SOUTH AFRICA




- Home of Christiaan Barnard, Nelson Mandela, Dave Matthews, Desmond Tutu
- Preterm birth rate – 8 (births <37 weeks per 100 live births)
- Preterm birth rate – USA – 12 per 100 births
Source: https://www.healthynewbornnetwork.org/country/south-africa/
South Africa, officially the Republic of South Africa (RSA), is the southernmost country in Africa. South Africa is the largest country in Southern Africa and the 25th-largest country in the world by land area and, with close to 56 million people, is the world’s 24th-most populous nation. South Africa is a multiethnic society encompassing a wide variety of cultures, languages, and religions. Its pluralistic makeup is reflected in the constitution‘s recognition of 11 official languages, which is the fourth highest number in the world. Since 1994, all ethnic and linguistic groups have held political representation in the country’s democracy, which comprises a parliamentary republic and nine provinces. South Africa is often referred to as the “rainbow nation” to describe the country’s multicultural diversity, especially in the wake of apartheid. The World Bank classifies South Africa as an upper-middle-income economy, and a newly industrialised country. South Africa is still burdened by a relatively high rate of poverty and unemployment, and is also ranked in the top 10 countries in the world for income inequality. In South Africa, private and public health systems exist in parallel. The public system serves the vast majority of the population, but is chronically underfunded and understaffed. The wealthiest 20% of the population use the private system and are far better served. About 79% of doctors work in the private sector.
Source: https://en.wikipedia.org/wiki/South_Africa




INNOVATIONS
We note and appreciate the efforts of many Nations World-Wide working together to bring universal healthcare to our global population and our Neonatal Womb community members!

High Aspirations for Universal Healthcare in South Africa
On 21 June 2018, the Minister of Health published the draft National Health Insurance Bill, 2018 (NHI Bill) for public comment. The NHI Bill aims to enable access to free, universal, high-quality healthcare for all, by creating a single national health insurance fund; and would centralise procurement of medical supplies by the State.
Mobilizing Tech for Moms: MomConnect in South Africa
Published on Jun 11, 2018- Through programs like MomConnect in South Africa, Johnson & Johnson uses mobile technology to reach 6 million moms in 10 countries with health information provided by BabyCenter.

MomConnect: Fostering a long-term, supportive dialogue with mothers in South Africa
As patient groups go, pregnant women and new mothers are among the most motivated. They’re eager for information on how to care for themselves and their children, and quick to take action to ensure their children have the best start in life. But in some low-income countries around the world, accessing high-quality health information at exactly the right time is not always easy. Recognizing the role a mobile phone could play in reaching expectant and new mothers, Johnson & Johnson made a commitment to Every Woman Every Child in 2010 to work with partners to reach women in six countries with evidence-based messages to motivate behavior change, and increase the likelihood that women would seek out antenatal health services.
Eight years after the initial Johnson & Johnson commitment, three of the six country programmes (Bangladesh, India, and South Africa) have reached more than a million mothers each.
How did this happen?
MomConnect, South Africa’s national mobile messaging service, is a useful case study. It has had a true commitment to universal coverage right from the start, and currently reaches over 60% of all eligible pregnant women in the country through over 95% of public clinics – the highest population coverage of any program of its kind in the world. The program is managed by the South African National Department of Health, with a diverse range of funding, technology, health and research organizations at the table.
To encourage uptake, BabyCenter collaborated with local partners to create messages that were carefully targeted to be relevant to the mother’s pregnancy stage or baby’s age. Messages were designed to have a warm, culturally-sensitive and relatable tone, and to provide parenting support and content to promote bonding, alongside more technical health promotion messages.
There have been several key elements to MomConnect that have made scale possible:
- It is accessible through all mobile phones. It uses the most simple USSD and SMS mobile technologies – despite their high costs at scale – to ensure that no mother is excluded because of the kind of phone she has. But as user habits have changed, MomConnect has also recently expanded to include WhatsApp as a richer and more affordable messaging platform.
- The messaging engages and empowers users, fostering a relationship of trust with the service and the health system. In a sample of 2000 women, 98% found the messages helpful, 77% felt better prepared for delivery, 81% shared their messages with family and friends, and 70% wanted more messages per week.
- It has had critical public-sector ownership. Private funders, with a larger appetite for risk, have contributed upfront investment and technical know-how to get MomConnect started, but only in the context of strong public leadership and an enabling policy environment.
- It can be adapted over time. The platform has been built with open architecture and open standards so that new features and functionality of increasing complexity can be added to engage new partners and users over time.
- It integrates supply and demand. The service doesn’t just push out messaging, but enables two-way interaction between the pregnant mother and the health system through phone-based surveys and a helpdesk. This enables real-time data collection on user knowledge, attitudes, practices, and experiences of service delivery to inform health care improvements.
With a technology platform now reaching over a million active users, MomConnect made it possible to bring direct messaging to mothers across the country with a flip of a switch during South Africa’s recent Listeriosis outbreak. MomConnect’s critical challenge remains long-term sustainability. Beyond maintaining its existing digital infrastructure, it needs to be agile to evolve in line with the technology landscape and the habits and needs of its users.
It will always need some degree of private funding for innovation, and it is critical that an ecosystem of funders and partners stay the course to collectively refine and augment this important public good for collective impact.
You can learn more about MomConnect in South Africa by reading this commentary and this article in the British Medical Journal.
- Download PDF
- Full Text
MomConnect & WhatsApp
Published on Jan 22, 2018-Animation shared at CES 2018 on the innovation behind the South African Department of Health’s MomConnect and NurseConnect platforms.


