

 BRASIL/BRAZIL
BRASIL/BRAZIL
the LARGEST country in South America, and fifth largest country in the world…



COMMUNITY
Healthcare in Brazil is a constitutional right. It is provided by both private and government institutions. The Health Minister administers national health policy. Primary healthcare remains the responsibility of the federal government, elements of which (such as the operation of hospitals) are overseen by individual states. Public healthcare is provided to all Brazilian permanent residents and foreigners in Brazilian territory through the National Healthcare System, known as the Unified Health System (Portuguese: Sistema Único de Saúde, SUS). The SUS is universal and free for everyone.
Source: https://en.wikipedia.org/wiki/Healthcare_in_Brazil
Country/Brazil (Global Average – 11.1%) Rate: 9.2% Rank: 107
Kathy: I recently met a young mother of a late term preemie who shared a NICU experience that was intellectually, emotionally and financially challenging. Resources to guide her through this experience were few and far between. Current research indicates that even late preterm birth babies experience a variety of significant physical, neurological, medical and related challenges and needs. Although this group of preterm birth survivors may experience less complications than their micro-preemie brothers and sisters, late preterm birth preemies present unique needs/complications that we must continue to explore and understand. One issue that concerns me is the increase in non-emergency C-Section deliveries and the potential associated effects of this medical practice on our preterm birth community at large.

Brazil’s Women Are Pushing Back Against Rampant C-Sections
MOTHERBOARD – Marina Lopez – 12/07/16
Brazil has become a C-section capital of the world—a lucrative trend for doctors. But women are demanding the right to vaginal births.
Suzana Silva de Sousa was just three months pregnant when her doctor tried to schedule a cesarean section. De Sousa, 29, asked about a natural birth, but he pushed her towards the C-section surgery.
“I had a natural birth in mind, but I had no idea how hard it would be [to find a doctor],” de Sousa told me in Sao Paulo. “The easiest path was surgery, and that’s not normal,” she said.
De Sousa is one of thousands of Brazilian women fighting for greater access to natural births in what has become the C-section capital of the world. Here 80-90 percent of women in private hospitals, and 40 percent of women in public hospitals opt for the surgery, versus 32 percent in the United States and 9 percent in England. Compare that to the World Health Organization recommendation of 15 percent. The WHO warns that unnecessary C-sections can harm both the mother and baby. Not to mention they can rack up unnecessary health bills.
But that trend may finally be starting to change. Doulas and home births are becoming increasingly trendy and the Brazilian government has been pushing hospitals to increase their natural birth rates.
Despite a decreasing mortality rate, Brazil ranks alongside Congo and Nigeria as producing the largest number of premature babies in the world. The number of babies born prematurely in Brazil has nearly doubled over the last decade, to 11 percent of all births, according to a 2012 study by the World Health Organization. Researchers see a link between c-section rate and the rise in premature births.
In a country where women regularly undergo plastic surgery, C-sections have become a commonplace status symbol. Luxury hospitals offer everything from manicures to massages and happy hours following the surgery. But while many mothers have been taught to prefer C-sections, the health system does too. Doctors favor the procedure, which is more profitable and allows them to schedule back to back deliveries. Vaginal births cost on average $300 in Brazil, while C-sections can go for as much as $5,000, according to the Brazilian Medical Association.
Low-income mothers like de Sousa have even fewer options when it comes to delivery without surgery. In public hospitals, queues of women waiting to give birth can drive doctors to medically speed up deliveries and rush the process. The popularity of C-sections has also meant that fewer doctors have experience delivering children in any other way. Meanwhile, home births and doulas, increasingly popular options, are expensive and not covered by insurance.
So when de Sousa came across Casa Angela, a natural birth clinic on the outskirts of a favela in Sao Paulo, she knew it was the right place for her. The non-profit clinic, which caters to low-income women, emphasizes minimal interference from doctors. Each room comes equipped with bathtubs, yoga balls and monkey bars to help speed up delivery. The center also offers workshops on breastfeeding, prenatal yoga and welfare referral services.
“Low-income women going through a natural birth in a Brazilian hospital can be emotionally, culturally and physically isolated,” said Anke Riedel, a coordinator at the center. “They often have less self esteem and don’t know their rights when it comes to births.”
