"Our Mission is to create an active & supportive alliance of Preterm Birth Survivors/NICU Grads & Community Members."
Author: Kathy Papac and Kathryn (Kat) Campos
Kathryn (Kat) Campos: Hello, I am a former 24 week gestation micro-preemie. I lost my twin brother Cruz at birth and encountered open heart surgery with no anesthesia at 3 weeks old weighing 1lb 3oz/0.58kg. I served on the University of Washington Medical Center Advisory Board Neonatal ICU Council from 2013 to 2015. I am passionate about assisting and supporting our Global NICU Community. If your a Preterm Birth/NICU Survivor this blog is dedicated to you, your family, and all members of the NICU Community. Together lets support other Preemie Survivors, Preemies, Preemie families, Preemie Community, Neonatal and related Staff, Providers, Professionals and Facilities. We ALL have stories to share and preemie journeys to help empower!
Kathy Papac: Preemie Mom of surviving (Kathryn) and a deceased (Cruz) 24 week gestation twins. Neonatal Womb journeyer, counselor/legal expert with an MA certificate in Spirituality, Health and Medicine from Bastyr University.
Passionate Global Community participant. Our goal is to recognize, honor and empower the Neonatal Womb community and shine light upon the presence and potentiality of the preterm birth survivors as vital community participants.
Randomly, we choose to take a look at Sri Lanka, knowing so little about this interesting and beautiful country. Our curiosity revealed an exciting connection between Sri Lanka and our home, Seattle, WA, USA!
SriLanka:
Wikipedia: Sri Lanka, officially the Democratic Socialist Republic of Sri Lanka, is an island country in South Asia near south-east India. Sri Lanka’s documented history spans 3,000 years, with evidence of pre-historic human settlements dating back to at least 125,000 years. Its geographic location and deep harbours made it of great strategic importance from the time of the ancient Silk Road through to World War II. Sri Lanka was known from the beginning of British colonial rule until 1972 as Ceylon. Sri Lanka’s recent history has been marred by a thirty-year civil war which decisively ended when the Sri Lankan military defeated the Liberation Tigers of Tamil Eelam in 2009. A diverse and multicultural country, Sri Lanka is home to many religions, ethnic groups, and languages. Sri Lanka is a republic and a unitary state governed by a semi-presidential system. Sri Lanka has a universal health care system that extends free healthcare to all citizens, which has been a national priority.
Sri Lanka Preterm Births – Per WHO/Born Too Soon:
Preterm births in Sri Lanka are 10.7%, and the Sri Lanka is ranked 81 globally in the number of preterm births. “Born too Soon” also reports that Sri Lanka is one of seven low- and middle-income countries that have halvedtheir preterm deaths within a decade (as of 2012). The additional countries include Turkey, Belarus, Croatia, Ecuador, El Salvador, Oman and China.
Our journey to Sri Lanka led us to: INTERGROWTH-21st –
The International Fetal and Newborn Growth Consortium for the 21st Century, or INTERGROWTH-21st, is a global, multidisciplinary network of more than 300 researchers and clinicians from 27 institutions in 18 countries worldwide and coordinated from the University of Oxford. The INTERGROWTH-21st project was a multi-centre, multi-ethnic, population-based project, conducted between 2009 and 2014, in eight demarcated urban areas: Pelotas, Brazil; Shunyi County, Beijing, China; Central Nagpur, India; Turin, Italy; Parklands Suburb, Nairobi, Kenya; Muscat, Oman; Oxford, UK, and Seattle, USA. Its primary aim was to study growth, health, nutrition and neurodevelopment from <14weeks of gestation to 2 years of age, using the same conceptual framework as the WHO Multicentre Growth Reference Study, so as to produce international prescriptive standards for pregnancy dating, maternal weight gain, fetal growth, newborn size, the postnatal growth of preterm infants and cognitive development at 2 years of age. INTERGROWTH -21st developed scientifically robust clinical tools to be used to monitor and evaluate maternal and fetal wellbeing, as well as infant health and nutrition at an individual and population level (birth weight, head circumference, length standards). Through this project INTERGROWTH-21st developed Preterm Size at Birth References and Z Scores (Standard Deviations) and online browser based tools that enable birth weight, length and head circumference to be classified according to these international references. On Feb. 19, 2016 Intergrowth-21st announced the availability of Very Preterm Size of Birth References and Z Scores.
An article dated Dec. 11, 2015 in the Global Health Network (https://tghn.org/) reported:“SriLankabecomes the first country to adopt the INTERGROWTH-21st Preterm Standards”
Webinar:In January 2014, Professors Stephen Kennedy and Jose Villar, Co-Directors of the Oxford Maternal and Perinatal Health Institute, and “chief architects” of the INTERGROWTH-21st Project discussed the objectives, design and emerging findings from the world’s largest collaborative venture in the field of perinatal health research.
Part 2 (Journeys of Grief, Guilt, Guts and Gratitude):-GUILT
Miriam Webster: Simple Definition ofguilt:
:responsibility for a crime or for doing something bad or wrong
:a bad feeling caused by knowing or thinking that you have done something bad or wrong
In the preterm birth community, guilt is often experienced in relationship to “What Ifs” and “If Onlys”, and many Partners within our community experience guilt in some capacity related to the traumas that connect us.
Healthy Children.org published this updated article (11/21/2015) “Common Parent Reactions to the NICU”. The article briefly addresses the range of reactions and emotions parents may experience following their first moments in the NICU, such as Fear, Anger, Loss, Guilt, Powerlessness, and Feeling on Display. Regarding Guilt the article states:
“It took us a long time to resolve our guilt. We asked the ‘what if’ and ‘why us’ questions for months. But we did nothing wrong. We had good prenatal care. What happened to us was nobody’s fault.
Most parents express feelings of guilt after the birth of a sick or premature baby. You may ask yourself, “What did I do to cause this?” or “What could I have done to prevent this?” And nearly every parent unnecessarily laments, “If only I hadn’t….” Mothers, especially, examine their lives since the day they became pregnant—wondering if they could have changed the outcome by making different decisions or if their circumstances had been different.
For most babies in the NICU, the reasons they were born sick or premature are not known. If necessary, let go of guilty feelings, which will give you more energy to care for yourself and your new baby. It is also important to try and share these feelings with the NICU team. Often the NICU team can provide answers and comfort”.
We sometimes lock ourselves into a “closet” of guilt, perhaps to avoid taking action. In reality, however, the door isOPEN!Allow guilt to fade with the setting sun. Welcome in the light of transformation as the sun arises.
Kathy: My experience of guilt was stronger more in relationship to the twin (Cruz) whom I feel (from a spiritual perspective) choose not to remain in this realm, than it was in relationship to the surviving twin (Kat) due to the fact that I have had an opportunity to contribute in a positive way to Kat’s current life journey. As parents we can identify a myriad of issues that we imagine we “may” be guilty of. Guilt itself offers an opportunity to look more intently into an event, our motivations and actions, etc., but beyond expanding our immediate perspective guilt is not a feeling that contributes to the well-being of ourselves or others. I encourage our community partners to choose love, take action, and positively transform our feelings of guilt in order to support our health and well-being, and in doing so the health and well-being of others.
Kat: I feel some guilt that my brother Cruz passed while I was able to survive our birth. I experience some guilt that my family was caught in the trauma of caring for a child that lived while living in the anguish of another’s passing. Some guilt still remains present in my heart when I am in the NICU or hear a story of a fellow preemie that passes or has a challenging outcome. Within myself I question “why did I make the estimated 15% chance of life for babies born at 24 weeks gestation?” Acknowledging my feelings of guilt allows me to take action, and to recognize and seize the opportunity to move the stagnant energy of guilt into a positive energy of healing, love and action. Healing and wholeness are a process…
Meditation is a powerful way to transform the energies of feelings! Abundant, diverse and free guided imagery resources are available on YouTube. We loveThe Honest Guys and recommend this Guided Meditation as a tool for transforming guilt into a positive energy.
GUIDED MEDITATION – OvercomeGuilt ; The Honest Guys – Published on Aug 9, 2016
Some people find it difficult to overcome guilt, to forgive themselves. This can become a difficult load to bear. This meditation will help you to forgive yourself and leave the guilt behind you.
GUTS
1.Google: (informal) personal courage and determination; toughness of character.
We travel, each of us, on a Hero’s Journey through life. As a Neonatal Womb traveler, we have all been challenged to choose love over fear, staying over fleeing, seeing over denial. Perhaps courage is the act of knowing ourselves deeply, accepting and creating space to experience the wholeness of who we are, and living within the integrity of our beingness with presence and compassion towards ourselves and others. We are a community of Heroes.