Association of Gestational Age at Birth With Symptoms of Attention-Deficit/Hyperactivity multimedia icon
JAMA NETWORK ORIGINAL INVESTIGATIONMultimedia-August 2018
KEY POINTS
Questions Is the association between gestational age at birth and symptoms of attention-deficit/hyperactivity disorder the same at 5 and 8 years of age, and are there possible sex differences in the associations?
Findings In this population-based cohort study of 113 227 children that used a sibling comparison approach to adjust for confounding, an association was found between early preterm birth (gestational age <34 weeks) and symptoms of attention-deficit/hyperactivity disorder in preschool and school-age children.
Meaning The findings illustrate potential gains of reducing preterm birth and the importance of providing custom support to children born preterm to prevent neurodevelopmental problems.
Abstract-
Importance Preterm birth is associated with an increased risk of attention-deficit/hyperactivity disorder (ADHD); however, it is unclear to what extent this association can be explained by shared genetic and environmental risk factors and whether gestational age at birth is similarly related to inattention and hyperactivity/impulsivity and to the same extent in boys and girls.
Objectives To investigate the association between gestational age at birth and symptoms of ADHD in preschool and school-age children after adjusting for unmeasured genetic and environmental risk factors.
Design, Setting, and Participants In this prospective, population-based cohort study, pregnant women were recruited from across Norway from January 1, 1999, through December 31, 2008. Results of a conventional cohort design were compared with results from a sibling-comparison design (adjusting for genetic and environmental factors shared within families) using data from the Norwegian Mother and Child Cohort Study. Data analysis was performed from October 1, 2017, through March 16, 2018.
Exposures Analyses compared children and siblings discordant for gestational age group: early preterm (delivery at gestational weeks 22-33), late preterm (delivery at gestational weeks 34-36), early term (delivery at gestational weeks 37-38), delivery at gestational week 39, reference group (delivery at gestational week 40), delivery at gestational week 41, and late term (delivery after gestational week 41).
Main Outcomes and Measures Maternally reported symptoms of ADHD in children at 5 years of age and symptoms of inattention and hyperactivity/impulsivity at 8 years of age. Covariates included child and pregnancy characteristics associated with the week of delivery and the outcomes.
Results A total of 113 227 children (55 187 [48.7%] female; 31 708 [28.0%] born at gestational week 40), including 33 081 siblings (16 014 female [48.4%]; 9705 [29.3%] born at gestational week 40), were included in the study. Children born early preterm were rated with more symptoms of ADHD, inattention, and hyperactivity/impulsivity than term-born children. After adjusting for unmeasured genetic and environmental factors, children born early preterm had a mean score that was 0.24 SD (95% CI, 0.14-0.34) higher on ADHD symptom tests, 0.33 SD (95% CI, 0.24-0.42) higher on inattention tests, and 0.23 SD (95% CI, 0.14-0.32) higher on hyperactivity/impulsivity tests compared with children born at gestational week 40. Sex moderated the association of gestational age with preschool ADHD symptoms, and the association appeared to be strongest among girls. Early preterm girls scored a mean of 0.8 SD (95% CI, 0.12-1.46; P = .02) higher compared with their term-born sisters.
Conclusions and Relevance After accounting for unmeasured genetic and environmental factors, early preterm birth was associated with a higher level of ADHD symptoms in preschool children. Early premature birth was associated with inattentive but not hyperactive symptoms in 8-year-old children. This study demonstrates the importance of differentiating between inattention and hyperactivity/impulsivity and stratifying on sex in the study of childhood ADHD.
Helga Ask, PhD1; Kristin Gustavson, PhD1,2; Eivind Ystrom, PhD1,2; et al Karoline Alexandra Havdahl, PhD1,3; Martin Tesli, MD, PhD1,4; Ragna Bugge Askeland, MSc1; Ted Reichborn-Kjennerud, MD, PhD1,5
Author Affiliations Article Information
- 1Norwegian Institute of Public Health, Oslo, Norway
- 2Department of Psychology, University of Oslo, Oslo, Norway
- 3MRC Integrative Epidemiology Unit, Bristol Medical School (Population Health Sciences), University of Bristol, Bristol, United Kingdom
- 4NORMENT, KG Jebsen Centre for Psychosis Research, Division of Mental Health and Addiction, Oslo University Hospital, Oslo, Norway
- 5Institute of Clinical Medicine, University of Oslo, Oslo, Norway
JAMA Pediatr. 2018;172(8):749-756. doi:10.1001/jamapediatrics.2018.1315
Source: https://jamanetwork.com/journals/jamapediatrics/article-abstract/2685909

