





Preterm Birth Rates – Colombia
Rank: 114 –Rate: 8.8% Estimated # of preterm births per 100 live births (USA – 12 %)
Source: https://www.marchofdimes.org/mission/global-preterm.aspx
Colombia, officially the Republic of Colombia is a country largely in the north of South America, with territories in North America. Colombia is bounded on the north by the Caribbean Sea, the northwest by Panama, the south by Ecuador and Peru, the east by Venezuela, the southeast by Brazil, and the west by the Pacific Ocean. It comprises 32 departments and the Capital District of Bogotá, the country’s largest city. With an area of 1,141,748 square kilometers (440,831 square miles), Colombia is the fourth-largest country in South America, after Brazil, Argentina and Peru. It is also the 25th-largest country in the world, the fifth-largest country in Latin America, and the fourth-largest Spanish-speaking country.
The overall life expectancy in Colombia at birth is 74.8 years (71.2 years for males and 78.4 years for females). Healthcare reforms have led to massive improvements in the healthcare systems of the country, with health standards in Colombia improving very much since the 1980s. Although this new system has widened population coverage by the social and health security system from 21% (pre-1993) to 96% in 2012, health disparities persist.
Through health tourism, many people from over the world travel from their places of residence to other countries in search of medical treatment and the attractions in the countries visited. Colombia is projected as one of Latin America’s main destinations in terms of health tourism due to the quality of its health care professionals, a good number of institutions devoted to health, and an immense inventory of natural and architectural sites. Cities such as Bogotá, Cali, Medellín and Bucaramanga are the most visited in cardiology procedures, neurology, dental treatments, stem cell therapy, ENT, ophthalmology and joint replacements because of the quality of medical treatment.
Source: https://en.wikipedia.org/wiki/Colombia

COMMUNITY
Cuddling Preemies Kangaroo Style Helps Into Adulthood
By Maggie Fox -Dec. 12, 2016
Cuddling small and premature babies in a style known as “kangaroo mother care” helps them in life decades later, researchers reported Monday.
They found that babies held upright and close to bare skin and breastfed, instead of being left in incubators, grew up with fewer social problems. They were far less likely to die young.
It’s a reassuring finding for parents who may worry that tiny and premature babies are safer in an incubator than in their arms, the team wrote in their report, published in the journal Pediatrics.
Kangaroo mother care was first described in Colombia, and the team of experts there who first showed it was safe did a 20-year follow-up to see how the babies fared as they grew up. They tracked down 494 of the original 716 children who were born prematurely from 1993 to 1996 and randomly assigned to get either kangaroo mother care or standard handling.
“The effects of kangaroo mother care at one year on IQ and home environment were still present 20 years later in the most fragile individuals, and kangaroo mother care parents were more protective and nurturing,” Dr. Nathalie Charpak and colleagues at the Kangaroo Foundation in Bogota, Colombia, wrote in their report.
“At 20 years, the young ex-kangaroo mother care participants, especially in the poorest families, had less aggressive drive and were less impulsive and hyperactive. They exhibited less antisocial behavior, which might be associated with separation from the mother at birth,” they added.
“Kangaroo mother care may change the behavior of less well-educated mothers by increasing their sensitivity to the needs of their children, thus making them equivalent to mothers in more favorable environments.”
Twenty million babies are born at a low birth weight every year around the globe, the World Health Organization reports. The U.S. has one of the highest rates of pre-term and low-weight births — about one in 12 births, according to the March of Dimes.
It defines low birthweight as being when a baby is born weighing less than 5 pounds, 8 ounces.
Most of these small babies are premature and they are at high risk of dying, of developing cerebral palsy, or having learning disabilities, and they can grow up more prone to a range of diseases.
High-tech care can help, but WHO promotes the simpler, low-tech approach alongside modern medical care — or instead of it in some poor settings.
“Kangaroo mother care is care of preterm infants carried skin-to-skin with the mother. It is a powerful, easy-to-use method to promote the health and well-being of infants born preterm as well as full-term. Its key features are: early, continuous and prolonged skin-to-skin contact between the mother and the baby; exclusive breastfeeding (ideally); it is initiated in hospital and can be continued at home; small babies can be discharged early; mothers at home require adequate support and follow-up,” WHO said.
“It is a gentle, effective method that avoids the agitation routinely experienced in a busy ward with preterm infants.”
And it’s safe, WHO added. “Almost two decades of implementation and research have made it clear that kangaroo mother care is more than an alternative to incubator care.”
Charpak’s team found the babies randomly assigned to get this treatment were 39 percent more likely to live into adulthood. They had stayed in school longer and earned more as adults.
It didn’t work miracles. Children with cerebral palsy were equally likely to have symptoms whether they had the kangaroo care or not, and more than half the people in the entire group needed glasses. The children given standard care had higher math and language scores in school, while IQ levels were about the same in both groups.
But overall, the findings support the benefits of kangaroo mother care, the team concluded.
“Our long-term findings should support the decision to introduce kangaroo mother care to reduce medical and psychological disorders attributable to prematurity and low birth weight,” they wrote.
“We suggest that both biology and environment together might modulate a powerful developmental path for these children, impacting until adult age,” they added.
“We firmly believe that this is a powerful, efficient, scientifically based health intervention that can be used in all settings.”

Kat and I have danced Zumba for the past 13 years and are both certified instructors. Kat teaches several Zumba and Strong Nation (HITT) classes every week. Zumba founders Alberto “Beto” Pérez (Colombian native), Alberto Perlman, and Alberto Aghion built a worldwide global health and fitness community (180 countries) that we are grateful to be a part of. Zumba in the streets? That’s what it’s all about! And our Neonatal Womb Community? We all need to do a little dancing. This pandemic has been challenging and we have a ways to go! Let’s move forward with curiosity, creativity, some crazy footwork and a focus on taking active care of ourselves and each other.
Colombia: Bogota Police help fight corona-virus isolation blues with dance classes
Apr 1, 2020
Colombian national police officers took to Bogota’s streets on Tuesday with loud speakers and dance tunes to encourage citizens to get some exercise and help them get through self-isolation with high spirits. “We are working at the moment on the idea of prevention to help people in everything that relates to tranquility in terms of their spiritual, physical and mental control in relation to the entire quarantine due to COVID-19,” said national police colonel Doris Manosalva. Footage shows police officers coordinating the dance operation before heading out to the streets to dance, calling on people to join them as well as reminding everybody the importance of staying inside. Police officers go to a different area of the city every day to reach as many citizens as possible.

