palsy. Assessment of motor movements based on heart rate is a novel way of detecting abnormal pathologies that could help in earlier detection of cerebral palsy. In this Special Issue, Maeda et al., from Japan, present an algorithm to extract the movement patterns of premature neonates, as assessed through a combination of heart rate and video recordings of general movements. The authors demonstrated that it is possible to use an algorithm-based approach to assess general movements using instantaneous heart rate monitoring; however, they caution that it is essential to distinguish artifacts, such as a care intervention, using a supplemental video recording . Nevertheless, as fetal movements indicate fetal wellbeing, movement pattern assessment using algorithmic tools could be valuable for assessing motor and cognitive functions in premature infants after birth.
Early diagnosis and appropriate intervention can minimize the risk of developmental delays sometimes seen in premature neonates. A randomized controlled study comparing standardized early physical therapy versus no intervention in preterm infants from 32 weeks of gestation to 2 months corrected age demonstrated no differences between the group. However, factors such as the dose, intensity of intervention, parental compliance, and the shorter duration of intervention might have contributed to an absence of difference between the groups. The authors also highlight that engaging with and educating parents demonstrating poor compliance with therapy techniques for prolonged periods is essential to derive benefits .
Implementation of neuroprotective care in the neonatal intensive care unit is essential for optimal neurodevelopmental outcomes in premature neonates. Therefore, reducing pain is critical for neuroprotective care in premature infants. Dusek et al. studied the possibilities of influencing the procedural pain associated with retinopathy of prematurity (ROP) screening using oral clonidine. The authors assessed the pain and vegetative scores of using oral clonidine versus standard care during routine ROP exams. Although they did not demonstrate any difference between the groups, the absence of severe complications with clonidine may make it a potential candidate in future studies addressing neonatal pain.
The clinical care of neonates is the focus of this Special Issue. Traumatic lumbar puncture (LP) has been a problem confounding the diagnostic evaluation of neonates, especially in extremely low birth weight infants. In addition to ensuring the proceduralist′s technique, skills, and experience, it is also essential to use the correct size of needle when performing a procedure. In a study in this Special Issue, a smaller gauge (25G) lumbar puncture needle not only resulted in a decreased incidence of traumatic LP, but also a reduction in desaturation episodes during the procedure. This study is a step in the right direction for providing neuroprotective care to these fragile infants. Future studies should address optimal positioning, non-invasive imaging techniques to facilitate easier insertion, and needle size stratification based on gestational age or birth weight in order to optimize the success of vital neonatal procedures.
Improving the outcomes of neonates is best accomplished by preventing hospital-acquired infections and ensuring the optimal screening of newborns in the intensive care unit. The World Health Organization has described antimicrobial resistance as a serious threat to public health; hence, screening fragile infants for multidrug-resistant microbes is essential. Out born infants admitted to neonatal units in Turkey were meticulously screened using perirectal swab cultures and were found to have a 27.2% and 4.8% positive screening rate for carbapenem-resistant Enterobacterales (CRE) and vancomycin-resistant Enterococci (VRE), among the 125 referrals from the outside hospitals. This result reinforces the need for antibiotic stewardship to prevent multidrug resistance, and high vigilance and attention to screening when these vulnerable neonatal patients are referred from centers in which antibiotic policies are unclear.
Next-generation sequencing (NGS) and exome and genome sequencing using targeted panel molecular genetic analysis have contributed significantly to advances in newborn care. In this issue of Advances in Newborn Care, Zaza et al. describe a neonate with a cleft palate and an aortic root aneurysm, with a pathogenic mutation of exon 8 of TGFBR2 confirming a diagnosis of Loeys–Dietz syndrome. Advances in molecular genetics will help better diagnose rare conditions using genetic mutations, thus contributing to earlier detection of conditions and better management of these infants. Neonates with special conditions and genetic syndromes require a higher level of care and treatment strategies, and standardized tools to enhance their recovery. Vogt et al. propose an enhanced recovery protocol for patients undergoing the Kasai procedure for biliary atresia. The checklist includes, among other elements, parental education, preoperative dextrose-containing fluids, maintaining normothermia, adequate analgesia, and initiation of early feeds. The checklists almost always provide a framework for clinicians to optimize outcomes in complex patients such as those requiring the Kasai procedure.
With the increasing survival of premature infants, many patients go home with an accompanying increase in respiratory morbidities post-discharge. The widespread use of palivizumab helps to reduce re-admission rates and complications from infection with respiratory syncytial virus. The feasibility of home immunization with palivizumab without any serious adverse events is reported in this Special Issue . The advantages of home immunizations include higher parental satisfaction and well-being for the whole family. This study is a step towards personalized medicine within a unique population, which may help them to avoid visiting the hospital or clinic and potentially being exposed to children with other droplet infections. On the note of personalized medicine, there is an increase in the growing adult population who were born prematurely and are thus at extremely high risk of developing various comorbidities such as systemic hypertension, metabolic syndrome, reduced exercise tolerance, pulmonary hypertension, chronic obstructive pulmonary disease, and cardiac failure. Holistically addressing the problems of adults born preterm will help promote cardiovascular health, wellness, and quality of life over their lifetime. Despite the large number of resources invested in the survival and care of extremely premature infants, it is surprising that minimal resources are available regarding commitment to wellness as infants grow into children and adults. Vital screening programs, effective communication, targeted counseling and therapeutic interventions, and a seamless transition of care from a pediatric clinician to an adult health care provider would improve the quality and longevity of life of those born extremely preterm.
Infants Exposed to Substances Prenatally Also Have Increased Exposure to Unsafe Sleep Practices
Unsafe sleep practices may be a more common cause of sudden unexpected infant death cases where children are born exposed to drugs, according to a new study. The article, “Sleep-Related Sudden Unexpected Infant Death Among Infants Prenatally Substance Exposed,” published in the December edition of Pediatrics, looked at data from the Centers for Disease Control and Prevention SUID and Sudden Death in the Young Case Registry. Data showed that of 2,010 infants with sleep related deaths, 14% had been born drug exposed with nearly a third of all infants dying from suffocation. Among the sleep-related deaths, about half happened in an adult bed with infants sharing the space with a sleeping adult. Overall, 1 in 4 deaths of prenatally exposed infants involved supervisors who were both impaired and bedsharing. Non-Hispanic white infants were disproportionately impacted, making up nearly half of those prenatally exposed who died in their sleep. These infants were also more likely to be exposed to social drivers of poor health and family vulnerability such as poverty and barrier to prenatal care. Study authors advocated for expanded prevention efforts such as safe sleep messaging while arguing more needs to be done to address the social needs of these families.
The American Academy of Pediatrics is an organization of 67,000 primary care pediatricians, pediatric medical subspecialists and pediatric surgical specialists dedicated to the health, safety and well-being of infants, children, adolescents and young adults.
A genetic signature in newborns can predict neonatal sepsis before symptoms even start to show, according to a new study
The study, led by UBC and SFU researchers in collaboration with the Medical Research Council (MRC) Unit The Gambia, has the potential to help healthcare workers diagnose babies earlier, including in lower- and middle-income countries (LMICs) where neonatal sepsis is of particular concern. The research, published today in eBiomedicine, is funded by the National Institutes of Health and the Canadian Institutes of Health Research.
“Neonatal sepsis is caused by the body’s irregular response to a severe infection that occurs within the first 28 days of life. Globally, it affects around 1.3 million babies annually, and unfortunately, in LMICs, those rates are higher,” said first author Andy An, a UBC MD/PhD student who completed the research as a doctoral student in the department of microbiology and immunology. “Even when treatment is successful, sepsis can have lifelong effects because it can lead to developmental delay in children, imposing cognitive deficits and long-term health issues. By recognizing it as early as possible, we can treat infants promptly and ideally, head off these harms.”
Neonatal sepsis causes an estimated 200,000 deaths worldwide each year, with the highest rates in LMICs. In Canada, the risk is lower at about one in 200 live births, but higher in prematurely born babies.
Rolling the dice on health
Diagnosing sepsis is challenging for doctors and families. The symptoms can look like many other illnesses, and tests to check if sepsis is present can take several days, aren’t always accurate, and are largely only available in hospitals. The uncertainty can delay urgent treatment with antibiotics.
“Knowing that sepsis is impending would also allow physicians more time to determine the appropriate treatment to use,” said co-senior author Dr. Bob Hancock, professor in the UBC department of microbiology and immunology. “The consequences of neonatal sepsis are so severe in the most vulnerable individuals that providing an early diagnosis to assist and guide physicians could save lives.”
Equitable access to healthcare
The researchers participated in a large study in The Gambia where blood samples were taken from 720 infants at birth. Out of this cohort, 15 babies developed early-onset sepsis.
The researchers used machine learning to map the expression of genes active at birth, in search of biological markers that could predict sepsis.
“We found four genes that, when combined in a ‘signature’, could accurately predict sepsis in newborns nine times out of 10,” said co-senior author Dr. Amy Lee, assistant professor in the SFU department of molecular biology and biochemistry. “This was a unique opportunity where samples were available from all babies in this cohort on the day of birth, meaning we could study the genes expressed in the sepsis babies before they got sick. Most other studies have only published markers that were present when the babies were already ill, and this would therefore not be a predictive signature.”
“The early recognition of sepsis is vital for infants’ survival, and identifying markers that might allow us to ‘predict’ babies at particular risk would be an enormous advantage, since we could then target specific surveillance and treatment of such infants,” said Dr. Beate Kampmann, who led the clinical component of the study at the MRC Unit in The Gambia.
The researchers hope the signature will one day be incorporated not only into PCR tests in hospitals, but also in portable, point-of-care devices.
“There are point-of-care devices available that can test for gene expression, for instance, COVID-19 and influenza, with a single drop of blood. They can operate anywhere with a power source including batteries and can be used by anyone, not just trained healthcare providers,” Dr. Hancock. “These portable devices could be retooled to recognize this ‘signature’ relatively easily and inexpensively.”
The next step for the research would involve a large prospective study to show the signature is successful at predicting sepsis in other populations and prove its methodology, and then the development of point-of-care tools for approval by relevant government bodies.
Ready to kick off the new year with fresh goals and BIG dreams? This fun and interactive video is perfect for kids, parents, and educators! We’ll share simple and achievable New Year’s resolution ideas for kids to help them learn goal-setting in a positive and exciting way.
Welcoming the New Year with Hope and Resilience
As preemie warriors, we step into 2025 with gratitude and pride, not just for how far we’ve come but for the people who made our journey possible. This new year is a moment to reflect on the strength and resilience that define us—and to honor the families, parents, caregivers, and healthcare providers who stood by us every step of the way.
Our journey has been shaped by many. For some, families and communities stood as steadfast advocates, offering love and support through difficult decisions and uncertain times. For others, healthcare providers brought their expertise and compassion to the forefront, working tirelessly to help achieve the best possible outcomes. Together, these connections have been a source of strength, ensuring care and hope in moments that mattered most.
2025 is a celebration of this community of support. Together, we’ve proven that resilience is a collective effort. Every milestone we’ve reached—every breath, every step, every moment of growth—is a shared triumph, a testament to the power of unity and the impact of care.
This year, let’s continue to inspire and uplift one another. Our stories remind the world that we as preemie warriors have so much to offer, and that progress in neonatal care depends on the passion and dedication of our neonatal womb community, preemie warriors, families, and professionals alike. By sharing our journeys, we create a ripple effect—sparking change, advancing care, and building a future where every preemie has the best chance to thrive.
Here’s to 2025: a year to honor the bonds that sustain us, the progress we’ve made, and the hope we carry forward. Together, we rise, stronger and more united than ever.
CGI Animated Short Film: “Miles to Fly” by Stream Star Studio | CGMeetup
Follow your Dreams – Miles to Fly is a graduation short made by 4 students from Multimedia University, Malaysia released in 2020. The story is about an ambitious boy who dreams of becoming a pilot but is torn between helping his mother’s bakery to survive, or pursuing his dream.
Scotland is a country that is part of the United Kingdom. It contains nearly one-third of the United Kingdom’s land area, consisting of the northern part of the island of Great Britain and more than 790 adjacent islands, principally in the archipelagos of the Hebrides and the Northern Isles. To the south-east, Scotland has its only land border, which is 96 miles (154 km) long and shared with England; the country is surrounded by the Atlantic Ocean to the north and west, the North Sea to the north-east and east, and the Irish Sea to the south. The population in 2022 was 5,439,842 and accounts for 8% of the population of the UK. Edinburgh is the capital and Glasgow is the largest of the cities of Scotland.
There are an estimated 29 million nurses worldwide and 2.2 million midwives. WHO estimates a shortage of 4.5 million nurses and 0.31 million midwives by the year 2030.
That will bring the a global shortage of health workers estimated for 2030 to 4.8 million nurses and midwives, with the greatest gaps found in countries in Africa, South-East Asia and the WHO Eastern Mediterranean Region, as well as some parts of Latin America.
Nurses and midwives play a pivotal role in improving health and contributing to the wider economy. Investing in them is imperative to achieve efficient, effective, resilient and sustainable health systems. They not only provide essential care but also play a critical role in shaping health policies and driving primary health care. Nurses and midwives deliver care in emergency settings and safeguard the sustainability of health systems globally.
More than 80% of the world’s nurses work in countries that are home to half of the world’s population. And one in every eight nurses practices in a country other than the one where they were born or trained.
Higher levels of female nurses are positively correlated with health service coverage, and life expectancy and negatively correlated with infant mortality.
Overview
Nurses and midwives are central to Primary Health Care and are often the first and sometimes the only health professional that people see and the quality of their initial assessment, care and treatment is vital. They are also part of their local community – sharing its culture, strengths and vulnerabilities – and can shape and deliver effective interventions to meet the needs of patients, families and communities.
WHO response
WHO’s work relating to nursing and midwifery is currently directed by World Health Assembly resolution WHA74.15 (2021) which calls on WHO Member States and WHO to strengthen nursing and midwifery through the Global Strategic Directions for Nursing and Midwifery (SDNM) 2021–2025. The SDNM is an interrelated set of policy priorities that can help countries to ensure that midwives and nurses optimally contribute to achieving universal health coverage (UHC) and other population health goals .
The SDNM comprises four policy focus areas: education, jobs, leadership, and service delivery Each area has a “strategic direction” articulating a goal for the five-year period, and includes between two and four policy priorities If enacted and sustained, these policy priorities can support advancement along the four strategic directions: 1) educating enough midwives and nurses with competencies to meet population health needs; 2) creating jobs, managing migration, and recruiting and retaining midwives and nurses where they are most needed; 3) strengthening nursing and midwifery leadership throughout health and academic systems; and 4) ensuring midwives and nurses are supported, respected, protected, motivated and equipped to safely and optimally contribute in their service delivery settings.
WHO engages ministries of health, the Government Chief Nurses and Midwives (GCNMOs) and other relevant stakeholders to enable effective planning, coordination and management of nursing and midwifery programmes in countries. The Global Forum for the Government Chief Nurses and Midwives, established in 2004, is organized by WHO and meets every two years. It is a Forum for senior nursing and midwifery officials to develop and inform areas of shared interest. WHO also engages with academic institutions specialised in nursing and midwifery. Forty-seven academic centres are designated as Collaborating Centres for Nursing and Midwifery with WHO. The academic centres are affiliated to the Global Network of WHO Collaborating Centres for Nursing and Midwifery.
