


Lebanon, officially the Republic of Lebanon, is a country in the Levant region of West Asia. Situated at the crossroads of the Mediterranean Basin and the Arabian Peninsula, it is bordered by Syria to the north and east, Israel to the south, and the Mediterranean Sea to the west; Cyprus lies a short distance from the coastline. Lebanon has a population of more than five million and an area of 10,452 square kilometres (4,036 sq mi). Beirut is the country’s capital and largest city.
Lebanon is a parliamentary democracy that includes confessionalism. The National Pact, erected in 1943, laid out a governing arrangement intended to harmonize the interests of the country’s major religious groups. The President has to be a Maronite Christian, the Prime Minister a Sunni Muslim, the Speaker of the Parliament a Shi’a Muslim, the Deputy Prime Minister and the Deputy Speaker of Parliament Eastern Orthodox. This system is intended to deter sectarian conflict and to represent fairly the demographic distribution of the 18 recognized religious groups in government.
Source: https://en.wikipedia.org/wiki/Lebanon
- GLOBAL PRETERM BIRTH RATES – Lebanon
- Estimated # of preterm births: 9.6 per 100 live births
- (Global Average: 10.6)
- Source- WHO Preterm Birth Rate (Per 100 Live Births)


Background
Most of the Infant and Family Centered Developmental Care (IFCDC) Standards focus on evidence-based approaches to care of the baby and family while in intensive care. An ever expanding literature provides rationale for promoting the best care environments for the baby’s developing brain, as well as for parents’ physical and emotional adjustment as they transition to parenthood. As babies may spend days, weeks, and sometimes months during a critical time for brain and behavioral organization, an emphasis has been placed on neuroprotective caregiving strategies and environmental protection to enhance medical, developmental, and psychosocial outcomes.
Both neurodevelopmental and physiological research focus primarily on the age range of babies from birth to discharge, typically ending at 40 weeks post-conceptional age, or when the baby goes home. As babies may be discharged at earlier ages than in previous years—when medically stable, but before many neurodevelopmental tasks have been firmly established (e.g., coordinated eating, sleeping, and regulation)– it is important to extend the focus to the weeks and months after discharge when the baby is still in a developmental fast track.
Babies deemed medically stable enough to transition home need appropriate supports for discharge and preparation for life after hospitalization. A growing literature documents best practices for that preparation, assuring a smooth and uncomplicated transition to community services.
Post-discharge visits to the baby’s pediatrician typically focus on medical stability, as is appropriate. However, most follow-up clinic visits, which include developmental assessment and monitoring, may not occur until the baby is 3-6 months of age. Early intervention services in the United States provide developmental assessment and intervention, if appropriate, for those babies who are “categorically eligible” through Part C of the Individuals with Disabilities Education Act (IDEA). https://www.ed.gov/laws-andpolicy/individuals-disabilities/idea.
Each state determines the qualifications for eligibility, often including diagnoses of established conditions that demonstrate evidence of significant developmental delay (e.g., Down syndrome, chromosomal abnormalities, deafblind conditions, etc.). Often, low birthweight is either not included or restricted to birthweight under 1200 grams, which excludes those babies who have been identified as likely to have lingering developmental deficits (e.g., late preterm babies 34-36 weeks post-conceptual age). Part C assessment and follow-up are mandated to occur within a 45-day timeframe. However, many babies are not identified while they are in the hospital and may not be deemed eligible until obvious developmental concerns surface.
Rationale for assuring continuity of developmental and psychosocial supports from hospital to home.
Support for early brain organization during the neonatal period and throughout the first years of a baby’s life is critical for later development. The literature is replete with evidence regarding neurophysiological and behavioral development, as well as an emphasis on the need for appropriate relationship environments to promote optimal outcomes. Emerging evidence of specific brain development during the first few months of a baby’s life (often referred to as “the fourth trimester”) lends emphasis to the importance of not only understanding the enormity of brain development during this period, but also the potential opportunities for creating appropriate environments and caregiving.
The impact of early birth, medical complexities, and associated hospitalizations on brain development and organization indicates that short and long-term neurophysiologic, behavioral, and mental health outcomes are affected. These and many other outcome studies emphasize the need for early, appropriate environmental and developmental protections, as well as individualized care. Given the recent findings regarding the significant brain development and organization during the first three to six months (in addition to development during the last trimester), it becomes apparent that a significant focus should be on effective interventions both before and after discharge.
Brain and behavior development in parents
Brain changes also occur as parents are transitioning to becoming primary caregivers of their new baby. Emerging evidence of neuroendocrine, neurophysiologic, and behavioral changes during pregnancy, delivery, and postpartum indicates that the experience of becoming parents—for both mothers and fathers — has significant implications for later physical and mental health. Fewer studies indicative of brain changes in parents of early born and medically fragile babies are available; however, there are clear associations with parental mental and physical health challenges.
Punctuated events and recalibration