WARRIORS:
Are you familiar with Bethany Hamilton, the surfer who lost her left arm in a shark attack (2003)? Bethany resumed surfing about one month after the accident, and went on to win a national pro surfing title in 2005. Now, at 26 years of age, Bethany, a wife and mother, is an inspiration to many. This influential surfer is quoted as saying ““Courage doesn’t mean you don’t get afraid. Courage means you don’t let fear stop you” and “I don’t want easy, just possible”. Please enjoy this short video about courage, personal experiences, and choices of a young girl.
Our intent for the next few blogs is to openly address critical emotions that deeply, uniquely yet universally connect and impact partners within the Neonatal Womb community. So often within our community we feel we need to take this journey in silence, often alone with our feelings, even within our family and work family units. Currently, there is an abundance of grief related resources available to preterm birth families within the USA including diverse in-person, telephonic, on-line resource opportunities. We are aware of a clear and concerning lack of resources available to support our healthcare brothers and sisters through their experiences of grief and related emotions. Warriors, understanding grief will empower our capacity to fully experience and acknowledge our own emotional being as we journey forward, while empowering our capacities for empathy, kindness, joy, health and strength.
Part 1 – Grief
Dictionary.com: Definition of grief: noun
keen mental suffering or distress over affliction or loss; sharp sorrow; painful regret.
a cause or occasion of keen distress or sorrow.
Kathy: The anguish and grief experienced by the mother represented in the video below is not unlike the anguish and grief I experienced with the death of Kat’s twin brother, my son Cruz
NATURE | Unforgettable Elephants | A Mother’s Anguish | PBS
Kat: I grieve for the loss of my brother Cruz on this earthly plane, and cherish my connection with him in our spiritual togetherness. As an adult, I have become increasingly present with my feelings of grief, and with the emotional pain and sorrow of those who enter into the preterm birth experience.
A child’s death arouses an overwhelming sense of injustice for lost potential, unfulfilled dreams and senseless suffering. Parents may feel responsible for the child’s death, no matter how irrational that may seem. Parents may also feel that they have lost a vital part of their own identity.
Living with Grief:
Coping with death is vital to your mental health. It is only natural to experience grief when a loved one dies. The best thing you can do is allow yourself to grieve. There are many ways to cope effectively with your pain.
Seek out caring people. Find relatives and friends who can understand your feelings of loss. Join support groups with others who are experiencing similar losses.
Express your feelings. Tell others how you are feeling; it will help you to work through the grieving process.
Take care of your health. Maintain regular contact with your family physician and be sure to eat well and get plenty of rest. Be aware of the danger of developing a dependence on medication or alcohol to deal with your grief.
Accept that life is for the living. It takes effort to begin to live again in the present and not dwell on the past.
Postpone major life changes. Try to hold off on making any major changes, such as moving, remarrying, changing jobs or having another child. You should give yourself time to adjust to your loss.
Be patient.It can take months or even years to absorb a major loss and accept your changed life.
Seek outside help when necessary. If your grief seems like it is too much to bear, seek professional assistance to help work through your grief. It’s a sign of strength, not weakness, to seek help.
Helping OthersGrieve:
If someone you care about has lost a loved one, you can help them through the grieving process.
Share the sorrow. Allow them – even encourage them — to talk about their feelings of loss and share memories of the deceased.
Don’t offer false comfort. It doesn’t help the grieving person when you say “it was for the best” or “you’ll get over it in time.” Instead, offer a simple expression of sorrow and take time to listen.
Offer practical help. Baby-sitting, cooking and running errands are all ways to help someone who is in the midst of grieving.
Be patient.Remember that it can take a long time to recover from a major loss. Make yourself available to talk.
Encourage professional help when necessary. Don’t hesitate to recommend professional help when you feel someone is experiencing too much pain to cope alone.
Helping Children Grieve:
Children who experience a major loss may grieve differently than adults. A parent’s death can be particularly difficult for small children, affecting their sense of security or survival. Often, they are confused about the changes they see taking place around them, particularly if well-meaning adults try to protect them from the truth or from their surviving parent’s display of grief.
Limited understanding and an inability to express feelings puts very young children at a special disadvantage. Young children may revert to earlier behaviors (such as bed-wetting), ask questions about the deceased that seem insensitive, invent games about dying or pretend that the death never happened.
Coping with a child’s grief puts added strain on a bereaved parent. However, angry outbursts or criticism only deepen a child’s anxiety and delays recovery. Instead, talk honestly with children, in terms they can understand. Take extra time to talk with them about death and the person who has died. Help them work through their feelings and remember that they are looking to adults for suitable behavior.
Kathy:I regret not helping Kathryn and Cruz’s siblings with their grief processes. Overwhelmed with my own anguish, caring for Kat, working full time, I was profoundly engaged in a moment by moment effort to just make it through. I have since apologized, and want to thank my oldest child Jesse for stepping in to help me care for his brother and sisters.
Death of a child:
The Luminous Light Beach Ceremony Carly Marie Dudley –Published on Dec 20, 2013
“It is with the greatest joy on this Saturday morning that I share with you all the film clip from our Luminous Light Beach Ceremony that we held back in November, to honour all of the babies and children that are no longer with us. We had 180 people come to share in this very beautiful sunset with us. As we tied ribbons to the peace branch we spoke messages of love to our children and the breeze took those messages out into the universe. Each person was invited to write their child’s name on a seashell at the beginning of the ceremony. During the ceremony we called out the names of over 300 babies and children. As those names were called we invited the parents to come forward to place their seashell in the sand next to the flame of remembrance. Next to the flame was a package of letters sent to me from last year’s prayer flag project and a list of names with messages of love from over 4000 families from all over the world. Once the family members and friends had placed their seashells in the sand, they were offered a handful of flower petals to take down to the ocean to give to the waves in an act of peace and remembrance. After the sun had set, that is when we began the bubble release. It was the most beautiful scene. Adults, teenagers, children and babies all surrounded by thousands and thousands of bubbles. Finally we gave out sparklers and glow sticks and the evening came to a close under the full moon and stars with families sharing their hearts on the beach with strangers. We covered the seashells with beach sand so that a part of our babies and children would remain at the beach together forever more. This was an evening that will be held in my heart and soul forever. I cannot thank everyone who came enough for without them, it would not have been possible. Please, when you have a spare 8 minutes, take some time out of your day and be a part of that beautiful evening.– With love, Carly Marie”
HEALTHCARE PROVIDERS
Our comprehensive efforts to identify and explore grief support for healthcare providers remains a frustrating and concerning endeavor. Our interviews with medical providers reinforce our understanding that a large portion of our Neonatal Womb Community does not have humane access to grief support resources. It seems to us to a large extent that grief in the healthcare, and especially in the physician and medical student communities, is denied, dismissed, buried, and our souls are broken. The Industry promotes, acknowledges the positive impact, and encourages provider “presence” with the patient population, but discounts the critical needs of the providers to be supported in being present with the wholeness of their own being. It is not possible to be fully present for someone else if one is not able to be present within their own being.
Nurses:We were able to identify several sources to support the grief process within the vibrant community of nursing professionals where the sharing of emotions such of grief are often encouraged and healing is supported. Nurses often mentor students in ways to seek grief support, acknowledge feelings, and function professionally within the healthcare environment.
“How Nurses Can Grieve the Loss of a Loved One or Special Patient”-by TAMMY RUGGLES, BSW, MA.-
(10 ideas for touching the void: Below we summarize this helpful article):
Listen to music. * Kat and I are both certified Zumba instructors, and we love Latin music. Neither of us speaks fluent Spanish (Kat speaks pretty good Portuguese). We acknowledge the healing capacity of music and how in some ways not understanding the lyrics of the songs frees us to connect fully with the emotion of the music and that connection allows us to acknowledge and say hello to the energies of our own feelings and senses. ”Words” are not required.
Be alone with yourself
Get out the photo albums
Do something in honor of your lost loved one.
Clear out the mementos, not the memories.
Visit a support group in person or online.
Help others through their grief.
Clear out the mementos, not the memories.
Visit a support group in person or online.
Help others through their grief.
The New York Times – “When Doctors Grieve”
By LEEAT GRANEK – MAY 25, 2012 (Leeat Granek is a health psychologist and a postdoctoral fellow at the Hospital for Sick Children in Toronto.)
In this article Leeat Granek reports “Our study took place from 2010 to 2011 in three Canadian hospitals. We recruited and interviewed 20 oncologists who varied in age, sex and ethnicity and had a wide range of experience in the field — from a year and a half in practice in the case of oncology fellows to more than 30 years in the case of senior oncologists. Using a qualitative empirical method known as grounded theory, we analyzed the data by systematically coding each interview transcript line by line for themes and then comparing the findings from each interview across all interviews to see which themes stood out most robustly”.