WHO has established a Nursing and Midwifery Global Community of Practice (NMGCoP). This is a virtual network created to provide a forum for nurses and midwives around the world to collaborate and network with each other, with WHO and with other key stakeholders (e.g WHO collaborating centres for nursing and midwifery, WHO Academy, Nursing and Midwifery Associations and Institutions.) The network will provide discussion forums, a live lecture programme, opportunities to develop and share policies, WHO documents and tools, and facilitated innovation workshops, masterclasses and webinars.
The Nursing and Midwifery Global Community of Practice is free to join and available to nurses and midwives everywhere.
From May 2022 it will be possible to access the virtual community via a smartphone, by downloading the Nursing and Midwifery Global Community of Practice App Nurses Beyond the Bedside_WHO_CSW66 Side Event available for Android and IOS system via the APP store.
Watch this amazing Scottish artist sing Yellow by Coldplay with me! @AndrewDuncan
Open Access to Neonatal Drug Development Education Modules
Mary A. Short MSN, RN – Volumn19/Issue 5 May 24
Critical Path Institute (C-Path) announces the launch of Bridging the GAP: Empowering Neonatal Nurses in Drug Development for Neonates, a comprehensive series covering the history of neonatal drug development, approaches to promote drug development for neonates, pharmaceutical industry decision-making processes, and strategies for advocating neonatal needs. Developed in collaboration between its International Neonatal Consortium (INC) and the National Association of Neonatal Nurses (NANN), this series aims to empower neonatal nurses and interested neonatal health care professionals with the knowledge needed to actively participate in research and ensure better outcomes for our tiniest patients.
“As an organization committed to advancing neonatal research and care, we recognize the vital role nurses and clinicians play in the hospital setting,” said INC Executive Director Kanwaljit Singh, MD, MPH. “This collaboration with NANN represents a pivotal step forward in our mission to support and empower neonatal nurses and clinicians. By engaging them in developing these educational modules, we aim to enhance their understanding and involvement in neonatal clinical trials and drug development.”
The modules aim to provide foundational knowledge on innovative, regulated medicines development for neonates, including pipeline decision-making factors and addressing neonatal needs within the current environment. Upon completion of the presentations and activity evaluations, participants can earn up to 4.5 FREE CE credits and 2.56 FREE pharmacology credits. NANN is an accredited provider of nursing continuing professional development recognized by the American Nurses Credentialing Center’s Commission on Accreditation. The content is appropriate for AMA PRA Category 2 Credit. The presenters reflect the diversity of neonatal stakeholders, as illustrated in Figure 1, which outlines the module titles and the presenters involved.
Background:
Neonates are therapeutic orphans, underserved by the drug development community, and lag in the development of new, safe, and effective therapies. Most NICU drugs are off-label, impacting their safety and efficacy evaluation. Nurses play a vital role in administering medications and monitoring their effects but often lack a comprehensive understanding of clinical trials and drug development processes in the NICU. Critical Path Institute (C-Path) is an independent nonprofit established in 2005 as a public-private partnership in response to the FDA’s Critical Path Initiative. C-Path’s mission is to lead collaborations that advance better treatments for people worldwide. Globally recognized as a pioneer in accelerating drug development, C-Path has established numerous international consortia, programs, and initiatives that currently include more than 1,600 scientists and representatives from government and regulatory agencies, academia, patient organizations, including parent/family advocates, nursing organizations, disease foundations, and pharmaceutical and biotech companies. INC, established in 2015 as a public-private partnership within the construct of C-Path, advances the unmet drug development needs in the neonatal population.
INC conducted a multistakeholder (neonatologists, neonatal nurses, parents) survey to explore communication practices and stakeholders’ perceptions and knowledge regarding the conduct of clinical trials in the NICU. Survey results indicated that most neonatologists (82%) responded that medications are insufficient to meet the needs of critically ill neonates and identified a knowledge gap for nurses regarding drug development. Degl et al. conclude that the engagement of nurses at all stages of neonatal research is suboptimal and indicates a need for nurses to be educated about research. Beauman et al. report additional findings specific to nurse respondents from the multistakeholder survey. Nurses expressed a learning need because they historically lacked effective education to prepare them for competent participation in neonatal research, especially in informing study design. The authors recommend leveraging neonatal nurses’ unique and essential role as key stakeholders from the onset of the study design to enhance the conduct of neonatal clinical research and improve care for premature and sick neonates.
To address the survey findings, industry representatives held an education workshop on Pharmaceutical Drug Development for Neonates at the 2019 INC Annual meeting intended for all neonatal stakeholders, including academics, clinicians, and regulators. The INC Communication Workgroup updated the content for the recently launched education modules, emphasizing the significance of the information for nurses, but the content remains relevant to other neonatal healthcare professionals.
Product Description:
“Consistent with our mission to elevate and transform neonatal care, NANN is grateful to bring forth this important collaboration with INC and give all neonatal nurses access to these outcome improving modules,” said NANN Executive Director Molly Anderson. “We know neonatal nurses have the expertise and knowledge to play an essential role in drug development that benefits their patients. NANN seeks out partnerships with organizations like INC that allow us to empower deepened nurse involvement with all aspects of care throughout their careers.”
The series includes access to seven on-demand video modules related to nurse-informed neonatal study design for drug development to provide context for the importance and implications for neonatal nurses. The NANN iLEARN site provides a platform for open access. Share the product flyer with colleagues to provide the QR code for access.
Antibiotics are life-saving drugs and essential for the treatment of many serious infections, but widespread inappropriate use is now common and has become a major contributor to the development of antibiotic resistance (ABR). ABR is an urgent global public health and socio-economic threat, generating calls for actions from the World Health Organization and the US Centers for Disease Control and Prevention (CDC). Left unchecked, ABR is poised to reverse a century of medical progress, rendering antibiotics ineffective in treating even the most common infectious diseases. Infants admitted to neonatal intensive care units (NICUs) are at high risk for the development and transmission of multidrug-resistant pathogens, particularly where hospital stays are prolonged because of prematurity or congenital anomalies.3 Worldwide, sepsis is the third leading cause of neonatal mortality, with antibiotic resistant pathogens responsible for approximately 30% of deaths.
Antibiotics are the most common medication prescribed in NICUs, with wide variability in use, regardless of the level of care or complexity of patients.5 On any given day, 40% of infants admitted to a NICU are prescribed antibiotics, with an estimated 90% exposed to antibiotics over the duration of their NICU stay. A recent study published in The Lancet Regional Health-Southeast Asia found that the most commonly prescribed antibiotics in Southeast Asia are now only 50% effective at treating sepsis and meningitis in newborns. Furthermore, there is increasing evidence that preterm infant antibiotic exposure is associated adverse outcomes including alteration in the intestinal microbiome, necrotizing enterocolitis, invasive fungal infections, retinopathy, and late-onset sepsis.5 Early life antibiotic exposure is also associated with future health problems including childhood obesity, asthma, allergic disorders, and inflammatory bowel disease. Therefore, it is important to find strategies to reduce antibiotic use in the NICU patient population.
ANTIBIOTIC STEWARDSHIP
According to the Society for Healthcare Epidemiology of America, the Infectious Diseases Society of America, and the Pediatric Infectious Diseases Society, the major objective of antibiotic stewardship (AS) is to achieve the best clinical outcomes related to antibiotic use while minimizing toxicity and other adverse events, thereby limiting the emergence of ABR bacterial strains. AS – a core strategy to combat ABR – is intended to ensure patient safety through the implementation of combined, coordinated interprofessional interventions to optimize how antibiotics are used. Studies indicate that the implementation of AS initiatives in NICUs is associated with a significant decrease in the overall days of therapy and reduction in use of broad-spectrum antibiotics, such as cephalosporins, without adverse issues. However, significant gaps exist between CDC recommendations to improve antibiotic use and antibiotic practices during the neonatal and newborn period. Until recently, AS interventions focused primarily on improving clinician antibiotic prescribing practices through formulary restriction and prospective audit with feedback. However, with more nurses in the frontline of healthcare than any other healthcare profession, the CDC, the American Nurses Association (ANA), the International Council of Nurses and The Joint Commission, have endorsed nurses’ active participation in AS activities to expand the reach and impact of stewardship programs. A recent survey of NICU nurses found that most were familiar with the term AS, yet over half reported administering an antibiotic to a patient who they thought was an inappropriate choice and most reported not questioning the treating provider about antibiotic choice, dose or route of administration.
THE ROLE OF NEONATAL NURSES AND NEONATAL NURSE PRACTITIONER IN ANTIBIOTIC STEWARDSHIP
As trusted professionals, expert clinicians, and advocates for their patient’s health, neonatal nurses and neonatal NPs are well qualified to make significant contributions to the reduction of ABR through active engagement in AS. There are multiple AS activities to consider now.
Advance your knowledge. Read the articles cited in this editorial. Participate in educational opportunities (eg, grand rounds, seminars, webinars) to advance your antibiotic, ABR and AS knowledge. Learn with and from others by starting an interprofessional AS journal club or lunch-and-learn at your practice setting. Contact the National Association of Neonatal Nurses and encourage them to provide state-of-the-science ABR and AS educational sessions specific to neonatal care and evidence-based antibiotic prescribing.
Advocate for the adoption and evaluation of at least one nurse driven AS recommended action in your practice setting. Many preterm infants who do not have infections receive antibiotic treatment in the setting of negative cultures. Consider implementing daily antibiotic timeouts.
Antibiotic time-outs involve a daily formal antibiotic review, often conducted during clinical rounds, to determine if a modification or discontinuation of a patient’s antibiotic therapy is warranted. The time-out approach is in keeping with nurse engagement in prevention of central line-associated bloodstream infections, which includes a daily formal review of central line necessity. Bedside neonatal nurses are well positioned to lead reassessment of antibiotic treatment for they know how long a patient has been receiving antibiotic(s) and when diagnostic test results become available. For additional examples of nursing interventions that may have an important impact on promoting nurse engagement, read the recommendations from the ANA/CDC Workgroup and an article providing a framework to guide AS nursing practice.
Become an antibiotic stewardship champion. Neonates are entitled to receive antibiotic therapy that is based on evidence and best practice, but might be overlooked in hospital AS programs. Build and strengthen partnerships and facilitate communication between the NICU clinical staff and your organization’s AS team (physicians, clinical pharmacists, clinical laboratory personnel). Reach out to the AS team to learn about the overall AS program and specific AS NICU strategies. Engage and educate NICU staff about AS to increase their buy-in and awareness of nursing-related AS practices. Consider AS within the tenets of patient safety, and promote local-level “stewarding” behaviors that tap into the interprofessional NICU team’s collective knowledge, expertise, relationships and wisdom.15 NICU AS nursing practices should be intentionally selected, and strategically align with the organization’s AS program, giving ample consideration to the local context and tailored to the needs and resources of the NICU patients and clinical setting.
Monitor your antibiotic prescribing practices. A core AS strategy is tracking and reporting of provider antibiotic prescribing. Audit and feedback, includes analyzing antibiotic prescribing data and providing feedback to clinicians aimed at helping them understand their antibiotic prescribing habits. These data are most effective when individual results are compared to other clinicians in the clinician’s area and/or specialty (e.g., NNP peer comparisons). If you are a prescriber and are not receiving peer comparison audit and feedback data, work closely with your practice colleagues to develop a process to audit patterns of antibiotic prescribing to gauge appropriateness.
Use evidence-based clinical decision support systems. Clinical decision support systems are electronic tools or software that provide guidance to providers in making both diagnostic and therapeutic choices for patients.16 Applications range from pop-up reminders during a patient encounter, to automated order entry, to electronic guides, including dynamic interactive programs that tailor guidelines to specific patients. Such systems can be particularly useful when applied to antibiotic prescribing. Engage and partner with the NICU clinical team to identify the most useful systems to enhance clinical guideline adherence, decrease antibiotic consumption, or narrow the spectrum of antibiotic usage.
ABR has been aptly described as a subtle, slow moving catastrophe. AS programs aim to optimize antibiotic use to prevent the emergence of resistant pathogens and protect patients from the adverse effects of unnecessary antibiotics. We posit that all NICU nurses have a central role to play in the safe and responsible use of antibiotics and suggest several strategies for NICU nurses to engage in preventing unnecessary antibiotic exposure in this highly vulnerable population. We encourage you to seize the moment and become active, engaged stewards!
Jennifer Degl, MS, Deb Discenza, MA, Mitchell Goldstein, MD, MBA, CML
In contemporary healthcare settings, the role of a Neonatal Intensive Care Unit (NICU) Volunteer Coordinator is indispensable, as it embodies the essence of compassionate care and community support for families navigating the challenges of premature births and neonatal health complications. While volunteer coordinators are often relied upon to fulfill this critical role, it is imperative to recognize the value they bring to the table and advocate for establishing a paid position dedicated to this noble cause.
Parents experience trauma regardless of what level NICU their baby is in and no matter the length of their NICU stay, and so it is vital that we push for a national campaign to address the inequity in order to help families bond and start the healing process before discharge. Not doing so can lead to trauma-related family issues at home. Currently, we largely focus on preparing parents for discharge across all things involving care of the infant. Why would we leave out the important topic of mental health Not addressing this important issue is tantamount to failure for that infant’s long term outcome, not to mention the outcome of the family unit as well. A NICU Volunteer Services Coordinator can alter that trajectory.
The NICU Volunteer Services Coordinator serves as a beacon of hope and support for families enduring the emotional rollercoaster of having their newborn hospitalized. This position encompasses a myriad of responsibilities aimed at fostering a nurturing environment within the NICU, where families feel empowered and supported throughout their journey. From recruiting additional NICU graduate parents to serve as volunteers to organizing crucial training sessions on mental health first aid and active listening, the coordinator plays a pivotal role in equipping volunteers with the necessary skills to provide invaluable support to NICU families.
Furthermore, the coordinator is a liaison between volunteers, nursing staff, and physicians, ensuring seamless communication and collaboration for improving patient care. Facilitating regular meetings and educational events creates opportunities for peer to-peer support among parents and disseminates vital information on neonatal care practices, empowering families to make informed decisions regarding their child’s healthcare journey.
The significance of celebrating milestones and raising awareness cannot be overstated in the NICU setting. The coordinator spearheads initiatives such as NICU Awareness Month/Day and World Prematurity Month/Day, fostering community and solidarity among NICU families and staff. Moreover, their involvement n fundraising activities and grant writing endeavors ensures continued access to resources and services that benefit NICU babies and their families, underscoring their dedication to enhancing the quality of care provided.
Regarding qualifications and working conditions, the NICU Volunteer Services Coordinator must possess a unique blend of empathy, organizational acumen, and leadership skills. While a post-secondary education degree serves as a foundation, firsthand experience as a parent of a NICU graduate and previous involvement in peer mentoring or emotional support roles are invaluable assets. The flexible nature of the position, with a combination of on-site and remote work, accommodates the dynamic needs of NICU families while ensuring that the coordinator remains accessible and responsive to their concerns.
Crucially, advocating for a paid position for the NICU Volunteer Services Coordinator acknowledges the intrinsic value of their role and underscores the commitment of healthcare institutions to prioritize patient-centered care and community engagement. By investing in this position, hospitals enhance the support provided to NICU families and cultivate a culture of compassion and collaboration that is essential for fostering positive health outcomes.