As babies transition from being fetuses to newborns, there is a significant impact on their brain and behavioral organization. The environment is significantly different, necessitating adaptation from uterine to a maternal caregiving environment. This dramatic change has been referred to as a “punctuated event,” which signifies a significant change in both physiology and behavior, resulting in a period of adaptation and recalibration of behavior.
As previously proposed, a similar punctuated event occurs when the baby transitions from the familiar hospital caregiving environment to the novel home/community environment. (39, 40) It is no wonder that the babies who transition home experience changes in physiology and behavior as a result. Often, medical issues arise, sleep states are disorganized, feeding challenges occur, and previously effective calming strategies seem to be ineffective. If the parent and baby have not had a chance to experience intimate and consistent caregiving in the hospital, which provides the continuity of a trusting relationship, there can be challenges in the process of recalibration.
Parents also experience significant life-changing events to which they must adapt and recalibrate. Pregnancy to delivery and delivery to parenting represent significant punctuated events that may cause other physiologic and/or mental health concerns to emerge. Most parents of term and medically stable babies have had opportunities to adapt to this change cognitively and psychologically. For parents who have a challenging pregnancy, a difficult delivery, and/or a baby at risk for medical challenges, these punctuated events can raise physiological and psychological challenges to which recalibration is complicated.
As with the transition home for babies, the transition home for parents can be disorganizing and difficult. Parents may not only be dealing with their own physical and/or mental health issues as a result of pregnancy, delivery, and hospitalization of their baby, but with the full-time care and adjustment to care in their own home environment. (48-50) Often, the demands of baby care and selfcare are discrepant, resulting in poor sleeping and eating, lack of exercise and social interactions, and other mental health concerns becoming issues that need to be addressed. Unfortunately, these issues may not be addressed quickly and may persist for the first 3-6 months of the family’s life together at home.
Relationship environments are essential for optimal development.
One of the most significant influences on babies’ outcomes is the relationship environment with their primary caregiver. Given the significant neurophysiological and behavioral changes that occur in both newborns and their parents during the first few months after delivery, the development of robust and mutually supportive interactions is fraught with a variety of challenges and successes. These are particularly challenging for parents who come to parenting with significant mental health issues, economic and/or cognitive challenges, few social supports, and/or limited educational backgrounds. Effective interventions have been developed to enhance the parent/baby relationships applied in community settings.
Although effective interventions in communities to promote relationships between parents and their babies have been developed, the application of these programs for parents of medically fragile or early born babies and related research is limited. Having a hospitalized baby presents challenges to early relationship development. A multitude of medical, psychosocial, environmental, cultural, and systems events can challenge early relationship development. Early separation of baby and parent, postpartum medical issues in the postpartum period, family and job responsibilities, grief reactions and fear, poor communication with professionals, as well as restrictive policies and procedures, are but a few of the interfering variables that can affect robust relationship development.
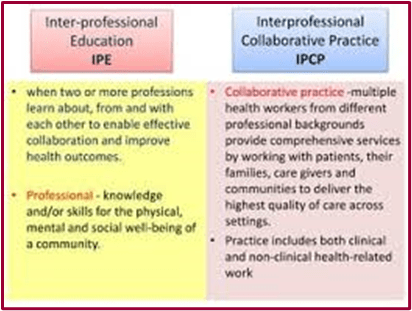
The Infant and Family Centered Developmental Care (IFCDC) Standards address continuity from the hospital to the community.
The IFCDC standards emphasize the importance of collaboration with parents to ensure they are well-prepared to support their baby’s development both in the hospital and after discharge. Each NICU system should engage in collaborative efforts among team members, including parents and caregivers.
The focus should promote and ensure parents’ preparation for transition to community resources, which can be accomplished by providing competent and relevant physical, developmental, and psychosocial services throughout the hospital stay and into the community.
The IFCDC standards also emphasize the need for collaboration with follow-up and community providers who will support their families in the weeks and months after hospitalization.
Conclusion:
Continuity during the transition from intensive care to the family’s home and community presents neurophysiological, psychosocial, and behavioral challenges for both babies and their parents. These occur during a particularly vulnerable time, as the last trimester and the first 3-6 months represent a sensitive period of brain, behavior, and relationship development. Interventions in the hospital should focus not only on neurodevelopmental support and environmental protection but should also emphasize parental involvement in preparation for supporting their baby’s development after discharge. As delineated in the IFCDC standards, it is essential for the intensive care community to not only engage parents as team members and prepare them during hospitalization for post-discharge care, but also to ensure continuity of well-prepared community support and medical follow-up. Currently, the kind of intervention that addresses the specific needs of babies and their parents — early and often, during the first 3-6 months —is not consistently practiced in the United States. There is a need for appropriately trained providers who can sensitively and knowledgably address health, development, relationship, and mental health, development, relationship, and mental health issues for vulnerable families during this vulnerable period.
View additional graphs and info