Psychologist Granlek stated “Our study indicated that grief in the medical context is considered shameful and unprofessional. Even though participants wrestled with feelings of grief, they hid them from others because showing emotion was considered a sign of weakness. In fact, many remarked that our interview was the first time they had been asked these questions or spoken about these emotions at all”.
Unacknowledged grief was described as “exactly what we don’t want our doctors to experience: inattentiveness, impatience, irritability, emotional exhaustion and burnout”.
In Summary the article proposes “To improve the quality of end-of-life care for patients and their families, we also need to improve the quality of life of their physicians, by making space for them to grieve like everyone else”.
A Poem – El Curandero –Rafael Campo
I am bathing. All my greyness— The hospital, the incurable illnesses, This headache—is slowly given over To bathwater, deepening it to where
I lose sight of my limbs. The fragrance, Twenty different herbs at first (dill, spices From the Caribbean, aloe vera) Settles, and becomes the single, warm air
Of my sweat, of the warmth deep in my hair— I recognize it, it’s the smell of my pillow And of my sheets, the closest things to me. Now one with the bathroom, every oily tile
A different picture of me, every square One in which I’m given the power of curves, Distorted, captured in some less shallow Dimension—now I can pray. I can cry, and he’ll
Come. He is my shoulder, maybe, above The grey water. He is in the steam, So he can touch my face. Rafael, He says, I am your saint. So I paint
For him the story of the day: the wife Whose husband beat purples into her skin, The jaundiced man (who calls me Ralph, still, Because that’s more American), faint
Yellows, his eyes especially—then, Still crying, the bright red a collision Brought out its perfect vessel, this girl, This life attached to, working, the wrong thing
Of a tricycle. I saw pain— Primitive, I could see it, through her split Chest, in her crushed ribs—white-hot. Now, I can stop. He has listened, he is silent.
When he finally speaks, touching my face, It sounds herbal, or African, like drums Or the pure, tiny bells her child’s cries Must have been made of. Then, somehow,
I’m carried to my bed, the pillow, the sheets Fragrant, infinite, cool, and I recognize His voice. In the end, just as sleep takes The world away, I know it is my own.
~~~~~~~~~~~~~~~~~~~~
Grief is only one aspect of Physician and Medical Student Suicide, but it may be a critical one. Although the article below is relatively long, it is very pertinent to the Neonatal Womb Community. Excellent medical care is critical to the health of the preterm birth community at large. Given the shortage of healthcare providers nationally and globally, the fact that the preterm birth community is large and preterm birth infant survival rates are increasing we need to support health and well-being of our healthcare partners. The comprehensive, thought provoking, and current Physician Suicide article below is one of numerous writings we reviewed that addressed the increasing necessity to provide appropriate, effective, accessible and safe/accepted support to the Global and National Healthcare Community at large, and to our Neonatal Womb partners Worldwide.
Physician Suicide
-July 28, 2016 Author: Louise B Andrew, MD, JD; Chief Editor: Barry E Brenner, MD, PhD, FACEP
It has been known for more than 150 years that physicians have an increased propensity to die by suicide. It was estimated in 1977 that on average the United States loses the equivalent of at least one small medical school or a large medical school class to suicide.[1] Exact numbers are not known. Although it is impossible to estimate with accuracy because of inaccurate cause of death reporting and coding, the number most often used is approximately 3-400 physicians/year, or perhaps a doctor a day. Of all occupations and professions, the medical profession consistently hovers near the top of occupations with the highest risk of death by suicide.
Sadly, although physicians globally have a lower mortality risk from cancer and heart disease relative to the general population (presumably related to knowledge of self-care and access to early diagnosis), they have a significantly higher risk of dying from suicide, the end stage of an eminently treatable disease process. Perhaps even more alarming is that, after accidents, suicide is the most common cause of death among medical students.
In every population, suicide is almost invariably the result of untreated or inadequately treated depression or other mental illness that may or may not include substance or alcohol abuse, coupled with knowledge of and access to lethal means.[2]Depression is at least as common in the medical profession as in the general population, affecting an estimated 12% of males and up to 19.5% of females.[3, 4]Depression is even more common in medical students and residents, with 15-30% of them screening positive for depressive symptoms.[5, 6, 7, 8, 9] This is not an isolated North American phenomenon. Studies from Finland, Norway, Australia, Singapore, China, Taiwan, Sri Lanka, and others have shown increased prevalence of anxiety, depression, and suicidality among students and practitioners of medicine.[10, 11, 12, 13]
However, because of the stigma associated with depression in almost all cultures, which seems to be greatly magnified among medical practitioners, self-reporting likely underestimates the prevalence of the disease in medical populations. Indeed, although physicians seem to have generally heeded their own advice about avoiding smoking and other common risk factors for early mortality, they are decidedly reluctant to address depression, a significant cause of morbidity and mortality that disproportionately affects them. Depression is also a leading risk factor for myocardial infarction in male physicians, and it may play a role in immune suppression thus increasing the risk of many infectious diseases and cancer.[14, 15, 16, 17, 18, 19, 20, 21]
Because of their greater knowledge of and better access to lethal means, physicians have a far higher suicide completion rate than the general public. The most reliable estimates of successful completion of suicide range from 1.4-2.3 times the rate achieved in the general population. Although female physicians attempt suicide far less often than their counterparts in the general population, their completion rate equals that of male physicians and, thus, far exceeds that of the general population (2.5-4 times the rate by some estimates).[3, 4]
A reasonable assumption is that underreporting of suicide as the cause of death by sympathetic colleagues certifying death may well skew these statistics; consequently, the real incidence of physician suicide is probably somewhat higher than the prevailing estimate.
The most common psychiatric diagnoses among physicians who complete suicide are affective disorders (eg, depression and bipolar disease), alcoholism, and substance abuse. The most common means of suicide by physicians are lethal medication overdoses and firearms.[22, 23]
Depression in Physicians
Physicians are demonstrably poor at recognizing depression in patients, let alone themselves. Furthermore, they are notoriously reluctant to seek treatment for any personal illness. This may be especially true in the case of potential mental illness. A survey of American surgeons revealed that although 1 in 16 had experienced suicidal ideation in the past 12 months, only 26% had sought psychiatric or psychological help. There was a strong correlation between depressive symptoms, as well as indicators of burnout, with the incidence of suicidal ideation. More than 60% of those with suicidal ideation indicated they were reluctant to seek help due to concern that it could affect their medical license.[24]Other studies in press and in progress reveal that this concern about regulatory intervention is a very common concern hampering help seeking for mental health issues. In addition, other research suggests that 1 in 3 physicians has no regular source of medical care.[25]
Reluctance to recognize depression in a colleague is a tendency shared and imposed by other physicians, who may be well intentioned, habitually emotionally distanced from colleague/competitors, and/or feeling temporarily vulnerable themselves. Even when healthy, physicians find it difficult to ask for help of any kind. When they are depressed and feeling less than adequate, they find it even more difficult—and when they can bring themselves to ask, they sometimes find that the help they need is remarkably difficult to obtain.
To some extent, however, physicians’ reluctance to reach out is self-imposed. They may feel an obligation to appear healthy, perhaps as evidence of their ability to heal others. Inquiring about another physician’s health can shatter this mutual myth of invulnerability, and volunteering support or assistance unasked may seem like an affront to a colleague’s self-sufficiency. Thus, the concerned colleague or partner may say nothing, while wondering privately if the colleague has become impaired.
Unconsciously defending against this painful vulnerability, partners or significant others may also fail to notice significant depression or withdrawal, attributing behavioral changes instead to stress or overwork. Nearly every article about a physician’s suicide contains a quotation from some close contact, occasionally a spouse, saying something like, “I never had any idea that he/she was suffering.”[26]Of course, many physician obituaries omit the fact that the “sudden death” was a completed suicide.
Depressed physicians who do reach out may find that they receive only limited understanding or sympathy from colleagues. There is no specialized training for a physician’s physician (as there is, for example, for the pope’s confessor). Most physicians either shrink from this role or perform it poorly.
For many experiencing depression, the early symptoms are physical. A physician unable to diagnose his or her own symptoms commonly feels incompetent. To admit one’s inability to diagnose oneself to another colleague is to admit failure. When this admission is met with avoidance, disbelief, or derision by a reluctant treating physician, it can only reinforce a depressed physician’s feelings of worthlessness and hopelessness.
Physicians find it painful to share their experience of mental illness with others and know that doing so is somewhat risky; therefore, published accounts of physician depression are very difficult to find. However, recent highly publicized cases of resident and physician suicides and subsequent sharing of experiences of depression by physicians[27]suggest that either the incidence of depression is rising, or we are beginning to be more able to admit and to address the immensity of the problem.