In conclusion, establishing a paid position for the NICU Volunteer Services Coordinator is not merely a bureaucratic formality but a testament to the unwavering commitment of healthcare institutions to uphold the highest standards of patient care and support. By recognizing the invaluable contributions of these dedicated individuals, we affirm our collective responsibility to ensure that every NICU family receives the compassion, guidance, and support they deserve during their journey toward healing and hope. And in the end, the hospital, as a whole, wins substantially through quality improvement scores and community appreciation. It is worth the investment because the benefits are tenfold.
Midwifery Review: Adding Care by Midwives Improves Birth Outcomes
August 15, 2023 – by Robert Forman
Midwife care can improve pregnancy outcomes for mothers and babies, says new “Expert Review” from Yale faculty
The practice of midwifery is less common in the United States than in other countries and other cultures, which is a shame because adding care by midwives generally improves childbirth outcomes, according to two Yale faculty members who have published an “Expert Review” in the American Journal of Obstetrics & Gynecology. Holly Powell Kennedy PhD, MSN,CNM, the Helen Varney Professor of Midwifery, and Joan Combellick, PhD, MPH,CNM, assistant professor of nursing, along with their colleagues, examined the scientific literature related to midwifery and childbirth, and conclude that many measures of successful pregnancy are elevated when midwives play a central role.
They cite the approach to midwifery that is standard in other countries, especially in wealthy European nations, where women have as much as seven times the access to midwives that they do in the United States. They report that midwifery care has improved outcomes by 56 different measures—including lower morbidity and mortality among mothers and newborns, fewer preterm births and low birthweight infants, and reduced interventions in labor.
The authors acknowledge that differences in those countries’ overall health systems make a substantial contribution to good outcomes, but say it’s the integral role of midwives that matters most. “In other countries, midwives make up the basic maternity care provider workforce, and then, obstetricians are used as the specialists that they are, surgeons who are there to handle complications,” says Combellick. “[Midwives] are the experts in normal childbirth, which happens the majority of the time.” Combellick adds that midwives also extend their care beyond pregnancy. “We also do well-person preventive care, across the lifespan from teenagers through postmenopausal people, so it isn’t only pregnancy-related.”
The Value of Midwives at the Baby’s Arrival
But the continuum of pregnancy, birth, and postnatal care is what midwives are best known for, and where the contribution of midwives can differ sharply from what is often considered standard care. Kennedy says a very basic way that outcomes can improve is because prenatal care by midwives is not squeezed into appointments of a set duration, where the provider may not have the time to fully answer the patient’s questions. Kennedy notes that in some settings, midwives caring for a woman throughout the pregnancy bring continuity and can structure longer appointments. Having more time permits building better rapport with a mother-to-be and helps her feel more respected, which often translates into a smoother pregnancy.
“In our paper, we discuss some of the research done about respect. It’s true for any kind of health care, but particularly in prenatal care,” says Kennedy. “It can amount to being highly disrespected and simply having to wait two hours for a very short prenatal visit. If people aren’t feeling respected or safe, they’re less likely to keep coming in for prenatal care.” Combellick adds that this can be especially true for women of color, for whom the cumulative race-based disrespect they endure in their daily lives can make the pressures of pregnancy more intense.
When the time for delivery arrives, a few statistics are especially striking. First-time mothers giving birth at medical centers where midwives were on their care team were 74% less likely to have their labor induced, 75% less likely to receive oxytocin augmentation, and 12% less likely to deliver by cesarean than their counterparts at medical centers without midwives in attendance.
Midwives and Ob/gyns Collaborate During Childbirth
Combellick says that on a collaborative team, the pregnant person is at the center of care, with everyone contributing their particular expertise. Whether to wait and allow labor to continue at its own pace, to induce, or to perform a cesarean can generally be a shared decision that involves patient understanding and consent. “We are collaborators,” says Combellick. “We work in conjunction with physicians. To have two viewpoints thinking about one person is a really strong style of care.”
At Yale, Kennedy and Combellick contribute to the midwifery faculty practice supporting student midwives as they learn. Faculty practice midwives are also active with obstetricians-in-training. “We contribute to the resident training program,” Combellick says. “So the residents, when they first come, are assigned to follow a midwife. Around the country, midwives often play a role in demonstrating ‘here’s what normal physiologic birth looks like,’ and that occurs at Yale.”
Hugh S. Taylor, MD, chair and Anita O’Keeffe Young Professor of Obstetrics, Gynecology & Reproductive Sciences at Yale School of Medicine, says this collaboration has been good for all involved. “It’s important that all of our practitioners get exposure and training on the collaborative practice model. The trainees participate in these teams and get a living example of how collaboration results in outstanding care. It was very important to establish that program—not only for patient care but for our residents and students.”
Taylor says that both for prenatal care and during deliveries, the presence of midwives on the care team can be invaluable. “Most of the prenatal care in our collaborative practice is delivered by midwives, with appropriate escalation and/or referral when things get complicated. If somebody develops diabetes or high blood pressure in pregnancy, we get the physician involved. However, for routine prenatal care or uncomplicated deliveries, we try to keep the physician in the background.”
Kennedy and Combellick both hope that the profile of midwifery in this country will rise, both through growing what Combellick now calls a “relatively small midwifery workforce” that attends only 10 to 12% of births in the United States, and by reforming practices related to health care delivery at large. “It’s not a simple, magical thing about the midwife,” Kennedy concludes, “but really about the model of care: that it’s accessible, it’s available, it’s respectful.” Those changes for the better, they say, would be nothing short of radical, and they are doing their part to gather the available evidence and advocate for change to happen.
Find clinical answers at the point of care or anywhere you need them! Now you can access UpToDate’s current, synthesized clinical information — including evidence-based recommendations — quickly and easily on your iPad, iPhone, or iPod touch.
Notes: To use the mobile app you must first create an UpToDate account. Use this link on the WCMC-Q network to create an account.
Do you need evidence-based answers to clinical questions at the point of care? The First Consult iPhone/iPad app is your solution. The app allows First Consult’s trusted answers to be stored on your iPhone, iPad, or iPod touch. A data connection is required for the initial content download and content updates, but is not required to use the app itself.
Notes: Log in with your ClinicalKey account created from a WCMC-networked computer.
DynaMed Plus™ is the clinical reference tool that physicians go to for answers to clinical questions. Content is written by a world-class team of physicians and researchers who synthesize the evidence and provide objective analysis. DynaMed Plus topics are always based on clinical evidence and the content is updated multiple times each day to ensure physicians have the information they need to make decisions at the point of care.
Note: To use this app begin by clicking on the “Get the DynaMed Plus Mobile App” link on the DynaMed Plus homepage. See this link for more information.
Touch Surgery is an interactive mobile surgical simulator that guides you step-by-step through every part of an operation, and every decision that’s made along the way. It’s the OR in your pocket.
Preop Eval organizes and presents much of the guidance that one needs in order to evaluate and prepare adult patients for non-cardiac surgery. It is based upon the guidelines on this topic from the American College of Cardiology of 2014, the European Society of Anaesthesiology of 2011, , and more. The app contains 1 algorithm and 3 resources: the cardiac evaluation algorithm, guidance on starting and stopping key medications in the perioperative period, guidance on timing of surgery after cardiac events, and guidance on preoperative testing. It also contains a review of preoperative evaluation mainly for students and residents.
AO Surgery Reference is an online repository for surgical knowledge. It describes the complete surgical management process from diagnosis to aftercare for all fractures of a given anatomical region, and also assembles relevant material that the AO has published before.
drawMD General Surgery’s content was developed by physicians and clinical practitioners to facilitate discussion of the most common conditions and procedures. The drawMD platform allows you to easily annotate any condition on our pertinent medical illustration or you can easily upload your own images.
In Scotland, we believe that parenting is one of the most important jobs in the world. The work we do preparing our children for the future will ultimately shape our world in the years to come. With that in mind, we want to make sure that Scotland was the best place in the world to grow up in. That’s why, in 2017, we launched the Baby Box initiative, which is designed to give every single baby in Scotland an equal start in life.
New babies need a surprising amount of stuff! Scotland’s Baby Box is packed full of clothes, bedding and lots of other useful things to help give your baby the best possible start in life
Pathway 2: What are Maternity and Neonatal Psychological Interventions Teams? How can they help me?
INNOVATIONS
Prevention of Neurological Sequelae in Preterm Infants
by Eduardo Gonzalez-Moreira, Thalía Harmony, Manuel Hinojosa-Rodríguez, Cristina Carrillo-Prado,María Elena Juárez-Colín,Claudia Calipso Gutiérrez-Hernández, María Elizabeth Mónica Carlier, Lourdes Cubero-Rego, Susana A. Castro-Chavira, and Thalía Fernández / Published: 2 May 2023
Abstract
Background: Preterm birth is one of the world’s critical health problems, with an incidence of 5% to 18% of living newborns according to various countries. White matter injuries due to preoligodendrocytes deficits cause hypomyelination in children born preterm. Preterm infants also have multiple neurodevelopmental sequelae due to prenatal and perinatal risk factors for brain damage. The purpose of this work was to explore the effects of the brain risk factors and MRI volumes and abnormalities on the posterior motor and cognitive development at 3 years of age. Methods: A total of 166 preterm infants were examined before 4 months and clinical and MRI evaluations were performed. MRI showed abnormal findings in 89% of the infants. Parents of all infants were invited to receive the Katona neurohabilitation treatment. The parents of 128 infants accepted and received Katona’s neurohabilitation treatment. The remaining 38 infants did not receive treatment for a variety of reasons. At the three-year follow-up, Bayley’s II Mental Developmental Index (MDI) and the Psychomotor Developmental Index (PDI) were compared between treated and untreated subjects. Results: The treated children had higher values of both indices than the untreated. Linear regression showed that the antecedents of placenta disorders and sepsis as well as volumes of the corpus callosum and of the left lateral ventricle significantly predicted both MDI and PDI, while Apgar < 7 and volume of the right lateral ventricle predicted the PDI. Conclusions: The results indicate that preterm infants who received Katona’s neurohabilitation procedure exhibited significantly better outcomes at 3 years of age compared to those who did not receive the treatment. The presence of sepsis and the volumes of the corpus callosum and lateral ventricles at 3–4 months were significant predictors of the outcome at 3 years of age.
New Gene Therapy Trial Shows Restored Hearing and Speech in Children Born Deaf, Treated in Both Ears
Administering gene therapy in both ears of five children with DFNB9 led to additional benefits compared to previous trial, including sound source localization and hearing in noisy environments.
Ryan Jaslow – Program Director, External Communications – Research, Mass General Brigham- rjaslow@mgb.org
06/05/24
Key Takeaways
A new clinical trial in Shanghai, China, in partnership with Mass Eye and Ear researchers, demonstrated the restoration of hearing in both ears in five children born with autosomal deafness caused by mutations in the OTOF gene.
All children gained ability to determine locations that sounds came from and improved speech perception in noisy environments.
The trial is the first to provide gene therapy for this form of inherited deafness to children in both ears, and the researchers hope to expand this work internationally.
Boston, Mass. — A novel gene therapy designed to target a form of inherited deafness restored hearing function in five children who were treated in both ears. The children also experienced better speech perception and gained the ability to localize and determine the position of sound. The study, the world’s first clinical trial to administer a gene therapy to both ears (bilaterally), demonstrates additional benefits than what were observed in the first phase of this trial, published earlier this year, when children were treated in one ear. The research was led by investigators from Mass Eye and Ear (a member of the Mass General Brigham healthcare system) and Eye & ENT Hospital of Fudan University in Shanghai, and findings were published June 5th in Nature Medicine.
“The results from these studies are astounding,” said study co-senior author Zheng-Yi Chen, DPhil, an associate scientist in the Eaton-Peabody Laboratories at Mass Eye and Ear. “We continue to see the hearing ability of treated children dramatically progress and the new study shows added benefits of the gene therapy when administrated to both ears, including the ability for sound source localization and improvements in speech recognition in noisy environments.”
The researchers noted their team’s goal was always to treat children in both ears to achieve the ability to hear sound in three dimensions, a capability important for communication and common daily tasks such as driving.
“Restoring hearing in both ears of children who are born deaf can maximize the benefits of hearing recovery,” said lead study author Yilai Shu MD, PhD, professor, director of Diagnosis and Treatment Center of Genetic Hearing Loss affiliated with the Eye & ENT Hospital of Fudan University in Shanghai, “These new results show this approach holds great promise and warrant larger international trials.
Over 430 million people around the world are affected by disabling hearing loss, of which congenital deafness constitutes about 26 million of them. Up to 60 percent of childhood deafness is caused by genetic factors. Children with DFNB9 are born with mutations in the OTOF gene that prevent the production of functioning otoferlin protein, which is necessary for the auditory and neural mechanisms underlying hearing.
This new study is the first clinical trial to use bilateral ear gene therapy for treating DFNB9. The new research presents an interim analysis of a single-arm trial of five children with DFNB9 who were observed over either a 13-week or 26-week period at the Eye & ENT Hospital of Fudan University in Shanghai, China. Shu injected functioning copies of the human OTOF transgene carried by adeno-associated virus (AAV) into the inner ears of patients through a specialized, minimally invasive surgery. The first case of bilateral treatment was conducted in July 2023. During follow-up, 36 adverse events were observed, but no dose-limiting toxicity or serious events occurred. All five children showed hearing recovery in both ears, with dramatic improvements in speech perception and sound localization. Two of the children gained an ability to appreciate music, a more complex auditory signal, and were observed dancing to music in videos captured for the study. The trial remains ongoing with participants continuing to be monitored.
In 2022, this research team delivered the first gene therapy in the world for DFNB9 as part of a trial of six patients in China treated in one ear. That trial, which had results published in TheLancet in January 2024, showed five of six children gained improvements in hearing and speech. Shu initially presented the data at the 30th annual congress of European Society of Gene and Cell Therapy (ESGCT) in Brussels, Belgium in October 2023, becoming the first in the world to report clinical data on using gene therapy to restore hearing.
“These results confirm the efficacy of the treatment that we previously reported on and represent a major step in gene therapy for genetic hearing loss,” said Shu. Shu trained under Chen for four years as a postdoctoral fellow at Mass Eye and Ear, with their collaboration continuing for more than a decade since he returned to Shanghai.
“Our study strongly supports treating children with DFNB9 in both ears, and our hope is this trial can expand and this approach can also be looked at for deafness caused by other genes or non-genetic causes,” added Chen, who is also an associate professor of Otolaryngology–Head and Neck Surgery at Harvard Medical School. “Our ultimate goal is to help people regain hearing no matter how their hearing loss was caused.”
Currently, there are no drugs available to treat hereditary deafness, which has made room for novel interventions like gene therapies.
Mass General Brigham’s Gene and Cell Therapy Institute is helping to translate scientific discoveries made by researchers into first-in-human clinical trials. Chen and his colleagues are working with the Institute to develop platforms and vectors with good manufacturing practice standards that would enable his team to more easily test this therapeutic approach with other genes in the future.
The authors note that more work is needed to further study and refine the therapy. The bilateral study requires more consideration compared to the unilateral (one-ear) study as operations in both ears, in the course of one surgery, doubles the surgical time. Furthermore, by injecting double doses of AAVs into the body, the immune response is likely to be stronger and the potential for adverse effects could be greater. Looking ahead, more patients as well as a longer follow-up duration are necessary, and continued analysis of gene therapies and cochlear implants in larger randomized trials will be valuable.