How California Became The Only State To Lower Its Infant Mortality Rate
Here’s how they’re saving the lives of more premature babies.
By Anna Almendrala – 08/08/2018
California was the only state to significantly reduce the rate of stillbirths and newborn deaths from 2014 to 2016.
In 2014, Dr. Elizabeth Rogers and her colleagues at the UCSF Benioff Children’s Hospital in San Francisco noticed a disturbing trend among the tiniest preemies in their neonatal intensive care unit: a high rate of brain bleeds among these babies born before 28 weeks’ gestation.
Rogers wondered if other NICUs had seen an increase as well or if there was something about her patient population that put them at particular risk.
Intracranial hemorrhages, caused by the rupture of immature blood vessels in the brain, are a major cause of death in very preterm babies, as well as a complication linked to developmental delays and cognitive deficits later in life. Driving down the rate of such complications is one way that hospitals can help reduce the number of early infant deaths.
Compared to other rich countries, the U.S. has unacceptably high rates of perinatal deaths, a category that covers stillbirths and deaths within the first week of life. And the most recent data suggest those numbers are not improving ― except in California. That state was the only one to see a decrease in perinatal deaths from 2014 to 2016, according to a report published Wednesday by the Centers for Disease Control and Prevention’s National Center for Health Statistics.
The reason for California’s success may be a statewide data project that has been gathering information from hospitals for the past two decades. In any other state, Rogers and her colleagues would have struggled to find an answer to her initial question about the prevalence of brain bleeds. But because they were in California, Rogers was able to log into a data dashboard created by the California Perinatal Quality Care Collaborative. The easy-to-use clearinghouse of real-time information from more than 90 percent of California hospitals that treat babies in NICUs let her compare her unit’s outcomes to those at similar units.
What she found shocked her. UCSF was seeing brain bleeds in more than 15 percent of NICU babies, or nearly four times the rate at comparable hospitals of the same size and expertise.
“I was able to go to the dashboard and say, ‘Not only do we think this is a problem, but this really is a problem,’” said Rogers, who is director of the hospital’s intensive-care small-baby program.
Armed with that information, she persuaded hospital administrators to allocate resources to the issue; gathered a group of doctors, nurses, therapists, technicians, janitors and parents to consider what steps to take; and produced a training manual for staffers.
I was able to go to the dashboard and say, ‘Not only do we think this is a problem, but this really is a problem.’ Dr. Elizabeth Rogers
It isn’t clear what causes brain bleeds in premature babies, so Rogers’ group tackled the issue in multiple ways. Starting in 2014, women who went into labor preterm received a shot of steroids to strengthen their babies’ brains. Immediately after birth, the clamping of a preemie’s umbilical cord was delayed 45 seconds, which is known to decrease brain bleeds.
Everyone who interacted with the babies, from X-ray techs to sanitary workers, received training on how to create a calm environment, which included intervening as little as possible and using low voices if they had to speak.
In about three years, UCSF reduced the rate of brain bleeds to 3.8 percent, just a quarter of what it had been and on par with comparable hospitals in the state. This decrease set off a cascade of other positive outcomes. Deaths in the NICU were cut almost in half, dropping from 11.9 percent to 6.8 percent over that time period. Rates of necrotizing enterocolitis ― another common complication among premature babies ― went down as well, which Rogers attributed to the hospital’s increased attention to their littlest patients.
The speed at which Rogers and her team implemented research-based change was remarkable and unusual. It takes an average of 17 years for research data to alter standard medical practice, in part because of entrenched hospital bureaucracies that favor tradition, a systemic reluctance to spend money on monitoring and prevention, and medical staff who may feel competitive and territorial.
Without the initial comparative data, Rogers is convinced she wouldn’t have been able to revamp her NICU’s systems so fast and the rates of hemorrhage would have remained high.
Hospitals in general need to become better at rapidly adjusting and refining their care when it’s lacking or when new research points to a better way of doing things, Rogers argues.
Across the rest of the country, rates of stillbirths and deaths within a week after birth remain at a standstill. In one state, Missouri, the rate has actually gone up since 2014. California has the third-lowest rate, following Washington state and Wyoming.
“To see the results … is a huge reward,” said Rogers. “It’s a huge validation that all of this effort is worth it.”
They’ll pay thousands to monitor one baby’s heart rate, but there’s no money set aside to monitor the monitors. Dr. Jeffrey Gould, co-founder of the California Perinatal Quality Care Collaborative
While the larger issue of American infant mortality is now more widely recognized, it wasn’t in the public consciousness 21 years ago when Dr. Jeffrey Gould, then a researcher with the University of California, Berkeley, began to compile a single statewide database of numbers on newborn deaths and complications, paid for by the state.
The project grew as Gould convinced neonatologists, hospitals, insurance payers, public health experts and state agencies that it was in everyone’s interest to share NICU data in real time. With its wealth of information, the California Perinatal Quality Care Collaborative also develops best practice standards and toolkits to help hospitals implement those practices. It periodically launches initiatives aimed at improving care in one particular area, such as breastfeeding in the NICU, using antibiotics and reuniting these vulnerable newborns with their families.
The model of the California Perinatal Quality Care Collaborative has spread across the country, albeit only in recent years. Most states now have some kind of perinatal quality collaborative, but they aren’t created or funded equally. Because California was the first, none of the other state collaboratives has as much data or experience. And though some of them provide education on better practices, they don’t seek to help hospitals implement specific changes ― an aspect of California’s collaborative that makes membership so worthwhile. This means the gains California has seen are not guaranteed in other parts of the country.
Gould, now a professor of neonatal and developmental medicine at Stanford, is especially frustrated that hospitals still hesitate to invest real money in trying to improve the quality of care.
“One of the big drawbacks in this country is that quality improvement is not really seen by hospital administrators as a line item kind of thing,” Gould said. “They’ll pay thousands to monitor one baby’s heart rate, but there’s no money set aside to monitor the monitors.”
The annual cost of membership in the California Perinatal Quality Care Collaborative is $13,000 to $15,000, depending on the size of the hospital, and it gives them access to the data dashboard. Participation in each individual initiative is optional and costs an additional fee ― around $8,500 per hospital ― to defray the additional costs for data collection, training and network access.
Meanwhile, the average daily cost of one baby’s care in a NICU is more than $3,000.
More data may ultimately ease this problem too, Rogers said. Besides helping doctors make the case to administrators for more resources for the NICU, as she did, better information leads to more effective and efficient care, which can lead to cost savings.
When a state does decide to invest in improving outcomes for preemies, hospitals may not know where to start. Gould’s suggestion: Use the data to find the low-hanging fruit, and then build on those first successes.
That’s exactly what Rogers is doing. The doctor is now turning her attention to necrotizing enterocolitis, a bacterial infection in the gut that can destroy intestinal walls. As brain bleeds have continued to decrease, necrotizing enterocolitis has become the biggest contributor to preemie deaths in her unit.
Again, armed with data, Rogers convinced the hospital to free up some funding for her unit to take part in the California Perinatal Quality Care Collaborative’s current effort to improve nutrition in NICUs. For premature babies, this boils down to hospital policies that encourage and assist mothers to pump breast milk soon after the baby’s birth ― a difficult task for women who have just experienced a stressful and unexpected early delivery.
Because formula feeding is one of the only consistent risk factors for necrotizing enterocolitis, breast milk ― especially milk produced by the baby’s mother ― decreases the odds that a premature baby will develop the infection. It’s so good for NICU patients, Rogers said, that doctors look at it more like medicine than food.


Brazil changes maternity leave for mothers of premature babies – a step to a fairer and more humane scenario of the labour market for all women
Brazil (2019): The maternity leave for mothers of premature babies is extended. Last month Brazil’s Supreme Federal Tribunal decided to prolong the period of maternity leave for mothers of premature infants. We talked to Denise Leao Suguitani, founder and executive director of GLANCE partner parent organisation Brazilian Parents of Preemies’ Association (Prematuridade.com), member of the GLANCE advisory board, about this important adjustment in Brazilian law.
- Ms Suguitani, Brazil took another big step to strengthening maternal rights. What brought this change to come?
We, the organized civil society, were finally able to raise awareness for the Brazilian Governments about the challenges prematurity brings along. It seems they have understood the essentiality of protecting motherhood and childhood, especially for more delicate babies like the premature ones. Although the decision is valid only for mothers working on a formal contract, it is a huge step towards a fairer and more humane scenario of the labour market for all women.
- Ms Suguitani, your parent organisation spoke to the lawyers who placed the injunction that was eventually approved. What changes for mothers of premature babies in Brazil from now on?
Women in the workforce in Brazil have 120 days of standard maternity leave, which begins on the day of the delivery. From now on, mothers of premature babies can require a new beginning of maternity leave, if their baby needs to be in the hospital for more than two weeks. Once the baby is discharged, the maternity leave with its 120 days starts anew – regardless of how long the baby had to stay in hospital.
- The initial decision of Minister Fachin was valid until the Brazilian Federal Supreme Court plenary confirmed the new law, on April 3rd. How do you assess that victory in the Court?
We were really optimistic that the injunction would not be overturned since we have been working for the approval of this law for over 5 years now, dialoguing with politicians and decision makers. It is such a great achievement for the cause of prematurity in our country and a big step for our society.
Ms Suguitani, thank you so much for taking the time to speak with us.
Source: https://www.glance-network.org/news/details/brazil-extends-maternity-leave/