Marriage is in most populations considered to be an effective buffer to emotional distress. This does not seem to be true for women physicians.[23] It is believed that physician divorces are less frequent compared to the general population, but marital problems are common, perhaps in part because of the tendency of physicians to postpone addressing marital problems and to avoid conflict in general.[28]Marital problems, separation, or divorce can certainly contribute to depressive symptoms, which can increase the likelihood of suicidality if unaddressed.
Physicians are a “high control” population (along with law enforcement, lawyers, and clergy), and situations that decrease physicians’ ability to control their environment, workplace, or employment conditions predictably play a higher role in physician suicide than they do in lower control populations.[23] The massive changes that have taken place in medicine in the past several decades, leading to increased workloads and regulatory requirements coupled with decreased ability to control income and patient safety and liability concerns also predictably lead to higher levels of stress, job dissatisfaction, burnout, and depression in physicians.
Litigation-related stress can precipitate depression and, occasionally, suicide.[29, 30]The suicide note of a Texas emergency physician, written the day after he settled a malpractice case, read, “I hope that my death will shed light on the problem of dishonest expert testimony.”[31]Some physicians have completed suicide upon first receipt of malpractice claims, after judgments against them in court, or after financially motivated settlements foisted upon them by a malpractice insurer solely in order to cut the insurer’s losses. Any settlement in a malpractice case is by law reported to the National Practitioner Data Bank, which is yet another source of distress and stigma that can contribute to depression.
Other physicians have attempted or completed suicide in response to employment discrimination relating to judgments or settlements or upon the realization that they are no longer able to practice because of discrimination by liability insurers who refuse to insure them because of past judgments or settlements or because of regulatory licensure investigations or limitations or databank reporting,[32, 33] or in the setting of forced hospitalization or treatment for chemical dependency when a dual diagnosis has not been justified under medically accepted standards.[34]
Problems With Treating Physician Depression
Many clinicians are uncomfortable treating fellow physicians, especially in the realm of mental health.[35]The “VIP syndrome,” characterized by well-intentioned, but superficial or inadequate, treatment based on collegiality and concerns about confidentiality, can detract from the effectiveness of therapy.
Mental health experts who have studied physician depression and suicide stress that immediate treatment and confidential hospitalization of suicidal physicians can be lifesaving—more so than in other populations.[36]Yet, the specters raised by this approach—the fear of temporary withdrawal from practice, of lack of confidentiality and privacy in treatment, or of loss of respect in the community—are often major impediments that hinder physicians from reaching out in a time of crisis and seeking effective treatment.[32, 37, 38]
Physicians who have reported depressive symptoms (even those for which they are receiving effective treatment) to their licensing boards, potential employers, hospitals, and other credentialing agencies have experienced a range of negative consequences, including loss of their medical privacy and autonomy, repetitive and intrusive examinations, licensure restrictions, discriminatory employment decisions, practice restrictions, hospital privilege limitations, and increased supervision.[39, 40, 41, 37, 38]
Such discrimination can immediately and severely limit physicians’ livelihoods as well as the financial stability of their families. For this reason, well-meaning colleagues or family members who are aware of the depression sometimes discourage physicians from seeking help.
Licensure concerns
Medical licensure applications and renewal applications frequently require answers to intrusive questions regarding the physician’s mental health history and may be out of compliance with the provisions of the Americans with Disabilities Act (ADA).[42, 43, 44, 41, 45]
Most states have physician health programs that may or may not be associated with the medical licensing authority, and many have regulations that allow a physician enrolled in a physician health program who is compliant with treatment to check “no” on the mental health questions on licensure applications. However, physicians who are contemplating or in need of treatment are almost universally unaware of such “safe harbor” provisions.
Most physicians assume that any state agency or treating physician will share confidential information about them to the licensing authority.[46]Additionally, any lack of disclosure on an employment or credentialing application can be cited as grounds for termination or decredentialing.
Insurance concerns
Discrimination in obtaining insurance coverage is a common, but little publicized problem for physicians with mental illness. Health, disability, life, and liability insurance may all be denied to a physician who admits to depression.
Even if disability insurance has previously been procured, its use may subject physicians to repeated humiliating and invasive examinations by detached and dubious “independent medical examiners” for the insurer, whose motivation is to cut company losses. Many physicians affected by mental illness feel that insurers expect them to adhere to the standard prescription “physician, heal thyself.”
Self-treatment
Despite the protections afforded by law to citizens and other professionals who have disabilities, the potentially devastating effects triggered by a physician’s self reporting of depression may delay or, in effect, preclude appropriate treatment.
Although everyone knows that a doctor who treats himself or herself “has a fool for a patient,” we also know that most physicians treat themselves anyway, at least on occasion. This is especially likely when the physician believes that the consequences of seeking treatment may subject him or her to stigma, shame, or worse.
Because many states require reporting by other licensed physicians of a physician who may be suffering from a potentially impairing condition, physicians can be reluctant to seek treatment from colleagues, or from utilizing their insurance coverage, or even from using their own names when seeking treatment. A physician whose thought processes are clouded by depression and the anticipated consequences of seeking treatment for it may honestly believe that self-treatment is the only safe option. One analysis of physician suicide data relative to nonphysician victims revealed a much lower prevalence of antidepressant medication in the blood of physician victims, which is an objective indication of the truth that physicians do not receive mental health care in proportion to their need.[23]Too often, however, attempts at self-treatment are unsuccessful. Failure to obtain consultation and treatment for depression needlessly and significantly increases the risk of physician suicide.
Depression in Medical Trainees
Prospective medical students and residents are extremely unlikely to report a history of depression during highly competitive selection interviews. The prevalence of depression in these populations and in medical student and postgraduate trainees is unknown, but it is estimated to range from 15-30%.[5, 6, 7, 8, 9, 47] After accidents, suicide is the most common cause of death among medical students. In one study, 9.4% of fourth-year medical students and interns reported having suicidal thoughts in the previous two weeks.[6]
One report has suggested that depression is not uncommon in pediatric residents (up to 20% self reported in 3 programs). This preliminary study found that residents who experienced depression may be as much as 6 times more likely than nonaffected controls to make medication errors.[48]Other studies have confirmed the association of depression with self-perceived medication and other errors.[49]Recently skyrocketing rates of burnout being reported among physician trainees and physicians have garnered attention[50]. Although burnout does not necessarily lead to depression, some of the symptoms are similar; and burnout probably contributes to the development or onset of depression in those who are predisposed.
Stressful aspects of physician training—such as long hours, having to make difficult decisions while being at risk for errors due to inexperience, learning to deal with death and dying, frequent shifts in workplace, and estrangement from supportive networks, such as family—could add to the tendency toward depressive symptoms in trainees.
Harassment and belittlement by professors, higher-level trainees, and even nurses contribute to mental distress of students and development of depression in some.[51]Even positive workplace changes, such as translocations to secure further training or job advancement, can contribute to job-related stress. Suicide in medical trainees is most likely to occur just prior to beginning clinical rotations, or prior to or at the beginning of residency.
A few schools are implementing programs to recognize and deal with depression and other stresses in medical trainees.[52, 53, 7, 54, 55, 9]The American Foundation for Suicide Prevention has created a video on the topic for physicians and other medical trainees.[56]
Education and Resources
Depression, like substance abuse, is not only more common in physicians than in the general public but also more readily treatable as a rule. This is because of physicians’ strong self motivation to continue successful pursuit of a professional calling, which is an important source of their self-esteem.
More education is needed regarding this disease and its disproportionate and needless toll on the medical profession, beginning in the earliest stages of physician training.[57]In addition, there is an urgent need to change the attitudes of those in health care (including those in the regulatory system), as well as the attitudes of the general public, toward mental illness. Such changes might encourage physicians to be more receptive to a diagnosis of depression and enable them to feel free to seek treatment without the fear of repercussion.
Physicians themselves need to be aware of the existence of physician health programs in nearly every state and province, which allow a physician who is compliant with treatment to avoid disclosing depression or other stable illnesses that do not interfere with ability to practice to licensing authorities.[58] But they also need to be circumspect in dealing with these agencies, and to proceed with caution and full knowledge of the process before entering into it, because of the risk of being entailed into substance abuse programs, if no concomitant substance use disorder exists.[45]
The American Medical Association had a 2009 directive from its House of Delegates to work with the Federation of State Medical Boards and Federation of State Physician Health Programs to study barriers to effective utilization of physician health programs, including assurance of confidentiality safeguards, and to educate members and others regarding the relationships between state licensing authorities and physician health programs. It is unclear what if any effect this activity has had on physician willingness to seek help for mental illnesses. However, the AMA and other organizations have realized that there is an emerging crisis of burnout in physicians and medical trainees, and are taking steps to address at least the burnout component.