HEALTH CARE PARTNERS
Delayed cord clamping and cord-blood milking are proactive medical procedures offering hope for more effective preterm delivery methodology. If shown to be effective over time, these procedures could impact preterm birth babies in a positive way world-wide. 😊
 Neonatal Research Institute at Sharp Mary Birch Hospital for Women & Newborns WebsEdgeHealth – Published on Apr 24, 2018
Neonatal Research Institute at Sharp Mary Birch Hospital for Women & Newborns WebsEdgeHealth – Published on Apr 24, 2018
Experts at Sharp Mary Birch Hospital for Women and Newborns established the Neonatal Research Institute (NRI) to identify and disseminate the latest evidence-based best practices for newborn care. Sharp Mary Birch is the busiest maternity hospital in California, with a baby born every hour on average. That volume provides doctors and researchers with a unique opportunity to create a strong research infrastructure that will yield meaningful breakthroughs. Already, breakthroughs related to cord-blood milking and delayed cord clamping have shown improvements in brain, lung, and heart function for newborns. Now the NRI is building for the future with a clinic that will track the health outcomes of its patients through childhood, demonstrating the long-term benefits of interventions which can be initiated in the first moments of life.

BLOG: Born Too Soon in a Country at War. Their Only Hope? This Clinic.
This baby girl has stopped breathing. She was born prematurely and is only 3 weeks old. Her mother, Restina Boniface, took her to the only public neonatal clinic in South Sudan. The country is one of the toughest places in the world for newborns with health problems to survive.
Ten feet away sits a donated respiratory machine that could save the baby. But lacking a critical part, it goes unused.
The doctor tries to resuscitate the baby for several minutes. Finally, she begins breathing on her own.
One in 10 babies brought to this clinic will die, most from treatable conditions. But many mothers have nowhere else to go.
South Sudan, the world’s youngest nation, is in the midst of a humanitarian crisis. A brutal civil war has drained the economy. As hospitals closed, doctors were forced to flee. Inside the clinic, many babies remain nameless. Their mothers know they may not make it. “Our mothers here, they come for help,” said Rose Tongan, a pediatrician. “And you pity them. You can’t do anything.”
Electricity cuts out for days at a time.
There is no formula for the premature babies, no lab for blood tests, no facility for X-rays.
There are no beds for breast-feeding mothers. They must sleep outside, where they are at risk of infection and vulnerable to assault. “I feel like: What can I do?” Dr. Tongan said.
Hellen Sitima’s 3-day-old daughter is sick. “When we get home, then that’s the time to name the baby,” she says.
Dr. Tongan has no access to lab tests, but she determines that Ms. Sitima’s baby has a respiratory infection.
The infection clears, and Ms. Sitima takes her daughter home. She names her Gift.
Ms. Boniface’s baby, who was resuscitated earlier, died in the clinic. She was never named.
Kassie Bracken is a video journalist for The New York Times, and Megan Specia is an editor on the International Desk. They were 2018 fellows with the International Women’s Media Foundation’s African Great Lakes Reporting Initiative.
 How do we help preterm birth partners in countries at war? Human Security, physician/health care provider access and simple, effective, portable resources are things to consider.
How do we help preterm birth partners in countries at war? Human Security, physician/health care provider access and simple, effective, portable resources are things to consider.