INNOVATIONS
Association of Air Pollution and Heat Exposure With Preterm Birth, Low Birth Weight, and Stillbirth in the USA Systematic Review
Bruce Bekkar, MD1; Susan Pacheco, MD2; Rupa Basu, PhD3,4; et alNathaniel DeNicola, MD, MSHP5 – June 18, 2020
Key Points:
Question Are increases in air pollutant or heat exposure related to climate change associated with adverse pregnancy outcomes, such as preterm birth, low birth weight, and stillbirth, in the US?
Findings In this systematic review of 57 of 68 studies including a total of 32 798 152 births, there was a statistically significant association between heat, ozone, or fine particulate matter and adverse pregnancy outcomes. Heterogeneous studies from across the US revealed positive findings in each analysis of exposure and outcome.
Meaning The findings suggest that exacerbation of air pollution and heat exposure related to climate change may be significantly associated with risk to pregnancy outcomes in the US.
Abstract
Importance Knowledge of whether serious adverse pregnancy outcomes are associated with increasingly widespread effects of climate change in the US would be crucial for the obstetrical medical community and for women and families across the country.
Objective To investigate prenatal exposure to fine particulate matter (PM2.5), ozone, and heat, and the association of these factors with preterm birth, low birth weight, and stillbirth.
Findings Of the 1851 articles identified, 68 met the inclusion criteria. Overall, 32 798 152 births were analyzed, with a mean (SD) of 565 485 (783 278) births per study. A total of 57 studies (48 of 58 [84%] on air pollutants; 9 of 10 [90%] on heat) showed a significant association of air pollutant and heat exposure with birth outcomes. Positive associations were found across all US geographic regions. Exposure to PM2.5 or ozone was associated with increased risk of preterm birth in 19 of 24 studies (79%) and low birth weight in 25 of 29 studies (86%). The sub-populations at highest risk were persons with asthma and minority groups, especially black mothers. Accurate comparisons of risk were limited by differences in study design, exposure measurement, population demographics, and seasonality.
Conclusions and Relevance This review suggests that increasingly common environmental exposures exacerbated by climate change are significantly associated with serious adverse pregnancy outcomes across the US.
Introduction
The current climate crisis, also known as climate change or global warming, has been widely recognized as an environmental emergency that threatens many critical resources and protections including sustainable food and water supplies, natural disaster preparedness, and US national security. However, as the World Health Organization and The Lancet Countdown have identified, one of the greatest consequences of climate change is its association with human health.
Specific to women’s health, the American College of Obstetricians and Gynecologists position statement recognizes that “climate change is an urgent women’s health concern as well as a major public health challenge.” The associations of climate change with women’s health have been further outlined to include a wide range of undesirable outcomes, such as worsening of cardiac disease, respiratory disease, and mental health, and exposure to an increasing number of infectious diseases.
These adverse health effects are most consequential to at-risk populations, which include a high number of pregnant women and developing fetuses. The obstetrical literature has included numerous observational studies demonstrating an association between air pollution and heat and increased risk of adverse birth outcomes. Two components of air pollution that are exacerbated by climate change and continued use of fossil fuels are fine particulate matter less than 2.5 μm in diameter (PM2.5) and ozone.
In this review, we assessed the associations between exposure to PM, ozone, and heat and preterm birth, low birth weight, and stillbirth. Although these associations have largely been studied in a global setting, we focused specifically on the US population, in which these exposures are increasingly common.
Methods
Scope of Review
For this systematic review, we evaluated evidence of the association between air pollution and heat on the adverse obstetrical outcomes of preterm birth, low birth weight, and stillbirth. The Arskey O’Malley methodologic framework for a scoping review was used.18,19 This study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline.
Research Questions
The following specific key questions were addressed in this review. Is prenatal exposure to PM2.5 or ozone associated with increased risk of preterm birth? Is prenatal exposure to PM2.5 or ozone associated with increased risk of low birth weight? Is prenatal exposure to PM2.5 or ozone associated with increased risk of stillbirth? Is prenatal exposure to heat associated with increased risk of preterm birth? Is prenatal exposure to heat associated with increased risk of low birth weight? Is prenatal exposure to heat associated with increased risk of stillbirth?
Discussion
Studies across diverse US populations were identified that reported an association of PM2.5, ozone, and heat exposure with the adverse obstetrical outcomes of preterm birth, low birth weight at term, and stillbirth. More than 32 million births were analyzed, with a mean (SD) of 565 485 (783 278) births per study. In each analysis of climate change–related exposure and adverse obstetrical outcome, most of the studies found a statistically significant increased risk (Table). The highest number of studies were found for risk of preterm birth (29 studies) and low birth weight (32 studies), whereas limited studies were identified for stillbirth (7 studies) because of the lack of available data for health studies.
Our review contributes the largest number of recent studies (2007-2019) focusing solely on US populations and is the first, to our knowledge, to combine the increasingly common exposures of air pollutants and heat associated with a series of adverse obstetrical outcomes. Our findings are consistent with other review articles that were not included in our analysis (all included non-US participants). Reviews that examined PM2.5 found consistently positive association with preterm birth and low birth weight or continuous birth weight, and 1 systematic review and meta-analysis on stillbirth risk showed elevated effect estimates for both PM2.5 and ozone, although they did not achieve significance. Five reviews that focused on heat exposure found an association with preterm birth in most studies, as did 4 that analyzed low birth weight and 2 analyzing stillbirth risk.
The adverse obstetrical outcomes examined in this study are known to be complex, heterogeneous, and multifactorial in origin; several animal studies suggested that both air pollutant and heat exposure may contribute to adverse obstetrical outcomes. Regarding preterm birth, mechanisms that implicate toxic fine particulates include maternal hematologic transport of inhaled noxious chemicals, the triggering of systemic inflammation, or alterations in function of the autonomic nervous system. Low birth weight may be associated with air pollutants by direct toxic effects from fetal exposure, altered maternal cardiac or pulmonary function, systemic inflammation from oxidative stress, placental inflammation, altered placental gene expression, or changes in blood viscosity; multiple effects may operate simultaneously. Mechanisms for the association of air pollutants with stillbirth may involve alterations in oxygen transport, DNA damage, or placental injury. The cause-specific analysis by Ebisu et al of stillbirths reinforces the apparent association of injury to the fetal-placental unit with air pollutant exposure compared with other possible causes.
Heat exposure may contribute to prematurity through labor instigation from dehydration (via prostaglandin or oxytocin release), from altered blood viscosity, and/or by leading to inefficient thermoregulation; it may also trigger preterm premature rupture of membranes and thus preterm birth during the warm season. Likewise, heat exposure may impair fetal growth by reducing uterine blood flow and altering placental-fetal exchange. Mechanisms associated with elevated temperatures and stillbirth include the initiation of premature labor (as noted above), lowering amniotic fluid volume, damaging the placenta, or causing abruption.
Biologic plausibility is further supported by other recent studies not included in this review. The study by Casey et al of preterm birth rates in California before and after coal power plant closures showed a 27% reduction during the 10-year period after closure. Currie et al found that among 1.1 million live births in Pennsylvania, the risk of low birth weight was higher within 3 km of a fracking site compared with the background risk and increased by 25% within 1 km of a site.
This review revealed a disproportionate effect on populations defined as pregnant women with certain medical conditions or specific race/ethnicities. Women with asthma may be particularly susceptible to adverse outcomes, such as preterm birth and stillbirth, in association with PM2.5 exposure during gestation. Among racial/ethnic groups, our findings suggest that black mothers are at greater risk for preterm birth and low birth weight. Social determinants of health, including residence in urban areas with higher exposure to air pollutants and long-term high levels of stress, are known to contribute to adverse obstetrical outcomes. A recent study from California suggested that PM2.5 exposure alone was associated with an equivalent amount of the racial disparity (black vs white) in preterm birth rates as did other demographic and social factors. Our research suggests that these environmental exposures further exacerbate that background risk and could be included among these social determinants.
Regarding both air pollutant and heat exposure, associations with adverse birth outcomes were found across the continental US. For example, studies on air pollution and low birth weight found an association in 19 states in the Northeast (10), Southeast (5), Midwest (2), Mountain (1), and West (1) regions. California, known for both high temperatures and unhealthy particulate and ozone levels, was included in the greatest number of studies showing a positive association (13), followed by Massachusetts (6), Georgia (5), and Florida (4). The exposures are complex; even within 1 state, the weather patterns, geography, and urbanization may create zones with widely different pollution risks, as shown by Tu et al in Georgia.
Future research is needed to further identify at-risk populations, high-exposure geographic areas, and effects of seasonality. This ongoing research may be enhanced by improved geographic information systems that can be mapped onto existing US public health data-banks such.
Conclusions
This review suggests that increasingly common environmental exposures exacerbated by climate change are significantly associated with serious adverse pregnancy outcomes across the US. It appears that the medical community at large and women’s health clinicians in particular should take note of the emerging data and become facile in both communicating these risks with patients and integrating them into plans for care. Moreover, physicians can adopt a more active role as patient advocates to educate elected officials entrusted with public policy and insist on effective action to stop the climate crisis.
Source: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2767260