Since 7 October 2023, 47% of attacks on health care – 65 out of 137 – have proven fatal to at least one health worker or patient in Lebanon, as of 21 November 2024.
This is a higher percentage than in any active conflict today across the globe – with nearly half of all attacks on health causing the death of a health worker.
In comparison, the global average is 13.3%, based on the SSA’s figures from 13 countries or territories that reported attacks in the same period, 7 October 2023–18 November 2024 – among them Ukraine, Sudan and the occupied Palestinian territory (oPt). In the case of oPt, 9.6% of the total number of incidents has resulted in the death of at least one medical professional or patient.
According to the SSA, 226 health workers and patients were killed in Lebanon and 199 injured between 7 October 2023 and 18 November 2024.
In the same period, the SSA registered a combined total of 1401 attacks on health in oPt, Lebanon and Israel – 1196 in oPt, 137 in Lebanon and 68 in Israel.
Civilian health care has special protection
“These figures reveal yet again an extremely worrying pattern. It’s unequivocal – depriving civilians of access to lifesaving care and targeting health providers is a breach of international humanitarian law. The law prohibits the use of health facilities for military purposes – and even if that is the case, stringent conditions to taking action against them apply, including a duty to warn and to wait after warning,” said WHO Representative in Lebanon Dr Abdinasir Abubakar.
International humanitarian law states that health workers and facilities should always be protected in armed conflicts and never attacked. Health facilities must not be used for military purposes, and there should be accountability for the misuse of health facilities.
“There need to be consequences for not abiding by international law, and the principles of precaution, distinction and proportionality should always be adhered to. It’s been said before, indiscriminate attacks on health care are a violation of human rights and international law that cannot become the new normal, not in Gaza, not in Lebanon, nowhere,” said WHO Regional Director for the Eastern Mediterranean Dr Hanan Balkhy.
The majority of incidents in Lebanon impact health workers
The majority (68%) of incidents in Lebanon registered by the SSA impacted health personnel, a pattern seen repeatedly in the last few years, including in Gaza in the past year. In Lebanon, roughly 63% affected health transport and 26% affected health facilities.
Attacks on health care hit twice. First, when health workers lose their lives or when a health centre is obliterated, and again in the following weeks and months when the injured can’t be treated, those who are dependent on regular care don’t receive it and when children can’t be immunized.
“Casualty numbers among health workers of this scope would debilitate any country, not just Lebanon. But what the numbers alone cannot convey is the long-term impact, the treatments for health conditions missed, women and girls prevented from accessing maternal, sexual and reproductive health services, undiagnosed treatable diseases and, ultimately, the lives lost because of the absence of health care. That is the impact that’s hard to quantify,” said Dr Abubakar.
1 in 10 hospitals in Lebanon directly impacted
The greater the blow to the health workforce, the weaker the longer-term ability of a country to recover from a crisis and deliver health care in a post-conflict setting.
Lebanon is a lower middle-income country with a fairly advanced health system that’s been hit hard by multiple crises in recent years. After hostilities in Lebanon escalated in September 2024, the growing number of attacks on health have caused further strain on an already over-burdened system.
Today, the country’s health system is under extreme duress, with 15 out of 153 hospitals having ceased to operate, or only partially functioning. Nabatieh, as an example, one of Lebanon’s 8 governorates, has lost 40% of its hospital bed capacity.
“Attacks on health care of this scale cripple a health system when those whose lives depend on it need it the most. Beyond the loss of life, the death of health workers is a loss of years of investment and a crucial resource to a fragile country going forward,” Dr Balkhy concluded.
So far this year, between 1 January 2024 and 18 November 2024, a total of 1246 attacks on health care were registered globally, in 13 countries or territories, killing 730 health workers and patients and injuring 1255.
Note to editors
The Surveillance System for Attacks on Health Care (SSA), established in 2017 by the World Health Organization, is an independent global monitoring mechanism whose goal is to collect reliable data on attacks on health care and to then identify patterns of violence that inform risk reduction and resilience measures so that health care is protected. The SSA also provides an evidence base for advocacy against attacks on health care.

