


Kuwait, officially the State of Kuwait, is a country in West Asia and the geopolitical region known as the Middle East. It is situated in the northern edge of the Arabian Peninsula at the tip of the Persian Gulf, bordering Iraq to the north and Saudi Arabia to the south. With a coastline of approximately 500 km (311 mi), Kuwait also shares a maritime border with Iran, across the Persian Gulf. Most of the country’s population reside in the urban agglomeration of Kuwait City, the capital and largest city. As of 2024, Kuwait has a population of 4.82 million, of which 1.53 million are Kuwaiti citizens while the remaining 3.29 million are foreign nationals from over 100 countries. Kuwait has the third largest foreign-born population in the world.
Like most other Arab states of the Persian Gulf, Kuwait is an emirate; the emir is the head of state and the ruling Al Sabah family dominates the country’s political system. Kuwait’s official state religion is Islam, specifically the Maliki school of Sunni Islam. Kuwait is a high-income economy, backed by the world’s sixth largest oil reserves.
Kuwait has a state-funded healthcare system, which provides treatment without charge to holders of a Kuwaiti passport. A public insurance scheme exists to provide healthcare to non-citizens. Private healthcare providers also run medical facilities in the country, available to members of their insurance schemes. As part of Kuwait Vision 2035, many new hospitals have opened.
Source: https://en.wikipedia.org/wiki/Kuwait
- GLOBAL PRETERM BIRTH RATES – Kuwait
- Estimated # of preterm births: 9.3 per 100 live births/Global Average: 10.6
- Source- WHO Preterm Birth Rate (Per 100 Live Births)
- WHO Prematurity
- World Population Review
- WHO Country Consultation of Low and Preterm Birth Weight

COMMUNITY

Antenatal Depression and its Associated Factors: Findings From Kuwait Birth Cohort Study
Published 15April 2024

Reem Al-Sabah, Abdullah Al-Taiar, Ali H. Ziyab, Saeed Akhtar & Majeda S. Hammoud
Abstract
Background
Pregnant and postpartum women are at high risk of depression due to hormonal and biological changes. Antenatal depression is understudied compared to postpartum depression and its predictors remain highly controversial.
Aim
To estimate the prevalence of depressive symptoms during pregnancy and investigate factors associated with this condition including vitamin D, folate and Vitamin B12 among participants in the Kuwait Birth Study.
Methods
Data collection occurred as part of the Kuwait Birth Cohort Study in which pregnant women were recruited in the second and third trimester during antenatal care visits. Data on antenatal depression were collected using the Edinburgh Postnatal Depression Scale (EPDS), considering a score of ≥ 13 as an indicator of depression. Logistic regression was used to investigate factors associated with depressive symptoms in pregnant women.
Results
Of 1108 participants in the Kuwait Birth Cohort study, 1070(96.6%) completed the EPDS. The prevalence of depressive symptoms was 21.03%(95%CI:18.62–23.59%) and 17.85%(95%CI:15.60-20.28%) as indicated by an EPDS ≥ 13 and EPDS ≥ 14 respectively. In the multivariable analysis, passive smoking at home, experiencing stressful life events during pregnancy, and a lower level of vitamin B12 were identified as predisposing factors. Conversely, having desire for the pregnancy and consumption of fruits and vegetables were inversely associated with depressive symptoms.
Conclusion
Approximately, one fifth of pregnant women had depressive symptoms indicating the need to implement screening program for depression in pregnant women, a measure not systematically implemented in Kuwait. Specifically, screening efforts should focus on pregnant women with unintended pregnancies, exposure to passive smoking at home, and recent stressful live events.
Source: https://link.springer.com/article/10.1007/s44197-024-00223-7

WHO compendium of innovative health technologies for low-resource settings 2024
18 July 2024
| Technical document

Overview
Access to appropriate, affordable, effective, and safe health technologies is paramount, especially in low-resource settings, where burden of non-communicable diseases adds on to the infectious diseases.
NCDs account for a staggering 74% of global deaths, with 86% of premature fatalities occurring in resource-constrained regions. Cardiovascular diseases, cancers, chronic respiratory conditions, and diabetes collectively contribute to over 80% of these premature NCD-related deaths. Addressing this challenge requires targeted interventions and innovative solutions tailored to LMICs.
The 2024 Compendium of Innovative Health Technologies for low-resource settings includes commercially available solutions and prototypes. This 7th edition showcases 21 technologies, each with a full assessment. It also includes updates for technologies previously featured in previous compendia editions. Assessments include clinical aspects, relation to WHO technical specifications, regulatory compliance, criteria on health technology assessment and health technology management, local production viability, and intellectual property considerations.
Beyond presenting these innovations, the Compendium serves as a catalyst for increased interaction among stakeholders—ministries of health, procurement officers, donors, developers, biomedical engineers, clinicians, and users. By providing evidence-based assessments and relevant information, it aims to drive use of innovative health technology and expand global access, particularly for low-resource settings for populations in need.
WHO Team
Access to Assistive Technology and Medical Devices (ATM), Access to Medicines and Health Products (MHP), Health Product Policy and Standards (HPS), Medical Devices and Diagnostics (MDD)
Editors World Health Organization ISBN: 978-92-4-009521-2
Source:https://www.who.int/publications/i/item/9789240095212

Humood AlKhudher
Humood – Kun Anta | حمود الخضر – كن أنت | Official Music Video
Humood Othman AlKhudher, commonly known as Humood Alkhudher, is a Kuwaiti singer and music producer.
* English Translation https://youtu.be/9JPaGW21Rzg


Navigating toward Neonatology: Interview with Doctor Andrew Hopper
Benjamin Hopkins, DO, Andrew Hopper, MD