Casa Angela is the only clinic of its kind in Sao Paulo, a city of 20 million people. Its services proved so popular that Brazil’s upper class women showed up at the center a few years ago, asking to deliver their babies there as well. Today, half of the 400 women who deliver at Casa Angela every year are low-income and pay nothing for their deliveries. The rest pay on a sliding rate with prices up to $2000—the full cost of a birth for the clinic. The clinic is funded partially by the government and partially through private donations.
Brazil’s government has now decided to support this shift. It is trying to expand the number of women following de Sousa’s path. In an effort to curb what it called a “C-section epidemic” and prevent premature births, Brazil passed a law in June requiring women to sign consent forms acknowledging the risks of a C-section before going into surgery. The government also launched a partnership with 26 hospitals called to promote vaginal births. Since the start of the project one year ago, vaginal births increased by 76 percent and complications during birth in three of the hospitals fell by half. The project is now expanding to 150 hospitals around the country. But critics say outspoken mothers and government pressure hinder doctors’ abilities to use their expertise to decide what’s best for the patient.
“It puts the doctor in a difficult situation and interferes in the process of delivery,”said Dr. Gutemberg Fialho, president of the Medical Union of Brasilia. “The government wants us to push for natural birth, but what ends up happening is that if you avoid interfering until the last minute, it can lead to complications or even death for the baby.”
Last year a baby died in central Brazil because the mother insisted on a natural birth despite the doctor’s objections. Following the incident, a court ruled that doctors were responsible for deciding on the final birthing plan. “It reinforces a doctor’s autonomy. Even if the parents want a natural birth, the doctor is not bound by their decision,” the Governor Valadares Association, one of the country’s oldest doctor’s unions, said in a statement.
But more Brazilians are still starting to believe that women should have more control over how they give birth, even if it’s inconvenient for their doctors.
“This has really been a movement started by mothers,” said Jose Moacir, a doctor at the clinic. “Women are taking the issue into their own hands and demanding that doctors rethink their practice.”
Source: https://motherboard.vice.com/en_us/article/9a38g8/brazil-c-sections-natural-births
INNOVATIONS
Imaging technology, safer transport for critically ill preemies, modified CPAP/ventilators for Neonatal Rescues are innovations that will positively impact our community!

Early Life Research- Posted on Tuesday 27th June 2017
University of Nottingham
Best paper prize at 12th IEEE Conference on Automatic Face and Gesture Recognition
Researchers from the Division of Child Health, Obstetrics and Gynaecology and the School of Computer Science have won the Best Conference Paper at the prestigious 12th IEEE Conference on Automatic Face and Gesture Recognition (FG2017) in Washington DC.
Submitted papers were reviewed by over 250 experts to decide on the winner. The paper, presented orally by Dr Mercedes Torres-Torres, described the clinical trial, GestATion, undertaken in Nottingham aiming to use machine learning to estimate gestation age in newborn babies using still images of the babies foot, face and ear. The method could be used in low-middle income countries where antenatal care is poor and many babies are born prematurely with no record of this or unable to decide on the care they require.
Dr Don Sharkey, Associate Professor of Neonatal Medicine and chief investigator, Dr Caz Henry, Carole Ward (all from Academic Child Health) and Dr Michel Valstar (Lecturer in Computer Science) were also authors of the paper. The study was funded by the Bill and Melinda Gates Foundation.

Saving newborns with the NeoLife Ventilator, created by BYU alums and students
Centre for Healthcare Technologies: World first for premature newborn research-
Although neonatal intensive care has advanced hugely in recent years with many more premature babies surviving, very preterm babies are still at risk of developing disabilities or neurological conditions. Many premature babies need to be taken some distance for specialist treatment within a few hours of birth. In the UK there are currently more than 16,000 neonatal inter-hospital transfers which is on the increase.
In a few years, premature babies could benefit from new safer systems for transporting them between hospitals thanks to pioneering research underway in Nottingham.

Clinicians, scientists and engineers at The University of Nottingham have studied the effects of noise, vibration and stress on premature babies in order to develop a safer, better transport incubator for use during transfers between hospitals for specialist care.