WARRIORS:
“Grief does not change you, Hazel. It reveals you.”
Grief is a dynamic emotion that calls for recognition in order to heal us as we evolve. Grief can freeze us, hide us, disguise us or even bury us. But grief can also empower us, strengthen us, deepen our capacities to love, connect and create! Life is about choices…….
(Friends, If you receive our blog post via email please follow our blog link to view video footage)
Besos (kisses) from the Zumba Instructors Convention in Orlando Florida where Kat, I and 7,000 plus global fitness instructors, our brothers and sisters, are dancing, sweating, engaging, and expanding our professional skills in the company of our global Zumba Tribe. Huge THANKS to the three Albertos who created and continue to evolve and empower the international Zumba community (180 countries, 15 million people, 200,000 locations). Zumba is committed to creating health, fitness, peace and love and for that we are joyously grateful.
Within the world of Healthcare communities, countries, and continents collide, connect, intersect, and merge to develop and transform individuals, resources, systems, processes, and medical solutions. A perspective in healthcare that attempts to be isolationist is not only myopic, it is not viable. Let’s travel with curiosity and open minds; keeping our eyes, ears and hearts open……
Cardiac Conditions and Preterm Birth – Close to our Hearts
Come walk with us through a bit of the history of pediatric cardiac surgery…. and celebrate the Global personality of healing, health and medicine.
Living and working in Guatemala resides a brilliant pioneer in pediatric cardiac surgery, Dr. Aldo Casteneda. Born July 17, 1930 in in Nervi, Italy to a Nicaraguan mother and a Guatemalan father, Aldo entered elementary school in Munich, Germany. When World War II began in 1939, his family, Guatemalan citizens, became “enemy aliens” and they were not allowed to leave Germany. Eventually, Dr. Castañeda received his MD training at the University of Guatemala and completed his training as a surgeon through the University of Minnesota. At 86 years of age, Dr. Casteneda continues to provide cardiac surgeries to the neediest children in Guatemala, Honduras, El Salvador, Nicaragua, Belize, Haiti and the Dominican Republic.
We initially discovered Dr. Casteneda in a short video provided by Hearts for Life Across the World-World Society for Pediatric and Congenital Heart Surgery (Every child born anywhere in the world with a congenital heart defect should have access to appropriate medical and surgical care) at: http://www.wspchs.org/index.php/interviews/78-interview-with-dr-aldo-castaneda-intro).
Walking around Greenlake in Seattle WA. one beautiful evening last week we located and listened to (one ear bud per person, nerdy-we know!) a more recent YouTube interview with Dr. Casteneda. The intro to the YouTube (below) itself presents a story of global and national medical significance. Please enjoy this short read:
Published on Dec 9, 2015
“Aldo R. Castañeda is a pioneer in pediatric cardiac surgery. He has been a vigorous supporter of early correction of complex cardiac malformations in infants and newborns. These efforts culminated in the successful repair of transposition in neonates, giving rise to the modern era of neonatal cardiac surgery. Under his mentorship William Norwood developed the Norwood operation for hypoplastic left heart syndrome.”
Dr. Castañeda received his training at the University of Guatemala and the University of Minnesota. Upon completion, he remained at Minnesota as a faculty member. In 1972 he accepted an appointment as Cardiac Surgeon-in-Chief at The Children’s Hospital in Boston and Professor of Surgery at Harvard Medical School. From 1981 to 1994 he served as Surgeon-in-Chief at The Children’s Hospital. Dr. Castañeda’s many contributions to pediatric cardiac surgery are remarkable and well documented in his more than 400 scientific articles and two books.
Dr. Castañeda’s work has spanned the globe. Upon retirement he returned to Guatemala and developed one of the most successful programs for pediatric cardiac surgery in Central America. More than forty of Dr. Castañeda’s trainees have served as chiefs of Pediatric Cardiac Units at institutions across the globe. In 2006 he was appointed to the Pediatric Cardiology Hall of Fame”.
Now, for the SHOW: Please enjoy Dr. Casteneda’s answers the questions posed. His unique personality really shines!
WSPF – “History of Medicine Series: Cardiac Surgery” with Dr. Aldo Castaneda, for OPENPediatrics”-
U.S. News & World Report has ranked Boston’s Children’s Hospital Heart Center # 1 in the Nation – Cardiology and Heart Surgery – 2016/17. Frank Pigula, MD, Director of the Neonatal Cardiac Surgery Service at Boston Children’s Hospital, discusses how the Heart Center team cares for the most complicated prenatal congenital cardiac diagnoses. This video provides a personalized look into the world of neonatal cardiac surgery.
Local Flavor–Shout Out ……and forever thank you’s to Kat’s Cardiac Surgeon, Margaret Allen M.D. – A National Library of Medicine Local Legend. Kat would not have survived her preterm birth if not for the skill, courage, and genius of her cardiac surgeon, Margaret Allen MD and her surgical and after care team. A pioneer in cardiac and transplant surgery, Dr. Allen’s legend continues to unfold through her research (tissue engineering, stem cells, and autologous cardiomyocytes for repair and regeneration of cardiac muscle). Dr. Allen’s inspiring biography can be found at: https://www.nlm.nih.gov/locallegends/Biographies/Allen_Margaret.html
WARRIORS:
Medical research exploring cardiac issues that challenge preterm birth survivors is relatively new. While preterm birth infant survival rates in the USA have dramatically improved over the past few decades, developing research reports that preterm birth has been identified as an emerging risk factor for arterial hypertension, diabetes mellitus, cardiovascular disease, and stroke in later life.
The following article in Forbes Magazine AUG 12, 2013 is interesting and provides us with an opportunity to explore related ongoing medical research.
“Based on results of new research, babies born prematurely may be at risk for structural heart abnormalities which can lead to additional cardiac risk factors such as high blood pressure as they age. This may ultimately impact individuals who are at risk for coronary artery disease, making early screening for high blood pressure particularly important for those who were born prematurely (< 37 weeks)”.
The article cited research in which investigators studied 102 premature infants from birth into their mid 20’s. The article stated “They compared their findings to 132 individuals who were full term, and found that progressing into adulthood, the right lower chamber of the heart (the right ventricle) was smaller in size, but had walls which were significantly thicker with a pumping mechanism which was less efficient compared to those born full term. They also found that the more premature the birth, the greater overall decrease in size as well as function of the right ventricle”.
Dr. Paul Lesson, the lead investigator from Oxford University’s Clinical Cardiovascular Research Facility in England stated “Up to 10 percent of today’s adults were born prematurely, and some have an altered higher cardiovascular risk profile in adult life”.
Dr. Adam Lewandowski, the Lead study author, agreed, explaining, “We are trying to dig deeper into what’s different about the hearts of those born preterm”. He added, “The potential scientific reasons why their hearts are different are fascinating and our study adds to the growing understanding of how premature birth shapes future heart health”.
The article begins with the following summary “Preterm birth, that is, delivery >3 weeks before term, affects an estimated 13 000 000 newborn infants annually, and rates are increasing. In only the United States, ≈500 000 infants are born preterm each year, and of these, 80 000 are delivered very preterm (>8 weeks before the expected date). Without effective care, the number of deaths among very preterm infants would equal that of major causes of death in adults such as Alzheimer disease or essential hypertension. Although mortality after preterm birth was high until a few decades ago, advances in perinatal medicine have resulted in almost universal survival, so the concept of prematurity nowadays is shifting from a pregnancy complication to a common developmental basis for a whole new generation of young adults. Although this progress is very welcome for women delivering preterm, their infants, and their families, there is an increasing concern because preterm birth has been identified as an emerging risk factor for arterial hypertension, diabetes mellitus, cardiovascular disease, and stroke in later life”. The article shares the following suggestion “The most obvious clinical implication of this new knowledge is that young people born very preterm need continued and tailored follow-up, taking the total cardiovascular risk factor burden into account”.
If these articles spike a bit of interest, you may also want to review this December 10, 2012 thought provoking article in Medscape Multispecialty “Premature Birth ‘Should Be New Risk Factor’ for Cardiovascular Disease” which offers interesting research/findings.- http://www.medscape.com/viewarticle/775950
The developing research into preterm birth and cardiovascular disease is new, exciting, and perhaps, for some, concerning. Further research may allow our preterm birth family to understand and promote our own health and well-being as we experience adulthood. Access to emerging medical research may inspire us to discuss questions and concerns with our personal health care providers as we responsibly choose to empower our own well-being. AlohaWarriors!