Intensive Care Neonates and Evidence to Support the Elimination of Hats for Safe Sleep
Fulmer, Megan BSN, RN-NIC; Zachritz, Whitney MSN, CPNP-BC, RN; Posencheg, Michael A. MD
Editor(s): Harris-Haman, Pamela A. DNP, CRNP, NNP-BC, Section Editor
Advances in Neonatal Care: June 2020 – Volume 20 – Issue 3 – p 229-232
Abstract
Background:
Although the incidence of sudden unexplained infant deaths has decreased over time with the use of safe sleep practices, one area that remains unclear is the safety of hats during infant sleep.
Purpose:
Decrease the risk of overheating or suffocation by removing NICU infants’ hats during sleep without increasing the relative risk of hypothermia during transition to an open crib.
Methods:
Removal of hats for routine thermoregulation, beyond the initial infant resuscitation and stabilization of NICU infant was implemented in 2015. Retrospective chart audits were conducted on all NICU infants between February 2015 and December 2016. Hypothermia (≤ 97.6°F) data during transition to an open crib was collected. Exclusion criteria included concurrent diagnosis of: sepsis, hyperbilirubinemia, congenital anomaly inhibiting infants thermoregulation and noncompliance with unit guideline for weaning infant to open crib.
Findings:
Over 18 months, 2.7% of infants became hypothermic (≤ 97.6°F) during transition to open crib, requiring return to isolettes.
Implications for Practice:
Hats were found to be unnecessary in maintaining thermoneutrality after weaning infants to an open crib in our NICU. By avoiding the use of hats in an open crib, it’s possible infants will avoid overheating and a risk of suffocation, creating a safer sleep environment.
Implications for Research:
The removal of hats during sleep to promote infant health should be considered for all infants.

PREEMIE FAMILY PARTNERS
Premature Baby Makes Full Recovery After Experimental Coronavirus Treatment | NBC News NOW
 Jun 22, 2020
Jun 22, 2020
Born premature at just 27 weeks, one baby is finally on his way home after battling both sepsis and COVID-19. NBC News’ Helena Humphrey spoke with the baby’s mother about his 47-day battle.

Preemie Parent Perspective: Addressing Health Equity and Cultural Competency in the NICU
Jenné Johns, MPH
In 2016, I published Once Upon A Preemie, a first- of its kind children’s book written to comfort parents of premature infants during their journey through the Neonatal Intensive Care Unit (NICU). During my journey, I discovered that reading to my micropreemie was the one activity as a mother that I could offer my son that helped normalize my overwhelming and traumatic NICU experience. During our nearly three-month stay in the NICU, I read to my son every day as research studies suggest that reading stimulates healthy brain development in preemies, and also helps to form a bond between parent and baby. Many of the bedtime stories that we read ended with a parent tucking the child into bed at home with Mommy and Daddy. That wasn’t our reality for three months. There were no books about us. Little did I know that in publishing my deepest emotions carried during and post NICU would lead me to become an author and speaker, but also an advocate and advisor for the needs of preemie parents, especially African Americans. As the mother of a micro-preemie and miracle baby born at 26 weeks and weighing 1 lb 15.3 ounces, I found myself advocating for his needs as I knew his life depended on it. Despite my 10-year career working to eliminate racial and ethnic disparities in health care, nothing prepared me for the heart-wrenching experience of my son’s premature birth. “Disparity” became real for me as my son joined the ranks of the nearly 500,000 premature babies born in the United States, nearly half to African American and Hispanic mothers. It was through this dual role that I experienced the NICU, one as a vulnerable micro-preemie mother, and the other as a health equity professional.
At birth, my son required life-saving medical interventions; oxygen, photo-therapy lights, feeding tubes, a heart monitor, medication, vitamins, and even caffeine. Over our nearly three-month stay in the NICU, I traveled through snowstorms and blizzards, to parent and nurture my baby. I only missed three days (two due to inclement weather and one self-care day). A typical day in the NICU lasted from 7 am until midnight, with many breaks to pump breast milk. My lactation consultant promised that my breast milk was liquid medicine. Midway through our NICU journey, I had to return to work, unlike many of my new NICU parent friends who were Caucasian. My advocacy skills were tested daily, as his life depended on how well I could speak “neonatology” language, I had to be his voice and articulate his needs. This was challenging because, after all, “I’m just a Mom,” an African American Mom, and not a doctor.
As a mother, my NICU journey was traumatic and filled with a sea of emotions, including fear, anxiety, helplessness, and isolation. Much of which NICU parents are facing due to the current COVID-19 pandemic. Many of my fears, concerns, and feelings of isolation were due to the NICU environment, which was not as culturally friendly and supportive, as I assumed it would be. I’m being generous by saying there was little cultural diversity; it was dismal at best. There were times when the lack of cultural sensitivity and bedside manner caused more pain than my son’s actual health status, and it made me very uncomfortable because as the end of each night, I had to trust my most prized possession with nurses and doctors who I did not always trust. Another challenge I faced as an African American preemie parent, was that although our larger hospital system had active and robust NICU parent support groups, these resources were not made available at the smaller hospital where I delivered my son. This hospital served more African American and lower-income families than the other hospitals. Many of the parents I developed a relationship with, felt as if our socio and emotional needs did not matter and were oftentimes dismissed because of this missing resource.
Lastly, I experienced inconsistent positive communication and relationships with many of the NICU staff. Although I now believe that all of the members of my son’s care team, held his safety and the quality of care they delivered to him with the utmost regard, our daily communication and interaction lacked humility, respect, and sensitivity. I will admit, I was not always the easiest or most cheerful mother to deal with, I now believe, that with trauma-informed and implicit bias training among hospital staff, the professional staff would have been better equipped to communicate and support my delicate and fragile nature.
Overall, a good deal of our NICU experience was positive; some experiences left permanent and negative memories that, to this day, cannot be erased. As much as I tried checking my professional credentials at the door before entering the NICU, my interactions with the NICU staff begged, yelled, and warranted us to have those tough cultural sensitivity conversations. Not in a negative way, but as an opportunity for forming better communication, respect, and, most importantly, trust. In my professional view, the NICU is a microcosm of the larger hospital system on steroids, particularly NICU’s serving low income and racially, ethnically, and linguistically diverse populations. Health disparities impacting the NICU are also a reflection of a larger hospital ecosystem. Below are my preemie parent and professional recommendations for integrating health equity and cultural competency in the NICU:
1. Prioritize health equity and cultural competency as strategic priorities and goals. Establishing opportunities for integrating and addressing health equity in short and long terms strategies ensures layers of accountability, allocation of funding, measurement, and documentation of outcomes. One example of an important health equity priority includes staff diversity. Peer-reviewed studies have shown that cultural congruence among patients and providers yields better health outcomes, better communication, and trust.
2.Make health equity, cultural competency, and implicit bias training mandatory for all NICU Staff. Participating in an annual training program is a great start to begin addressing and delivering equitable care to all NICU families. However, one-time training is not sufficient. Integrating health equity and implicit bias content into clinical rounds, staff development, and training opportunities are critical to reducing racial and ethnic disparities in the NICU.
3.Communicating in lay terms should be standard in every NICU. Literacy and health literacy levels are important considerations for family-centered and culturally appropriate care in the NICU. Regardless of one’s educational level, the NICU terminology is overwhelming and confusing for a new parent entering the NICU. Literacy and health literacy considerations are also important factors for families who are limited or non-English speaking. Break the communication barriers by speaking the same language and utilizing interpreters even if everyone speaks English. I had a great deal of respect and appreciation for the NICU staff who used lay terms and avoided NICU jargon when communicating with me. In time, I began understanding the NICU language; however, that wasn’t my job as a preemie parent. Preemie parents should be made to feel as comfortable speaking and interacting with NICU staff regardless of their literacy and health literacy levels.
4.Partner with parents to address the cultural competency, spiritual diversity, and unconscious biases that exist in the NICU. Listen to the voices of parents with multicultural backgrounds to be more sensitive to racial, ethnic, language, income, education, transportation, and spiritual needs. Encourage preemie parents to speak up. Staff should value their input. Allow parents to give their insights on their baby’s health status, and any gut feelings they may have about a diagnosis or new development. This is extremely important for minority parents who assume their voice and parental role is undervalued.
5.Engage and establish culturally congruent NICU family supports. Many minority parents may not immediately express a need for mental or emotional help while in the NICU for fear of being labeled. Where and when possible, make culturally congruent resources available to support these parents, even if the supports are outside of the NICU.
6.Make digital technology and virtual solutions available to parents with transportation, competing work schedules, or other barriers to delivering care to their preemies. This is most critical during the current COVID season, where parental fears and social distancing may prohibit them from visiting their baby. Creating safe opportunities for parents to connect with their babies is vital bonding via smart devices or other safe technology solutions.
Source:http://www.neonatologytoday.net/newsletters/nt-jun20.pdf