mOm – The Inflatable Incubator CBS News Report
Published on Jun 3, 2016 – James Roberts explain how the mOm incubator came to fruition
- *** Check out the evolution of this innovation at:
- http://www.momincubators.com/

PREEMIE FAMILY PARTNERS


Consuming fish may reduce premature birth risk
Eating fish or taking a fish oil supplement may reduce the risk of preterm birth among pregnant women with low level of omega-3 fatty acids, a new study has found.
The findings indicated that pregnant women who had low plasma levels of long chain n-3 fatty acids — found in fish oil — in their first and second trimesters were at a significantly higher risk of preterm birth as compared with women who had higher levels of these fatty acids.
The researchers suggest that low concentrations of certain long chain fatty acids — eicosapentaenoic acid and docosahexaenoic acid (EPA+DHA) — may be a strong risk factor for preterm birth.
“At a time when many pregnant women are hearing messages, encouraging them to avoid intake of fish altogether due to mercury content, our results support the importance of ensuring adequate intake of long chain omega-3 fatty acids in pregnancy,” said lead author Sjurdur F. Olsen from the Harvard T.H. Chan School of Public Health in Boston.
Preterm birth is a leading cause of neonatal death and is associated with cognitive deficiencies and cardiometabolic problems later in life among survivors.
For the study, published in the journal EbioMedicine, the research team examined 96,000 children in Denmark through questionnaires and registry linkages.
They also analysed blood samples from 376 women who gave premature birth (prior to 34 weeks of gestation) between 1996 and 2003 and 348 women who had a full-term birth.
All of the women gave blood samples during their first and second trimesters of pregnancy.
The analysis of the blood samples showed that women who were in the lowest quintile of EPA+DHA serum levels — with EPA+DHA levels of 1.6 per cent or less of total plasma fatty acids — had a 10 times higher risk of early preterm birth when compared with women in the three highest quintiles, whose EPA+DHA levels were 1.8 per cent or higher.
Women in the second lowest quintile had a 2.7 times higher risk compared with women in the three highest quintiles.
Source: https://www.dayafterindia.com/2018/08/03/consuming-fish-may-reduce-premature-birth-risk/
It is often difficult to know how to interact with a preemie parent or family member. Congratulating the preemie parents/family on the birth of their child, acknowledging their losses, concerns and the courage their journey requires, listening, helping out at their home, sitting in silence with them are actions preemie parents may truly appreciate. The preterm birth journey is unpredictable, often leaving friends and family feeling awkward and without behavioral guidelines.
Funny Things People Say To Mums Of Premature Babies
YouTube · 6/9/2015 by Channel Mum