Seattle Children’s Research Institute Secures $3 million for Seattle-PAP Infant Breathing Support Invention
“April 30, 2014 – Seattle – Today, Seattle Children’s Research Institute announced the receipt of a three year, $3 million dollar grant from the Bill Melinda Gates Foundation to conduct two clinical trials of Seattle-PAP, an affordable device intended to provide breathing support to premature infants. The trials will begin later this spring in the neonatal intensive care unit (NICU) at Texas Children’s Hospital, the largest NICU in the U.S., and will confirm whether Seattle-PAP fosters similar or better outcomes than other infant breathing devices, as preclinical research suggests. If results are favorable, Seattle-PAP, which was developed in-house at Seattle Children’s Research Institute, is expected to be commercially available to healthcare providers around the world by 2017.
Developed by a team co-led by Seattle Children’s CEO Tom Hansen, MD and Charles (Skip) Smith, PhD, Seattle-PAP is significantly cheaper to produce, operate, maintain, and repair than ventilators and other respiratory support devices typically used in U.S. healthcare facilities. These features make Seattle-PAP ideal for use in areas where access to healthcare resources may be limited. To operate the device, only relatively simple supplies are needed, including water, a continuous air supply, a breathing circuit tube, and a tube for the nose.”
“Worldwide, almost 1 million infants die each year from respiratory distress. Most of these deaths occur in resource-limited countries due to a lack of access to respiratory support devices commonly used in the developed world,” said Thomas Hansen, MD, CEO at Seattle Children’s. “Seattle-PAP may be a solution to this problem by making effective respiratory support accessible to newborns anywhere in the world.”
We will be exploring TRAUMA as we view our Neonatal Womb Community at home and abroad….
What is Trauma?
A deeply distressing or disturbing experience:
emotional shock following a stressful event or a physical injury, which may be associated with physical shock and sometimes leads to long-term neurosis.
Physical injury.
KAT-Currently I am working at Harborview Medical Center in Seattle, WA. as an office assistant in the Surgical Residency Department. Seeking a long-term career in surgery it is my pleasure to work alongside and learn from the amazing community members at Harborview Medical Center. At the trauma center of Harborview the sounds of sirens, helicopters, alarms, and codes are a familiar never-ending tune to an even greater symphony of staff and community members that orchestrate themselves on a daily basis to provide care to those whose lives change within an instant.
To me, trauma begins in an instant, often without warning as it deconstructs our reality and shakes us into a new world.
If you have been in the Neonatal ICU or received emergency preterm birth care trauma may be a part of your life story.
As a Neonatal ICU patient the majority of my care was focused on the trauma my tiny body endured each day as I fought, like many of my fellow preemie brothers and sisters, to live. I recognize my unanticipated birth and the loss of my twin brother Cruz was a horrific emotional shock to my family. In a past blog I shared that I received open heart surgery with no anesthia as a neonate. Though my body experienced harsh physical trauma I feel that the surgery may have been equally distressing to my surgeon, surgical and neonatal teams, and my family.
As members of the Neonatal Womb Family we have all have a relationship with trauma. We know what it means to will ourselves forward. I believe it is important for us as a community to acknowledge the trauma we have ALL encountered. Let us extend our deepest empathy and love to the families currently finding themselves in the traumatic experience of having a premature infant and the health-care providers that work within the environment of preterm birth associated trauma each day.
To my fellow NICU Grads/Premature Birth Survivors we have an important voice and role! We are valuable resources to our community! WE ARE SYMBOLS OF HOPE!
“Lighting the way, building community, empowering the NICU/Preterm Birth traveler”-The Neonatal Womb Foundation
Salsa, rumba and mambo… Gloria Estefan… plantains …white-sand beaches, rolling mountains …cigars and rum…
Recently, we shared the March of Dimes preterm birth report card for the USA, and Global Preterm Birth standings per WHO. We queried what can we learn from other nations that would move the USA from a C grade to an A grade? Globally, resources to empower positive changes domestically and abroad are present, accessible and evolving! As our doors open to Cuba; we open our eyes to the wealth of wisdom, experience, and medical resources Cuba presents to the Neonatal Womb Community globally and locally.
Low Birth Weight Outcomes:Why Better in Cuba Than Alabama?
Doctors Neggers and Crowe report that low birth weight (LBW; <2500 g) is the single most important factor affecting neonatal mortality and a significant determinant of post neonatal mortality. They indicate that LBW babies are at an increased risk for serious health problems, ranging from neurodevelopmental disabilities such as cerebral palsy and mental retardation to respiratory disorders. They note that in the United States, 65% of all infant deaths result from LBW and preterm birth. The authors report numerous factors associated with LBW including maternal age, race, weight before pregnancy, weight gain during pregnancy, prenatal care, and use of tobacco and alcohol products. In addition, socioeconomic conditions, nutrition during pregnancy, and anemia are key factors that have been proven to influence the prevalence of LBW. The article states “The percentage of LBW in Cuba is not only much lower than its neighboring developing countries such as Jamaica, Haiti, and the Dominican Republic, but is also lower than far more affluent countries such as England and the United States. Despite a per capita gross domestic product that places Cuba in the fourth quintile of nations, Cuba’s infant mortality rate rivals that of Canada and is lower than the average infant mortality rate in the United States and, in particular, the state of Alabama”. According to World Bank data, 100% of pregnant Cuban women receive prenatal care, defined as medical and nursing care recommended for women before and during pregnancy. In Cuba, implementation of universal health care with a strong focus on community-based services for prenatal care has significantly reduced the prevalence of LBW over the past 20 years. The article outlines several examples for implementing community-based prenatal care in the United States that were considered for adaptation on pilot scales in Alabama and North Carolina (USA).
According to the UN’s World Health Organization, Cuba’s health care system is an example for all countries of the world.
“The Cuban health system is recognized worldwide for its excellence and its efficiency. Despite extremely limited resources and the dramatic impact caused by the economic sanctions imposed by the United States for more than half a century, Cuba has managed to guarantee access to care for all segments of the population and obtain results similar to those of the most developed nations. During her recent visit to Havana in July of 2014, Margaret Chan, Director-General of the World Health Organization (WHO), impressed by the country’s achievements in this field, praised the Cuban health care system: ““Cuba is the only country that has a health care system closely linked to research and development. This is the way to go, because human health can only improve through innovation.”” She also praised ““the efforts of the country’s leadership for having made health an essential pillar of development””. Cuba’s health care system is based on preventive medicine and the results achieved are outstanding. According to Margaret Chan, the world should follow the example of the island in this arena and replace the curative model, inefficient and more expensive, with a prevention-based system. ““We sincerely hope that all of the world’s inhabitants will have access to quality medical services, as they do in Cuba,” she said””.
The article concludes with the following statement: “In praising Cuba, the World Health Organization stresses that it is possible for Third-world countries with limited resources to implement an efficient health care system and provide all segments of the population with social protection worthy of the name. This is possible if the political will exists to put human beings at the center of the project”.
In our “Healers” blog we touched upon the fact (WHO November, 2013) that globally there was a deficit of 7.2 million skilled health professionals, and the deficit is increasing…And the Largest Medical School in the World is in?
CUBA
Havana, Cuba:Latin American Medical School (ELAM) -“Supporting the world’s largest medical school in the education of socially committed physicians.”
“I know of no other medical school with an admissions policy that gives first priority to candidates who come from poor communities and know, first-hand, what it means to live without access to essential medical care. For once, if you are poor, female, or from an indigenous population, you have a distinctadvantage”. ~WHO Director-General Dr. Margaret Chan, visiting ELAM. Dr. Chan states “Cuba has the lowest infant mortality rate in the hemisphere: a child born in the eastern mountains of Cuba has a better chance of survival than a newborn in Washington DC. ” –Source-http://medicc.org/ns/?page_id=63
The Cuban success in decreasing LB weight infants is worthy of our attention. As we investigated Cuba’s health care system we stumbled upon this comprehensive experience based and awakening Ted Talkby journalist Gail Reed:Where to train the world’s doctors?
Journalist Reed discusses how the world’s largest medical school (Havana Latin American Medical School/ELAM) provides:
– community based learning
– teaches students to treat the whole patient
– promotes the concept that a good patient interview and a thorough clinical exam provide most of the clues for diagnoses saving costly technology for confirmation, importance of prevention
– a team approach to teaching, learning, working to support their mission In order totrain physicians “for people that need them the most; the over 1 Billion who have never seen a doctor”.
WARRIORS!
Did you know that surfing in Cuba was illegal for many years? This nostalgic and dynamic YouTube adventure takes us on a short and beautiful journey into Cuba!
The narrator tells us “I believe surfing makes me a better person, challenges me and makes me feel connected to my body and to the ocean in ways that transcend simply being in the water and riding waves.”