Welcome back to another installment. My name is Benjamin Hopkins, and I am currently a post-grad year one pediatric resident at the University of California, San Francisco–Fresno. When ‘I grow up,’ I want to be a Neonatologist. Look at previous months’ journals for my earlier articles and follow along with this column as I navigate my way to becoming a neonatologist.
I am just over halfway done with my residency intern year. I have recently completed a rotation through inpatient wards, getting to see a variety of ages and patient presentations, along with consults to other specialties helping care for pediatric patients. I have been privileged to work closely with my fellow residents and supervising attendings who tailor their care for each patient they see.
This month, I had the privilege to talk with Dr. Andy Hopper, Chair of the LLU School of Medicine Promotions Committee and professor of pediatrics and neonatologist at Loma Linda University. We discussed the characteristics of an outstanding neonatologist, how he became a neonatologist, what a resident should prioritize, and some of his current interests and research.
What qualities are most essential to excel as a neonatologist?
First, you’ve got to like working with babies and the excitement of thinking about and caring for a young patient who has their entire life in front of them. Your interaction with them will allow them to achieve health so they can have that life in front of them. That’s always the prime directive for me when I’m looking to look after a baby. Can we get these kids through whatever problem they’re having so they can go home and live their best life? You have to have a passion for the patient population that you’re going to serve.
That goes for any specialty, but especially for the specialties that are critical care, where it takes more of an emotional burden from time to time and with the care and investment you have towards that patient population when there is, you know, loss or things don’t go the way we want them to and just making sure like we have support and things like that for those areas.
You’re also the doctor to the parents. Most parents, when they landed in the NICU, never planned for this to be the outcome. They’re immediately thrown into this rather harsh environment of bells, whistles, monitors, and people doing things that they’re not sure what they’re doing for their child, but it’s pretty scary. As the neonatologist, this is one of the areas that you have to work with them, and you’re educating them. We’re also trying to give them peace, and you’ll help them get through this. It is a team effort in our specialty, but the physician and the parents have to collaborate to make it work.
We have two daughters, and when I was a pediatric resident, my first daughter was born at 33 weeks. I don’t think we were particularly freaking out about that, but she was preterm. Then, my younger daughter was born when I was in my neonatology fellowship at Stanford. She was 27 weeks, and back in 1982, the year she was born, 28 weeks was considered the limit of viability; they’re different now, and the numbers have come down dramatically. However, I remember my faculty members saying that if she is not too aggressive, we may not want to go all out to resuscitate her because they were thinking the worst. Fortunately, she came out, and she was vigorous. Four hours out, she reached up and pulled her ET tube out; the rest is history.
Another beneficial quality in intensive care is when you’re looking at things to map out what you think will happen in the next 12 to 24 hours; what’s the worst-case scenario, and am I ready to deal with that? When they don’t happen, you’re thrilled, but when they do happen, you’re not caught off guard. I was the director of the ECMO program at Loma Linda for 10 years, and it was always determining who we would put on ECMO and when to do it. That’s where you have to sit down and map out what would be the things that would make me push towards putting this kid on ECMO. It’s an approach that uses differential and critical thinking so that you can be proactive rather than reactive. It’s not a good idea to be catching up with a kid in a code where you thought four hours ago we should have picked up on this, and we could have prevented this.
An excellent bedside nurse will make your night much better because you trust their assessment; I’ve had nurses call me and say, “I was here yesterday. I can’t put my finger on it today, but something’s not right with this kid.” That’s all I need to hear because then I will look carefully to say, what’s different? Is it a heart rate change since the kid has early onset sepsis, or is this a baby with a cardiac lesion that’s ductal dependent, and maybe the duct is closing? Very few things are crash-and-burn type things, but you need to be ready to recognize when those things are happening to connect on that.
When I was in training, we had fewer options; now, there are five or six different kinds of mechanical ventilation, and you use them for various reasons. When I was in training, you either mechanically ventilated them with a pressure-limited time cycle ventilator or didn’t. Those were the times when faculty were home at night, and you were there on the front lines. Part of that, I’m not saying it was always a good thing, but you were the person who had to make those decisions at 2 a.m.; there wasn’t anybody else around.
I remember, as a first-year fellow at Stanford, when I would call the attending and say, “I’ve got this sick kid with meconium aspiration and pulmonary hypertension; these are the things I’m doing. This is what I’m thinking about.” I remember the attending said, “Wow, that kid sounds sick. Good luck. I’ll see you tomorrow.” Then you think, “You know what, this is on me.” They don’t do that anymore, and I’m not saying that was a good role model of the time; it was just different in those days.
What caused you to pursue a career in neonatology?