HEALTHCARE PARTNERS

Skin-to-skin care helps newborn babies in many ways – brain development, regulating heart rate and body temperature, and bonding with their caregivers.
When a baby needs to be in the NICU, skin-to-skin care is especially important, but there can be challenges.
The team at Regional One Health’s Sheldon B. Korones Newborn Center is helping address that through an innovative use of existing equipment that helps facilitate skin-to-skin care.
After a baby is born, skin-to-skin contact is a powerful tool to bond with your baby, improve their brain development, and help them regulate their heart rate and body temperature. But when a baby needs to be in the NICU, skin-to-skin care can be more challenging.
“After a routine delivery, moms are encouraged to have skin-to-skin care right away,” said Ajay Talati, MD, medical director at Regional One Health’s Sheldon B. Korones Newborn Center. “If the baby has to go straight to the NICU for treatment, that can’t happen.”
Challenges can remain once a baby is in the NICU, said Kelley Smith, NICU Nursing Manager. If a baby is on an oscillator, a mechanical ventilation device used to help premature or ill infants breathe, they are connected to tubing that has to stay at the same level as their incubator.
“With an oscillator, the tubing is very stiff – it can’t be bent,” Smith explained. “That makes it hard to move the baby into the parents’ arms for skin-to-skin care.”
The NICU team started looking for a solution and found it in an innovative new use for a piece of equipment that is commonly found in other parts of the hospital.
Cardiac chairs are typically used to help cardiac and stroke patients rest in an optimal position. Because the chairs can go up and down, recline, and even lay flat, Smith and Assistant Nursing Manager Heather Burgess saw an opening to use them in the NICU for skin-to-skin care.
“With this chair, we can have the mom or dad sit in the chair and raise the chair to the level of the oscillator’s tubing,” Smith said. “It makes it easier to get the baby out of the incubator.”
Skin-to-skin care helps babies in a number of ways. “After a routine delivery, moms are encouraged to have skin-to-skin care right away,” said Ajay Talati, MD, medical director at Regional One Health’s Sheldon B. Korones Newborn Center.
A generous Regional One Health Foundation supporter stepped up to donate a cardiac chair to the NICU, and the nursing team is now educating patients about its use and making it available to all families that can benefit. Along with families whose baby is on an oscillator, moms who have had a C-section are finding the chair useful.
“Many moms can’t sit upright for 12 to 24 hours after a C-section, and it can be uncomfortable trying to get in and out of a chair,” Dr. Talati said. “We use it whenever a mom or baby needs it. It’s great for when a baby is too sick to be lowered or when a mom has pain after a C-section.”
Burgess said finding a solution was important to the NICU team because skin-to-skin care has many proven medical benefits for babies and moms.
For the baby, skin-to-skin care helps regulate body temperature, breathing and heart rate and improves brain development, Burgess said. For moms, skin-to-skin can help improve breastmilk production, regulate postpartum hormone balance, and reduce anxiety and stress.
There’s also the matter of bonding, which applies not only to new moms, but to all caregivers.
“We encourage parents to do skin-to-skin care in the first week of their baby’s life, especially for very small, very sick babies,” Smith said. “When you have a baby in the NICU, you’re anxious and afraid, so sometimes parents wait until they go home. That can be a missed opportunity for bonding. The sooner we start skin-to-skin, the better off the family unit will be.”
Dr. Talati, Smith and Burgess have seen the value of skin-to-skin care on multiple occasions.
Moms, dads and other caregivers can all take part in skin-to-skin care. “We encourage parents to do skin-to-skin care in the first week of their baby’s life, especially for very small, very sick babies,” NICU Nursing Manager Kelley Smith said.
The first mom to use the chair had impressive results. “Her baby came off the oscillator the next day!” Smith said. “It’s amazing to see. We’ll have babies on an oscillator with an oxygen saturation in the low 90s…then they do skin-to-skin and it shoots up to 100!”
Burgess said another mom provided skin-to-skin care in the NICU every day, and it contributed to her baby getting healthy enough to go home much sooner than originally expected.
Dr. Talati said there is plenty of evidence behind those individual experiences. Factors like better milk production and better feeding, the ability to regulate body temperature and heart rate, and increased oxygen saturation can all help a baby get stronger.
“It’s a lot of little things that can add up to the baby making faster progress toward going home,” he said. “We hope it can speed that up and we can help more babies go home sooner.”