-Published on Jun 11, 2013 Ola Libre – A Waterlust film about surfing in Cuba. A film by Mike Gibbons & Patrick Rynne aimed at exploring and supporting the emerging surf culture of Cuba.
How do you choose to be challenged, and what connects you to your body, to nature and our oneness on this life journey?
In the spirit of acknowledging our own development The Neonatal Womb Foundation will “tweek” our Foundation affirmation statement from “Lighting the way, building community, empowering the NICU traveler” to an expanded affirmation of “Lighting the way, building community, empowering the NICU/Preterm Birth traveler”in order to represent our intent to bring light, empowerment and connection into the World of the preterm birth collective.
Today, we want to share a very brief overview of the preterm birth status of our global and national community through the “eyes” of some of well-known preterm birth resources.
WHO? …….
The World Health Organization (WHO) is a specialized agency of the United Nations that is concerned with international public health. It was established on 7 April 1948, headquartered in Geneva, Switzerland.
WHO – Preterm Birth Overview:Preterm is defined as babies born alive before 37 weeks of pregnancy are completed. There are sub-categories of preterm birth, based on gestational age:
extremely preterm (<28 weeks)
very preterm (28 to <32 weeks)
moderate to late preterm (32 to <37 weeks).
Key facts – Preterm Birth
Every year, an estimated 15 million babies are born preterm (before 37 completed weeks of gestation), and this number is rising.
Preterm birth complications are the leading cause of death among children under 5 years of age, responsible for nearly 1 million deaths in 2013.
Three-quarters of them could be saved with current, cost-effective interventions.
Across 184 countries, the rate of preterm birth ranges from 5% to 18% of babies born.
Why does preterm birth happen?
Preterm birth occurs for a variety of reasons. Most preterm births happen spontaneously, but some are due to early induction of labour or caesarean birth, whether for medical or non-medical reasons.
Common causes of preterm birth include multiple pregnancies, infections and chronic conditions such as diabetes and high blood pressure; however, often no cause is identified. There could also be a genetic influence. Better understanding of the causes and mechanisms will advance the development of solutions to prevent preterm birth.
The 10 countries with the greatest number of preterm births:
India
China
Nigeria
Pakistan
Indonesia
The United States of America
Bangladesh
The Philippines
The Democratic Republic of the Congo
Brazil
Nationally…
March of Dimes: The mission of the March of Dimes is to improve the health of babies by preventing birth defects, premature birth and infant mortality.
The March of Dimes, which was initially called the National Foundation for Infantile Paralysis, was founded by President Franklin D. Roosevelt on January 3, 1938, as a response to U.S. epidemics of polio.
Per Wikipedia the name “March of Dimes” — is a play on the contemporary radio and newsreel series, The March of Time — was coined by stage, screen and radio star Eddie Cantor. He inspired a nationwide fundraising campaign in the week preceding President Roosevelt’s birthday on January 30, 1938. Lapel pins were sold for ten cents each; special features were produced by the motion picture studios and radio industry; and nightclubs and cabarets held dances and contributed a portion of the proceeds.
Eleanor Roosevelt and Lucille Ball at the 1944 President’s fundraising Birthday Ball (We LOVE Lucy)
In 1976 it became known as the March of Dimes Birth Defects Foundation. In 2007, the name became the March of Dimes Foundation.
We appreciate The March of Dimes, a National non-profit organization that has grown into a globally connected and dynamic infant and maternal care resource.
The March of Dimes reports the following national preterm birth status:
2015 premature birth report card – USA – 9.5% (per 100 births) – Grade – C
Lowest Preterm Birth Rate by State – Oregon 7.7 per 100 births
Highest Preterm Birth Rate by State – 12.9 Mississippi
Lowest Preterm Birth Rate by City: Portland, Oregon – 7.2
Highest Preterm Birth Rate by City: Shreveport LA – 18.8
What can we learn from Oregon that will allow us to reduce preterm birth rates in Mississippi? And what can we learn from other nations that will help us move our C grade to an A grade in the USA?
RESEARCHhas shown there are multiple factors contributing to the U.S.’s high preterm birth rate. This YouTube video (Why USA You Tube Published on Dec 20, 2014) may offer some insight!
WARRIORS-Surprised that the USA is in the top 10 of Countries with greatest number of preterm births? One of the joys of journeying globally if the opportunity to see the Neonatal Womb from various perspectives and to share information and experiences that will benefit and strengthen our pre-term birth community as a whole!
Neonatal Womb Warriors appreciates and honors the profound commitment and courage a NICU/Preterm birth infant father’s journey entails. THANK YOU!
WARRIORS: Today we celebrate Fathers. Each of us arrived into a world of unique and diverse family circumstances. Some of us are NICU graduates; while many experienced alternative pre-term birth care. We all have fathers or at least hopefully father figures in our lives. Unless we become NICU fathers, or make a concerted effort to gain the perspectives and stories of our fathers, it may be difficult to comprehend the challenges they faced as the parent of a premature infant. Too often their experiences are silenced and ignored.
An article from Preemie Babies 101 Hand to Hold Parent Blog article titled “An Interview With A NICU Dad”; provides a recent father’s response to a wife’s questions regarding a father’s preemie experience.
Dealing with the immense feeling of helplessness. I always felt it was my job to take care of my family and when something happens that is so out of your control, you just feel so powerless. And, then, when I had to go back to work two weeks after my son was born, it was extremely hard to only see him for a short time each day. I felt like I was missing out on so much! Plus, it’s impossible for co-workers and family to understand what you are going through, so there really is no one outside of the NICU that you can talk to about it.
What advice do you have for current NICU dads?
As scared or uncomfortable as you may feel right now, try to help take care of the baby any way you can or are allowed to. Some of the nurses were better at this than others, but asking me to change my son’s diapers and bottle feed him helped to make the whole experience feel more normal. Hang in there and don’t isolate yourself because that will only make you feel worse. Your baby and your baby’s mother need you to be there as much as you can be. Also, I learned so much about my son’s health, and premature babies in general, from the many conversations I had with the nurses and doctors in the NICU. What I learned from them helped me feel less anxious and more confident that my son was going to be fine.”
YOU MAY NEED TISSUES……
This you tube video shares the feelings and thoughts of a few preterm birth fathers, and may shine light upon this particular entrance into fatherhood.
Rex NICU Stories: Dad to Dad – Published on Mar 14, 2014
A Personal Thank you…..
Many preemie babies worldwide do not have a father to help care for them. Working as a volunteer in a local NICU I (Kat) witnessed an event in the life of a micro-preemie and the family that claimed her! Struggling daily to survive and thrive this little being was barely “keeping her head above water” until an amazing family came into her life! The effects of the couple’s loving visits were quickly noticed in the improvement of the baby’s vitals, and overtime, in the steady advancement in the baby’s overall health. Eventually, the baby left the NICU in the arms of the loving adoptive father and mother. The baby continued to grow and I have no doubt that the adoptive parent’s touch, attention, and deep love for the baby played a crucial part in the survival and vitality of the precious child.
We want to SHOUT OUT this week to renown and globally cherished Healer AMMA, who will be visiting the Seattle area on her North American Tour (http://amma.org/meeting-amma/north-america) on June 4 and June 05, 2016. She has been an important part of our healing journeys for many years. Amma’s beauty, wisdom, grace and compassion inspire us daily. Please note that the global tour dates are also posted.
Mata Amritanandamayi, also known as Amma , or the hugging saint, is widely regarded as one of India’s foremost spiritual leaders. Amma says that her religion is love. A compassionate healer, she has never asked anyone to change their religion; only to contemplate the essential principles of their own faith and try to live accordingly. But Amma is also an impassioned force to be reckoned with! She has created an International Network of Charitable Organizations -Embracing the World (http://www.embracingtheworld.org/ ) – an NGO with special Consultative Status to the United Nations that is active in 40 Countries. And although Amma may be small in stature, she is expansive of heart, a beautiful songstress who connects directly to the poorest of poor. The “Crown Jewell” health care center of Embracing the World, Amrita Institute of Medical Science or Aims (1600 bed super-specialty hospital ) is one of Asia’s most advanced and premier medical institutions. Interested in learning more about Amma and her humanitarian efforts ? You Tube videos and even full length movies are available for your viewing pleasure. And like Pope Francis and the His Holiness the Dalai Lama, Amma radiates Joy! (when in doubt, choose Joy! Joy heals….).
Healers:
Merriam Webster defines Healer as one that heals. We are thinking that you and I could have come up with that definition!