I can tell you precisely what happened when I was doing my pediatric rotation as a third-year medical student, and I was assigned to a NICU. I went to the University of Texas in San Antonio, and we were down at a county hospital. The intern became ill and was off. The senior resident and attending said, “Okay, you’re a third year medical student; you’re now the intern.” I got promoted very quickly, which was scary, but it was also exciting to be given that responsibility. I had a lot of guidance; that wasn’t something I just did, but I enjoyed the mix of doing procedures, putting in lines, being able to intubate, and putting in chest tubes. Plus, you’re the doctor, the whole doctor, not just the orthopedist or the hematologist. You’re the doctor, covering everything for this unique population. I wouldn’t do well in a clinic setting because I like the adrenaline rush of helping a kid when you don’t know which way things are going. I like the excitement of inpatient medicine and the ability to be that detective to figure out the most likely thing that’s going on. I did my neonatal training at Stanford, but then I was in a quandary about whether I wanted to do PICU. I had the option of going to CHOP, but the way they did their PICU training was they had you go through anesthesia training and then, on top of that, to PICU. After three years of residency and neonatology, my family asked if I was serious about another five or six years. I then ended up going to UCSF to do an additional year there in the old hospital in Parnassus, where we had a Peds ICU on the sixth floor, and we had cardiac and post-cardiac recovery.
As the PICU fellow, the cardiac surgeon would come in, do an extensive surgery, and it’s five o’clock, and he’s telling you about all the horrible things that could happen after the surgery, and then, his parting words are, “don’t let this kid die.” That was before we had good monitoring or many medications. We had isoproterenol and epinephrine, and it was a juggling act, where you were at the bedside all night trying to keep this kid in bounds so that the following day, you could sign out to the next person; the whole mindset was to keep him alive till 8.05. There was much fear back then; it’s much better now, but it was through fear and intimidation for some of those encounters.
What do you now know that you wish you knew before going into neonatology?
That’s a good question; if I replayed my career, I was focused on clinical stuff. When I was a fellow at Stanford, we had a rotation where you were on service for an entire month, morning and night, seven days a week; you would rely on your colleagues to support you. I would have liked to have had an opportunity to focus on research and academics for a year after the clinical training. If I could replay what I did again now, I would have taken that extra year in pulmonology or neurology because those are the things I’m passionate about. You learn on the job; at the time, I didn’t think I could put my family through that. It’s not always apparent that that’s something I could have done. But if I could replay that, I would have tried to do an extra year or two. Many people now have MD/PhD degrees, which is fine. I didn’t need a PhD, but an additional year of training in working with people would have been a way to solidify a more substantial research career for me.
What are you currently working on? I’m working part-time now and fill in when people need help. We have a fellowship program, and I have three fellows I mentor and help with their SOC projects required for fellowship. I miss bedside teaching, but I give lectures and didactics for fellows. We have a couple of new faculty members that I’m also trying to work with, and I am trying to educate our nurses because you need to have excellent nurses. That’s what makes a unit good: good nurses and RTs. It was much different then, but one of the reasons you could survive a crazy month of fellowship was because you had RTs that were on to help you, and they were very professional in what they were doing. Fostering teamwork and education is something I still enjoy.
I am still particularly energized when I go to a good research meeting. It excites you; I’m jealous of guys like you who are beginning their careers because I can only imagine what new neonatology will be like in 10 years. You’ll also have all kinds of genetic capabilities to make diagnoses and genetic-based treatments. Neonatology is a relatively new field with new treatments. My career has been almost 40 years, and when I started, we didn’t have surfactants or artificial surfactants. We barely had TPN, which was adult TPN watered down for babies. We didn’t have nitric oxide treatment or neonatal ECMO. All these things resulted from people doing research and wanting to improve the outcome of kids.
Even in a unit like Kaiser, the way that they do their research may be less of a bench-top approach, but they do some incredible QI work that helps develop protocols. We have a small baby unit with extremely preterm kids, and everything is driven by protocol. However, the idea is that you’re constantly refining and evaluating those protocols to see if they’re the best. You’re analyzing, making changes, and evaluating the changes to see if that makes things better. It is a good way to do medicine in general, and neonatology thrives on that approach.
What would you encourage a future neonatologist to prioritize and be involved in? I
t’s a little different now; people come into the fellowship, and they have been doing neonatal electives, and that is to their advantage is to have a little bit of familiarity with neonatology so you’re not going to freak out. We have a massive unit with high acuity, which can be overwhelming for somebody with no neonatal background before the pediatric residency program. I’m not saying it’s right or not, but residents in pediatrics used to have six months of neonatology. Now that’s been watered down by the ACGME, you only have three months. You’re coming into a fellowship with a significantly different background than we did before. You’ll learn to be an outstanding neonatologist.
What you want to do now is take advantage of some ancillary subspecialties like cardiology. I would also consider doing a PICU elective because many of these babies will graduate and go to the PICU. We have babies in our unit in Loma Linda that are seven or eight months old. They’re no longer neonates, so having that experience is beneficial. Neurology is another area where there’s so much of it in neonatology that a good neurology background, teaming up with a neonatal neurologist who cares about those babies, can show you how to do an appropriate, careful physical and neurologic exam. Take advantage of that stuff because you don’t get a chance to do that later on.
Having been in this field for this long, I have a couple of things I did that I have enjoyed: working at Loma Linda and the friendships of my colleagues—I value what they do. They’re good people, and our group is collegial. It’s stressful, so the ability to work with people who care for you makes a big difference. You may not be close buddies with them all, but they respect you, and you respect them. An example is if you were sick and you couldn’t do your call, I can tell you my experience has been if I call in and say, “Hey, you know, I’m sick this evening. Can anybody take my call?” Usually, within 10 minutes, somebody says, “Yeah, I’ll do your call.” That kind of support makes a big difference; people have your back, which is nice; generally, it’s a great specialty.