COMMUNITY
Our environment has a significant impact on preterm birth, offering us the opportunity to invest in preterm birth prevention in many innovative and financially beneficial ways.
Closing coal, oil power plants leads to healthier babies
Mind & body, Research, Science & environment By Robert Sanders, Media relations| May 22, 2018/May 23, 2018
Shuttering coal- and oil-fired power plants lowers the rate of preterm births in neighboring communities and improves fertility, according to two new University of California, Berkeley, studies.
The researchers compared preterm births and fertility before and after eight power plants in California closed between 2001 and 2011, including San Francisco’s Hunters Point plant in 2006.
Overall, the percentage of preterm births – babies born before 37 weeks of gestation – dropped from 7 percent in a year-long period before plant closure to 5.1 percent for the year after shutdown. Rates for non-Hispanic African-American and Asian women dropped even more: from 14.4 percent to 11.3 percent.
Preterm births, which can often result in babies spending time in a neonatal intensive care unit, contributes to infant mortality and can cause health problems later in life. The World Health Organization estimates that the cost of preterm births, defined as births between 32 and 37 weeks of gestation, accounts for some $2 billion in healthcare costs worldwide.
The 20-25 percent drop in preterm birthrates is larger than expected, but consistent with other studies linking birth problems to air pollution around power plants, said UC Berkeley postdoctoral fellow Joan Casey, the lead author of a study to be published May 22 in the American Journal of Epidemiology.
Another paper published May 2 in the journal Environmental Health used similar data and found that fertility – the number of live births per 1,000 women – increased around coal and oil power plants after closure.
“We were excited to do a good news story in environmental health,” Casey said. “Most people look at air pollution and adverse health outcomes, but this is the flip side: We said, let’s look at what happens when we have this external shock that removes air pollution from a community and see if we can see any improvements in health.”
Retiring fossil fuel power plants
The findings, she said, could help policy makers in states like California more strategically plan the decommissioning of power plants as they build more renewable sources of energy, in order to have the biggest health impact.
“We believe that these papers have important implications for understanding the potential short-term community health benefits of climate and energy policy shifts and provide some very good news on that front,” said co-author Rachel Morello-Frosch, a UC Berkeley professor of environmental science, policy and management and of public health and a leading expert on the differential effects of pollution on communities of color and the poor. “These studies indicate short-term beneficial impacts on preterm birth rates overall and particularly for women of color.”
In a commentary accompanying the AJE article, Pauline Mendola of the Eunice Kennedy Shriver National Institute of Child Health and Human Development said: “Casey and colleagues have shown us that retiring older coal and oil power plants can result in a significant reduction in preterm birth and that these benefits also have the potential to lower what has been one of our most intractable health disparities. Perhaps it’s time for the health of our children to be the impetus behind reducing the common sources of ambient air pollution. Their lives depend on it.”
The researchers compared preterm birth rates in the first year following the closure date of each power plant with the rate during the year starting two years before the plant’s retirement, so as to eliminate seasonal effects on preterm births. They also corrected for the mother’s age, socioeconomic status, education level and race/ethnicity.
Dividing the surrounding region into three concentric rings 5 kilometers (3 miles) wide, Casey delved into state birth records to determine the rate of preterm births in each ring.
Those living in the closest ring, from zero to 5 kilometers from the plant, saw the largest improvement: a drop from 7 to 5.1 percent. Those living in the 5-10 kilometer zone showed less improvement. Those living in the 10-20 km zone were used as a control population. They also considered the effects of winds on preterm birth rates, and though downwind areas seemed to exhibit greater improvements, the differences were not statistically significant.
As a control, they replicated their analysis around eight power plants that had not closed, and found no before-versus-after difference, which supported the results of their main analyses. There did not appear to be any effect on births before 32 weeks, which Casey said may reflect the fact that very early births are a result of problems, genetic or environmental, more serious than air pollution.
Casey noted that the study did not break out the effects of individual pollutants, which can include particulate matter, sulfur dioxide, nitrogen oxides, benzene, lead, mercury and other known health hazards, but took a holistic approach to assess the combined effect of a mix of pollutants.
“It would be good to look at this relationship in other states and see if we can apply a similar rationale to retirement of power plants in other places,” Casey said.
Other co-authors of the AJE paper are Deborah Karasek, Kristina Dang and Paula Braveman of UC San Francisco, Elizabeth Ogburn of the Johns Hopkins University Bloomberg School of Public Health in Baltimore and Dana Goin of UC Berkeley.
This research was supported by the UC San Francisco California Preterm Birth Initiative, which is funded by Marc and Lynne Benioff. Additional support was provided by grants from the National Institute of Environmental Health Sciences (K99ES027023, P01ES022841, R01ES027051) and the U.S. Environmental Protection Agency (RD-83543301).
Source:http://news.berkeley.edu/2018/05/22/closing-coal-oil-power-plants-leads-to-healthier-babies/
Domestic Violence is a factor that increases preterm birth rates, and is a preterm birth factor we can change together. Investment in the prevention of preterm birth should always be a primary objective.
Domestic Violence Statistics (USA-2017)
- Every 9 seconds in the US a woman is assaulted or beaten.
- Around the world, at least one in every three women has been beaten, coerced into sex or otherwise abused during her lifetime. Most often, the abuser is a member of her own family.
- Domestic violence is the leading cause of injury to women—more than car accidents, muggings, and rapes combined.
- Every day in the US, more than three women are murdered by their husbands or boyfriends.
- The costs of intimate partner violence in the US alone exceed $5.8 billion per year: $4.1 billion are for direct medical and health care services, while productivity losses account for nearly $1.8 billion.
- Source: https://domesticviolencestatistics.org/domestic-violence-statistics/