Paper cited: Wang, H et al. “Bilateral gene therapy in children with autosomal recessive
The Neuroimaging Group, at the Department of Paediatrics, in collaboration with Bliss, the charity for babies born premature or sick, has launched a new suite of information resources for parents of neonates, designed to make them feel more confident about being involved in the care of their babies.
While evidence demonstrates that parents can play a positive role in comforting their baby during painful procedures, practice in the UK lags far behind. However new research by the Neuroimaging Group, published in the Lancet Child & Adolescent Health and Pain has brought further proof of the positive impact that being involved in their baby’s care has on parents.
The Parental touch trial (Petal) aimed to assess whether parental touch at a speed of approximately 3 cm/s to optimally activate C-tactile nerve fibres, provides effective pain relief during a heel-prick procedure. While there was no difference in the babies’ brain, behavioural or heart rate response to pain regardless of whether the parent touched their baby before or after the painful procedure, the findings did demonstrate that the majority of parents had positive emotions when involved in their child’s care – such as feeling useful and reassured – and an overall decrease in parental anxiety after their participation.
These new resources, a combination of beautifully curated and informative videos, FAQs and online information content, have been developed in light of the collaboration with parents and healthcare professionals. They are free to access online and set out in detail the many ways that parents can touch and comfort babies of all gestations during painful procedures on the neonatal unit, including skin-to-skin care.
Commenting on the research in an accompanying Lancet Child and Adolescent Health editorial, Ruth Guinsburg, said: ‘This study is an example of excellence in research. The trial was carefully designed with a clear question, strict inclusion and exclusion criteria, a well-designed and reproducible intervention based on biological plausibility, and defined outcomes, with the strength of using an objective rather than a subjective measure of pain. Only with trials like this might we transform faith in scienceand test the efficacy of traditional aspects of parental care in order to incorporate them, or not, in bundles to alleviate the pain in neonates.’
Dr. Rebeccah Slater, Professor of Paediatric Neuroscience and Senior Wellcome Fellow at the Neuroimaging Group, said: ‘Working with parents, babies and healthcare professionals to better understand how we can support premature and sick babies during painful procedures has been a highlight of my career. Developing these resources with Bliss has placed families at the heart of all the research we do, and has directly improved our engagement with families and the quality of our research. We will continue to find new ways to support parents and their babies when painful procedures form an essential component of neonatal care.’
Dr. Roshni Mansfield, a Paediatrics trainee and NIHR Academic Clinical Fellow in the Paediatric Neuroimaging Group said: ‘The Petal trial has highlighted the importance of involving parents in the provision of care and comfort for relieving their child’s pain. Future studies can build upon the insights gained from this trial including the positive parental experiences observed in this study. Prospective research might, for example, exercise a more spontaneous approach to delivering the gentle touch, such as allowing parents to stroke their child at their own pace, for as long as they need to calm and comfort their child, rather than a more mechanical and precise application.’
Dr. Maria Cobo, a postdoctoral researcher who managed the trial, added: ‘Another positive aspect of the study was the high degree of involvement by both fathers (35%) and mothers (65%) in delivering the parental touch to their babies. This contrasts with many studies, where only mothers’ opinions and involvement have been sought.’
Caroline Lee-Davey, Chief Executive of Bliss, said: ‘We are thrilled to have worked alongside the amazing team of researchers at the University of Oxford to further our understanding on the importance of parental involvement in their babies’ neonatal care. We know that babies have the best chance of survival and quality of life when their parents are empowered to be partners in their care but, sadly, we hear all too often that parents are not informed about their babies’ procedures or the role that they can have in comforting their baby. The outcomes of this research have directly shaped a new suite of Bliss information for parents and healthcare professionals which will help to validate what families often instinctively know to be true – that no matter how unexpected or strange the neonatal environment can feel, they are still their baby’s parent and they have a vital role to play in their comfort and care.’
Additional funding from the Wellcome Trust enabled Bliss to develop these valuable resources for families, including new information, video content filmed at John Radcliffe Hospital’s neonatal unit giving precious insight into neonatal care, as well as translated flyers for neonatal units and a webinar for healthcare professionals on how to support parents to be involved in their babies’ procedures. These resources were created in collaboration with parents and healthcare professionals, and included a listening event with the Raham Project, a CIC supporting ethnic minority families, where four mothers shared their neonatal stories.
Empowering the Unsung Heroes: Siblings of NICU Warriors
When a baby is born prematurely or with critical health needs, the entire family is thrust into a world of uncertainty and emotional upheaval. While much attention is rightfully focused on the newborn and parents, siblings often navigate this journey with a unique blend of resilience and vulnerability. These brave siblings of preemie babies deserve recognition and support for the vital role they play in the family’s NICU journey.
Siblings of NICU babies often experience a whirlwind of emotions, from fear and confusion to jealousy and isolation. It’s essential to create an environment where their feelings are acknowledged, and their contributions celebrated. Simple actions, like involving them in care routines or creating special sibling-only times, can foster a sense of inclusion and importance. Encouraging open conversations about their fears and questions can also help them feel more connected and less isolated.
Educational resources tailored to siblings can also be beneficial. Books, videos, and activities that explain the NICU environment in age-appropriate terms can demystify the experience and reduce anxiety. These resources help siblings understand the medical aspects of their baby brother or sister’s care, making the hospital environment less intimidating. Providing clear and accessible information empowers siblings by giving them a sense of control and understanding in an otherwise overwhelming situation. Resources such as Hand to Hold, Bliss, Miracle Babies Foundation, and Canadian Premature Babies Foundation, offer valuable insights and practical tips for supporting siblings during this challenging time.
Recognizing the importance of supporting siblings of NICU babies is essential for fostering a positive family dynamic and ensuring the emotional health of all children involved. By acknowledging their unique experiences and providing targeted support, parents and caregivers can help these strong siblings navigate the complex emotions and challenges they face, contributing to the overall resilience and well-being of the entire family navigating the NICU journey.
These resources provide valuable insights and practical tips to help siblings navigate the complex emotions and experiences associated with having a brother or sister in the NICU:
Hand to Hold provides comprehensive resources to support siblings of NICU babies, including tips for preparing siblings for NICU visits and strategies for making them feel included in their baby brother or sister’s care.
Bliss is a UK-based charity that provides comprehensive support for families of premature and sick babies. They offer resources and guidance specifically designed for siblings, including advice on how to involve them in the care process and ways to help them understand and cope with the NICU environment.
Miracle Babies Foundation (Australia): Sibling Support
Miracle Babies Foundation is an Australian organization dedicated to supporting premature and sick newborns, their families, and the hospitals that care for them. They provide resources tailored for siblings, helping them navigate the emotional and practical challenges of having a brother or sister in the NICU.
Canadian Premature Babies Foundation Sibling Support
The Canadian Premature Babies Foundation (CPBF) offers a range of resources to support families of premature babies across Canada. They provide specific guidance and materials for siblings, including educational resources and support groups to help them cope with their sibling’s NICU stay.
Boy’s Heart Melts As He Meets Baby Sister After NICU Stay
Sep 11, 2023
A three-year-old boy who could not meet “his” baby sister while she spent her first days in the NICU lit up when he was finally able to hold her for the first time. Dominic “Dommy” Voso, from Rome, Georgia, told his parents the newborn would be “his” baby, having asked mom and dad for a sibling for a long time, proudly telling others when his mom was pregnant. But unfortunately for Dommy, mom Chrissy, 30, had preeclampsia during her pregnancy, which meant that Mia had be delivered at 35 weeks and four days. Mia then had trouble breathing, which caused her to spend her first 12 days in the NICU. This period was extremely tough for Dommy, as he had been desperate to meet his newborn sister, but only adults and siblings over 13 years of age could enter the NICU. Added to this difficulty, Chrissy had to spend an extra eight days in hospital, too, so Dommy couldn’t understand why he could see his mom but not his little sister. But that all changed on July 4 when Dommy sat in his family’s home and Chrissy came in holding Mia. When Dommy was then presented with his little sister, he immediately beamed with joy, holding her before bringing toys and books to share with her.
This inspiring video highlights the experiences and resilience of siblings of Preemie Warriors:
Since 2011, Yemen has been facing a political crisis, marked by street protests against poverty, unemployment, corruption, and President Saleh’s plan to amend Yemen’s constitution and eliminate the presidential term limit. Subsequently, the country has been engulfed in a civil war with multiple entities vying for governance, including the government of President Hadi (later the Presidential Leadership Council), the Houthi movement‘s Supreme Political Council, and the separatist Southern Movement’s Southern Transitional Council. This ongoing conflict has led to a severe humanitarian crisis and received widespread criticism for its devastating impact on Yemen’s people.
The ongoing humanitarian crisis and conflict has received widespread criticism for having a dramatic worsening effect on Yemen’s humanitarian situation, that some say has reached the level of a “humanitarian disaster”. Yemen is one of the least developed countries in the world, facing significant obstacles to sustainable development and is one of the poorest countries in the Middle East and North Africa region. The United Nations reported in 2019 that Yemen had the highest number of people in need of humanitarian aid, amounting to about 24 million individuals, which is nearly 75% of its population.
Estimated # of preterm births: UNKNOWN per 100 live births
(Global Average: 10.6)
Source- WHO Yemen – Healthy Newborn Network 6.8% preterm birth rate, 39% of infant mortality
COMMUNITY
Expanding capacity for publication in nursing: Experiences from a writing for publication group
Highlights
Despite expert knowledge and expertise, nurses often do not write for publication.
Barriers to writing for publication are commonly reported by nurses.
A virtual, Writing for Publication Program was convened to overcome these barriers.
The group of clinical and academic nurses successfully published a manuscript.
Recommendations for overcoming writing for publication barriers provided.
Abstract
Nurses have valuable knowledge and expertise to share. Yet, for a variety of reasons, many nurses do not write for publication. Members in one Sigma Theta Tau International chapter requested information about publishing so a writing for publication program (WPP) was convened. Ten nurses from diverse clinical and academic backgrounds participated. The goal of the WPP was to support a small group of nurses to advance knowledge and develop practical skills through the development of a manuscript with mentorship from doctorally-prepared nurses with publishing experience. The anticipated effect was that participants would share what they learned with colleagues or mentor others to publish in the future. Beginning with informational sessions to lay the foundation for writing and publishing, the WPP included biweekly, two-hour online sessions over a seven-month period whereby individual and group writing with embedded peer and WPP leader feedback occurred. WPP participants gained proficiency in searching online databases, synthesizing published literature, and working as a member of a writing team. The group successfully published a manuscript based on a topic of interest. This current article describes the structured support and mentorship provided during the WPP with recommendations for overcoming publication barriers commonly described in the literature.
Background
Barriers to writing for publication are widely reported in nursing literature. Writing barriers are described as situational or personal (Tivis & Meyer, 2018) and internal or external (Oman et al., 2016). Situational and external barriers to writing for publication include a lack of time, family commitments, lack of resources, inadequate access to technology, insufficient organizational support, or a workplace culture that does not value writing and dissemination (Ansryan et al., 2019; Oman et
Forming the group
In August 2021, the annual general membership meeting for one chapter of Sigma Theta Tau International (Sigma) was held. Based on member requests, the educational focus of the general membership meeting, held online via the chapter’s discussion board, was writing for publication. Over the three-day meeting, those with publication experience were encouraged to share insights related to publishing. Members without publication experience reflected on publishing myths and barriers to writing for
Developing the manuscript
The goal of the WPP was to train a small cohort of nurses on how to write a single manuscript on a topic of interest and submit it to a peer-reviewed nursing journal. Wood (2018) and Bourgault (2023) note that some of the earliest decisions should be selecting the topic of the manuscript, identifying the intended audience, and selecting the journal the manuscript should be submitted. Oman et al. (2016) concur that successfully writing a manuscript is enhanced when the topic relates to lived
Reflections from group members
Two months after the second manuscript was accepted for publication, participants were asked to complete an anonymous survey to ascertain perspectives about the WPP. All ten members completed the survey. Resoundingly participants believed the WPP was a ‘well run,’ ‘helpful,’ and a ‘worthwhile’ experience. WPP leaders were ‘well prepared’ and ‘professional and skilled in guiding the process.’
The topics that members were already familiar with before participating in the WPP were writing
Lessoned learned with recommendations
Reflection by WPP leaders yielded several lessons learned with recommendations for overcoming known barriers to writing for publication. Insufficient time is frequently cited as a barrier to writing for publication (Ansryan et al., 2019). The structure of the WPP program was feasible to accomplish personal and collective goals. Two-hour, bimonthly meetings allowed sufficient time to complete the session agenda without burdening participants who may have competing work and family demands.
Conclusion
Writing for publication is an expectation of all nurses because it improves the quality of patient care to achieve optimal outcomes while also advancing the nursing profession. An innovative, virtual WPP successfully guided 10 academic and clinical nurses to publish a manuscript in a respected, peer-reviewed journal (Chargualaf et al., 2023). Participants largely reported feeling more confident in their own ability to publish in the future. Thus, the goal of the WPP was met.
The violence, suffering, and death from the terrorist attack on Israel and the Israel-Hamas War weigh on us all. Pediatricians—who are called to care for children and keep them safe and healthy—have been reaching out to the American Academy of Pediatrics expressing anguish, outrage, and a deep desire to help stop the killing, ease the suffering, and protect all children from harm.
We are shaken and pained by what is happening in Israel and Gaza, and we are also alarmed by the increasing acts of violence and intimidation we’ve been witnessing in this country toward Jews, Muslims, and those with ties to Israel or Palestine. Many pediatricians and the families they care for have experienced such incidents.
As antisemitic and anti-Palestinian hate speech have been surging on social media, acts of hate have also been increasing in the United States and around the world. There has been an unprecedented rise in incidents of antisemitism, Islamophobia, and anti-Palestinian racism in this country according to data from the Anti-Defamation League and the Council on American-Islamic Relations. And reports of violent hate crimes targeting Jews, Muslims, and Arabs have risen steeply across the United States.
As people at home and abroad confront these issues and as world leaders debate how to move forward, one thing is certain: all children affected deserve our unconditional support.
It will always be the mission of the American Academy of Pediatrics (AAP) to advocate for children’s protection, health, and safety, no matter what, no matter where—be it in the United States, Israel, Gaza, the West Bank, Ukraine, South Sudan, Armenia, Syria, Yemen, Myanmar, Ethiopia, Democratic Republic Congo, or other conflict-torn areas that receive less media attention.
As pediatricians, pediatric medical subspecialists, and pediatric surgical specialists, we understand that the profound cost of any war is measured in children’s lives—those lost to violence and those forever changed by it. We know that what happens to these children today and what we do for them will help determine what becomes of this generation tomorrow.
In 2018, the Academy published a policy statement and accompanying technical report, “The Effects of Armed Conflict on Children,” which began with the following statistic: 1 in 10 children are affected by armed conflict. By 2021, 1 in 6—or about 449 million children worldwide—were living in a conflict zone. Africa had the highest overall number of children impacted by conflict (180 million), followed by Asia (152 million), and the Americas (64 million). Today, that figure is tragically even higher.
Our policy details both the acute and long-term effects of armed conflict on child health and well-being and uses a children’s rights-based approach as a framework for the AAP, child health professionals, and national and international partners to respond in the domains of clinical care, systems development, and policy formulation.