PREEMIE FAMILY PARTNERS

Developmental Care

The majority of babies born prematurely do well and develop normally, however, the risk of developmental problems is considerably higher than in the rest of the population and the risk increases proportionately with the degree of prematurity. About half of the infants born preterm (before 28 weeks) will require some form of specialist help when they start school: for those born between 28 and 32 weeks this figure decreases to 30%. The range of problems is wide and they often overlap or present in clusters so that a child may have a complex developmental profile.
Problems include:
- Altered pain perception
- Anxiety and Depression
- Attachment disorders
- Attention deficit disorder
- Autism
- Behavioural problems
- Cerebral Palsy
- Cognitive deficits
- Co-ordination disorders
- Executive Functions
- Feeding problems
- Hearing loss
- Hyperactivity (related to attention deficit)
- Language delay
- Memory
- Perceptual motor problems
- Sensory Processing
- Social isolation
- Specific learning deficits (e.g maths)
- Timidity/withdrawal
- Visual deficits
Developmental care improves the potential of infants who are disadvantaged by premature birth or adverse perinatal events by supplementing and humanizing high tech medical care.
In many units the focus of developmental care is Family Centered Care (FCC). In FCC units the importance of the family as the most significant influence on the infant’s well being and development is underlined and parents and healthcare professionals work in partnership, with open communication. FCC places the infant firmly in the context of the family, acknowledging that the family is the most constant influence on an infant’s development. Adjusting to parenting in the NICU following a traumatic birth experience or pre-term delivery can be difficult. Assisting mothers and fathers adapt to their parenting roles in the NICU is part of developmental care. FCC is sensitive to the nature of personal, social and cultural influences upon each family.
Another view of developmental care focuses on the NICU environment, particularly in adapting the physical environment to provide appropriate sensory stimulation, to protect the baby from stress and to promote sleep. The immature central nervous system of the neonate is in a critical period of rapid growth and increasing specialization, all designed to take place in quite a different settling e.g. the mothers womb. The NICU is not the optimal sensory environment for preterm and newborn development. The infants’ behavioural cues are the best guide to whether or not the environment (sensory, temporal and social) is conducive to the current development needs of the infant and the environment needs to be organized in such a way to meet the infant’s developmental expectations.
Individualised developmental care is care that is responsive to the ever changing needs of the infant. Behavioural cues help us understand the infant’s competency, strengths, sensitivity, vulnerability and developmental goals. The leading mode of individualized developmental care is the NIDCAP- Newborn Individualised Developmental Care and Assessment Programme. Many of the NICUs in Ireland have NIDCAP trained professionals. To learn more about NIDCAP visit www.nidcap.org.
MEETING THE NEEDS OF THE NEONATE
Physiological stability is important for brain development. The way that the NICU environment, light and noise, the timing of events, handling and positioning can have a positive or negative effect on heart beat, respiratory pattern, oxygenation, intracranial pressure, temperature and oxygen consumption.
Minimising the pain and stress of the neonate because of the long term impact on behaviour and sensory processing is an important aspect of developmental care. Many benign routine aspects of neonatal care such as nappy change and bathing can be stressful for the premature infant and developmental care ensures that such procedures are adapted to minimize distress to the infant.
Protecting Sleep. REM or active sleep is associated with brain development whilst quiet sleep is associated with growth. Sleep protection relies on the caregiver’s ability to distinguish different states of arousal.
Enhanced nutrition. Developmental care can support nutrition by helping the infant to conserve energy and to digest food in addition to providing effective support for breast feeding.
Appropriate sensory experience. Certain kinds of stimulation are required to trigger normal development whilst inappropriate stimulation that is out of phase with developmental brain expectation can result in some systems failing to develop. By observing the infants behaviour the caregiver can learn which sensory stimulations are appropriate.
Parenting and attachment. Parenting style has a significant impact on development and learning how their infant communicates is an integral component of developmental care for families. The high tech environment of the NICU can have an adverse impact upon attachment. Developmental care facilitates this attachment process and allows the parent/infant relationship to develop, supports the parents as they get to know their infant and grows their confidence as primary caregivers.
Protecting postural development. Development care can protect infants from the acquired postural deformities that can result from long periods of lying flat on a bed (e.g flat head syndrome), retracted shoulders (e.g.arms held in the W position), legs abducted and externally rotated (e.g. frog leg position), and torticollis. Adequate positioning support combined with frequent position changes can counteract these deformities which can otherwise delay the acquisition of skills such as sitting and walking, self comforting, feeding and fine motor co-ordination.
EXAMPLES OF DEFENSIVE/AVOIDANCE BEHAVIOUR IN THE NEONATE
Agitation Arching Bracing position of legs Colour changes Coughing Crying Diffuse states Eye floating Finger splay Fussing Glazed look
Grimmacing Hiccoughs High guard hands Jerky movement Limp or stiff posture Looking away Mouth hanging open Pauses in breathing Positioning Salute Sighing
Sneezing Staring Sudden movement Straining Squirming Tongue thrusting Tremulousness Twitching Whimpering Yawning
EXAMPLES OF COPING/APPROACH BEHAVIOUR IN THE NEONATE
Easily consoled Frowning Grasping Healthy Colour Holding on Hands to mouth
Hands clasped together
Moving hand to face
One foot clasping the other
Orientation to voice or sound
Perky attentive expression
Relaxed open face
Responsive smiling Restful sleep Smooth movements Soft flexed position Settles self Snuggling when held
SENSORY DEVELOPMENT
The senses mature in the following order:
- Touch
- Vestibular (response to movement in space)
- Chemosensory (taste and smell)
- Hearing
- Vision
TOUCH
Different kinds of touch activate different sensory receptors in the skin. Light, feathery touching can be arousing and preterm infants may react irritably. Gentle deep pressure touch is more soothing for the infant. Infants may seek comfort through tactile self-regulatory strategies such as grasping and bracing. Boundaries (nesting) , wrapping and cradling the feet, head or body with still hands have an organizing input.
VESTIBULAR
The vestibular apparatus located in the inner ear responds to movement through space and the effects of gravity. Vestibular input is thought to promote maturation of the other systems.
The movement experienced by infants in the NICU is often sudden and unpredictable and their fragile vestibular systems can become easily overloaded. It is important that infants are prepared for position changes by providing adequate support and moving slowly and gently.
TASTE AND SMELL
The infant is exposed to many noxious smells in the NICU. Staff should minimize unpleasant olfactory experiences e.g alcohol wipes, plaster removers, strong perfume, strong hand creams etc, deliver medications separately from milk, and facilitate positive olfactory experiences by encouraging close contact with parents.
Taste may be affected by intrusive oral experience e.g. prolonged use of endotracheal tube and this may contribute to later feeding difficulties.
HEARING
Protecting sleep is an important factor in auditory development and the sound environment of the NICU should be monitored to reduce background noise (e.g bins, phones, placing objects on the incubator). Background noise should be kept very quiet, average max. 45 decibels per hour as noise makes it difficult for the infant to hear and respond to the human voice. Parents should be encouraged to speak softly with their infant.
VISION
REM sleep is essential for development of the visual system. As the eyelids of the neonate are thin and let considerable light through, the ambient lighting of the NICU should be adapted e.g placing incubator covers over the isolettes. Pupil contraction reflex is only effective from 32 weeks and the infant is unable to regulate light entering the eye before then.
INTEROCEPTION
Interoception is a sense that allows us to notice internal body signals like a growling stomach, racing heart, tense muscles or full bladder. Our brain uses these body signals as clues to our emotions. Research shows that the ability to clearly notice body signals is linked to the ability to identify and manage the following emotions and more:
Hunger Tiredness Focus Fullness/Thirst Need for Bathroom Calm Pain Anger Boredom Illness Anxiety Sadness Body Temperature Distraction
ATTENTION AND INTERACTION
- Up to 32 weeks Infants are easily overloaded by sensory experience.