Domestic Violence Can Double Risk of Preterm Birth
Physical injuries and inadequate maternal care lead to serious complications-
- January 13, 2017 By domesticshelters.org
- A study out of the University of Iowa revealed what most of us could have already guessed—domestic violence during pregnancy puts both mom and baby at increased risk for serious health problems. Published this past March in BJOG: An International Journal of Obstetrics and Gynaecology, the results show intimate partner violence during pregnancy is “significantly associated with” preterm birth (before 38 weeks) and low birth weight, finding that women who endured abuse while pregnant were almost twice as likely to deliver their babies preterm.
- Trauma to a woman’s abdomen, as well as sexual abuse, may increase the risk of spontaneous abortion, preterm delivery, low birth weight or neonatal death, say researchers, but the risks aren’t limited just to those abused physically. Adverse birth outcomes are also linked to increased stress, inadequate nutrition and prenatal care, and negative maternal behavior. This could include smoking, drinking or not sleeping, says family practice doctor and American Academy of Family Physicians Board Chair, Wanda Filer, MD.
- “Different people cope differently with stress,” says Filer. Being stressed, drinking, smoking and not staying active can cause high blood pressure, which can have negative implications on the health of the placenta, she says. After 20 weeks, high blood pressure could lead to a condition called preeclampsia, which can cause serious damage to the mother-to-be’s organs, such as the brain and kidneys. While this condition is rare, roughly affecting only about 5 percent of pregnant women, it can lead to more serious complications such as seizures. This is classified as eclampsia, a condition which can be fatal.
- Other complications of high blood pressure during pregnancy include placental abruption—an emergency condition in which the placenta detaches from the uterus prematurely—as well as low birth weight and an increased risk of C-section birth.
- The National Institutes of Health (NIH) estimates abusers target more than 300,000 pregnant women in the U.S. each year, adding that the number may be even higher than that given the reluctance of survivors to disclose abuse, especially during pregnancy.
- This, combined with the fact that the NIH also lists homicide as one of the leading causes of death of pregnant women (Filer says she believes it is the leading cause of death, though research varies), means women with abusive partners who become pregnant should be aware that their lives are in danger in more ways than one.
- “When a woman is pregnant, she is developing a relationship with, and focusing on, this new baby. And as we know, the abuser wants the focus on him,” says Filer. “My suspicion is the abuse escalates to turn the focus back on the abuser. It’s a way to exert control.”
- Filer has been an outspoken advocate for more domestic violence training among medical professionals for the last 25 years. Luckily, she believes there have been significant improvements in the screening process of pregnant women by their medical staff to ask about domestic violence in the home.
- “Twenty-five years ago, it [screening] was non-existent. Now, it’s routine. I have seen a better interface between domestic violence shelters and the medical community.” In Pennsylvania, where Filer practices, she says it’s not uncommon for domestic violence shelters to come into medical practices and do hour-long presentations on the victim services they offer.
- What You Can Do
- It is always your call whether or not to reach out for help, and when, as a survivor of abuse. Only you know when it’s safe to do so. However, if you’re looking for a window to reach out to an advocate, consider doing it during one of your prenatal appointments when your partner is either not with you, or not in the room, suggests The National Domestic Violence Hotline. You can ask your doctor or nurse if you can call a local shelter or national crisis hotline from the safety of their office.
- Also make sure to inform your doctor of any injuries or health concerns you have as a result of the abuse. This includes physical injuries, high stress levels or a lack of access to proper prenatal care, such as if your abuser is preventing you from eating healthy, sleeping or otherwise taking care of yourself. Full disclosure of any health concerns will give your baby the best chance for proper medical care.
WARRIORS:
- Healing Preverbal Trauma-Dr. Arielle Schwartz
- Posted on March 2, 2018 by Arielle Schwartz
- Finding Freedom through Trauma Recovery
This post discusses the therapeutic treatment of preverbal trauma. Sometimes the most persistent PTSD symptoms are connected to events for which you have no clear memory. This might be the case if you were told that your life is the result of an unwanted pregnancy, if you endured medical complications around your birth, if you grew up neglected, or if you suffered from child abuse.
In addition to these early memories, some people are unable to remember traumatic events that occurred later in life. This is because traumatic stress can impair brain structures involved with memory. I refer to these as nonverbal trauma memories.
Preverbal trauma and nonverbal trauma memories typically do not have associated words or a clear and coherent story. In contrast, they might come in the form of flashes of images, disconnected fragments, or uncomfortable physical sensations with no known cause.
Most importantly, you might ask whether healing is possible if you are unable to remember these traumatic events?
“In my experience, memory retrieval is not always possible. Moreover, many therapists do clients a disservice when they make memory retrieval the focus of therapy. However, there is hope—you can heal whether or not you remember your preverbal trauma.”
-Dr. Arielle Schwartz
Regaining Emotional Control
Babette Rothschild, trauma expert and author of The Body Remembers vol. 2 (2017), writes “Loss of control is at the core of PTSD.” This statement is a firm reminder that an essential component in healing trauma involves reclaiming a sense of control in your life, now. The first stage of trauma treatment is stabilization which involves successfully managing symptoms of traumatic stress such as anxiety, panic attacks, dissociation, or somatic distress.
When you are no longer overwhelmed by your trauma memories you can cultivate the freedom to live the life you want now.
Since preverbal memories are often related to very young time in your life, healing involves building resources in the here and now and can help you compassionately attend to the pain from your past. Resources for trauma recovery including reclaiming a sense of safety, grounding, and containment.
Memory Retrieval or Trauma Recovery?
Once you have access to resources, you might choose to work with the sensations, emotions, or memory fragments associated with preverbal trauma and nonverbal memories. However, it is important to be cautious when working with preverbal and nonverbal memories as these fragments and sensations do not necessarily represent an exact replay of original events.
Traumatic experiences are stored with emotional information disconnected from contextualizing information. When we remember any memory, we are almost always inserting new information related to our present state of mind and environment. This is especially true for preverbal and nonverbal memories because the original experience is lacking essential details. As human beings, we are storytellers and we will fill in missing elements of memories—we have a fundamental need to develop a narrative that is consistent with our current beliefs and sense of self.
The goal of therapy for preverbal trauma and nonverbal memories is not memory retrieval. Sometimes memories arise spontaneously; but, even in such moments we must uphold that memory is vulnerable to influence.
In contrast, the goal of therapy is trauma recovery in which you actively distinguish the past from the present, develop a sense that you are at choice about how to respond to your world now, and experience of yourself as a resilient.
Healing preverbal trauma involves working with any present symptoms of anxiety, panic attacks, dissociation, or somatic distress. It is common to feel nauseous, numb, foggy, fatigued, or disconnected when preverbal or nonverbal trauma memories arise. Therefore, healing requires the careful guidance of a well-trained therapist, using fine-tuned approaches such as EMDR Therapy, somatic psychotherapy, and Parts Work therapy. Throughout the process, you learn to become highly descriptive of your somatic experience, work through “stuck” sensations in your body, and attend to unmet childhood needs from your past as a resourced adult in the present.
Again, and it is worth reiterating, the outcome of successful trauma treatment is to recognize that the trauma is in the past…and that it is over.
Source: https://drarielleschwartz.com/healing-preverbal-trauma-dr-arielle-schwartz/#.W6SIFsHQZeU
KAT CHAT