Our policy calls on governments to safeguard children and for pediatricians and health organizations to be involved both in preventing and responding to armed conflict. It advocates for integrating core human rights principles set forth in the United Nations Convention on the Rights of the Child (UNCRC) treaty into US policy.
To fulfill these rights, the policy lays out a number of detailed recommendations for mitigating the harms of child conflict both in clinical practice and in social systems serving children. This includes ensuring child health professionals who care for children affected by armed conflict have access to training in trauma-informed care, which involves recognizing and mitigating the harmful effects of these experiences. And it highlights opportunities for public policy advocacy, which include:
Ending the participation of children younger than 18 years of age in armed conflict and ensuring all children are protected from torture and deprivation of liberty, including extended or arbitrary detention;
Upholding the Geneva Conventions with respect to maintaining the sanctity of safe places for children, ensuring medical and educational neutrality, and allowing children fleeing armed conflict to petition for asylum and be screened for evidence of human trafficking;
Ensuring that children are not separated from their families during displacement and resettlement, and in the event of separation, prioritizing family reunification;
Protecting children from landmines, unexploded ordnances, small arms, and light weapons through effective clearing efforts and strict control on their sale, ownership, and safe storage;
Affording children a voice in creating policy and programs that prevent and mitigate harmful effects of armed conflict; and
Providing children affected by armed conflict access to educational opportunities as part of an environment conducive to their reintegration into society.
2023 AAP Board of Directors
2024 AAP Board of Directors
Sandy L. Chung, MD, FAAP
Benjamin D. Hoffman, MD, FAAP
Benjamin D. Hoffman, MD, FAAP
Susan J. Kressly, MD, FAAP
Moira A. Szilagyi, MD, FAAP
Sandy L. Chung, MD, FAAP
Dennis M. Cooley MD, FAAP
Margaret C. Fisher, MD, FAAP
Patricia Flanagan, MD, FAAP
Patricia Flanagan, MD, FAAP
Warren M. Seigel, MD, FAAP
Jeffrey Kaczorowski, MD, FAAP
Margaret C. Fisher, MD, FAAP
Patricia Purcell, MD, MBA, FAAP
Michelle D. Fiscus, MD, FAAP
Jeannette “Lia” Gaggino, MD, FAAP
Jeannette “Lia” Gaggino, MD, FAAP
Dennis M. Cooley, MD, FAAP
Gary W. Floyd, MD, FAAP
Susan Buttross, MD, FAAP
Martha C. Middlemist, MD, FAAP
Greg Blaschke, MD, MPH, FAAP
Yasuko Fukuda, MD, FAAP
Yasuko Fukuda, MD, FAAP
Madeline M. Joseph, MD, FAAP
Madeline M. Joseph, MD, FAAP
Charles G. Macias, MD, FAAP
Angela M. Ellison, MD, MSc, FAAP
Constance S. Houck, MD, FAAP
Kristina W. Rosbe, MD, FAAP
Joelle N. Simpson, MD, FAAP
Joelle N. Simpson, MD, FAAP
In examining the entire policy in light of the Israel-Hamas War, we determined it was missing important elements to emphasize the protection of children during war and the Academy’s opposition to religious persecution of any kind. We voted unanimously to add the following to the policy statement:
Children should never be harmed because of the religious, cultural, and other beliefs and values of the child and/or their family;
Harm to children should never be used as a tool or tactic of war or conflict; and
Children should be protected from the direct effects of armed conflicts and their food, housing, health, and other basic needs safeguarded.
With the magnitude of the suffering and so many children hurting at home and abroad, this is a distressing time to work in pediatrics. The pain of our members is palpable; both the urgent desire to do all we can to protect children in Israel and Gaza and the fear and concern we are experiencing as acts of hate proliferate in the United States. Yet our common mission and the outpouring of support and solidarity among our member pediatricians reminds us there is light in the darkness.
We use our platform as the world’s largest pediatric organization to speak out against violence, hate, antisemitism, Islamophobia, and enmity toward Jews, Muslims, Israelis, and Palestinians and to speak up on behalf of all children suffering in armed conflict. We stand with everyone in the pediatric profession in these times of tragedy as we continue our work of healing, protecting, and caring for the world’s children.
Question How are maternal social determinants of health associated with discussions and decisions surrounding redirection of care for infants born extremely preterm?
Findings In this cohort study of 15 629 infants born extremely preterm, Black mother-infant dyads were significantly less likely to have redirection of care discussions than White mother-infant dyads, and Hispanic mother-infant dyads were significantly less likely to have redirection of care discussions than non-Hispanic mother-infant dyads.
Meaning Research is needed to understand the possible reasons and solutions for differences in redirection of care discussions for critically ill infants by race and ethnicity.
Abstract
Importance Redirection of care refers to withdrawal, withholding, or limiting escalation of treatment. Whether maternal social determinants of health are associated with redirection of care discussions merits understanding.
Objective To examine associations between maternal social determinants of health and redirection of care discussions for infants born extremely preterm.
Design, Setting, and Participants This is a retrospective analysis of a prospective cohort of infants born at less than 29 weeks’ gestation between April 2011 and December 2020 at 19 National Institute of Child Health and Human Development Neonatal Research Network centers in the US. Follow-up occurred between January 2013 and October 2023. Included infants received active treatment at birth and had mothers who identified as Black or White. Race was limited to Black and White based on service disparities between these groups and limited sample size for other races. Maternal social determinant of health exposures were education level (high school nongraduate or graduate), insurance type (public/none or private), race (Black or White), and ethnicity (Hispanic or non-Hispanic).
Main Outcomes and Measures The primary outcome was documented discussion about redirection of infant care. Secondary outcomes included subsequent redirection of care occurrence and, for those born at less than 27 weeks’ gestation, death and neurodevelopmental impairment at 22 to 26 months’ corrected age.
Results Of the 15 629 infants (mean [SD] gestational age, 26 [2] weeks; 7961 [51%] male) from 13 643 mothers, 2324 (15%) had documented redirection of care discussions. In unadjusted comparisons, there was no significant difference in the percentage of infants with redirection of care discussions by race (Black, 1004/6793 [15%]; White, 1320/8836 [15%]) or ethnicity (Hispanic, 291/2105 [14%]; non-Hispanic, 2020/13 408 [15%]). However, after controlling for maternal and neonatal factors, infants whose mothers identified as Black or as Hispanic were less likely to have documented redirection of care discussions than infants whose mothers identified as White (Black vs White adjusted odds ratio [aOR], 0.84; 95% CI, 0.75-0.96) or as non-Hispanic (Hispanic vs non-Hispanic aOR, 0.72; 95% CI, 0.60-0.87). Redirection of care discussion occurrence did not differ by maternal education level or insurance type.
Conclusions and Relevance For infants born extremely preterm, redirection of care discussions occurred less often for Black and Hispanic infants than for White and non-Hispanic infants. It is important to explore the possible reasons underlying these differences.
Premature births, after years of steady decline, rose sharply in the U.S. between 2014 and 2022, according to recently published data from the Centers for Disease Control and Prevention. Experts said the shift might be partly the result of a growing prevalence of health complications among mothers.
“I’m not too surprised that these are the changes we’re seeing,” said Dr. Nahida Chakhtoura, chief of the pregnancy and perinatology department at the Eunice Kennedy Shriver National Institute of Child Health and Human Development. “We know that maternal complications have been on the rise for the same time period.”
Births before 37 weeks of gestation increased by 12 percent, though there were fluctuations during the pandemic years, with slight decreases in 2020 and 2022. Deliveries at or after week 40 declined during the study period. Increases in premature birth rates were similar across races and age groups, but the largest jump was among mothers aged 30 and above.
It is a reversal of promising trends before 2014, when premature births had been steadily declining and full-term deliveries were on the rise. Though the latest report doesn’t delve into the causes, it is “concerning,” Dr. Chakhtoura said, particularly because premature babies generally face increased risks for health complications.
One of the reasons for the rise might be that women are having babies later in life, said Dr. Vanessa Torbenson, an obstetrician and gynecologist at the Mayo Clinic in Minnesota. Older maternal age, she added, presents an increased risk of health complications that may require an early induction. Overall rates of high blood pressure in particular have been on the rise in recent years. According to the C.D.C., almost 16 percent of women who delivered in hospitals had some kind of hypertensive disorder in 2019, and those issues were most common among women 35 and older. Rates of gestational diabetes have also grown, especially among older mothers.
Generally, “the further along you go in pregnancy, the higher the chance of survival” for the baby, said Dr. Dawnette Lewis, director of Northwell Health’s Center for Maternal Health and a maternal fetal medicine specialist. Studies have found that a baby delivered at 23 weeks, for example, has a roughly 55 percent chance of survival, with chances increasing each week after that, Dr. Lewis said. The American College of Obstetricians and Gynecologists recommends inducing labor at or before 37 weeks when medically necessary.
The latest C.D.C. data is “skimming the surface,” Dr. Lewis said. One of the many unanswered questions is why there were few differences in premature birthrates across races, given that research consistently shows that rates of pre-eclampsia and hypertension are disproportionately higher among Black women. Understanding who was induced and why might shed some light on that question, she added.
Despite the concerns around later maternal age, many of the health risks can be managed, Dr. Lewis said. “Anyone who’s considering a pregnancy, regardless of their age, should see a health care practitioner so that they can be evaluated and, in case that they do have any medical conditions, that they can get those under control before attempting a pregnancy.”
There’s no doubt early in the pandemic, healthcare workers were pushed to their limits. Crowded hospitals required doctors and nurses to work long hours caring for patients suffering from an unprecedented and unpredictable COVID-19 virus. The pressure and demands of the situation put a physical and mental strain on those seeing patients.
According to a 2021 survey published in the Journal of General Internal Medicine of more than 500 healthcare workers and first responders, a substantial majority of respondents reported experiencing clinically significant psychiatric symptoms, including:1
anxiety (75%)
depression (74%)
post-traumatic stress disorder (38%)
recent thoughts of suicide or self-harm (15%)
To support healthcare workers’ mental health during the pandemic, many people were inspired to establish organizations. Below are three that sprung up over the past few years and continue to make a difference in the lives of doctors, nurses, and other frontline workers bearing the brunt of caring for the public during the ebb and flow of the pandemic.
Dr. Lorna Breen Heroes Foundation
Lorna Breen, MD, was a seasoned emergency room physician at New York Presbyterian Hospital in Manhattan when the COVID-19 crisis hit. In a period of three weeks, Breen treated COVID patients, contracted COVID herself, and returned to an overwhelming number of critically sick patients. At the peak of COVID, she worked 15 to 18-hour shifts with limited PPE, insufficient supplies, and not enough equipment to care for patients; some of who were dying in the hallways.
When Breen called her sister Jennifer to share that she was overwhelmed and exhausted to the point that she couldn’t get out of her chair, Jennifer and her husband Corey Feist went to Manhattan and took Breen to a mental health hospital, where she stayed for 10 days, receiving the first mental health treatment of her lifetime. A few days into her stay, Breen called her sister to express concern that her career as a physician was ruined because she was receiving mental health treatment.
When Breen returned to work on April 1, 2020, her fear continued, as she worried her colleagues would notice she couldn’t keep up. Breen died by suicide on April 26, 2020.
What Lorna was feeling is felt by doctors and nurses across the country today. The average person can ask for help, but not healthcare workers; in [several] states, they can lose their license for seeking [treatment for mental health]. That’s unacceptable.
According to a 2022 Medscape report, when physicians were asked why they have not sought help for burnout or depression, their top reasons were:2
I can deal with this without help from a professional (49%)
Don’t want to risk disclosure to medical board (43%)
Concerned about it being on my insurance record (32%)
Concerned about my colleagues finding out (22%)
After Breen’s death, the Feists went on the “Today” show to spread awareness about the mental health strain healthcare workers faced during the pandemic. After the show, they received an outpouring of support from the healthcare workforce, thanking them for sharing Breen’s story. One sentiment they heard often was the need for change when it comes to questions on licensure applications and hospital credentialing applications that ask about a person’s prior mental health history.
The responses moved them to establish the Dr. Lorna Breen Heroes Foundation, which aims to reduce burnout of healthcare professionals and safeguard their well-being and job satisfaction by:
Advising the health care industry to implement well-being initiatives
Building awareness of these issues to reduce the stigma; and
Funding research and programs that will reduce health care professional burnout and improve provider well-being.
“While Lorna is our beacon and inspiration, we started the organization because we heard from the healthcare force (hundreds) after she died that something needed to change,” said Feist. “Now, what we have is a huge subsection of our healthcare workforce who has experienced repetitive trauma for two years. For some of them, this has been 9/11 every day for two years, and because of their fear of repercussions to continue working, they are going to suffer in silence.”
On March 18, 2022, the foundation’s work helped pass the Dr. Lorna Breen Health Care Provider Protection Act, which establishes grants and requires other activities to improve mental and behavioral health among healthcare providers.
The more we talk about mental health, the more we normalize it and give others permission to speak. Lorna was the toughest person I knew in the world and she was a seasoned physician in New York. She worked through Ebola in New York and other crises. This wasn’t about being tough.
He added that many solutions to the problem are complex, but that small actions can help.
“[Like] someone being vulnerable and recognizing the need for self-care, and peer support (recognizing a colleague who needs support) that don’t cost money. We need to make it clear that you care for yourself and colleagues just as you would your patients,” he said.
The foundation’s next mission is to raise awareness among medical licensing boards, nursing boards, and hospital systems about the impact of including mental health questions on applications. They hope licensing boards will change questions to reflect current mental health impairment and exclude past ones.
“We are asking all hospitals in this country to simply publish to their workforce that they can get mental health support without repercussions, which can be a life-saving opportunity for all of the healthcare community,” said Feist.
The Emotional PPE Project
In March 2020, Ariel Brown, PhD, neuroscientist, was talking to her neighbor and friend Daniel Saddawi-Konefka, MD, critical care physician and anesthesiologist at Massachusetts General Hospital, when she was moved to help with the COVID crisis.
“Dr. Dan…is responsible for directing [about] 100 anesthesiology residents and was struggling with the best way to support them during the onslaught of COVID,” said Brown. “I wanted to help and so I put out a call on social media to see if any of the therapists in my network wanted to volunteer some of their time to help these folks who were fighting on the frontline of the pandemic.”
The therapists raised their hands in droves to offer free therapy to healthcare workers. When Brown passed on their contact information to the residents, many reached out to therapists for help at a no-cost, no-insurance, streamlined option for healthcare workers to seek mental health care.
Because of the goodwill of the mental health provider community and because of the great need in the healthcare worker community, things grew very quickly. I put together a team, which I led to set up to be able to scale. Two years later, we are a national nonprofit organization that has over 700 volunteer therapists and has served over 2,000 healthcare workers across the nation.
Over the course of the pandemic, she has learned that healthcare workers face significant barriers to getting support for their mental health. The Emotional PPE Project is designed to streamline mental health service by lifting barriers, including:
Financial: Facilitating services at no cost and with no insurance.
Access: A streamlined process to connect with therapists
Stigma: Remaining 100 percent confidential and unaffiliated with any organization that employs healthcare workers
“Overall, we seek to take away every barrier that we can so that the folks experiencing unprecedented stress and trauma can have a streamlined connection with someone that can help,” said Brown.