The initial work, led by Associate Professor of Neonatal Medicine Dr Don Sharkey, has recently been published and provides the most detailed assessment of vibration exposure in newborn babies to date. Very premature babies who need to be transported between hospitals for life saving care are more likely to develop brain injury. This can lead to life-long disabilities and neurological conditions such as cerebral palsy. This type of brain injury is most likely to happen in the first few days of life when many of these babies are transferred. The team speculate that the significant vibration and noise the babies are exposed to could be a major contributing factor in the stress and brain injury observed.
Working with Professor Donal McNally, and others at the Centre for Healthcare Technologies, the team have also crash tested current newborn restraint systems used during the transport and believe they can be significantly improved.
The team are now undertaking a 3 year project to develop the next generation of neonatal transport system that aims to reduce the vibration and noise, whilst improving the comfort and safety, to reduce the stress for the baby and hopefully improve neurological outcomes.
The research is large collaborative effort with Industrial partners including ParAid Medical. The team has been awarded £872,000 by the NIHR to support this project, in addition to over £300,000 already awarded, and hope to have the new system available in 3-4 years that will improve the care of babies for years to come.
Source: http://www.healthcaretechnologies.ac.uk/news.aspx

HEALTH CARE PARTNERS
We are experiencing a global and local health care provider shortage. This shortage will increase over time, We are facing a health care shortage crisis. The Neonatal Womb/Preterm Birth community must support the development, retention, viability, and well-being of our health care partners. Globally, our Warriors themselves represent 11.1% of the global population. Our preterm birth family of parents, scientists, family members, friends, health care providers, scientists, researchers, innovators, financial support investors, teachers, funding sources, etc. touch the majority of our human population at large. We all need each other in order to survive, thrive, and live fulfilling lives with joy, in health and wellness.
New Research Shows Increasing Physician Shortages in Both Primary and Specialty Care
Wednesday, April 11, 2018
The United States could see a shortage of up to 120,000 physicians by 2030, impacting patient care across the nation, according to new data published today by the AAMC (Association of American Medical Colleges). The report, The Complexities of Physician Supply and Demand: Projections from 2016-2030, updates and aligns with estimates conducted in 2015, 2016, and 2017, and shows a projected shortage of between 42,600 and 121,300 physicians by the end of the next decade.
“This year’s analysis reinforces the serious threat posed by a real and significant doctor shortage,” said AAMC President and CEO Darrell G. Kirch, MD. “With the additional demand from a population that will not only continue to grow but also age considerably over the next 12 years, we must start training more doctors now to meet the needs of our patients in the future.”
The Life Science division of IHS Markit, a global information company, conducted this fourth annual study of physician supply and demand on behalf of the AAMC. The study modeled a wide range of health care and policy scenarios, such as payment and delivery reform, increased use of advanced practice nurses and physician assistants, and delays in physician retirements.
The report aggregates the shortages in four broad categories: primary care, medical specialties, surgical specialties, and other specialties. By 2030, the study estimates a shortfall of between 14,800 and 49,300 primary care physicians. At the same time, there will be a shortage in non-primary care specialties of between 33,800 and 72,700 physicians. These findings are consistent with previous reports and persist despite modeling that takes into account the use of other health professions and changes in care delivery.
As in prior projections, much of the increased demand comes from a growing, aging population. The U.S. population is estimated to grow by nearly 11%, with those over age 65 increasing by 50% by 2030. Additionally, the aging population will affect physician supply, since one-third of all currently active doctors will be older than 65 in the next decade. When these physicians decide to retire could have the greatest impact on supply.
This year’s report also repeated an analysis first conducted in 2017, which examined physician workforce demand if underserved populations had care utilization patterns similar to groups with fewer barriers to health care and physician access. According to the data, if people living in non-metropolitan areas and people without insurance used care the same way as insured individuals in metropolitan areas, the nation would have needed an additional 31,600 physicians in 2016, with nearly half of those needed in the South. If all Americans had utilization patterns similar to non-Hispanic white populations with insurance in metropolitan areas, the U.S. would need an additional 95,100 doctors immediately.