I am walking the path of a preterm birth survivor…. At 27 years of age repressed feelings are knocking at my door.
First Step -Regression Therapy
Following months of seeking to identify a therapist to best meet my needs I discovered a hopeful match. And she was great!
I was genuinely afraid of stepping into the dark abyss of repressed feelings and visceral knowing. My love for my preterm brothers and sisters inspired me to move forward with courage and resolve. The therapist offered numerous healing modalities and I choose regression therapy to begin this part of my wellness adventure.
Lillian (not her actual name) welcomed me with a broad smile, bright blue eyes, and open arms directing me into a sacred healing space. Completed patient paperwork in hand, Lillian conducted a comprehensive interview while preparing me to enter the mysteries of my deeper, fuller self. During the long session, we meditated, explored my birth story, loss of my twin, heart surgery and my NICU experiences. At times during the session I experienced strong physical pressure and pain, changing breathing patterns, but I contained my emotions (a clear indication of my defensiveness). At times Lillian expertly changed the course of our journey to compliment my readiness to move further into my past. The session ended with a review of the healer’s prescription (journaling), a plan for our next session, and a discussion of potential side effects of treatment.
One week post-session following periods of head, back, shoulder, lung, and chest pain, unanticipated waves of emotion, fatigue followed by sporadic energy bursts I am feeling a little more free, a bit more aware of triggers, and relief that I choose to confront my fears and to seek wholeness. I remain focused on learning to feel safe in my body and with others. I am learning to recognize my feelings and to “sit with” uncomfortable emotions. This step , the first of many, is filled with compassion for myself and others. I travel, not alone, but with you in my heart.
Love, Kat