Healthcare workers, find a therapistinThe Emotional PPE Project directory
Licensed therapists, sign up to volunteer your time
Anyone, supportthe organization by making a tax-deductible donation
Therapy Aid Coalition
As the world started to shut down due to COVID-19 in March of 2020, Jennifer Silacci, LCSW, psychotherapist, felt grateful she could work from home and shelter in place although anxious about the virus.
I wondered, if those of us at home felt so overwhelmed, how were those on the frontlines coping? How were they processing the anxiety around constant exposure to a potentially deadly virus? And what could I do to help them?
She decided to offer free and low-cost therapy sessions to healthcare workers and asked her colleagues if they would join her. Word spread, and before she knew it, thousands of volunteer therapists from across the country joined Silacci.
“Quite honestly, I had no idea how to manage this new, growing network of volunteers, or the thousands of emails pouring into my inbox, so I asked everyone I could think of for help. Childhood friends and even some kids I babysat (now adults) stepped up. A friend connected us with her law firm, and soon we were a fully formed 501(c)(3) public charity,” she said.
Within months of putting out the initial call, Silacci established the Therapy Aid Coalition, now made up of over 3,000 licensed therapists, who offered free and low-cost online therapy to essential workers in the United States.
Because confidentiality is a concern for many healthcare professionals, and many do not want to utilize employee assistance programs (EAPs), health insurance, or support and resources from their hospitals and clinics, Silacci said her service offers them the opportunity to connect with a therapist anonymously. Over the past two years, the program has served thousands of essential workers throughout the country.
“I think the pandemic and the amazing work of so many nonprofits…have shed light on the need for mental health support, destigmatization, and advocacy for mental wellness within the healthcare professions,” she said.
Because the Therapy Aid Coalition continues to receive hundreds of requests monthly, Silacci said, normalizing the fact that healthcare professionals “while perhaps heroic in their actions—are still painfully and beautifully human” needs to become more understood.
“We all have a breaking point. It is my belief that individuals that have been on the frontlines may not even fully realize the impact of their experience just yet. Some are still running on adrenaline. Some are still numb and just trying to make it through another shift,” she said. “I believe we will see a greater need for mental health support among frontline workers in the next year or two, as they finally come up for air, and have the time and space to unthaw, and digest all that has unfolded.”
Those affected also include mental health professionals, Silacci added, and taking care of therapists is also one of her objectives. While the Therapy Aid Coalition currently offers free and low-cost services, it plans to pay therapists via stipends as it accumulates grants.
Those affected also include mental health professionals, Silacci added, and taking care of therapists is also one of her objectives. While the Therapy Aid Coalition currently offers free and low-cost services, it plans to pay therapists via stipends as it accumulates grants.
“We want services to be free to essential workers, but we also believe it is absolutely not fair to ask therapists to continue to offer pro-bono sessions two years into the pandemic,” she said. “[Therapists] are essential workers, and also qualify for free short-term sessions with us!”
The roles of professionals in society are shifting thanks to the development of truly useful and powerful generative artificial intelligence. Every industry will be impacted, but we have already seen that healthcare, with its heavy use of data and technology, will be disrupted more than most.
Generative AI has the potential to revolutionize the way we treat disease, develop new medicines and personalize treatments to fit individual patients. It will also fundamentally change both the day-to-day working lives of doctors, nurses and other clinical health professionals and even the way they are seen by society. As a result, they will find they are more reliant than ever on the human qualities like compassion, communication and the instinct that many who fill these jobs have for providing care.
So here’s my overview of some of the most dramatic and meaningful transformations we can expect to see in the near future, as well as some of the practical and ethical challenges that will have to be overcome.
AI As A Diagnostic Assistant
Generative AI helps with diagnosing conditions by interpreting data and providing clear, in-depth insights into what is known about the patient. It can be used to examine hundreds of X-ray, MRI and CT scans and quickly give a statistical summary of its findings. This will lead to more accurate, data-driven diagnosis of many common or not-so-common conditions.
This communication can then be fine-tuned depending on the role of the healthcare professional who is using it, whether a doctor, nurse, consultant or specialist. Communicating only the insights relevant to them means there will be less noise between the professional and the specific information they need.
The World Economic Forum has also predicted that generative AI will lead to improved outcomes as it becomes able to efficiently extract data from the many disparate and siloed sources that have traditionally existed across healthcare.
It will also increasingly be used to create synthetic data, which is artificially generated to resemble real-world information. This is particularly useful for situations with limited training data, such as with rare conditions and diseases. It can also reduce the security and data protection measures that healthcare professionals must take when working with real patients’ personal data. Synthetic data can also be used to simulate healthcare scenarios like pandemics or the emergence of antibiotic-resistant organisms that could cause a global healthcare crisis.
Automating Routine And Administrative Tasks
It will become increasingly common for medical professionals to use generative AI to automate many of the repetitive and routine administrative tasks they carry out every day. This will free up their time to focus on directly providing care, as well as continuing their training and learning.
From managing and updating patient records to scheduling appointments, healthcare professionals engage in many time-consuming tasks that can be streamlined or even entirely taken over by AI. According to one study, doctors spend half of their working day on tasks involving maintaining electronic health records.
Generative AI can drive more efficient EHR management by intelligently organizing doctors’ notes, test results and medical imaging. It can then provide quick summaries of individual patients, highlighting aspects of their health that are a concern and generating reports for other professionals. Automating many of these tasks is likely to also have the effect of reducing errors that could impact quality of care and patient outcomes.
Generative AI In Drug Discovery
The same capabilities that allow generative AI to create text and writing can also be used to develop new candidate medicines and vaccines for clinical trials. This means that researchers can speed up the lengthy process of shortlisting potential candidates.
Last year, Oxford-based biotech firm Etcembly produced the first immunotherapy drug created with the help of generative AI.
The process promises to speed the transition of potentially lifesaving new treatments from lab to patient, ultimately leading to better patient outcomes. This indicates that just like doctors and nurses, healthcare researchers and scientists will also have powerful generative AI tools to enable them to work more quickly and efficiently.
Ethical Consideration: The Human Touch
Clearly, however, integrating generative AI into healthcare in this way creates a long list of ethical challenges that can’t be ignored. This is because most use cases revolve around the use of personal data. This means that safeguarding against data leaks, losses and breaches is of paramount importance.
It’s also essential that AI algorithms make decisions that are transparent and explainable—this will be crucial for building the public trust essential for these systems’ potential to be realized.
The damage that can be caused by bias in data is also more pronounced than in nearly any other field. Its been shown that generative AI models can amplify bias present in training data. We know that women and people from minority ethnic backgrounds are more frequently diagnosed due to their underrepresentation in medical studies, and this issue could scale as AI becomes more widely used.
Data, models and outcomes must all be continually monitored and updated in order to mitigate these biases, which could otherwise further perpetuate inequalities.
Like many other professionals, those in healthcare will find themselves required to learn the skillset of the AI ethicist. This means developing the capability to evaluate potential use cases in order to determine whether applying AI is likely to cause damage, risk or danger, and ensuring adequate guardrails are in place at all times.
The Future Of Doctors And Healthcare Workers
Doctors, nurses and other clinical healthcare professionals are probably more insulated than many from the risks of being replaced by AI. Their jobs require them to function at an advanced level across many human skills that machines will not replicate any time soon. Intuition and experience all play a role, and that isn’t going to change.
AI does, however, offer the opportunity for these professionals to redefine the way they work and even their role in wider society. Shifting to models of work that allow them to spend more time with patients will also mean more time to continue their ongoing education and develop their own medical expertise.
This is likely to lead to new specializations as the need grows for clinical staff focused on AI-enhanced diagnoses, data-driven medicine and ethical AI, as well as helping patients navigate the range of new AI-assisted treatment options that will become available.
With AI handling routine analysis, record keeping and interpretation of scans, imaging and other data, doctors and nurses will spend more time getting to the bottom of more complex and nuanced patient issues.
Ultimately, the essence of providing healthcare will continue to revolve around empathy, compassion and the human touch. Generative AI creates the opportunity to augment these qualities in ways that will make professionals in this field even more essential to society. Those who are able to embrace this paradigm shift will find they are able to use their skills and training to cure sickness and improve patient lives in ever more rewarding ways.
Neonatal Neurocritical Care: Past, Present and Future – Fernando Gonzalez, MD (11/13/2023)
Dec 15, 2023
Title: Neonatal Neurocritical Care: Past, Present and Future Speaker: Fernando Gonzalez, MD Co-Director, UCSF Neuro-Intensive Care Nursery Director, Residency Molecular Medicine Track Co-Leader, SPR Pediatrician-Scientist Development Professor of Pediatrics, University of California, San Francisco Presented by leading researchers from UCSF Pediatrics, from other departments at UCSF and outside institutions, Frontiers in Child Health Research is an interactive series meant to facilitate scientific exchange and stimulate new ideas.
Skin-to-skin transfer from the delivery room to the neonatal unit for neonates of 1,500g or above: a feasibility and safety study
Front. Pediatr., 20 March 2024 Meline M’Rini* Loïc De Doncker Emilie HuetCéline RochezDorottya Kele Neonatal Department, Hôpital Universitaire de Bruxelles, Hôpital Erasme, Université Libre de Bruxelles, Brussels, Belgium
Objective: Immediate skin-to-skin contact (SSC) is already standard care for healthy term newborns, but its use for term or preterm newborns requiring admission to neonatal intensive care unit (NICU) with or without respiratory support is challenging. This study aimed to assess the safety and feasibility of SSC during the transfer of newborn infants, using a new purpose-built mobile shuttle care-station, called “Tandem”.
Material and methods: A monocentric prospective observational study was conducted at the tertiary referral center of the Université libre de Bruxelles in Brussels, Belgium after ethical approval by Hopital Erasme’s Ethics Committee (ClinicalTrials.gov ID: NCT06198478). Infants born with a birth weight above 1,500 g were included. Following initial stabilization, infants were placed in SSC with one of their parents and transferred to the NICU using the Tandem.
Results: Out of 65 infants initially included, 64 (98.5%) were successfully transported via SSC using the Tandem. One transfer was not successful due to last minute parental consent withdrawal. The median (range) duration of continuous skin-to-skin contact after birth was 120 min (10–360). SSC transfers were associated with gradually decreasing heart rate (HR) values, stable oxygen saturation levels (SpO2), and no increase in median fraction of inspired oxygen (FiO2). Heatloss was predominantly observed during initial setup of SSC. There was no significant difference in the occurrence of tachycardia, desaturation or hypothermia between preterm and term neonates. No equipment failures compromising the transfer were recorded.
Conclusion: Skin-to-skin transfer of infants with a birthweight of equal or above 1,500 g using the Tandem shuttle is feasible and associated with stable physiological parameters. This method facilitates early bonding and satisfies parents.
The fasting month of Ramadan: Does intermittent fasting of pregnant women influence the risk for preterm birth?
POSTED ON 18 MARCH 2024
Fasting during Ramadan is a valuable experience for Muslims all over the world. Even though it is not compulsory for pregnant women to participate in fasting, many choose to do so. However, the question arises as to whether abstaining from food and water throughout the day could have an impact on the well-being of the unborn child. To answer this question, fourteen studies from seven countries were reviewed, involving more than 2,800 expectant mothers. The results show that Ramadan fasting influences neonatal weight and other parameters of foetal health. However, most of the effects, including the risk for preterm birth, were found to be non-significant. This indicates that fasting during Ramadan is not harmful for the baby overall, and that the decision to participate in Ramadan fasting should therefore be left to the mother.
Ramadan is a month focusing on prayer, community, and reflection for all Muslims around the world. Central to this is the Ramadan fasting (RF), which is a form of intermittent fasting in which no food or water is consumed from sunrise to sunset. The abstinence from water during the fasting period makes RF more intense compared to other forms of intermittent fasting. While RF is obligatory for healthy Muslims, breastfeeding mothers and pregnant women are exempt from fasting and can decide for themselves whether they feel fit enough to participate or not. The Muslim population makes about ¼ of the world’s population, and accordingly many pregnant women face the question if they can participate in RF without harming the foetus. This concern arises from the fact that an adequate supply of nutrients is important to meet the needs of both mother and foetus, and neonatal weight is a direct indicator of the foetus’ wellbeing.
A total of 14 studies from seven countries examined the topic and the results were analysed in an overall review. The 2,889 participating mothers lived in Turkey, Iran, Lebanon, Pakistan, the UK, the Netherlands, and Saudi Arabia.
Ramadan fasting has a significant influence on birth weight
Several different measurements indicate foetal health and can be used to analyse the effects of RF on the unborn child. One indicator is neonatal weight. The findings varied in the different studies examined, but the overall effect showed a significantly lower birth weight in fasting mothers. The amniotic fluid index (AFI), a standardised indicator of foetal well-being, also showed a significant effect. The combination of dehydration during RF, longer daytimes, and temperatures above 36°C led to a reduction of the AFI in fasting mothers. Further significant correlations were found between RF and foetal femur length and RF and lower biparietal diameter assessing foetal size in fasting mothers.
The results on gestational age at delivery were contradictory but insignificant altogether. When analysing the impact on preterm birth (PTB), only one study showed a slightly increased incidence of PTB when the mother was fasting. The increase was not statistically significant and all other studies that examined PTB reported no association, leading to the redeeming conclusion that RF has no effect on the likelihood of PTB.
Various other measures showed no significant impact of RF on foetal health, including foetal body weight, length, head circumference, and abdominal circumference of the infant. The biophysical profile also did not change for fasting mothers, nor did the foetal movements, breathing movements, tone, amniotic fluid volume or the Apgar Score.
Fasting for expectant mothers is not harmful to neonatal health overall
Although RF affects foetal growth, it is not associated with poorer neonatal health. The negative associations between fasting and foetal well-being were stronger when the mother fasted during the second or third trimester of her pregnancy. Furthermore, all associations between RF and reduced health were predominantly found in lower quality studies, which supports the evidence that fasting is safe for pregnant women. Thereafter, current scientific evidence shows that fasting during Ramadan is not harmful to the foetus and can be practiced by pregnant women. The decision to fast should therefore be made by the pregnant woman herself, in consultation with her doctor, who will take her individual health status into account. The wellbeing of the foetus depends more on the type of food the mother eats during the fast-breaking period of Ramadan.
Trauma in infancy can have a lingering effect throughout life
In adulthood, these children “are more vulnerable to stress-related health outcomes, like diabetes, and mental health issues, addiction and obesity,” one expert says
By Katie C. Reilly – March 20, 2022
Are infants too young to experience and remember painful emotions or traumatic events? A growing body of research suggests no, and researchers believe that if left untreated, trauma experienced in infancy can sometimes result in lifelong health consequences.
Beyond such obvious triggers as war and terrorism, exposure to domestic violence, natural disasters such as a house fire, physical abuse and community violence are examples of experienced events that can be traumatic for infants, experts say.
“It is easy to assume that babies don’t remember trauma because they express their experiences differently,” Tessa Chesher, an clinical assistant professor of psychiatry and behavioral sciences at Oklahoma State University who specializes in infant and early childhood mental health, says in an email. “At [8 to 12] weeks of age, babies have stored enough memories that [the babies] start to anticipate their caregiver’s behavior based on previous behaviors. They start to respond based on the experiences they have had.”