In addition to training more physicians, the AAMC believes that a multi-pronged approach is necessary to ease the physician shortage. Medical schools and teaching hospitals are educating future physicians in team-based, interprofessional care, developing innovative care delivery and payment models, and integrating cutting-edge technology and research into the patient care environment. The AAMC also supports legislation that would increase federal support for an additional 3,000 new residency positions each year over the next five years. These additional slots are crucial since every medical school graduate needs to complete training after medical school to practice independently.
In addition, the AAMC supports federal incentives and programs such as the National Health Service Corps, Public Service Loan Forgiveness, the Conrad 30 Waiver Program, and Title VII/VIII workforce development and diversity pipeline programs, all designed to recruit a diverse workforce and encourage physicians to enter shortage specialties and to practice in underserved communities.
“Medical schools and teaching hospitals are working to ensure that the supply of physicians is sufficient to meet demand and that those physicians are ready to practice in the health care system of future,” Kirch said. “To address the doctor shortage, medical schools have increased class sizes by nearly 30% since 2002. Now it’s time for Congress to do its part. Funding for residency training has been frozen since 1997 and without an increase in federal support, there simply won’t be enough doctors to provide the care Americans need.”
Source: https://news.aamc.org/press releases/article/workforce_report_shortage_04112018/

Limiting Resident Hours Ups Satisfaction, No Effect on Education
Veronica Hackethal, MD March 28, 2018
Residents with limited work hours report more satisfaction with their training and work–life balance than those with flexible hours and longer shifts, according to results from the Individualized Comparative Effectiveness of Models Optimizing Patient Safety and Resident Education (iCOMPARE) trial.
The study, published online March 20 in the New England Journal of Medicine, also shows that limiting residents’ work hours does not appear to affect educational outcomes. “Many educators have worried that the shift work created by limited duty hours will undermine the training and socialization of young physicians,” principal investigator David Asch, MD, from the University of Pennsylvania in Philadelphia, said in a press release. “Educating young physicians is critically important to health care, but it isn’t the only thing that matters. We didn’t find important differences in education outcomes, but we still await results about the sleep interns receive and the safety of patients under their care,” he added.
The issue goes back at least to 2003, when the Accreditation Council of Graduate Medical Education (ACGME) limited resident work hours to 30-hour shifts and 80-hour work weeks. In 2011, the ACGME further limited shifts to 16 hours for first-year residents (interns). Before these changes, resident hours were generally unrestricted. Ninety-plus hour work weeks and 36-hour shifts were often the norm. Program directors often justified these long hours by saying they contributed to continuity of care and helped train physicians to function successfully while sleep-deprived and under pressure.
Early evaluations showed that the restriction in work hours did not significantly affect patient outcomes. Yet program directors still reported that the quality of training and professional development of residents may be suffering. And they continued to voice concerns about the safety and quality of patient care. To find out what is really going on, researchers conducted a randomized trial at 63 internal medicine residency programs across the United States between July 2015 and June 2016.
They assigned 31 programs to standard work hours with limited work hours according to the 2011 ACGME policies: maximum 16-hour shifts for interns, maximum 28-hour shifts for more senior residents, at least 8 hours off between shifts, maximum 80-hour work weeks, and at least 1 day off every 7 days. The other 32 programs were assigned to use flexible work hours, with maximum 80-hour work weeks and 1 day off every 7 days, but no restrictions on shift length or mandatory time off between shifts.
For the current analysis, 23 trained observers followed the daily shifts of 80 interns (44 in flexible programs, 36 in standard programs) to evaluate activities and time spent in patient care vs education. The researchers also assessed medical knowledge by comparing scores on the American College of Physicians second-year in-training exam, and they surveyed trainees and program directors to assess their perceptions about satisfaction, education, burnout, work intensity, and continuity of care.
Results showed no significant differences in time spent on direct patient care for trainees in flexible programs (13.0%) vs standard programs (11.8%; P = .21). Residents in both types of programs also spent the same amount of time on education: 7.3 hours per shift for both (P > .99). Likewise, residents in flexible and standard programs had similar scores on in-training exams, even after adjusting for baseline scores that varied largely across programs (P < .001 for non-inferiority). In 2016, second-year residents in flexible programs had average scores of 68.9%, and those in standard programs had scores of 69.4%.