Have you ever wondered how the Neonatal Resuscitation Program (NRP) guidelines are created—and more importantly, who decides what changes and why? In this episode, we take you behind the scenes of the science and collaboration that shape NRP. From the rigorous evidence review conducted by the International Liaison Committee on Resuscitation (ILCOR) to how these findings are translated into bedside practice, you will learn exactly how research becomes reality.
Together, Dr. Gary Weiner and Amanda Williams break down the multi-layered process of evidence evaluation, guideline development, and educational translation, while highlighting the critical role nurses play in shaping the NRP used daily. Whether you are new to NRP or a seasoned instructor, this episode will inspire you to see the program through a whole new lens and recognize the power of your voice in shaping neonatal care.
Discover why NRP is more than a textbook—it is a living, breathing, global collaboration grounded in science and strengthened by the people who use it.

For the past 10 years, I have worked as a pediatrician and neonatal hospitalist in multiple Level 2 NICUs across Georgia and other states. Over time, I have come to a realization that I cannot ignore: there is a significant public health imperative—and a gap in equitable access—when it comes to developmental and family support services in Level 2 NICUs.
Level 3 and 4 NICUs often have consistent access to lactation consultation, feeding therapy, physical and occupational therapy, and even music therapy. In Level 2 settings, those services are less consistently available—sometimes absent altogether. This discrepancy has a lasting impact on infants and families.
The common perception is that if a baby is born at or after 32 weeks and weighs ≥ 1500 grams—the typical admission criteria for Level 2—that they have “made it.” But research tells a different story. Moderately and late-preterm infants, even those who meet Level 2 thresholds, remain at high risk for readmission, feeding difficulties, developmental delays, and long-term neurodevelopmental challenges (1-4). Prematurity in any form is not a short-term hurdle—it is a lifelong risk factor that requires intentional support from the start.
So, why are we not introducing key developmental concepts, early intervention techniques, and consistent family education into Level 2 NICUs? Why are we not equipping nurses and families with the same foundational knowledge and access to services that higher-level NICUs utilize?
The NICU is not only a place for acute medical stabilization—it is a unique window of opportunity to shape lifelong outcomes. Families in Level 2 units should see themselves as vital participants in their baby’s success and be empowered with the tools to support feeding, bonding, sensory development, and early learning before discharge. Nurses should have access to training that enables them to integrate trauma-informed, developmental care principles into their daily practice, even when an entire therapy team is not available on the unit.
I believe it is time to establish a Task Force on Level 2NICU Care, bringing together neonatologists, neonatal hospitalists, nurses, therapists, public health professionals, and parents, to examine the current state of developmental and family support services in these units, identify barriers, and develop scalable strategies for improvement.
Potential strategies include: • Standardized education for nursing staff on early-intervention techniques, family engagement, and trauma-informed developmental care.
• Telehealth access to lactation consultants, feeding/ occupational/physical therapists, and other specialists when on-site resources are limited.
• Parent-education toolkits that cover feeding, developmental milestones, safe sleep, and the importance of follow-up and early-intervention services.
• Structured discharge planning that includes referrals to early-intervention programs and developmental follow-up clinics for all eligible infants.
The public-health impact of closing these gaps is profound. If we can equip Level 2 NICUs with consistent developmental care education and tools, we can reduce readmissions, improve neurodevelopmental outcomes, and strengthen families’ ability to support their child’s growth and resilience.
The babies in Level 2 NICUs deserve the same intentional approach to developmental care as those in higher-level units. They may have “made it” past the highest-risk thresholds, but they have not yet crossed the finish line. We can—and must—do better.
Now is the time to act. Clinicians, hospital leaders, and policymakers must collaborate to prioritize Level 2 NICUs in state and national maternal-child health agendas. By identifying service gaps, piloting telehealth and staff-training models, and measuring family-centered outcomes, we can transform Level 2 NICUs from sites of short-term stabilization into launchpads for lifelong development, resilience, and equity.
Source: https://neonatologytoday.net/newsletters/nt-oct25.pdf

INNOVATIONS

Introduction: The huge prevalence of neurodevelopmental disorders underscores the necessity for novel, comprehensive prevention strategies for neuroprotective intervention, particularly in preterm infants. The COVID-19 pandemic has accelerated the transformation of healthcare services, emphasizing the use of digital resources. Given the rapid brain development in infants in the first 1,000 days of life and the demonstrated impact of adaptive neuroplasticity, the implementation of early and ecological interventions are essential for supporting optimal neurodevelopment in this vulnerable population. Aim of this project is to develop a digital tool for parent-led parent-based intervention and assess its feasibility and accessibility.
Materials and methods: We collected evidence on early intervention strategies for preterm infants through a non-systematic review of current literature to develop the platform and created an ad-hoc questionnaire to evaluate the tool’s feasibility and acceptability in our neurological follow-up.
Results: “NE@R” is a digital platform designed to support neurodevelopment through parents-delivered play. The platform offers evidence-based information, videos, and practical activities to enhance motor, cognitive, social, and language development at each developmental phase. We introduce the resource in our clinical setting and collect 100 preterm infants’ families feedback. The majority of parents reported finding the resource beneficial, with many expressing increased confidence in supporting their child’s development.
Discussion: Preterm babies families’ support represents a precious field of intervention both for parents and infants at risk. “NE@R” has proven to be an effective, low-cost tool within our follow-up program, aligning with the principles of family-centered care.