Faces of Africa : Surfers not Street Children
- This long video is inspirational, educational, heart-warming, raw and well-worth watching.
- CGTN Africa – Published on Mar 31, 2015
South Africa has hundreds of children living rough on the streets, many spiralling into crime and suffering from the effects of addiction. Eighteen year old Ntando Msibi has gone from street kid to surfing star with many awards to his name. He was helped to this path by the Durban charity, Surfers Not Street Children and credits them with rescuing him from the harshness of life on the streets. Amongst its many programmes aimed at getting street children get back into society, it is surfing that has proven the biggest hit leading to the transformation of lives that many had given up on and has become a new wave of change with young black surfers succeeding in a sport once known for the whites.
***Ntando Msibi became a Pro Surfer in 2016

 … Oh, Panama…………
… Oh, Panama…………





 Remarkable Improvements in Maternal and Child Health Care in
Remarkable Improvements in Maternal and Child Health Care in 


 Autism spectrum disorder and prematurity: towards a prospective screening program.
Autism spectrum disorder and prematurity: towards a prospective screening program. Success of
Success of 




 , another opens
, another opens 



 A kidney transplant surgery is performed at the Grodno Oblast Clinical Hospital
A kidney transplant surgery is performed at the Grodno Oblast Clinical Hospital




 Kat and I were pleased to read a copy of a recent letter sent by APHA to Washington DC encouraging support of federal research and promoting known interventions and community initiatives related to preterm birth.
Kat and I were pleased to read a copy of a recent letter sent by APHA to Washington DC encouraging support of federal research and promoting known interventions and community initiatives related to preterm birth.






















 Premature birth test being trialed
Premature birth test being trialed







 BRASIL
BRASIL








 By Robert Preidt, HealthDay Reporter
By Robert Preidt, HealthDay Reporter


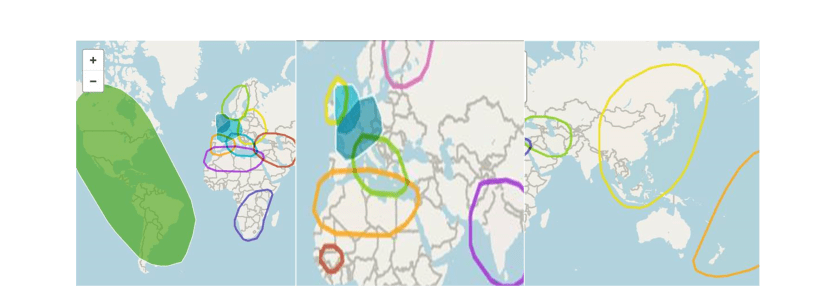 Genealogy of my maternal and paternal strands is pictured above. My brother Seth, sister Ciara and I took our DNA tests and found out our genetic make up is as shown in the photos above. Ethnically we are Western and Eastern European, Scandinavian, North African Berber, Senegalese/Central African, South African, Middle Eastern, South and East Asian, Latin, Indigenous to the Americas, and Polynesian.
Genealogy of my maternal and paternal strands is pictured above. My brother Seth, sister Ciara and I took our DNA tests and found out our genetic make up is as shown in the photos above. Ethnically we are Western and Eastern European, Scandinavian, North African Berber, Senegalese/Central African, South African, Middle Eastern, South and East Asian, Latin, Indigenous to the Americas, and Polynesian.






























 : the 2018
: the 2018