However, differences emerged when it came to satisfaction with work–life balance and education.Compared with interns in standard programs, those in flexible programs were almost 2.5 times more likely to report dissatisfaction with their overall well-being (odds ratio [OR], 2.47; 95% confidence interval [CI], 1.67 – 3.65) and were more than six times more likely to report dissatisfaction with how the program affects their personal lives with friends and family (OR, 6.11; 95% CI, 3.76 – 9.91). They also reported more than 1.5 times more dissatisfaction with the overall quality of education (OR, 1.67; 95% CI, 1.02 – 2.73). Yet both groups reported similarly high rates of burnout: 79% for flexible programs and 72% for standard programs.
In contrast, program directors of standard programs were more likely than those of flexible programs to report dissatisfaction with various aspects of training. For example, directors of standard programs reported more dissatisfaction with the quality and frequency of patient handoffs and the adequacy of bedside teaching, as well as the ability of interns to manage patients they admit and effectively perform their clinical duties.
“The takeaway is that interns were overall less satisfied with the flexible policies and the program directors were less satisfied with the standard approach,” senior author Judy Shea, PhD, from the University of Pennsylvania said in a press release. Principal investigator Asch added: “The residents are telling us something and program directors should listen carefully.”
Source: https://www.medscape.com/viewarticle/894509
Researchers Find Genes Linked to Preterm Birth
 By Robert Preidt, HealthDay Reporter
By Robert Preidt, HealthDay Reporter
WEDNESDAY, Sept. 6, 2017 (HealthDay News) — Researchers say they’ve pinpointed gene areas linked with preterm birth — and they said this could pave new ways to prevent the leading cause of death among children under age 5 worldwide.
The team looked at DNA and other data from more than 50,000 women from the United States and northern European countries. The researchers identified six gene regions that influence the length of pregnancy and the timing of birth.
“These are exciting findings that could play a key role in reducing newborn deaths and giving every child the chance to grow up smart and strong,” said Trevor Mundel, president of the Global Health Division at the Bill & Melinda Gates Foundation.

Taking Care of the NICU Graduate: A Team Approach
Bree Andrews, MD, MPH; Colleen Peyton, PT, DPT, PCS
- Pediatric Annals. 2018;47(4):e140-e141- Healio – Posted April 18, 2018
- There are three general types of neonatal intensive care unit (NICU) graduates with overlap in diagnosis and needs in infancy and early childhood: premature infants, infants with congenital malformations or anomalies requiring surgical and subspecialty follow up, and term infants with distress after birth.
- Most infants who stay in the NICU for more than 2 weeks require extensive follow-up care. These infants are often more medically complex and have increased risk of long-term neurodevelopmental impairments. Although NICU graduates are often medically managed by pediatricians in the community, a multidisciplinary approach can help to optimize neurodevelopmental trajectories. In this issue of Pediatric Annals, we are pleased to present the perspectives of professionals from various backgrounds, reflecting the multifaceted care that is often required in these high-risk NICU graduates.
- As clinicians, we are obliged to set the tempo throughout the NICU period regarding medical needs and clinical expectations at the time of discharge. We should also be mindful that parents will look to us for guidance about early childhood as well. Introductions to subspecialty teams and the interventions that take place in the NICU are crucial to long-term comfort and ease of the parents facing a different experience from some families after the birth of a child. A methodical approach to discharging an infant from the NICU can aid families and their physicians considerably in the months and years to come.
- In the case of the preterm infant, a pathway to discharge in the arenas of breathing, temperature control, feeding, and sleep should be explained as the child matures. Parents should be informed that growth and development of NICU graduates are typically “adjusted” back to take account of their prematurity. Parents should be provided with resources to understand medical problems, developmental milestones, feeding guidelines, overall safety, and specialized processes for making sure premature infants thrive after discharge.