The snuggle is real: Banners in the hospital hallway remind the families of premature babies of the importance of kangaroo care.
How ‘kangaroo care’ is helping tiny preemies grow and bond with parents
Helen Adams May 17, 2024
Maggie Gambon hadn’t had a baby shower yet or even bought maternity clothes. The lawyer-turned-marketer was still pretty far away from her due date. But her son Eli was arriving anyway – born March 8. “He weighed 1 pound, 11 ounces,” his mom said.
She’d known she was at risk for premature birth. Gambon had preeclampsia, “a life-threatening hypertensive disorder,” according to the Preeclampsia Foundation. It can lead to “a rapid rise in blood pressure that can lead to seizure, stroke, multiple organ failure and even death of the mother and/or baby,” the foundation’s website says.
“My OB at East Cooper sent me over here to MUSC for observation because of the preeclampsia. And then, while I was here for observation, pulmonary edema set in.” Pulmonary edema, which means too much fluid in the lungs, is life-threatening. That was a signal that her baby had to be born.
“They did an emergency C-section,” Gambon said of her cesarean section, a procedure that may have saved both her life and her baby’s.
Nurse Kara St Laurent, left, and respiratory therapist Rebecca Barbrey help Maggie Gambon settle in to snuggle with Eli. She’ll stay there for two or three hours at a time.
Eli was rushed to the neonatal intensive care unit at the MUSC Shawn Jenkins Children’s Hospital, where he’s had round-the-clock care ever since. His tiny body still needs time to grow before he’ll be big and healthy enough to go home to Summerville with his mom and dad.
Gambon or her husband visit every day. And they’ve learned something special that MUSC Children’s Health doctors and nurses know can help Eli thrive. Julie Ross, M.D., a neonatal specialist at the hospital, said it’s called kangaroo care or skin-to-skin care. Kangaroo, because kangaroo babies rush into their mothers’ pouches after birth, then stay there for months, feeding on their mothers’ milk and growing.
Whatever you call it, human babies need physical contact with a parent’s skin every day if possible. “Our goal is for parents to be able to do skin-to-skin care with their baby as soon as possible after delivery, ideally within the first 72 hours of life if they’re able. And then continuing that up to twice a day for as long as they would like to do that,” Ross said.
“Kangaroo care has significant benefits for preterm babies, including improved neurodevelopment. There are situations where skin-to-skin care can be challenging, based on how sick babies are at times, but we really try everything possible to make sure that it can happen, and when it’s not possible, we encourage parental contact in other ways, such as hand hugs and gentle touch during cares.”
It can be a little scary for the parents of a fragile-looking preemie like Eli. “It’s kind of a big production,” his mother said.
A nurse and a respiratory therapist are on hand to set them up for kangaroo care. Since Eli’s hooked up to machines, they slowly move him toward the bottom of his hospital bed. There, his mother leans over to pick him up carefully. They help her ease into a chair with her baby, where mother and son rest peacefully. She and her husband have seen what a difference it makes.
“We noticed that the days that we did kangaroo, he seemed to have a marked difference in how well he was doing. So we committed to doing it every day. Either I or my husband will be here to kangaroo with him,” Gambon said.
“And I don’t know if the research says if there’s any difference between mom or dad holding them or just human contact. We committed to ensuring he’s going to get skin to skin with one of us every single day, and he’s been doing so much better since we did.”
There’s plenty of science to back up the practice of skin-to-skin care. For example, the World Health Organization said research shows that it “significantly improves a premature or low-birthweight baby’s chances of survival.” It also can save up to 150,000 lives a year, according to the organization.
Delisa Abson smiles as her son, Braxton Abson grips her hand in the neonatal intensive care unit at the MUSC Shawn Jenkins Children’s Hospital. She regularly bonds with him through skin-to-skin contact.
Families in the MUSC Shawn Jenkins Children’s Hospital see banners in the hallways promoting the importance of kangaroo care. Delisa Abson, another mother whose baby needs a little time in the hospital before he’ll be healthy enough to go home, makes it part of her routine, too.
Ross, the neonatal specialist, described some of kangaroo care’s other benefits. “It helps with the baby’s temperature control; reduces stress, including decreasing pain during procedures; increases weight gain; and improves overall stability in heart rate and oxygen saturations. It benefits mom as well in terms of breast milk production and can decrease parental stress and support bonding. The body responds to the baby’s closeness.”
Gambon said she can feel it happening during and after skin-to-skin time with Eli. “Every time I put him back in bed, my breasts feel like they’re gonna explode.” That may not sound like a great feeling, but she’s thrilled to be able to supply that milk to her son. A nurse noticed he’s getting baby fat rolls – a good sign for a little boy who’s still weeks from his original due date.
And the connection Gambon has been able to solidify with Eli while still in the hospital has been remarkable. “It helped tremendously with bonding early on. He was born at 26 weeks gestation, so, initially, I kind of felt like, ‘Man, what just happened to me? Did I have a baby?’ It felt kind of like a mirage. But getting to have skin to skin with him and smell him and feel him … it’s real. It made it real.”

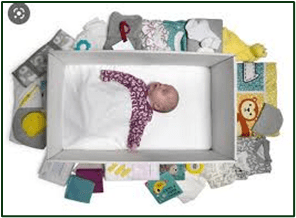
12 Preemie Must-Haves For Bringing Your Preemie Baby Home