Coastal Sunrise Father dances on TikTok for his son in NICU
 WSAV3 – Feb 5, 2020
WSAV3 – Feb 5, 2020

HEALTH CARE PARTNERS
Using Neonatal Intensive Care Units More Wisely for At-Risk Newborns and Their Families
DeWayne M. Pursley, MD, MPH1,2; John A. F. Zupancic, MD, ScD1,2 June 18, 2020
Escalating US health care expenditures, including estimates that 20% to almost 50% of these costs involve processes, products, and services that do not improve outcomes, have brought renewed attention to the need to improve value in health care.1 Among the 6 waste categories outlined by Berwick and Hackbarth, there has been considerable focus on opportunities to reduce overtreatment, “the waste that comes from subjecting patients to care that… cannot possibly help them… rooted in outmoded habits, supply-driven behaviors, and ignoring science.”
Neonatal intensive care unit (NICU) services are at particularly high risk of overuse. Hospital and professional services reimbursements, reflecting the acute and highly technical nature of intensive care, are favorable and remain closely linked to admission volume and patient days in most regions. Both a legacy of intervention and a fear of litigation in caring for an at-risk population can also contribute to ineffective testing and treatments. The neonatology community is, however, starting to recognize the potential for improving care and controlling resource utilization. A 2015 study describing a systematic process to identify ineffective or harmful neonatal tests and treatments yielded a “Choosing Wisely Top Five” list in part to guide these efforts. In recent years, the neonatal care value literature has evolved to also focus more broadly on trends relating to NICU utilization—specifically, increasing admission rates and longer lengths of stay.
In the study by Braun et al,3 investigators from Kaiser Permanente share a population-based study describing a decline in NICU utilization—both admission rates and patient days—during a 9-year period. This is an important study, as it describes a trend that is counter to several recent reports of unexplained increasing NICU utilization, particularly for more mature and higher birth-weight infants, using a clinical rather than administrative data set. It is also important because the results may have been associated with several intercurrent performance improvement initiatives. Kaiser Permanente is a large, integrated health care system with a diverse population and a population-based financial payment structure and is in many ways uniquely suited (and motivated) to undertake a project to identify and characterize potential approaches to safely reduce neonatal care that is costly, may be ineffective, separates families, and is potentially harmful. The authors used a risk-adjustment model to ensure that the improvements were associated with postnatal care practices and not with changes in case mix reflecting patients less in need of acute neonatal care. They were also careful to include balancing measures, such as readmission and mortality, among the outcomes. Also important is the residual practice variation, which may hint at future opportunities for reduction in NICU utilization.
In the study by Braun et al, 12% of more than 300 000 liveborn infants were admitted to the NICU. Contrary to public perceptions of NICUs as prematurity colonies, more than two-thirds of these admissions were infants born after 34 weeks gestational age with birth weights more than 2000 g. The risk-adjusted NICU admission rate, accounting for socioeconomic, prenatal, and delivery room variables to control for independent factors that might affect admission or length of stay, decreased 25% over the study period to 10.9% of births, with 92% of the decline represented by infants with greater gestational age and higher birth weights. Importantly, these changes occurred without evidence of higher 30-day readmission or mortality rates.
There are compelling reasons that these results might not have been a random occurrence, as the health care system’s clinical leadership had implemented several concurrent performance improvement initiatives associated with decreased NICU admissions. A revised policy raised the threshold for NICU admission by lowering the gestational age (<35 weeks) and birth weight (<2000 g) for which well-appearing preterm infants were routinely admitted. A decision support tool based on individual infant estimates of early onset sepsis risk was introduced to guide laboratory testing and empirical antibiotic treatment. Finally, obstetric policies to decrease the rate of nonmedically indicated deliveries before 39 weeks of gestation and to reduce nonmedically indicated nulliparous, term, singleton, and vertex cesarean births were introduced.
The findings by Braun et al3 stand in contrast to a national trend documented in a 2015 population-based study. In that study using a public data set, birth-weight–specific NICU admission rates of US neonates were examined over a 6-year period (2007-2012). During this time, despite adjustment for maternal and neonatal characteristics, NICU admissions increased by 23%. These increases were generally represented by larger and less premature infants, such that by the end of the study period, most NICU admissions were for infants with birth weight more than 2500 g.
Although not population-based, observations by NICU member collaboratives, such as the California Perinatal Quality Care Collaborative and the Vermont-Oxford Network, have documented substantial variations in NICU admission and length-of-stay profiles. One California Perinatal Quality Care Collaborative study from 2018 observed that 79% of NICU admissions in 2015 were among infants born at or after 34 weeks gestation, while 10% of infants with 34 or more weeks gestation were admitted to the NICU. Schulman et al5 documented a 40-fold variation among member hospitals in the proportion of NICU admissions meeting high acuity definitions. In a Vermont-Oxford Network6 study involving approximately 500 000 infants hospitalized for nearly 10 million days in 381 NICUs from 2014 to 2016, 74% of NICU admissions were infants at 34 or more weeks gestation and only 15% of admissions met high acuity criteria. The proportion of admissions, patient days, high acuity, and short stays varied significantly both within and between different NICU types.
The origins of NICUs go back a half century, and NICUs have contributed substantially to reductions in US infant mortality during this time, a period during which rates of prematurity and low birth weight have actually increased. In 1967, the infant mortality rate was 22.4 per 1000 live births. Fifty years later, in 2017, the rate had declined to 5.8 per 1000 live births, a remarkable 74% reduction. Neonatal intensive care is highly effective and has achieved these outcomes and corresponding reductions in morbidity by mitigating the effects of prematurity, congenital anomalies, and pregnancy and perinatal complications. In the early days, NICUs were in short supply and public health entities mobilized to develop regionalized perinatal systems to ensure that obstetric and neonatal patients at high risk had access to specialized services when indicated. As the neonatology workforce and NICU bed capacity increased, hospitals and hospital systems, seeking to become full-service systems, contributed to deregionalization, and there was increasing reliance on economic forces to regulate growth and distribution. In some areas, infants at high risk were distributed more broadly, including to smaller, lower-level units, resulting in less favorable outcomes. Because NICUs are high-margin services, there are significant pressures to expand capacity and maintain volume. This can lead to overuse, including more frequent admission of infants at low risk or a failure to focus sufficiently on care practices that could potentially reduce demand.
There is a cost to these practices. Although NICUs are effective, they are also expensive. Health care system costs are largely borne by government and business, and unwarranted increases may potentially compromise funding of other essential services. Importantly, there may be hidden financial harms for families as well, including costs associated with transportation or lost work days. There are also risks. Short NICU stays by infants at low risk may interfere with breastfeeding, expose them to infection, or increase antibiotic exposure. Additionally, family-infant separation may contribute to emotional risk.
It is not clear that increases in short term, low acuity, and high gestational age and birth-weight NICU admissions have benefited these infants and their families. In fact, the study by Braun et al suggests that it may be possible to reverse these trends without compromising and even potentially enhancing care. Rigorous adoption of evidence-based clinical practices, such as use of early onset sepsis decision support and obstetric policies to reduce non-medically indicated early deliveries and low-risk cesarean delivery rates is a start. There is also a need to examine the opportunities demonstrated by the enormous variation in NICU utilization and in specific NICU practices. These include gestational age thresholds for NICU admission; preferred sites of clinical evaluation, intravenous placement, and antibiotic administration for well-appearing infants with sepsis risk; preferred sites for monitoring and treatment and guidance for length of treatment for opiate withdrawal; and duration of apnea monitoring of preterm infants nearing discharge.
Neonatal intensive care is one of the major achievements of the last half century, and it has resulted in substantial reductions in mortality and long-term morbidity that benefit infants at high risk, including those born to mothers at substantial social risk. If the neonatology community is to successfully achieve the Triple Aim goal for neonatal intensive care—improved neonatal health, better family experience, and reduced cost—we must intensify efforts to learn how to use NICUs more wisely.
Published: June 18, 2020. doi:10.1001/jamanetworkopen.2020.5693
Corresponding Author: DeWayne M. Pursley, MD, MPH, Department of Neonatology, Beth Israel Deaconess Medical Center, 330 Brookline Ave, Boston, MA 02215 (dpursley@bidmc.harvard.edu).
Source: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2767254