Patricia Odero is an innovation facilitator extraordinaire based in Nairobi, Kenya, working for The Duke Global Health Institute. Patricia is trained in Medicine, Business and Social innovation and uses her skills and experience to help entrepreneurs in West Africa and beyond with funding and growth. She talks about the importance of networks, particularly in health entrepreneurship – long-term relationships and support programmes for organisations of different sizes and stages. Patricia has great advice for entrepreneurs and really interesting stories from the field. You can follow Patricia on Twitter @TrishOdero, BMJ Innovations @bmjinnovations and podcast host Helen Surana @hjsurana.
BMJ innovations is grateful to the World Innovation Summit for Health WISH for making this podcast series possible.
Takeaways
- Children born preterm were significantly less likely to complete high school or university compared with full-term peers, according to a large Quebec-based study.
- Non-graduation rates were highest among those born extremely preterm (40.2%) and lowest among full-term births (27.1%).
- Low maternal education, male sex, unmarried parents, and low neighborhood socioeconomic status were major predictors of poorer academic performance.
- The odds of completing high school are reduced among children born preterm vs full-term, according to a recent study published in JAMA Network Open.
Approximately 10% of infants are born preterm, which may cause early exposure to noxious factors and influence brain development, challenging neurodevelopment and mental well-being. Additionally, socioeconomic factors often prevent children from accessing support systems that can mitigate disabilities.
“Few researchers have conducted studies on long-term educational outcomes across the full spectrum of preterm birth using large population-based cohorts that account for other health-related determinants and socioeconomic factors,” wrote investigators.
Assessing preterm birth and education
The birth cohort case-control study was conducted to assess the impacts of preterm birth and sociodemographic factors on educational outcomes. Live preterm births in Quebec, Canada, between January 1, 1976, and December 31, 1995, were included in the analysis.
Each preterm individual was matched with 2 full-term patients, defined as 37- to 42-weeks gestation. Exclusion criteria included multiple pregnancies, triplet births, and death between 1976 and 2019 without Quebec Ministry of Education records.
Extremely preterm birth was defined as under 28 weeks, very preterm as 28 to under 32 weeks, and moderate-to-late preterm as 32 to 37 weeks. Forty-three years of follow-up data was obtained from administrative databases.
High school performance was measured using the final high school average recorded in the Quebec Ministry of Education database, using marks obtained in grades 10 and 11. Covariates included year of birth, birth order, sex, stillbirth history, primary language, matrimonial status at birth, maternal education, and neighborhood socioeconomic status.
Participant characteristics and academic performance
There were 297,820 participants included in the final analysis, 0.6% of whom were born extremely preterm, 4.4% very preterm, 27.9% moderate-to-late preterm, and 67% full-term. Under 11 years of maternal school were reported in 20.6%, 24%, 23%, and 20.3%, respectively.
Preterm birth groups also more often reported primary languages other than French or English, and more recent birth years were reported in those born extremely preterm. Overall, the rate of preterm births in Quebec rose from 4.6% between 1976 and 1980 to 6.1% between 1991 and 1995.
Significant differences were not reported in high school performance based on preterm birth, with final mean scores of 69.4, 70.2, 70.7, and 71 for extremely preterm, very preterm, moderately preterm, and term births, respectively. However, rates of not graduating from high school were 40.2%, 34.4%, 31.1%, and 27.1%, respectively.
This data indicated significantly reduced odds of high school graduation from preterm birth. These patients were also more likely not to graduate from university. Rates included:
- 83.3% for extremely preterm
- 80.2% for very preterm
- 78.2% for moderately preterm
- 75.8% for full-term
Socioeconomic and demographic influences
In regression analyses, a B coefficient range of 0.15 to 1.45 was reported for the link between preterm status and final high school average. Low maternal education, male sex, low neighborhood socioeconomic status, not being first-born, and mother not married had the most significant B coefficients for low average marks of 4.43, 2.84, 2.30, 2.30, and 1.98, respectively.
These results indicated reduced odds of graduating from high school or university among children born preterm vs their full-term counterparts. Investigators concluded long-term follow-up is needed in both health care and education among individuals born preterm.
This data highlights the importance of preterm birth prediction. Identifying individuals at an increased risk of preterm birth may be more accurate through the use of neighborhood-level indices, according to Daniel L. Kuhr, MD, third-year fellow in maternal fetal medicine at the Icahn School of Medicine at Mount Sinai.
According to Kuhr, an increase in prediction was only noticeable when including individual patient characteristics. This highlights a need to evaluate other social determinants of health that may influence preterm birth risk.
“The best thing that you can do is take a really good history when you meet a patient at the beginning of pregnancy, and really make sure you can get accurate gestational ages of delivery when possible, because we do know that history of a prior spontaneous preterm birth is also a risk factor,” said Kuhr.