Preparing to welcome a new baby home is a time of joy—and stress!—under the most ideal circumstances. But if your baby arrived early and is being cared for in the NICU, bringing them home comes with all of that joy — and a double helping of the stress.
Bringing a preemie home from the NICU requires some extra preparation so you can give your new baby the care they’ll need to grow and thrive. As you make your plans for your preemie’s homecoming, having the right gear and supplies can help to ease the transition and make it through the early days.
This guide can help you get ready, with a comprehensive checklist of preemie must-haves.
What do you do when baby comes home from NICU?
Hospital NICU’s are fully stocked with all the supplies and gear that are needed to care for premature babies. To make the transition from caring for your baby in the NICU to caring for your baby at home as easy as possible, it helps to make sure you have all the preemie must-haves on hand before your baby comes home. This checklist of preemie essentials can help you get organized and get ready:
- Diapers and Wipes: Most preemies require special-sized diapers so be sure to stock up on the sizes you need.
- Bottles: Ask the NICU staff about the best nipple types and bottles for your baby.
- Clothing: Newborn-sized clothing will likely be too big for your baby. You’ll need some cozy preemie-sized onesies and pajamas that fit your baby.
- Swaddle Blankets and Sleep Sacks: Keeping premature babies warm at home is essential, and swaddling can help your baby sleep longer and better. Ask the NICU nurses to help you perfect your swaddling techniques so your baby can get the rest they need.
- Sleeping Arrangements: The American Academy of Pediatrics recommends that babies sleep in a crib or bassinet with a firm mattress in their parents’ room for at least the first six months of their life. The MamaRoo Sleep® Bassinet offers a firm, flat sleeping surface and adjustable legs, making it a great preemie bassinet that you can use until your baby is 25 pounds or can push up on their arms and legs. Plus it has over 100 motion, speed, and sound combinations that can be tailored to baby’s needs.
- Baby Thermometer: A thermometer is an important part of premature baby care and health monitoring. Choose a thermometer that’s suitable for newborns.
- Bathtub: Make bath time easier with a tub designed for infants that can also double as a preemie essential, like the Cleanwater™ Tub—it comes with a newborn insert to cradle your preemie safely and is designed to grow with your baby.
- Nasal Aspirator: A basic bulb syringe or a device that helps to suction mucus from your baby’s nose, making it easier for them to breathe, suck, and eat.
- Medication Management: If your baby needs medications, consult with your NICU team to make sure you have all the medical supplies and prescriptions you need on hand to continue premature baby care at home.
The extended “bringing preemie home” checklist
Beyond these preemie must-haves, you may want some other items that can make premature baby care a little easier:
- Baby Monitor: Being able to keep an eye (and an ear) on your baby can give you some added peace of mind when you’re not in the same room.
- Baby Swing: A baby swing can be a familiar and safe space for your preemie when your tired arms need a break. More than 600 hospital NICUs across the country trust the MamaRoo® Multi-Motion Baby Swing™ to comfort the tiny babies in their care. Want to learn more about this preemie must-have? A NICU nurse explains why its parent-inspired motions keep preemies content and comfortable.
- Skin-to-Skin Gear: A specially made wrap or shirt makes it easy to give your baby the beneficial skin-to-skin contact they need.
Do NICU babies have a hard time adjusting to home?
Bringing a preemie home from the NICU might feel overwhelming, but there are ways to make it a little easier on you.
Use your time in the NICU to gain the confidence you need to care for your baby; the nurses can teach you how to care for preemies and provide any special care your baby needs, including soothing techniques that will calm your baby and help you all settle more easily into a routine. You can also turn to preemie essentials made to soothe babies.
As you and your baby adjust to life at home, it’s vital to establish a support system to help you cope with the sometimes overwhelming responsibilities and emotions that go along with premature baby care. Your partner, parents, relatives, and friends are probably eager to pitch in and help in whatever ways they can—providing meals, helping with household chores, or coming over to hold the baby so you can shower, eat, or just get a little break.
You may also want to seek out a support group that connects you with other parents whose babies were in the NICU to share stories about preemie parenting, trade tips, and get comfort from other new parents who are having similar experiences. A pediatrician who is experienced with caring for preterm babies can help you find a local or online group and can also direct you to any specialists you might need as your baby grows.
Get ready to bring your baby home
Bringing your preemie home from the NICUE is a time that’s both joyful and challenging for your family—but the right tools can help. Preemie must-haves like the MamaRoo® Multi-Motion Baby Swing™—which is used and trusted in more than 600 NICUs in the US—can help you re-create the nurturing environment of the NICU so your preemie can flourish.
And when you purchase these products for your baby, you’re helping –https://www.4moms.com/blogs/the-bib/12-preemie-must-haves-for-bringing-your-preemie-baby-home

HEALTHCARE PARTNERS
Surviving Residency: Insider Secrets from a Chief Resident (Don’t Be THAT Intern!) #residency

2,242 views Jan 20, 2024
I had the pleasure of interviewing one of my chief residents about the tips that he would give himself if he were to do residency again. What he shared with me was beyond inspiring. The individual who I had the pleasure of interviewing was Peter Konyn. He graduated from UC Davis with a B.S. in Pharmaceutical Chemistry, as part of the University Honors Program. He then enrolled at UCLA for medical school, where he graduated at the top of his class, including earning induction into both the AOA Honors Society and the Gold Humanism Honors Society. I think that the tips he shares here are things that I still think about to this day!


Mandatory Reporting in the NICU: Supporting Families with Substance Abuse
Wednesday Jan 08, 2025
In this episode, we explore the intersection of neonatal care, substance use disorders, and mandatory child protective services (CPS) reporting, particularly in the NICU setting. NICU nurses and advanced practice professionals often focus on managing neonatal withdrawal and supporting the baby’s immediate needs, but what happens when mandatory reporting policies impact the delicate relationship between mother and infant? How do these policies affect long-term bonding and family-centered care?
We’re joined by Dr. Kelly McGlothen-Bell, a nursing scientist and expert in reproductive justice and health equity, who brings a wealth of knowledge on the complexities of caring for families affected by substance use during pregnancy. Dr. McGlothen-Bell discusses the stigma surrounding substance use, the emotional and systemic challenges mothers face, and the significant role of CPS interventions, which can create barriers to consistent visitation and strain the mother-infant bond. She also highlights the need for a more integrated, compassionate approach to care, ensuring that families receive necessary services without punitive actions such as child removal when not warranted.
With 31% of births occurring in states with mandatory reporting laws, and nearly half of child removals linked to substance use, understanding the policies at play is critical for healthcare providers. Dr. McGlothen-Bell emphasizes the importance of understanding these policies, advocating for more equitable care, and addressing racial disparities within the child welfare system. The episode also explores how CPS involvement can affect long-term outcomes for families, including stress, relapse, and strained recovery.
Listeners will gain insights into the importance of clear communication, prenatal care, and the role of nurses and social workers in advocating for families both within and outside the NICU. We discuss how healthcare professionals can balance mandatory reporting with compassionate care, ensuring that families navigate the complexities of recovery, legal systems, and childcare with dignity and respect.
This episode is a must-listen for NICU nurses, social workers, and anyone working at the intersection of maternal and neonatal care, as well as those interested in the policy and systemic factors that influence family outcomes in the NICU and beyond.
CHNC 2024 COVERAGE – The Psychologically Minded NICU

The Incubator Channel Oct 28, 2024
Ben and Daphna speak with Dr. Melissa House, Chavis Patterson, and Kathleen Stanton about creating a “psychologically-minded” NICU, where mental health support is essential for families, staff, and patients alike. They discuss the upcoming CHNC workshop, “Combating Distress, Dissatisfaction, and Discord,” which introduces trauma-informed care, caregiver support, and the impact of chronic stress on NICU staff and families. Listen in as they share insights on fostering empathy, self-awareness, and a supportive NICU culture, helping caregivers bring their best selves to the bedside.