Why The Trauma Parents Experience In The NICU Follows Them Home
By COURTNEY COLLINS • FEB 14, 2020
Parents who’ve spent time in the neonatal intensive care unit (NICU) carry anxiety with them even after their baby is released.
The NICU’s constant barrage of doctors and beeping monitors is traumatic — and that trauma lingers.
Kepley Wakefield approaches life with typical 13-month-old vigor. A lot of smiling, excellent crawling acceleration and a fair amount of shrieking.
Her parents Courtney and Hollis Wakefield cherish her. They were by her side for each of the 95 days Kepley spent in the NICU.
“I had some bleeding at 21 weeks. So at that point, they put me on bed rest and we were having really difficult conversations,” Hollis said. “Viability is considered 24, so we had like two-and-a-half or three weeks to get through — which was a really, really scary time.”
Giving Birth At 24 Weeks
Hollis knew her pregnancy was going to be high risk. She was a 39-year-old cervical cancer survivor, so she and her wife had a plan for early labor. Even they weren’t prepared for delivery at 24 weeks, five days. But that’s when Kepley arrived, at 1 lb 10 ounces. The NICU team braced the Dallas couple for a long and frustrating road.
“They told us it would be like a roller coaster,” Hollis said. “They were like it’s going to be, you know, minute-to-minute some days. It’s not a straight line at all.”
Kepley started out in the NICU at UT-Southwestern’s Clements University Hospital, but eventually moved to the higher level NICU just down the road at Children’s Medical Center in Dallas. She was on a ventilator for three months.
When she was discharged, she still was tiny not even five pounds. She still needed supplementary oxygen and had weekly doctors appointments. Courtney says the stress from the NICU followed them home.
“I’m anxious all the time,” she said. “I have said, I have not been myself since Kepley was born.”
At-Home Risks
Because Kepley was born so early, her lungs weren’t fully developed. And because a ventilator helped her breathe for so long, those tiny lungs were also damaged. So even though Kepley is now thriving, flu season is a real threat. Her parents second guess every public outing, even quick trips to the store.
“And you’re thinking, do we risk it? Are we both going to be home where one of us could stay home?” Courtney said. “Just kind having to deal with that, even just for day-to-day tasks that we might normally bring a baby to. We’re having to kind of think twice.”
That’s not an overreaction. Doctors say catching a respiratory virus like RSV or the flu might put a premature baby right back in the hospital, which could re-traumatize those parents who’ve already spent time in the NICU.
Dr. Rashmin Savani is the chief of neonatal medicine at Children’s Health and UT Southwestern. He says even just the noise of endlessly beeping NICU monitors can overwhelm parents.
“The medical team and the nursing team they’re phenomenal, they understand what all these beeps are and when to respond, when to not respond.” Savani said. “But the family is bombarded with this sort of cacophony of alarms that are all designed to say ‘hey, pay attention to me.’ But for the family, it’s really scary.”
Children’s Health has a support crew in place to handle everything but the medicine. Every family has access to a team that includes a social worker, a psychologist and a chaplain.
‘Cutting The Umbilical Cord The Second Time’
Dr. Savani says Children’s Health also has a team devoted to helping a family transition to home — learning the ins and outs of complicated equipment and medication, as well as making sure the house is set up for a preemie, without the constant surveillance of doctors and nurses.
“And I actually call it you’re cutting the umbilical cord the second time,” he said. “And it’s a very scary thing for parents to go through.”
Hollis and Courtney Wakefield have been there. And while some things about caring for a preemie are old hat by now, they say some of those visceral NICU memories will never fade. There’s a visual reminder in the house too — a strand of colorful beads, so long it could wrap around Kepley’s tiny waist a dozen times. Courtney says each bead stands for something different Kepley went through in the NICU, for example: blood draws, surgeries and overnight stays.
One day, Kepley might decide to hang these beads on the wall — a memento of her earliest triumph.
For now though, she’s happy to use them as a teething toy.
Source: https://www.keranews.org/post/why-trauma-parents-experience-nicu-follows-them-home
WARRIORS:
Cultura de surf hecho en Chocó – Surf culture made in Chocó
Apr 10, 2017
Nestor Tello, Termales, Chocó, Colombia, 2015. Directed by Guillaume Parent y Sina Ribak Suport: masartemasaccion.org Fundación Buen Punto: clubdesurfdelchoco.com In this mini video series we meet with some persons from the Colombian Chocó region who live on the Pacific Coast, south of Nuquí. In Chocó exists a big contrast between the wealth of natural resources and the few opportunities of what we call development for its population. Same as in many rural areas in Colombia, corruption and violence are reality. Nevertheless, the visitor experiences an impression of freedom, tranquility and solidarity. Here, you (re-)connect with nature – you almost dissolve into it – and you feed on the philosophy and dreams of the Chocó people.
KAT’S CORNER