PREEMIE FAMILY PARTNERS


One of the first things that comes to mind when I think about the holidays is…food. Whether I’m crowded around a dinner table with family and friends or pulling my favorite cranberry and pear pie out of the oven to take to a holiday gathering, there’s something special about breaking bread with the ones you love.
Food, it seems, has a language of its own. In communities across the globe, food has a unique way of bringing people together. And this holiday season, we wanted to help you connect with your friends, family and with the World Relief community by sharing a few recipes from around the world in our new ebook — Breaking Bread Across Borders: Global Recipes from Refugee Kitchens.
https://worldrelief.org/blog-breaking-bread-recipes-around-the-world/DOWNLOAD THE RECIPES!
This ebook is filled with stories and recipes from immigrants who are part of World Relief Western Washington’s Commercial and Teaching Kitchen — an innovative program that connects members of the community with their immigrant neighbors through workshops and events led by immigrant chefs while providing low-cost commercial kitchen space for immigrant caterers to rent and run their businesses.
For women like Katya, who owned a bakery when she lived in Ukraine, the commercial and teaching kitchen is a way to bring people joy while pursuing her passion here in the U.S.
“I love to bring joy to people with my baking,” Katya said. “You become a piece of people’s special events [when you bake for them]. You become a piece of the joy.”
Source: https://worldrelief.org/blog-breaking-bread-recipes-around-the-world/

ABSTRACT
Background:
The formation of the family is interrupted following a Neonatal Intensive Care Unit (NICU) admission, and fathers report experiencing delayed infant bonding due to unit barriers and separation. Fathers state comfort with early infant bonding through language, fearing physical contact with the sick newborn. During hospitalization, active engagement supports ongoing infant/parent vocalization and infant stabilization.
Purpose:
This prospective descriptive pilot study explored the infant’s physiological response to the father’s voice during a live reading activity.
Methods:
After Institutional Review Board approval and consent, 27 infant/father dyads were observed pre/post and during a live reading activity. All infants were in private rooms and positioned supine in open cribs, adjusted to 36 weeks or greater postmenstrual age, in a 34-bed Level III NICU in the Midwest. Outcome measures included cerebral oxygenation, oxygen saturation, heart rate (HR), and respiratory rate. Infants were monitored for 30 minutes prior to father reading, 10 minutes during and 30 minutes post reading.
Results:
A clinically significant increase in cerebral oxygenation was noted, based on near-infrared spectroscopy readings in response to the father’s voice. Most infants had HR stabilization during the father’s active reading time frame.
Implications for Practice and Research:
NICU nurses and staff can encourage a father’s engagement through speaking or reading to their infant. Nursing staff can promote verbal engagement between father–infant dyads by role modeling this behavior at the bedside. NICUs can provide books for families to further encourage exposure to father’s voices. Further study of premature infants at earlier chronological and adjusted ages is needed.
About the Study
Anxiety disorders are defined and classified in diagnostic systems like the Diagnostic and Statistical Manual of Mental Disorders (DSM, currently version IV-TR, American Psychiatric Association) and the International Classification of Diseases (ICDS) (ICD, currently version 10, World Health Organization). Many anxiety disorders have clinical aspects across multiple systems, such as high levels of anxiety, physiological anxiety symptoms, and behavioural problems such as severe avoidance of fearful situations, and related discomfort or impairment. However, there are distinctions, and it’s worth noting that narrowly classified anxiety disorders like panic disorder, agoraphobia, and subtypes of certain phobias have a lot of phenotypic variety or heterogeneity.
From time to time, all children have worries and fears. However, anxiety in children can sometimes cross the line to a disorder that prevents them from normal everyday concerns doing the things they need to do. It may even prevent them from properly understanding life.
How do we determine whether the child’s worries and fears are more than just passing thoughts?
Here are a few questions to ponder:
• Do they express fear or anxiety on a regular basis, for weeks at a time?
• Is it difficult for them to sleep at night? Do they seem abnormally drowsy or exhausted during the day?
• Is it difficult for them to concentrate?
• Do they seem angry or easily irritated?
Anxiety disorders can manifest itself in a variety of ways in children. Some of the most common are:
Generalized Anxiety Disorder (GAD)
GAD children are overly concerned about a variety of things, including school, their own safety and health, the health of family members and friends, money, and the security of their families. The list could go on indefinitely. A child suffering from GAD may constantly imagine the worst-case circumstance. These anxieties may induce physical symptoms in children with GAD, such as headaches and stomach-aches. Because they are so burdened by their fears, your child may isolate themselves, avoiding school and friends.
Panic disorder
A panic attack is a sudden, acute experience of worry that occurs for no particular reason. The child’s heart may race, and he or she may be out of breath. The child may have tremors, dizziness, or numbness. (If the child is hyperventilating, encourage them to breathe gently and deeply.) Breathing through a brown paper bag can be beneficial.) Panic disorder is diagnosed when the child has experienced two or more of these episodes and is preoccupied with fears of them happening again.
Separation Anxiety Disorder (SAD)
Separation anxiety affects all children to some extent. It’s a normal developmental stage for babies and toddlers. Even older children, especially in new situations, may become clingy with their parents or caretakers. Separation anxiety disorder may affect older children who become especially upset when leaving a parent or another close relative, who have difficulty calming down after saying goodbye, or who become highly homesick and disturbed when away from home at school, camp.
Social phobia
In typical, everyday social circumstances, a child with social phobia experiences extreme anxiety and self-consciousness. This isn’t just a case of timidity. When talking with classmates, answering a question in class, or doing other common activities that require interacting with people, the socially anxious child is afraid of embarrassing themselves. This fear may prevent your child from attending school and participating in extracurricular activities. In severe instances, young children may even be unable to speak.
These are the type of anxiety disorders and their assessments on the children, to be considered by the parents, and treat their children accordingly.
Source: https://www.omicsonline.org/open-access/the-assessment-of-anxiety-in-children-and-the-types-of-anxiety-disorders-118047.html