- In the first article, “Follow-Up Care for High-Risk Preterm Infants,” Dr. Stephannie M. B. Voller overviews the medical issues and developmental concerns that a pediatrician should consider when caring for a high-risk preterm infant. In the second article, “Common Queries About Immunizations in Preterm Infants,” Dr. Ansul Asad provides answers to commonly asked questions about immunizations specific to infants born preterm. Next, Taylor Peters and Cecelia Pompeii-Wolfe in their article, “Nutrition Considerations After NICU Discharge,” highlight the nutritional concerns and provide feeding resources for clinicians and families of preterm infants.
- For children with congenital anomalies, especially where surgical intervention is needed, families can be taught about overarching clinical or genetic conditions while surgical procedures and planning ensue. Many centers have multidisciplinary groups for unique diagnoses such as cleft lip and palate, Prader-Willi syndrome, hyperinsulinism, neural tube defects, and others. Many conditions have support groups online for parents to unite and find novel evaluations or treatments.
- Infants facing distress after birth are unique and often need tertiary care. The most common reasons for a term infant to need NICU care are infection, respiratory distress, perinatal depression, and seizures. These conditions often require a set of interventions unique to the infant’s presentation. Although many patients will have short treatment courses for these illnesses, some will be protracted after long-term ventilation or extracorporeal membrane oxygenation.
- As patients in the NICU become more stable and approach graduation, the NICU team should build on the inpatient processes for outpatient care and care coordination. The specialized processes can include the use of durable medical equipment and specialized pharmacies for supplies and medications, respectively.
- Each medical problem should be detailed with the parents of NICU graduates; the importance of follow-up care should be emphasized, with the intent of having an ongoing discussion that imprints the parents with the education and capacity to seek that follow-up care. NICU graduates, including those with congenital anomalies, who are in distress after term birth or those born preterm are all at risk of having adverse neurodevelopmental outcome. In the article, “General Movements: A Behavioral Biomarker of Later Motor and Cognitive Dysfunction in NICU Graduates,” Drs. Colleen Peyton and Christa Einspieler provide an overview of a clinical tool that can be used in infants younger than age 5 months to predict neurodevelopmental outcome in high-risk infants. In the final article, “NICU Graduates: The Role of the Allied Health Team in Follow-Up,” Dr. Jane L. Orton and colleagues offer a comprehensive overview about the role of the allied health team in the care of infants at-risk or with known developmental issues.
- This issue is dedicated to exploring mechanisms of enhancing clinician and parent capacity to care for these patients after NICU discharge. Graduations come with hopes and dreams, but also concerns and uncertainties.
Source: https://doi.org/10.3928/19382359-20180320-03

PREEMIE FAMILY PARTNERS
Dads are more stressed than moms after bringing preemies home
Chicago Tribune Sunday May 06, 2018
Baby Ava weighed 2 pounds, 15 ounces when she was born 10 weeks early after her mother had preeclampsia. When she was born in 2014, she didn’t move or cry initially. Ava’s skin was too sensitive for clothing, her parents couldn’t hold her, and she was connected to all kinds of wires and monitors. After a five-week stay in the neonatal intensive care unit, where each day was a struggle, the Illinois couple got to bring their baby home — but after getting accustomed to having help from monitors, they knew the transition wouldn’t be easy.
“She wouldn’t be connected to monitors to tell us if she’s still breathing; we won’t have nurses constantly monitoring her,” said Ava’s dad, Irwin Obispo, a pharmacist manager at a local retail pharmacy. “The stress of having to take care of a preemie with all the extra monitoring and attention to care is highly overwhelming.”
There also was sleep loss paired with a day job and worries about his wife, plus the knowledge that the family had narrowly slipped through some very dangerous territory at the hospital. “I may have physically endured pain, but the emotional and mental pain of possibly losing his family is equally as hard,” said Michelle Obispo about her husband.
Contrary to popular belief, it’s the fathers whose stress levels rise when bringing premature NICU babies home from the hospital — while the mothers’ stress levels stay constant, according to a new study by researchers at Northwestern Medicine.
They found that before being discharged from the NICU, both parents had high levels of cortisol, the stress hormone. But during the two weeks after being discharged, the mothers’ stress levels returned to normal, while the fathers’ continued to rise. When the babies are in the hospital, they’re cared for by a team of nurses and physicians, said Craig Garfield, lead author of the study, and associate professor of pediatrics and medical social sciences at Northwestern University.