‘Vulnerable to stress-related illnesses’
Evelyn Wotherspoon, a social worker specializing in infant mental health, said that as they reach adulthood “infants and very young children who have had early exposure to trauma and chronic stress … are more vulnerable to stress-related health outcomes, like diabetes, and mental health issues, addiction and obesity. These children are much more vulnerable to all of these stress-related illnesses, and their brain may not develop the way it should.”
Although infants and young children are just developing, experts in infant mental health say they can experience a wide range of feelings that includes negative emotions, sadness or anxiety. A report by the American Academy of Pediatrics found that, by age 16, more than 2 in 3 children had said they had experienced a traumatic event.
According to aReport of the Task Force of the World Association for Infant Mental Health, rates of mental health disorders in infancy (which generally includes birth to age 3) are comparable to that of older children and adolescents. And one small study of 1-year-olds found that 44 percent of those who had witnessed severe violence against their mother by an intimate partner showed symptoms of trauma afterward, such as increased arousal, increased aggression or an interference with normal infant development. Infants and young children (under age 4) can develop post-traumatic stress disorders after events, according to a study in the Journal of the American Academy of Child & Adolescent Psychiatry.
Kathleen Mulrooney, a counselor who is also program director for the Infant and Early Childhood Mental Health Program for Zero to Three, a nonprofit organization dedicated to improving the lives of babies and toddlers, said it’s important to note that not every infant who experiences a trauma will be traumatized. As with adults, it depends on the infant, “because what is traumatic for one person is not for someone else,” Mulrooney says.
In this context, caregivers can be key in buffering small children from the effects of trauma by how they react. “The ability of parents or key caregivers to provide protection, to have a co-regulating role when it comes to the stress response is critical,” Mulrooney said in an email.
If a child has a significant trauma before age 2 but following the trauma “the baby has the powerful protective factors of consistent safety, love and security; there is a decreased likelihood of having mental health problems,” Chesher says in an email. “That doesn’t mean the baby didn’t suffer or that their body doesn’t remember that trauma, it means that there were protective factors around to mitigate the effects of the trauma.”
Regina Sullivan, a developmental behavioral neuroscientist and professor of psychiatry at NYU Grossman School of Medicine, says that while a primary caregiver cannot “buffer a small child from trauma in the environment — it’s called social buffering because the child’s fear response and stress hormone response is reduced — more recently, we have shown that the caregiver is actually blocking neural activity in the amygdala, the brain area responsible for fear.”
“Many brain areas in infants and small children are physically altered and the ability of those brain areas to talk to one another is also modified by trauma,” said Sullivan.
Trauma can be difficult to recognize
Yet trauma in infancy can be difficult to recognize given that infants are not yet verbal and rely on their caregivers to respond to their needs, which means a caregiver would have to be attuned to symptoms and seek help.
“A baby can’t just go up to you and say, ‘Hey this happened yesterday, I’m scared,’ Chesher says. “And so really learning the language of the babies is important and then educating people on how to read that language. And so, if we don’t know the red flags, then we are not identifying trauma and we can have longer term effects on the brain.”
Experts say some red flags of trauma for babies younger than 12 months are: feeding or sleep problems and not being able to be comforted by their caregiver. A toddler (between ages 1 and 3) can express themselves more verbally and physically than a baby. Some red flags of trauma in that age group can involve repeating traumatic events in their play or becoming aggressive, Chesher says.
“One of the issues is how that child expresses trauma might be through disruptive sleep or being a bit fussier,” Sullivan says, “things that occur in normal children for a host of many reasons, which makes it difficult to identify which child is going to respond to the trauma in a way that will be long lasting and damaging.”
If a parent or other caregiver is concerned, based on a child’s behavior and experiences, they should “ask to be referred to an infant and early childhood mental health specialist,” Chesher says.
Experts will look at a variety of factors, with the most critical being the relationship between the baby and their primary caregiver. In addition to observing that interaction, mental health experts may also look at “pregnancy history, birth history, medical history, development history, safety screeners, perinatal depression screener [for both parents], how the infant eats and how the infant sleeps,” Chesher says.
Different interventions
Depending on a child’s age, different interventions are available, including child-parent psychotherapy.
“It is essential that the parents or … their caregivers … are involved in a major way in the treatment because it is really through relationships with caregiving adults that infants thrive and do well,” Zeanah says.
To recover, an infant needs a caregiver in their life who can accurately read their cues and respond in a nurturing, patient manner, Wotherspoon says. “One of the most powerful therapeutic tools that we have is the relationship a child has with a nurturing caregiver and they only need one and it doesn’t have to be perfect. … An infant who gets that fairly early on can recover beautifully from trauma,” Wotherspoon says.
Increasing awareness about infant and early childhood mental health among both parents and medical practitioners is critical, experts say. But it’s also important for parents to understand what trauma is — and is not. A child “getting distressed is different than being traumatized,” Zeanah says.
“It’s important to distinguish from everyday events that might scare the child and are important in the child learning how to regulate their emotions and physiology versus trauma from horrible events such as a tornado or a parent who is repeatedly traumatizing the child unnecessarily through verbal or physical assaults,” Sullivan says.
“We want parents to enjoy this time in their life and not be fearful that they are going to traumatize their child by making them eat vegetables or get vaccinated,” she adds. “Those are normal experiences in life that the child needs to experience as part of [the] current world.”
NIU researcher’s innovation helps lead to device to prevent hearing loss in NICU infants
August 28, 2023
DeKalb, IL – Technology developed by NIU Electrical Engineering Professor Lichuan Liu and designed to prevent hearing loss in the most vulnerable of newborns could soon find its way into hospital neonatal intensive care units, or NICUs
NICUs can be noisy. The care units are louder than most home or office environments and have sound levels that often exceed the maximum levels recommended by the American Academy of Pediatrics. Hearing impairment is diagnosed in 2% to 10% of preterm infants, versus 0.1% of the general pediatric population.
Aiming to put her electrical engineering expertise to use to benefit others, Professor Liu invented an apparatus, system and method to significantly reduce harmful noises while maintaining communication between the newborns and their parents or caregivers.
In 2014, NIU began a partnership with Invictus Medical, a Texas-based medical device company, to commercialize the technology. NIU licensed its related patents to Invictus, while the company has continued to refine the incubator-based active noise control (ANC) device, now known as the Neoasis®.
In July, Invictus announced that the company had received a U.S. Food and Drug Administration (FDA) clearance-for-use declaration for the device.
The control unit front face and home screen on the Invictus Medical Neoasis® incubator-based active noise control (ANC) device. Photo courtesy of Invictus Medical
“With this clearance for use, Invictus has made a huge step towards deploying the Neoasis® ANC device in neonatal intensive care units,” said George Hutchinson, Ph.D., Invictus Medical’s chief executive officer. “It is well documented that a quieter environment has a positive impact, including improved sleep hygiene and weight gain in infants where both are critical for development.
“The NIU team has been a pleasure to work with,” Dr. Hutchinson added. “The Office of Innovation has been a great teammate throughout the entire process.”
The Neoasis® ANC device utilizes a proprietary, innovative active noise control (ANC) system to attenuate noise with canceling sound wave technology. At the same time, it allows a parent’s voice to be directed to the infant, which can also be beneficial for cognitive development. Invictus is currently exploring relationships with strategic partners to get the Neoasis® ANC device into NICUs—now possible with the FDA clearance.
While universities and researchers can realize typically modest financial benefits from technology transfer, the primary intent is to broaden the potential impact of research through the creation of innovative products and services for public benefit, said Karinne Bredberg, director of NIU’s Office of Innovation. The office has guided Liu through the partnership, patent processes and licensing.
“This is a big deal for Dr. Liu and for NIU,” Bredberg said.
“NIU research has produced other patents and licenses, but we believe this is the first NIU-licensed technology to be incorporated into a device that has an FDA clearance-for-use declaration,” Bredberg said.
Mark Hankins, NIU’s assistant director for technology transfer, credited the ingenuity of Professor Liu, as well as a great working relationship with Invictus Medical.
“Dr. Hutchinson in particular was very diligent in trying to move this technology forward and persevered through a number of roadblocks,” Hankins said.
Professor Liu said it was about a decade ago when President Lisa C. Freeman, then serving as NIU’s vice president for Research and Innovation Partnerships, brought Liu together with Invictus Medical. While Liu developed an initial prototype, the company refined the device, making the it more commercially accommodating for NICU environments.
“It’s a little different working with industry, as opposed to academia,” Professor Liu said. “It was a learning curve for me, but Invictus Medial has been very professional and easy to work with.”
NIU Professor Lichuan Liu is now conducting research on an artificial-intelligence algorithm that can detect the meaning behind babies’ cries.
“I think this is fantastic,” Liu said. “I kept working on this project and thought someday there would be payback.
“I have a passion or motivation to work to benefit others,” Liu added. “As a mom, I think this device is really something important. As an engineer, I’m happy to make an impact.”
Liu said her current research includes other ways to use noise cancellation. She is working on a pillow that would cancel out the racket of snoring, and she and NIU Nursing Professor Jie Chen are working on a system for adult intensive care units.
Additionally, Liu is working on an artificial intelligence algorithm that can listen to infant cries and determine whether they are normal or abnormal to potentially indicate a severe or chronic illness. Invictus might incorporate the technology into future versions of its Neoasis® ANC device.
Introduction: In a significant number of NICUs, mothers are unable to provide enough maternal milk to feed their premature babies, so healthcare workers rely on human milk banks. Unfortunately, this service is not available in many countries, such as Peru, where premature infants receive formula. The aim of this study was to determine the effectiveness of multisensory stimulation on mother’s own milk production.
Methods: Participants in this study were postpartum mothers of preterm infants 27–37 weeks gestational age. The participants were assigned to three groups: (1) audiovisual stimulation (SAV) (n = 17), (2) audiovisual and olfactory stimulation (SAVO) (n = 17), and (3) control (n = 16). A questionnaire was used to collect demographic and obstetric data, including a record of mother’s own milk volume.
Results: There was no significant difference between the SAV, SAVO and control groups regarding age, marital status, education level, occupation, number of children, mode of delivery, Apgar and birth weight. On the other hand, a significant difference was observed between the SAV and SAVO groups regarding the amount of milk produced, with higher production between the fourth and seventh day (Tukey p < 0.05). Similarly, milk volume was significantly greater in the SAVO group compared to the SAV and control groups (OR = 1.032, 95% CI = 1.0036–1.062, p < 0.027).
Conclusion: Multisensory stimulation in postpartum mothers of preterm infants caused an increase in the volume of mother’s own milk production. However, more research is needed to explain the findings presented in this study.
Advanced imaging and modeling in neonatal simulation
Jennifer Arnold, Niranjan Vijayakumar, Philip Levy
Abstract
Advances in modeling and imaging have resulted in realistic tools that can be applied to education and training, and even direct patient care. These include point-of-care ultrasound (POCUS), 3-dimensional and digital anatomic modeling, and extended reality. These technologies have been used for the preparation of complex patient care through simulation-based clinical rehearsals, direct patient care such as the creation of patient devices and implants, and for simulation-based education and training for health professionals, patients and families. In this section, we discuss these emerging technologies and describe how they can be utilized to improve patient care.
Introduction
Simulation is a powerful tool for improving education, patient safety, and innovation in any field of medicine.1 In neonatology, the opportunity to create realistic simulations to help prepare clinicians for high risk care of vulnerable patients is paramount.2 As the field of healthcare simulation advances, technologies for simulation are diversifying. With advances in modeling and imaging, broader and more realistic tools for education and training, and even opportunities to improve direct patient care are emerging. These include realistic models for preprocedural planning and clinical rehearsals, and innovative, bespoke patient specific devices and healthcare tools to use in clinical care. Current advances in specific technologies have allowed for this expansion, including point-of-care-ultrasound (POCUS), three dimensional (3D) and digital anatomic modeling, and extended reality technologies that are immersive digital recreations of reality, such as virtual reality (VR), augmented reality (AR), and mixed reality (beyond the scope of this article). In this article we review the types of imaging and modeling technologies available and how they can be applied to improve neonatal patient care and outcomes through healthcare simulation-based education (SbE), clinical rehearsals(SbCR), and more.
Section snippets:
Point-of-care ultrasound (POCUS)
POCUS, which is ultrasound performed and interpreted in real time by bedside clinicians, has been used by adult and pediatric specialties for many decades, with recognition that this technology may enhance quality of care and improve patient outcomes.3 Pediatric anesthesiology and adult emergency medicine were early adopters of POCUS, and pediatric critical care has increasingly utilized POCUS for central line placement and diagnostic imaging.4 POCUS has more recently been utilized in
Applications of imaging and modeling
The types of imaging and modeling described above are emerging tools now available in healthcare that can be applied in three specific ways: preparation for complex patient care through SbCRs, direct application for patient care, and simulation-based education and training.
Patient specific simulation-based clinical rehearsal (SbCR)
Simulation-based Clinical Rehearsal (SbCR) refers to the practice and rehearsal by clinicians to prepare for a patient-specific procedure or complex care process before providing direct patient care. These are typically rehearsed using physical 3DP or virtual models. SbCRs can be patient-specific (utilizing the patient’s exact anatomical data to create a model for rehearsal, such as practicing a specific congenital heart disease [CHD] repair on a 3DAM before operating on the patient) or
Imaging and modeling in direct patient care
While using immersive technologies as a part of the preparation for patient care is exceedingly valuable, there are additional applications as part of healthcare services provided directly to patients. In the next section we describe how 3DP, POCUS, and virtual modeling improve care delivery in neonatology and other fields of medicine.
Imaging and modeling in simulation-based education and training
Imaging, modeling and other emerging technologies are used in the education of healthcare professionals and patients, families, and other home caregivers. 3DAMs have been shown to improve performance and promote competency-based education. The benefits of 3DP in education include on demand reproducibility, the possibility to model different physiologic and pathologic anatomy from an endless dataset of images, and the possibility to share 3D models among different institutions.56 3DP has
Conclusion
In conclusion, imaging and modeling technologies have significantly advanced healthcare, including neonatal care. These technologies have enhanced education and training for all levels and types of learners, enabled better preparation and rehearsal for complex care, augmented diagnosis and applications of personalized treatment plans, and improved patient outcomes. From ultrasound to physical models to sophisticated virtual models, these tools provide invaluable insights into the delicate care.
MRI can be a powerful tool for diagnosing problems in newborns, but transferring infants to the radiology department for scanning creates a number of issues. Aspect Imaging has developed Embrace, a 1-telsa MRI scanner that can be installed in the neonatal intensive care unit (NICU) to enable MRI to be used at the bedside. Aspect Imaging demonstrated the Embrace scanner at the 2023 European Congress of Radiology (ECR) meeting.
Innovation and Comfort in the NICU: Enhancing the Neonatal Experience:
In the fast-paced world of neonatal care, where infants face immense challenges from their earliest moments, a wave of innovation is transforming the NICU into a place of both healing and joy. Amidst the beeping monitors and hushed whispers, new technologies and thoughtful touches are bringing smiles to the faces of families and healthcare professionals alike.
Imagine, for a moment, the introduction of point-of-care MRI machines, compact enough to fit beside a newborn’s crib yet powerful enough to provide detailed images without the need for transport. Picture tiny headphones delicately placed on the ears of our smallest patients, playing gentle melodies to soothe and comfort them during procedures. In these small yet significant advancements, the NICU transcends its clinical setting, becoming a sanctuary of warmth and reassurance.