✨ December Kindness for Neonatal Womb Warriors ✨
As December arrives—a month shaped by reflection, generosity, and deeper emotions—the Neonatal Womb Warriors community is reminded that kindness is one of the most powerful tools we have for calming fear and nurturing resilience. Many of us began life in fragile circumstances, where uncertainty, hope, and anxiety coexisted side-by-side. Because of that beginning, we understand how small comforts can soothe big worries. The neonatal world teaches us that healing happens moment by moment, and that gentleness, patience, and compassion are essential for helping families and children navigate anxious seasons.
For families with babies in the NICU, the holidays can intensify feelings of overwhelm, isolation, or emotional strain. Parents may carry silent anxiety about outcomes, siblings may sense stress without understanding it, and clinicians may feel the weight of supporting so many families at once. A simple act—sharing a grounding story of your own journey, sending a message of reassurance, offering a listening ear, or just showing presence without expectation—can ease the mental load for someone facing long days beside an incubator. These gestures remind families that they are not alone in managing the fear that often accompanies the NICU experience.
This month, we invite every Womb Warrior to choose a way—large or small—to give back emotionally or practically. Create a comfort bag for parents spending the holidays in the NICU. Donate time to a local children’s charity, NICU support network, or preemie nonprofit. Offer to read aloud or do a calming activity with siblings who may be feeling anxious. Volunteer at a community event that supports vulnerable families, or simply check in on someone who has been quiet. These actions not only lift others but also model for children that kindness is a powerful antidote to anxiety.
The strength of our community lies in its shared empathy—preemie survivors who have lived through uncertainty, NICU families who have learned courage through adversity, and clinicians who bring dedication and steadiness to every fragile moment. When we turn these lived experiences into acts of compassion, we help others feel grounded, less overwhelmed, and more hopeful. Kindness becomes the bridge between anxiety and reassurance, especially during a season that invites us to slow down and connect.
As we move through December, we encourage each of you to commit to one intentional act of kindness each week. Whether it’s offering comfort to a NICU family, expressing gratitude to a clinician, volunteering in your community, or choosing patience with yourself or your child during moments of stress—every act matters. Together, we carry forward the heart of Neonatal Womb Warriors: grounded in hope, strengthened by compassion, and united in helping families and children navigate anxiety with courage and care.


The whatifs/ A book to help kids overcome anxiety/bedtime story

Fun Story Time Kids Mar 30, 2022
What if my dog run away? what if I forget my homework? what if the sun stops shining? What if my crayon breaks? Will Cora be able to change her worry-filled thoughts into hopeful ones? Find out in this timely picture book about overcoming anxiety.























































































{kind=link}