“Acts” of healing may be mysterious, intentional , guided, unintentional, apparent or unrecognized. The presence and warm smile of an ER Patient Services Rep. can calm and inspire hope in the incoming patients and their loved ones. We have observed the obvious and subtle healing effects of particular wise and kind environmental service workers working within a health care setting. At times it seems that the disguise of anonymity provides an expanded opportunity to create, enhance, enable wholeness in ourselves and others.
WE have the capacity to enhance our own healing and support the healing of others. Our interaction and awareness of healers/healing in our lives is colored by our beliefs, education, cultural, societal, media presence, biology/biography and life experiences. The science of epigenetics may inspire us to choose to interpret our experiences with positive regard in order to enhance our own healing and well-being.
Many may be aware of contemporary well known healers such as:
Dr. Andrew Weil: an American physician, author, spokesperson, and broadly described “guru” for holistic health and integrative medicine, whose names also constitute an emerging brand of healthcare services and products in these fields-Wikipedia
Hawayo Takata: Hawayo Hiromi Takata, a Japanese-American born in Hanamaulu, Territory of Hawaii, who helped introduce the spiritual practice of Reiki to the Western World – Wikipedia
Judith Orloff MD, board certified psychiatrist and assistant professor of psychiatry at UCLA (http://www.drjudithorloff.com/about-judith-orloff.htm) advocates for “a democracy of healing”, wherein every aspect of our being is granted a vote in the search for total health. It is our birthright, both as health-care givers and health-care recipients, to reclaim our intuition to build energy and well-being.
Health Care Providers may also be powerful and effective healers. Those that are seem to have the ability to be deeply present with their patient, and whatever limited time they have with the patient may be experienced as “timeless”.
Why Healers?
We believe that the human experience is colored with opportunities for personal healing and abundant openings to impact the healing of others. Our unique and precious life journeys will allow us to deny, avoid, acknowledge, embrace and transform the challenges we face. Technology expands our capacity to access diverse and easily accessible health and healing resources, many of which are free! We do not have to wait for something to happen to transform us. We can choose to evolve in ways that empower and free us!
For preterm birth survivors in the USA there sometimes seem to be unspoken assumptions that may close rather than open doors to wholeness and healing. Please chew on this… and be aware that all humans have a right to experience wholeness, vitality, vulnerability and love.
Due to the substantial and increasing shortage of Health Care Providers it is incumbent upon us to empower ourselves and our communities with information that will expand our perceptions of healing, health and well-being. The global Neonatal Womb is in great need of expanded healthcare resources.
In a Publication dated November 2013, Global Health Workforce Alliance and World Health Organization; “A Universal Truth: No Health Without a Workforce” reported that there is a current deficit of about 7.2 million skilled health professionals. A projection model driven by population growth would lead to a global deficit of about 12.9 million skilled health professionals by 2035.
So while we determine how we may advance our Healthcare Workforce (the expansion of community health care workers is a compelling development globally and nationally) we can choose in this moment to acknowledge our ownership and abilities to positively impact our personal healing needs, desires and capabilities.
Last week we walked out the door of NICU-centered preterm birth care into the diverse Global Community of preterm infant care and preemie survivors. Open eyes and hearts allowed us to experience the Neonatal Womb on a broader basis. We hope humility and centeredness will guide our continued awakening to the dynamic nature of our Global Neonatal Womb community. Though intriguing and exciting the journey challenges us emotionally and intellectually. Our hearts expand as we witness the courage and strength of health care providers, families and preterm survivors. Intense love permeates our community. We will learn new language, evolve our perceptions, correct our misconceptions, expand our resources, create space to grow and share “solutions”.
We apologize in advance for our naiveté. Although our Neonatal Womb family includes NICU survivors; much of our family does not have access to NICU care. We are considering language that best identifies the portion of our community that represents our preterm survivors/Warriors. We Trust that we will be guided to effectively evolve our language and wisdom over time.
There is a new HeRO in town!
New Technology is Life-Saving Voice for Premature or Critically Ill Infants-
A new technology in the Neonatal Intensive Care Unit at UC San Diego Health is able to predict the risk of life-threatening infections up to 24 hours before they appear in severely premature or critically ill infants. The heart rate observation system (HeRO) is a new innovation worthy of exploring!
Interested? Please see the May 10, 2016 UC San Diego Health article by Michelle Brubaker:
WARRIORS: Surfing in Westport Washington is fun, but not easy. Waves break hard and fast, rides are short, and paddling out is physically ……strenuous. My sister Ciara and dog Bella motivate and inspire me. What, or who, inspires you to adventure into the unknown?
Join us as we explore our Global Neonatal Womb! As we seek to expand our introspective capacities we hope to increase our knowledge and understanding of our global families, their challenges, resources and research. Over time, with open minds and hearts, we will take a “peek” into Neonatal Womb communities around the world.
Our Journey begins with a wander into Healthy Newborn Network. HNN is a global community of maternal and newborn health professionals and practitioners who state in their website “about” section “The Healthy Newborn Network (HNN) is an online community dedicated to addressing critical knowledge gaps in newborn health”. The resources available through this expansive and globally connected online resource amazed and excited us.
The Republic of Uganda, a landlocked country in East Africa , is the world’s second most populous landlocked country. Uganda is one of the poorest nations in the world. In Uganda, 226,000 babies are born too soon each year and 12,500 children under five die due to direct preterm birth complications. Leading causes of neonatal deaths in Uganda (2013) include 31% due to preterm birth complications. Of the 10 Elements of Care recommended by WHO (World Health Organization) for improved preterm birth outcomes included in Uganda’s clinical standards of care are tocolytics, magnesium sulfate, antibiotics for preterm premature rupture of membranes, and kangaroo mother care.
In RECENT NEWS from Uganda Sandra Janet Birungi posted the following article related to preterm births on April 4, 2016 in the Daily Monitor: Study shows new method to test premature babies.
” KAMPALA. In the absence of weighing scales, measuring the size of a baby’s foot using the foot length card and danger sign screening cards can help identify if a baby is premature or has low birth weight, a new study has shown.
The study by the Makerere School of Public Health, which is being carried out in Iganga and Mayuge districts, targeted 80,000 women. Preliminary results registered a high survival rate for high risk babies admitted to the health facilities and those delivered at home. “Within four months, the trained 150 village health teams (VHTs) helped identify and counsel 764 mothers. Of these, 83 per cent were visited in the first 48 hours. VHTs screened and identified 78 high risk babies of whom 32 were low birth weight or preterm babies,” the study titled reads in part.
Dr. Getrude Namazzi, the lead researcher, said of the 280 high risk babies admitted to Iganga hospital for the past four months, 40 per cent were low birth weight. Of these, 91 per cent survived and were discharged alive and well.
Feet have more than 80 per cent sensitivity and specificity so they can be used to find low birth weight and pre-term babies and we have just found out that it works. The study has proved that high risk babies can survive and thrive even in resource-constrained settings using low cost strategies” Dr. Namazzi said while releasing the results in Kampala last Wednesday. “



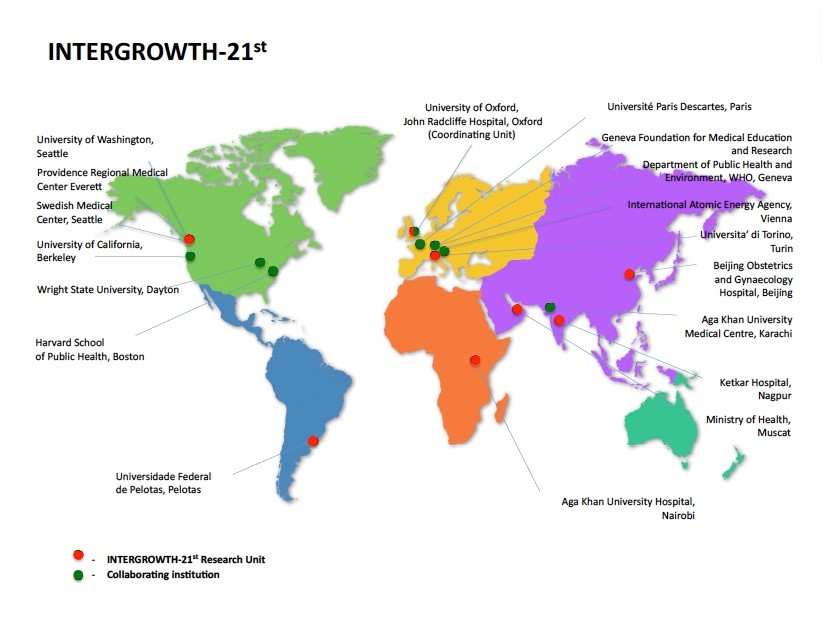
























")
")






