“When the baby comes home, suddenly baby needs care and support, mom needs care and support, and dad may still be trying to juggle work and his growing home responsibilities,” said Garfield, who also is an attending physician at Lurie Children’s Hospital. Mothers also tend to process the situation long before fathers do, which may account for their being able to adjust faster, said AnnaMarie Rodney, owner of Chicago Family Douglas. As soon as a woman gets pregnant, she begins to plan for her baby, while many men might not do as much until the baby is born.
“I talk to five to 10 moms a day, and the things I hear from them are that when they’re pregnant, their husbands don’t think their lives are going to change,” Rodney said. “When dads realize, ‘I’m a dad,’ — this changes everything — but now, if anything isn’t perfect, it’s an additional stress, and they really don’t know what to do with it.”
If the baby goes directly to the NICU, many fathers continue to feel powerless, said Jennifer Howard, a licensed professional counselor in Virginia who specializes in the treatment of perinatal mental health and is the mother of a preemie. In there, the machines, nurses and doctors take over, as the parents watch.
“When your baby is discharged from the NICU, it can feel quite overwhelming to transition to a position where you are now in charge,” Howard said. “This transition likely heightens dad’s feelings of insecurity about their ability to care for their baby.” The partners also are faced with a unique role, as they’re supposed to be the strong ones in this situation since they didn’t give birth, so they have to care for the mother and the baby. And while postpartum depression is a much-publicized medical problem facing mothers, men’s stress and postpartum issues haven’t been studied much until now.
“It’s largely misunderstood, but fathers also experience perinatal mood and anxiety disorders,” Howard said.About 1 in 7 women will experience postpartum depression, and 1 in 10 men will also experience it. An NICU stay is one of the factors related to postpartum depression, and it could affect men and women, Howard said. Fathers often are the first to see their preemies or sick children in the NICU because the mother is still in the recovery room. Fathers also watch emergency C-sections, and they are there during the crisis, while the mother may be under anesthesia or may not be as aware of what’s happening.
“If the birth was traumatic — for instance, if the baby was resuscitated — then dads may be exposed and more aware of the baby’s health concerns,” Howard said. “This can lead dads to experience symptoms of PTSD, as well.” But postpartum depression and stress symptoms after childbirth typically manifest differently in dads than in moms. Men will often be angry, irritable, will be more likely to abuse alcohol or other substances, and will withdraw and be alone, said Crystal Clancy, executive director of community engagement at Pregnancy & Postpartum Support Minnesota.They should seek professional help immediately, as they need to be healthy to properly care for their infant.
Source:http://www.chicagotribune.com/lifestyles/health/sc-fam-dads-stress-preemie-0213-story.html

EurekAlert! is an online, global news service operated by AAAS, the science society
Public Release: 5-May-2018 – Pediatric Academic Societies
Majority of late preterm infants suffer from morbidities resulting in hospital stay
Physiological immaturity plays an important role in producing poorer outcomes
TORONTO, May 5, 2018 – A new study found the majority of late preterm infants (LPTs) suffer from morbidities resulting in hospital stay. Although factors that result in LPT births do contribute to morbidity, physiological immaturity plays an important role in producing poorer outcomes. The research will be presented during the Pediatric Academic Societies (PAS) 2018 Meeting in Toronto.
LPTs constitute 70 percent of the preterm population. Common neonatal morbidities are higher in this group compared to term infants. Although this increased risk is attributed to physiological immaturity, recent studies indicate that immaturity itself may not be the sole cause of morbidity as all premature infants experience this risk, but suffer different outcomes. Some studies demonstrate that the risk of morbidities is determined by the causes of preterm delivery with immaturity acting as modulator. The relative contribution of these factors is unclear. The objective of this study was to assess the role of indications of delivery in LPT in determination of common neonatal morbidities that result in hospital stay.
The study was conducted as a retrospective cohort study of LPTs born in a single tertiary care centre between April 2014 and February 2016. Researchers categorized indications of birth as threatened preterm labor (TPTL), preterm premature rupture of membrane (PPROM) and medically indicated deliveries, which included maternal and fetal pathologies. Risk of hypoglycemia, hyperbilirubinemia, use of CPAP, and apnea of prematurity in LPT were estimated by calculating unadjusted and adjusted for gestational age risk ratios using multiple regression analysis with PPROM as a reference category.