INNOVATIONS

Occurrence and Time of Onset of Intraventricular Hemorrhage in Preterm Neonates A Systematic Review and Meta-Analysis of Individual Patient Data
Zsuzsanna Nagy, MD; Mahmoud Obeidat, MD; Vanda Máté, MD; et al Rita Nagy, MD, PhD; Emese Szántó, MD; Dániel Sándor Veres, PhD; Tamás Kói, PhD; Péter Hegyi, MD, DSc9; Gréta Szilvia Major, MD;
JAMA Pediatr. Published online December 30, 2024. doi:10.1001/jamapediatrics.2024.5998

Key Points
Question What are the occurrence and temporal distribution of intraventricular hemorrhage (IVH) in very preterm neonates during the first week of life?
Findings This systematic review and meta-analysis including 64 studies and 9633 preterm neonates found that the overall prevalence of IVH in preterm neonates has not changed significantly over the past 20 to 40 years. However, IVH earlier than 6 hours of life has been reduced to less than 10% of all IVH events.
Meaning These data suggest that although preventive measures have been implemented, IVH has occurred later but its prevalence has not been reduced.
Abstract
Importance Intraventricular hemorrhage (IVH) has been described to typically occur during the early hours of life (HOL); however, the exact time of onset is still unknown.
Objective To investigate the temporal distribution of IVH reported in very preterm neonates.
Data Sources PubMed, Embase, Cochrane Library, and Web of Science were searched on May 9, 2024.
Study Selection Articles were selected in which at least 2 cranial ultrasonographic examinations were performed in the first week of life to diagnose IVH. Studies with only outborn preterm neonates were excluded.
Data Extraction And Synthesis Data were extracted independently by 3 reviewers. A random-effects model was applied. This study is reported following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline. The Quality in Prognostic Studies 2 tool was used to assess the risk of bias.
Main Outcomes And Measures The overall occurrence of any grade IVH and severe IVH among preterm infants was calculated along with a 95% CI. The temporal distribution of the onset of IVH was analyzed by pooling the time windows 0 to 6, 0 to 12, 0 to 24, 0 to 48, and 0 to 72 HOL. A subgroup analysis was conducted using studies published before and after 2007 to allow comparison with the results of a previous meta-analysis.
Results A total of 21 567 records were identified, of which 64 studies and data from 9633 preterm infants were eligible. The overall rate of IVH did not decrease significantly before vs after 2007 (36%; 95% CI, 30%-42% vs 31%; 95% CI, 25%-36%), nor did severe IVH (10%; 95% CI, 7%-13% vs 11%; 95% CI, 8%-14%). The proportion of very early IVH (up to 6 HOL) after 2007 was 9% (95% CI, 3%-23%), which was 4 times lower than before 2007 (35%; 95% CI, 24%-48%). IVH up to 24 HOL before and after 2007 was 44% (95% CI, 31%-58%) and 25% (95% CI, 15%-39%) and up to 48 HOL was 82% (95% CI, 65%-92%) and 50% (95% CI, 34%-66%), respectively.
Conclusion And Relevance This systematic review and meta-analysis found that the overall prevalence of IVH in preterm infants has not changed significantly since 2007, but studies after 2007 showed a later onset as compared with earlier studies, with only a small proportion of IVHs occurring before 6 HOL.
Source:https://jamanetwork.com/journals/jamapediatrics/fullarticle/2828319

NICU nurses first in nation to use new technology as a bridge from parents to the youngest patients
12/18/2024

Carle Foundation Hospital (CFH) is the only Neonatal Intensive Care Unit (NICU) in the region offering Level III perinatal care for newborns with critical conditions. On average, staff care for 35 babies each day in the NICU from an area that stretches west from Bloomington and Decatur, east to Danville and south to Olney. This distance, and potentially long NICU stays, mean some parents may need to leave their healing babies at times in the care of CFH staff.
Now, Carle’s Neonatal Intensive Care Unit is helping parents stay connected with their babies through technology. It is the first unit in the U.S. to offer an innovative and secure application where nurses share photos and video as the baby progresses. It’s called vCreate and is already in use in the U.K.
“Leaving a newborn at the hospital is naturally stressful for parents, some with limited visits for a variety of reasons such as distance from the hospital, work commitments, or caring for siblings of the newborn,” Kara Weigler, RN, manager, Neonatal Intensive Care Unit said. “We receive such positive feedback from parents about having this application available. We can take video of a baby having a bath or photos of the newborns as they progress.”
Not only do parents receive visual updates on their baby’s progress, but nurses also mark special occasions such as visits with Santa Claus.
For Carle Health team members, offering this free tool is just part of the type of care experience they strive for every day. And with such limited options for the level of care the CFH NICU provides, they take that responsibility very seriously.
“If someone cannot deliver, due to a complex pregnancy, at their community hospital, they are transported here,” Weigler said. More than 100 transports arrive at Carle yearly.
Syvanna Keith, who also has a 3-year-old, drives an hour to see her baby who is in the NICU after surgery due to an intestinal blockage. “Having a baby in the NICU is stressful and the nurses in the NICU have been wonderful to work with. Seeing photos of baby Bryan Duane when I am not there really helps a lot.”
A Carle nurse discovered the vCreate application at a conference and introduced the idea to her colleagues. The only equipment the family needs is a smart cell phone to start receiving the photos and videos nurses record in the NICU. Parents may review the message in the language of their choice.