But the innovation doesn’t end there. Enter virtual reality (VR), once reserved for gaming enthusiasts, now offering parents a momentary escape to tranquil beaches or serene forests, providing a much-needed respite from the sterile surroundings. Meanwhile, specialized mobile apps empower parents to track their baby’s progress, celebrate milestones, and inject a touch of whimsy into their daily routines with photo filters that adorn their infants with superhero capes or astronaut helmets.
This harmonious blend of technology and compassionate care paints a future where laughter and joy are as integral to the NICU experience as medical treatment. It’s a future where parents find solace and moments of levity amidst the uncertainty, and where our smallest patients are given every opportunity not just to survive, but to thrive.
As we embrace these innovations, we usher in a new era of neonatal care—one filled with hope, imagination, and the promise of brighter beginnings for our tiniest heroes and their families.
Mom inspired to become a nurse after son’s diagnosis with heart defects
By Yi-Jin Yu – February 19, 2024
An Indiana mother was inspired to change careers after her second child was diagnosed with congenital heart defects and spent nearly two months in a neonatal intensive care unit.
With February being Heart Month, Calley Burnett is sharing her personal story to raise awareness about congenital heart defects, something she had no idea her son Spencer would have when he was born on July 26, 2016.
Burnett, who previously worked for a family business, is now a NICU nurse at Riley Hospital for Children in Indianapolis, the same hospital where Spencer was sent for further care days after his birth.
Calley Burnett was inspired to become a nurse after her second son, Spencer, was born with congenital heart defects.
Burnett’s positive experience with the Riley nurses and doctors who cared for Spencer left an indelible mark on her and in 2019, the mom of two decided to go back to nursing school and become a registered nurse.
“Spencer was born with congenital heart defects and that led my way into the nursing program after just being bedside for several weeks with Spencer at Riley,” the 39-year-old told “Good Morning America.”
Recent Stories from GMA
Burnett said even though it was a “very scary” time for her while Spencer was in the NICU, she and her family had a team of caring health providers who were dedicated to helping Spencer through his many treatments and hurdles.
Spencer had to spend nearly two months in the neonatal intensive care unit at Riley Hospital for Children in Indiananpolis, Indiana.
Spencer had to be treated for multiple heart defects, including coarctation of the aorta, ventricular septal defect, and patent ductus arteriosus. This meant a part of Spencer’s aorta was narrower than usual, he had an unclosed hole in his aorta and he also had a hole in the wall separating the two ventricles of his heart.
According to Burnett, Spencer needed to have a closed-heart surgery in August 2016 before he was discharged. Nearly a year later, the boy also had an open-heart surgery in July 2017, all to treat the various heart issues he was born with.
“We had just phenomenal nurses there that I still talk to today … Their bedside manner and how they made me feel and the trust that I had and the bond that we had, it just opened my eyes to say, ‘You know what, I think that this is something that I would love to do,'” Burnett explained.
It took Burnett, who had to take prerequisite classes, about two years to complete nursing school. The working mom said although it was “tough,” the sacrifices and the hard work were “very well worth it.”
After graduating, Burnett first took a job at another hospital but she knew she wanted to return to Riley, where the staff meant so much to her and Spencer.
“I knew immediately that I wanted to be with the babies. There’s just something about being at Riley and being with kids and tiny little infants that I just knew that’s where my heart was going to be as soon as I hit nursing school,” Burnett said.
Today, Spencer is an active second grader who plays basketball and soccer.
“He is a very spunky 7-year-old. He’s very athletic. He’s always on the go, always making me laugh. He is just loving life,” his mother told “GMA.”
Burnett says she’s staying on her toes as a NICU nurse at Riley, which she said “feels like home.”
“It’s a phenomenal feeling to be able to help the parents because I feel like I’ve been there. I can tell these moms and dads, ‘Hey, I’ve been where you are and I understand.’ And I just love it,” she said.
For others inspired to take a turn in their own careers or to go into nursing themselves, Burnett said she encourages them to take the leap.
“If that is your passion. I would 100% follow [it]. It’s worth it,” she said. ‘The journey is worth it. It’s tough. But what you get back from it is a hundred times better.”
On this episode of Nighty Nights with Miss Neli, we join our friend Kylo on his journey to grow big and strong so that he can go home with his family from the NICU. Book Description: This book takes readers on a journey with a micro premature baby named Kylo. Born weighing just 1 pound 3 ounces, Kylo may be small but that doesn’t stop him from being super. He’ll have to stay in the NICU (Neonatal Intensive Care Unit), which is way different from mommy’s belly until he’s big and strong enough to go home. But adventure and growth await him during his hospital stay. This story follows Kylo on his journey to grow stronger and bigger. SUPREEMIE KYLO’S JOURNEY THROUGH THE NICU
Forgotten Island – Paragliding on the island of Socotra (in English)
A group of professional test pilots explore the remote and rarely visited Island of Socotra off the coast of Yemen in the heart of the Middle East. Join them as they thermal up to 1000m over the Indian Ocean, battle 40 km/h winds, and fly from the longest caves in the orient. A 37 minute documentary including spectacular aerial footage from one of the few remaining flying secrets left on earth. #NOVAparagliders#NOVAwings#FLYnova#Gleitschirm#paragliding#parapente#parapendio#paragleiter#ForgottenIsland












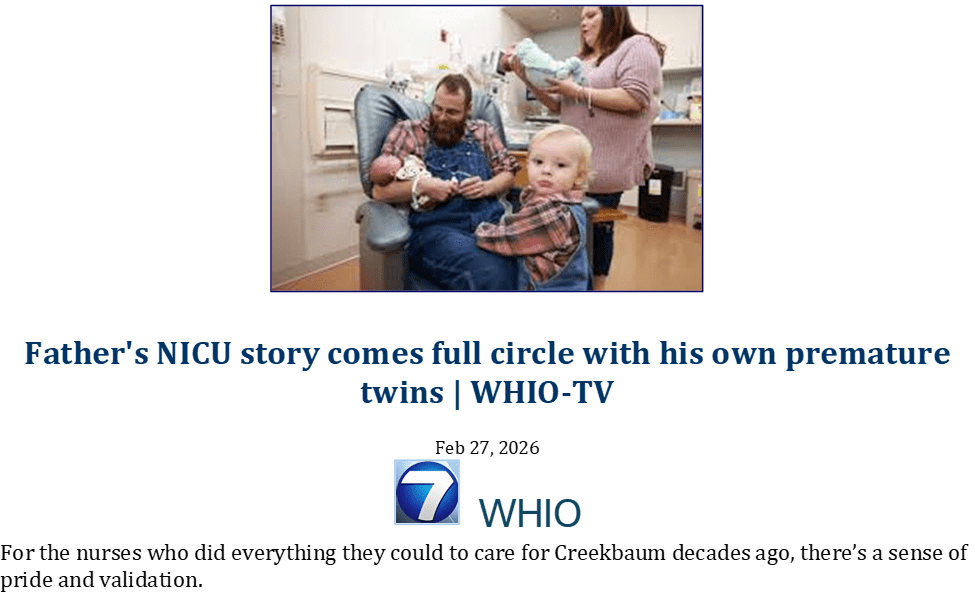



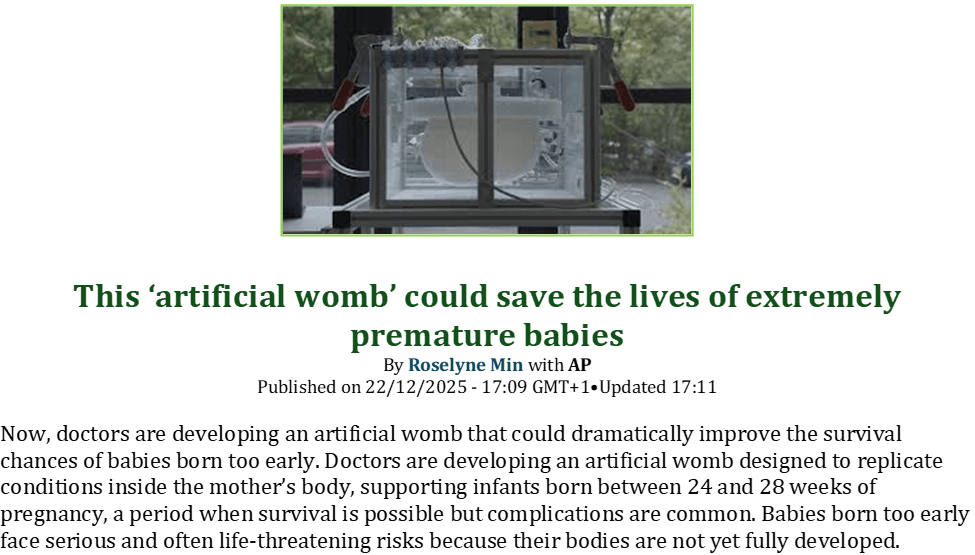
























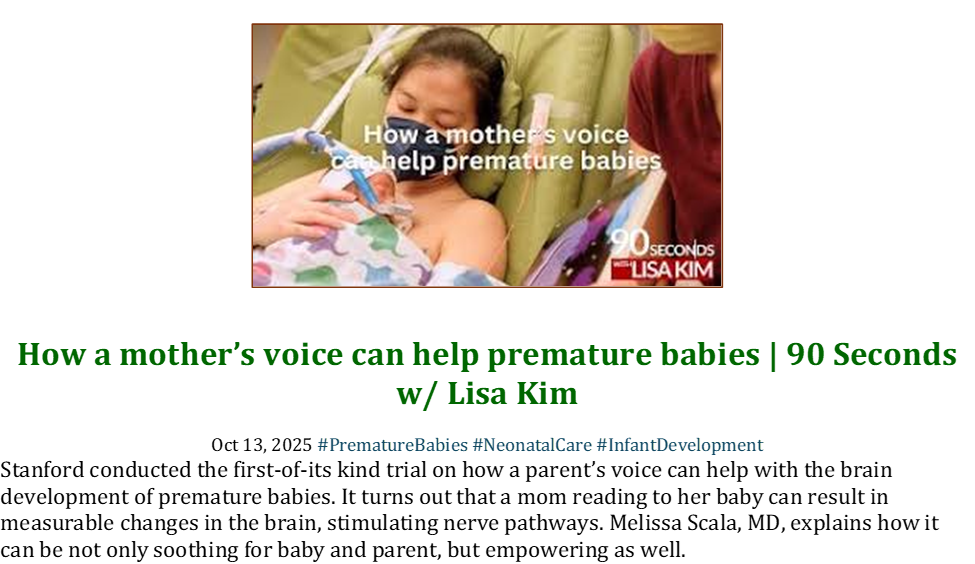





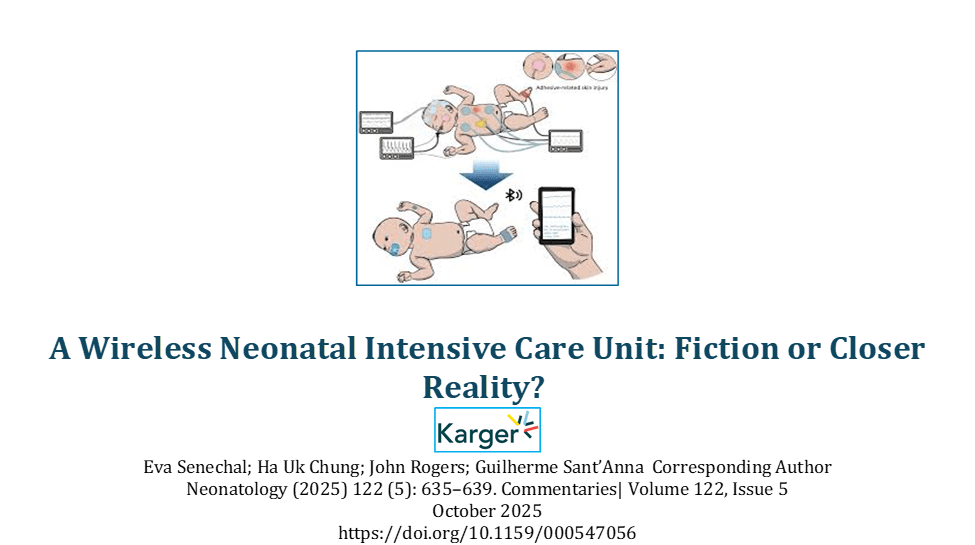










































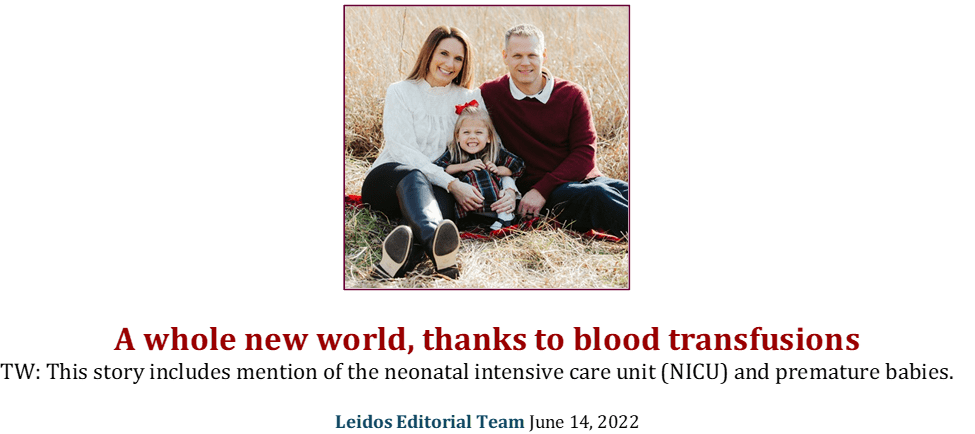

































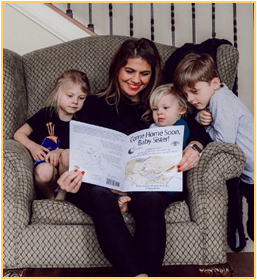

































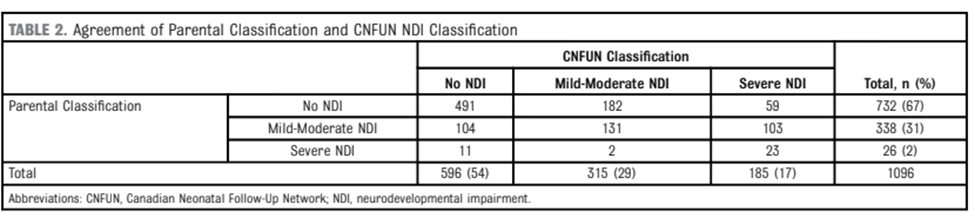




















































































































































{kind=link}