PPROM was responsible for 38.4 percent of deliveries, TPTL in 22.8 percent, and 39.1 percent were delivered due to various obstetric and fetal indications with pre-eclampsia and intrauterine growth restriction being the most common reason for medically indicated preterm deliveries. All morbidities were significant across gestational age, with increased risk with decreased gestational age, except hypoglycemia where the incident was highest at 36 weeks (66.7 percent), versus 28.5 percent at 35 weeks, and 22.7 percent at 34 weeks (p value=0.039).
Dr. Melissa Lorenzo will present the abstract, “Morbidity Risk Among Late Term Preterm Infants: Immaturity vs Indication of Delivery,” during the PAS 2018 Meeting on Tuesday, May 8 at 7:30 a.m. EDT.
Source: https://www.eurekalert.org/pub_releases/2018-05/pas-mol042618.php#.Wu600dAn3c0.email
WARRIORS:
As announced ![]() in our last Blog, moving forward I (Kat) will be sharing my preterm birth survivor story through our Writing-for- Wellness experience. I feel deeply connected to each and every one of you in my heart and soul. I have always considered myself a Global citizen. My genealogy tells me a story about the history of my body – a Global composition of DNA that looks like this:
in our last Blog, moving forward I (Kat) will be sharing my preterm birth survivor story through our Writing-for- Wellness experience. I feel deeply connected to each and every one of you in my heart and soul. I have always considered myself a Global citizen. My genealogy tells me a story about the history of my body – a Global composition of DNA that looks like this:
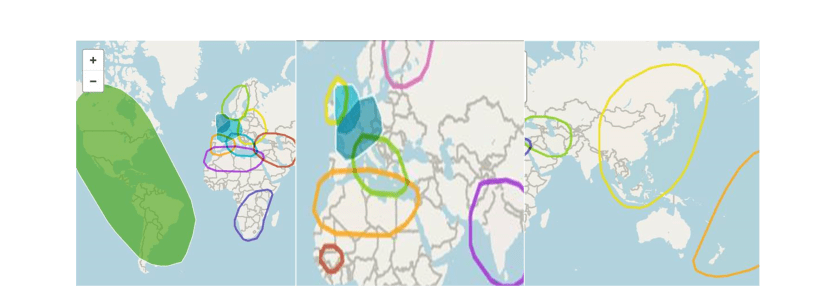 Genealogy of my maternal and paternal strands is pictured above. My brother Seth, sister Ciara and I took our DNA tests and found out our genetic make up is as shown in the photos above. Ethnically we are Western and Eastern European, Scandinavian, North African Berber, Senegalese/Central African, South African, Middle Eastern, South and East Asian, Latin, Indigenous to the Americas, and Polynesian.
Genealogy of my maternal and paternal strands is pictured above. My brother Seth, sister Ciara and I took our DNA tests and found out our genetic make up is as shown in the photos above. Ethnically we are Western and Eastern European, Scandinavian, North African Berber, Senegalese/Central African, South African, Middle Eastern, South and East Asian, Latin, Indigenous to the Americas, and Polynesian.
Hello World!
HUFFPOST SPORTS – 04/30/2018 – By Mary Papenfuss
Cowabunga! Brazilian Rodrigo Koxa Breaks World Record Surfing 80-Foot Wave 
“I got a present from God,” the gutsy surfer said at a World Surf League ceremony.
Brazilian Rodrigo Koxa has broken a world record by riding the biggest wave ever surfed, according to the World Surf League.
Koxa mastered the monster 80-footer off the coast of Nazaré, Portugal, in November. His record-breaking feat only became official Saturday, when it was recognized with the Quiksilver XXL Biggest Wave Award at a World Surf League ceremony in Los Angeles.
“The award goes to the surfer who, by any means available, catches the biggest wave of the year,” the league said in a statement. “Not only did Koxa win this year’s honor, but he now holds the Guinness World Record for the biggest wave surfed.”