Neonatal care and developmental outcomes following preterm birth: A systematic review and meta-analysis.
Burstein, Or Aryeh, Tamara Geva, Ronny Burstein, O., Aryeh, T., & Geva, R. (2024). Neonatal care and developmental outcomes following preterm birth: A systematic review and meta-analysis. Developmental Psychology. Advance online publication. https://doi.org/10.1037/dev0001844
Abstract
Major amendments in neonatal care have been introduced in recent decades. It is important to understand whether these amendments improved the cognitive sequelae of preterm children. Through a large-scale meta-analysis, we explored the association between prematurity-related complications, neonatal care quality, and cognitive development from birth until 7 years. MEDLINE, APA PsycInfo, and EBSCO were searched. Peer-reviewed studies published between 1970 and 2022 using standardized tests were included. We evaluated differences between preterm and full-term children in focal developmental domains using random-effects meta-analyses. We analyzed data from 161 studies involving 39,799 children. Preterm birth was associated with inferior outcomes in global cognitive development (standardized mean difference = −0.57, 95% CI [−0.63, −0.52]), as well as in language/communication, visuospatial, and motor performance, reflecting mean decreases of approximately 7.3 to 9.3 developmental/intelligence quotients. Extreme prematurity, neonatal pulmonary morbidities, and older assessment age in very-to-extreme preterm cohorts were associated with worse outcomes. Contemporary neonatal medical and developmental care were associated with transient improvements in global cognitive development, evident until 2 to 3 years of age but not after. Blinding of examiners to participants’ gestational background was associated with poorer outcomes in preterm cohorts, suggesting the possibility of a “compassion bias.” The results suggest that preterm birth remains associated with poorer cognitive development in early childhood, especially following pulmonary diseases and very-to-extreme preterm delivery. Importantly, deficits become more pervasive with age, but only after births before 32 gestational weeks and not in moderate-to-late preterm cohorts. Care advancements show promising signs of promoting resiliency in the early years but need further refinements throughout childhood.
Impact Statement
Preterm birth is related to persistent neurodevelopmental difficulties, yet it remains unclear whether changes in care improve outcomes. Covering 50 years of research, including 37,999 children (0–7 years), we found considerable cognitive disadvantages that steepen the earlier the preterm birth occurs and following neonatal brain or lung damage. These early-life difficulties intensify with age but only in very and extreme cases of prematurity. Importantly, changes in neonatal intensive care unit care protocols show some positive, though yet transient, signs of promoting resiliency.

Epigenetics Embedding of Oral Feeding Skill Development in Preterm Infants – A Study Protocol
Griffith, Thao PhD, RN; White-Traut, Rosemary PhD, RN, FAAN; Tell, Dina PhD; Green, Stefan J. PhD; Janusek, Linda PhD, RN, FAAN
Advances in Neonatal Care 24(6):p E88-E95, December 2024. | DOI: 10.1097/ANC.0000000000001216
Abstract
Background:
Preterm infants face challenges to feed orally, which may lead to failure to thrive. Oral feeding skill development requires intact neurobehaviors. Early life stress results in DNA methylation of NR3C1 and HSD11B2, which may disrupt neurobehaviors. Yet, the extent to which early life stress impairs oral feeding skill development and the biomechanism whereby this occurs remains unknown. Our team is conducting an NIH funded study (K23NR019847, 2022-2024) to address this knowledge gap.
Purpose:
To describe an ongoing study protocol to determine the extent to which early life stress, reflected by DNA methylation of NR3C1 and HSD11B2 promoter regions, compromises oral feeding skill development.
Methods:
This protocol employs a longitudinal prospective cohort study. Preterm infants born between 26 and 34 weeks gestational age have been enrolled. We evaluate early life stress, DNA methylation, cortisol reactivity, neurobehaviors, and oral feeding skill development during neonatal intensive care unit hospitalization and at 2-week post-discharge.
Results:
To date, we have enrolled 70 infants. We have completed the data collection. Currently, we are in the data analysis phase of the study, and expect to disseminate the findings in 2025.
Implications for Practice and Research:
The findings from this study will serve as a foundation for future clinical and scientific inquiries that support oral feeding and nutrition, reduce post-discharge feeding difficulties and lifelong risk of maladaptive feeding behaviors and poor health outcomes. Findings from this study will also provide further support for the implementation of interventions to minimize stress in the vulnerable preterm infant population.

100 Kids Describe Love | 100 Kids | HiHo Kids


A Message of Love and Resilience for My Fellow Preemie Warriors
Dear Fellow Warriors,
I want to take a moment to talk to you about love—not just the love we’ve received but the love we carry within ourselves. You’ve come so far, and every step of your journey has been marked by resilience fueled by love.
Love is what surrounded you in those early days. It’s the hands that held you, the whispers of encouragement when things felt uncertain, and the hope that never wavered. That love wasn’t just given to you—it became part of you, a quiet strength you carry forward every single day.
But here’s the beautiful thing about being a preemie: you’ve learned that love isn’t just something you receive; it’s something you radiate. Every time you take a step forward, every milestone you achieve, and every moment you choose to persevere, you remind the world what love in action looks like.
Life may present challenges, but love is your greatest ally. It’s the love you show yourself when you celebrate how far you’ve come. It’s the love you give others when you share your story, offering hope and inspiration. And it’s the love that reminds you that you are more than capable of facing anything that comes your way.
Resilience doesn’t mean you don’t face hardships. It means you face them with courage, with the knowledge that you’ve already overcome so much. Love and resilience go hand in hand—they’ve carried you this far, and they’ll continue to carry you wherever you dream of going.
So, to every preemie reading this: You are enough. You are strong. You are loved. And because of that love, there is nothing you can’t do.
Keep shining, keep thriving, and never forget the power of love within you.
With pride and encouragement, Kathryn Campos
NICU babies celebrate first Valentine’s Day


Preemie Love – Music video

This song aims to carry the premature cause and gather around common values. The video clip represents the struggle of prematurity through our little magician Julia, a former premature baby, who gets to the end of the race despite the obstacles with the help of caregivers.



Biscuit’s Valentine’s Day | Read Aloud by Reading Pioneers Academy

It’s Valentine’s Day and Biscuit is ready to play. What will he do? Woof! Let’s find out in this wonderful tale, “Biscuit’s Valentine’s Day” by Alyssa Capucilli.

Kitesurfing in Kuwait

















































































































































































































 Published on Jan 31, 2019 Physician Mental Health & Suicide
Published on Jan 31, 2019 Physician Mental Health & Suicide




















{kind=link}