We need these articles to inspire, guide and support our precious community

Survival of the littlest: the long-term impacts of being born extremely early
![]()
Babies born before 28 weeks of gestation are surviving into adulthood at higher rates than ever, and scientists are checking in on their health.
Amber Dance- NEWS FEATURE – 02 JUNE 2020

Scientists are watching out for the health of adults born extremely premature, such as these people who took part in a photography project. Credit: Red Méthot
They told Marcelle Girard her baby was dead.
Back in 1992, Girard, a dentist in Gatineau, Canada, was 26 weeks pregnant and on her honeymoon in the Dominican Republic.
When she started bleeding, physicians at the local clinic assumed the baby had died. But Girard and her husband felt a kick. Only then did the doctors check for a fetal heartbeat and realize the baby was alive.
The couple was medically evacuated by air to Montreal, Canada, then taken to the Sainte-Justine University Hospital Center. Five hours later, Camille Girard-Bock was born, weighing just 920 grams (2 pounds).
Babies born so early are fragile and underdeveloped. Their lungs are particularly delicate: the organs lack the slippery substance, called surfactant, that prevents the airways from collapsing upon exhalation. Fortunately for Girard and her family, Sainte-Justine had recently started giving surfactant, a new treatment at the time, to premature babies.
After three months of intensive care, Girard took her baby home.
Today, Camille Girard-Bock is 27 years old and studying for a PhD in biomedical sciences at the University of Montreal. Working with researchers at Sainte-Justine, she’s addressing the long-term consequences of being born extremely premature — defined, variously, as less than 25–28 weeks in gestational age.
Families often assume they will have grasped the major issues arising from a premature birth once the child reaches school age, by which time any neuro-developmental problems will have appeared, Girard-Bock says. But that’s not necessarily the case. Her PhD advisers have found that young adults of this population exhibit risk factors for cardiovascular disease — and it may be that more chronic health conditions will show up with time.
Girard-Bock doesn’t let these risks preoccupy her. “As a survivor of preterm birth, you beat so many odds,” she says. “I guess I have some kind of sense that I’m going to beat those odds also.”
She and other against-the-odds babies are part of a population which is larger now than at any time in history: young adults who are survivors of extreme prematurity. For the first time, researchers can start to understand the long-term consequences of being born so early. Results are pouring out of cohort studies that have been tracking kids since birth, providing data on possible long-term outcomes; other studies are trialing ways to minimize the consequences for health.
These data can help parents make difficult decisions about whether to keep fighting for a baby’s survival. Although many extremely premature infants grow up to lead healthy lives, disability is still a major concern, particularly cognitive deficits and cerebral palsy.
Researchers are working on novel interventions to boost survival and reduce disability in extremely premature newborns. Several compounds aimed at improving lung, brain and eye function are in clinical trials, and researchers are exploring parent-support programmes, too.
Researchers are also investigating ways to help adults who were born extremely prematurely to cope with some of the long-term health impacts they might face: trialing exercise regimes to minimize the newly identified risk of cardiovascular disease, for example.
“We are really at the stage of seeing this cohort becoming older,” says neonatologist Jeanie Cheong at the Royal Women’s Hospital in Melbourne, Australia. Cheong is the director of the Victorian Infant Collaborative Study (VICS), which has been following survivors for four decades. “This is an exciting time for us to really make a difference to their health.”
The late twentieth century brought huge changes to neonatal medicine. Lex Doyle, a paediatrician and previous director of VICS, recalls that when he started caring for preterm infants in 1975, very few survived if they were born at under 1,000 grams — a birthweight that corresponds to about 28 weeks’ gestation. The introduction of ventilators, in the 1970s in Australia, helped, but also caused lung injuries, says Doyle, now associate director of research at the Royal Women’s Hospital. In the following decades, doctors began to give corticosteroids to mothers due to deliver early, to help mature the baby’s lungs just before birth. But the biggest difference to survival came in the early 1990s, with surfactant treatment.
“I remember when it arrived,” says Anne Monique Nuyt, a neonatologist at Sainte-Justine and one of Girard-Bock’s advisers. “It was a miracle.” Risk of death for premature infants dropped to 60–73% of what it was before.
Today, many hospitals regularly treat, and often save, babies born as early as 22–24 weeks. Survival rates vary depending on location and the kinds of interventions a hospital is able to provide. In the United Kingdom, for example, among babies who are alive at birth and receiving care, 35% born at 22 weeks survive, 38% at 23 weeks, and 60% at 24 weeks.
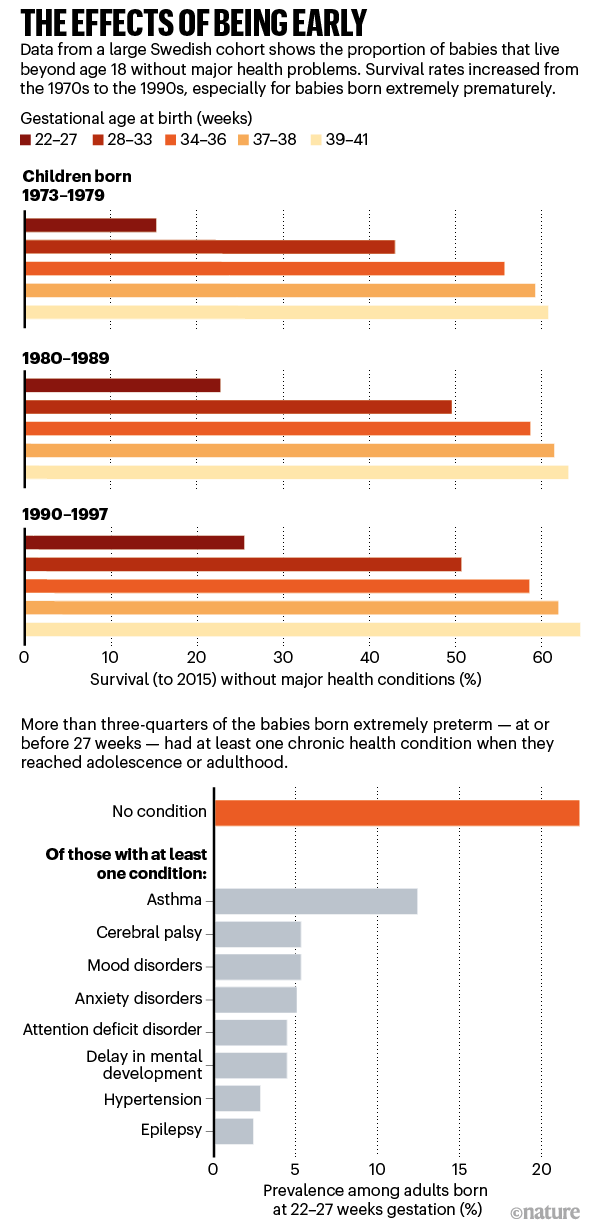
For babies who survive, the earlier they are born, the higher the risk of complications or ongoing disability (see ‘The effects of being early’). There is a long list of potential problems — including asthma, anxiety, autism spectrum disorder, cerebral palsy, epilepsy and cognitive impairment — and about one-third of children born extremely prematurely have one condition on the list, says Mike O’Shea, a neonatologist at the University of North Carolina School of Medicine in Chapel Hill, who co-runs a study tracking children born between 2002 and 2004. In this cohort, another one-third have multiple disabilities, he says, and the rest have none.
“Preterm birth should be thought of as a chronic condition that requires long-term follow-up,” says Casey Crump, a family physician and epidemiologist at the Icahn School of Medicine at Mount Sinai in New York, who notes that when these babies become older children or adults, they don’t usually get special medical attention. “Doctors are not used to seeing them, but they increasingly will.”
Outlooks for earlies
What should doctors expect? For a report in the Journal of the American Medical Association last year, Crump and his colleagues scraped data from the Swedish birth registry. They looked at more than 2.5 million people born from 1973 to 1997, and checked their records for health issues up until the end of 2015.
Of the 5,391 people born extremely preterm, 78% had at least one condition that manifested in adolescence or early adulthood, such as a psychiatric disorder, compared with 37% of those born full-term. When the researchers looked at predictors of early mortality, such as heart disease, 68% of people born extremely prematurely had at least one such predictor, compared with 18% for full-term births — although these data include people born before surfactant and corticosteroid use were widespread, so it’s unclear if these data reflect outcomes for babies born today. Researchers have found similar trends in a UK cohort study of extremely premature births. In results published earlier this year, the EPICure study team, led by neonatologist Neil Marlow at University College London, found that 60% of 19-year-olds who were extremely premature were impaired in at least one neuropsychological area, often cognition.
Such disabilities can impact education as well as quality of life. Craig Garfield, a paediatrician at the Northwestern University Feinberg School of Medicine and the Lurie Children’s Hospital of Chicago, Illinois, addressed a basic question about the first formal year of schooling in the United States: “Is your kid ready for kindergarten, or not?”
To answer it, Garfield and his colleagues analysed standardized test scores and teacher assessments on children born in Florida between 1992 and 2002. Of those born at 23 or 24 weeks, 65% were considered ready to start kindergarten at the standard age, 5–6 years old, with the age adjusted to take into account their earlier birth. In comparison, 85.3% of children born full term were kindergarten-ready.
Despite their tricky start, by the time they reach adolescence, many people born prematurely have a positive outlook. In a 2006 paper, researchers studying individuals born weighing 1,000 grams or less compared these young adults’ perceptions of their own quality of life with those of peers of normal birth-weight — and, to their surprise, found that the scores were comparable. Conversely, a 2018 study8 found that children born at less than 28 weeks did report having a significantly lower quality of life. The children, who did not have major disabilities, scored themselves 6 points lower, out of 100, than a reference population.
As Marlow spent time with his participants and their families, his worries about severe neurological issues diminished. Even when such issues are present, they don’t greatly limit most children and young adults. “They want to know that they are going to live a long life, a happy life,” he says. Most are on track to do so. “The truth is, if you survive at 22 weeks, the majority of survivors do not have a severe, life-limiting disability.”
Breathless
But scientists have only just begun to follow people born extremely prematurely into adulthood and then middle age and beyond, where health issues may yet lurk. “I’d like scientists to focus on improving the long-term outcomes as much as the short-term outcomes,” says Tala Alsadik, a 16-year-old high-school student in Jeddah, Saudi Arabia.
When Alsadik’s mother was 25 weeks pregnant and her waters broke, doctors went so far as to hand funeral paperwork to the family before consenting to perform a caesarean section. As a newborn, Alsadik spent three months in the neonatal-intensive-care unit (NICU) with kidney failure, sepsis and respiratory distress.
The complications didn’t end when she went home. The consequences of her prematurity are on display every time she speaks, her voice high and breathy because the ventilator she was put on damaged her vocal cords. When she was 15, her navel unexpectedly began leaking yellow discharge, and she required surgery. It turned out to be caused by materials leftover from when she received nutrients through a navel tube.
That certainly wasn’t something her physicians knew to check for. In fact, doctors don’t often ask if an adolescent or adult patient was born prematurely — but doing so can be revealing.
Charlotte Bolton is a respiratory physician at the University of Nottingham, UK, where she specializes in patients with chronic obstructive pulmonary disease (COPD). People coming into her practice tend to be in their 40s or older, often current or former smokers. But in around 2008, she began to notice a new type of patient being referred to her owing to breathlessness and COPD-like symptoms: 20-something non-smokers.
Quizzing them, Bolton discovered that many had been born before 32 weeks. For more insight, she got in touch with Marlow, who had also become concerned about lung function as the EPICure participants aged. Alterations in lung function are a key predictor of cardiovascular disease, the leading cause of death around the world. Clinicians already knew that after extremely premature birth, the lungs often don’t grow to full size. Ventilators, high oxygen levels, inflammation and infection can further damage the immature lungs, leading to low lung function and long-term breathing problems, as Bolton, Marlow and their colleagues showed in a study of 11-year-olds.
VICS research backs up the cardiovascular concerns: researchers have observed diminished airflow in 8-year-olds, worsening as they aged, as well as high blood pressure in young adults. “We really haven’t found the reason yet,” says Cheong. “That opens up a whole new research area.”
At Sainte-Justine, researchers have also noticed that young adults who were born at 28 weeks or less are at nearly three times the usual risk of having high blood pressure. The researchers figured they would try medications to control it. But their patient advisory board members had other ideas — they wanted to try lifestyle interventions first.
The scientists were pessimistic as they began a pilot study of a 14-week exercise programme. They thought that the cardiovascular risk factors would be unchangeable. Preliminary results indicate that they were wrong; the young adults are improving with exercise.
Girard-Bock says the data motivate her to eat healthily and stay active. “I’ve been given the chance to stay alive,” she says. “I need to be careful.”
From the start
For babies born prematurely, the first weeks and months of life are still the most treacherous. Dozens of clinical trials are in progress for prematurity and associated complications, some testing different nutritional formulas or improving parental support, and others targeting specific issues that lead to disability later on: underdeveloped lungs, brain bleeds and altered eye development.
For instance, researchers hoping to protect babies’ lungs gave a growth factor called IGF-1 — which the fetus usually gets from its mother during the first two trimesters of pregnancy — to premature babies in a phase II clinical trial reported in 2016. Rates of a chronic lung condition that often affects premature babies halved, and babies were somewhat less likely to have a severe brain hemorrhage in their earliest months.
Another concern is visual impairment.
Retina development halts prematurely when babies born early begin breathing oxygen. Later it restarts, but preterm babies might then make too much of a growth factor called VEGF, causing over-proliferation of blood vessels in the eye, a disorder known as retinopathy. In a phase III trial announced in 2018, researchers successfully treated 80% of these retinopathy cases with a VEGF-blocking drug called ranibizumab, and in 2019 the drug was approved in the European Union for use in premature babies.
Some common drugs might also be of use: paracetamol (acetaminophen), for example, lowers levels of biomolecules called prostaglandins, and this seems to encourage a key fetal vein in the lungs to close, preventing fluid from entering the lungs.
But among the most promising treatment programmes, some neonatologists say, are social interventions to help families after they leave the hospital. For parents, it can be nerve-racking to go it alone after depending on a team of specialists for months, and lack of parental confidence has been linked to parental depression and difficulties with behaviour and social development in their growing children.
At Women & Infants Hospital of Rhode Island in Providence, Betty Vohr is director of the Neonatal Follow-Up Program. There, families are placed in private rooms, instead of sharing a large bay as happens in many NICUs. Once they are ready to leave, a programme called Transition Home Plus helps them to prepare and provides assistance such as regular check-ins by phone and in person in the first few days at home, and a 24/7 helpline. For mothers with postnatal depression, the hospital offers care from psychologists and specialist nurses.
The results have been significant, says Vohr. The single-family rooms resulted in higher milk production by mothers: 30% more at four weeks than for families in more open spaces. At 2 years old, children from the single-family rooms scored higher on cognitive and language tests. After Transition Home Plus began, babies discharged from the NICU had lower health-care costs and fewer hospital visits — issues that are of great concern for premature infants. Other NICUs are developing similar programmes, Vohr says.
With these types of novel intervention, and the long-term data that continue to pour out of studies, doctors can make better predictions than ever before about how extremely premature infants will fare. Although these individuals face complications, many will thrive.
Alsadik, for one, intends to be a success story. Despite her difficult start in life, she does well academically, and plans to become a neonatologist. “I, also, want to improve the long-term outcomes of premature birth for other people.”
Source:https://www.nature.com/articles/d41586-020-01517-z
Cloud Surfing Roldanillo, Colombia in a Paraglider
Jan 30, 2017 Jonathan Kelley
Cloud Surfing Roldanillo, Colombia in a paraglider in January 2017




