

NORWAY


PRETERM BIRTH RATES – NORWAY
Rank: 172 –Rate: 6.0% Estimated # of preterm births per 100 live births
(USA – 12 %, Global Average: 11.1%)
Norway, officially the Kingdom of Norway, is a Nordic country in Northern Europe, the mainland territory of which comprises the western and northernmost portion of the Scandinavian Peninsula. The remote Arctic island of Jan Mayen and the archipelago of Svalbard also form part of Norway. Bouvet Island, located in the Subantarctic, is a dependency of Norway; it also lays claims to the Antarctic territories of Peter I Island and Queen Maud Land. The capital and largest city in Norway is Oslo.
Norway has a total area of 385,207 square kilometres (148,729 sq mi) and had a population of 5,425,270 in January 2022.[14] The country shares a long eastern border with Sweden at a length of 1,619 km (1,006 mi). It is bordered by Finland and Russia to the northeast and the Skagerrak strait to the south, on the other side of which are Denmark and the United Kingdom. Norway has an extensive coastline, facing the North Atlantic Ocean and the Barents Sea. The maritime influence dominates Norway’s climate, with mild lowland temperatures on the sea coasts; the interior, while colder, is also a lot milder than areas elsewhere in the world on such northerly latitudes. Even during polar night in the north, temperatures above freezing are commonplace on the coastline. The maritime influence brings high rainfall and snowfall to some areas of the country.
Health
Norway was awarded first place according to the UN’s Human Development Index (HDI) for 2013. In the 1800s, by contrast, poverty and communicable diseases dominated in Norway together with famines and epidemics. From the 1900s, improvements in public health occurred as a result of development in several areas such as social and living conditions, changes in disease and medical outbreaks, establishment of the health care system, and emphasis on public health matters. Vaccination and increased treatment opportunities with antibiotics resulted in great improvements within the Norwegian population. Improved hygiene and better nutrition were factors that contributed to improved health.
The disease pattern in Norway changed from communicable diseases to non-communicable diseases and chronic diseases as cardiovascular disease. Inequalities and social differences are still present in public health in Norway today.
In 2013 the infant mortality rate was 2.5 per 1,000 live births among children under the age of one. For girls it was 2.7 and for boys 2.3, which is the lowest infant mortality rate for boys ever recorded in Norway.
Source:https://en.wikipedia.org/wiki/Norway

COMMUNITY

Ten Years of Neonatal Intensive Care Adaption to the Infants’ Needs: Implementation of a Family-Centered Care Model with Single-Family Rooms in Norway
Lene Tandle Lyngstad 1, Flore Le Marechal 1, Birgitte Lenes Ekeberg1, Krzysztof Hochnowski 1, Mariann Hval 1, Bente Silnes Tandberg1

International Journal of Environmental Research and Public Health 13 May 2022, 19(10):5917
DOI: 10.3390/ijerph19105917 PMID: 35627454 PMCID: PMC9140644
Abstract
Ten years ago, the Neonatal intensive care unit in Drammen, Norway, implemented Single-Family Rooms (SFR), replacing the traditional open bay (OB) unit. Welcoming parents to stay together with their infant 24 h per day, seven days per week, was both challenging and inspiring. The aim of this paper is to describe the implementation of SFR and how they have contributed to a cultural change among the interprofessional staff. Parents want to participate in infant care, but to do so, they need information and supervision from nurses, as well as emotional support. Although SFR protect infants and provide private accommodation for parents, nurses may feel isolated and lack peer support.
Our paper describes how we managed to systematically reorganize the nurse’s workflow by using a Plan-Do-Study-Act (PDSA) cycle approach. Significant milestones are identified, and the implementation processes are displayed. The continuous parental presence has changed the way we perceive the family as a care recipient and how we involve the parents in daily care. We provide visions for the future with further developments of care adapted to infants’ needs by providing neonatal intensive care with parents as equal partners.
FULL ARTICLE: http://europepmc.org/article/MED/35627454

Sigrid, Bring Me The Horizon – Bad Life



The RHODĒ Study
Rhode Island Cohort Of Adults Born Prematurely
The Rhode Island Cohort Of Adults Born Prematurely — or “RHODĒ” Study — is a longitudinal study following a group of 215 infants born between 1985-1989 in Rhode Island. The study was previously known as the Infant Development Study. Prior waves of data collection occurred at birth, 1 month, 18 months, 30 months, 4 years, 8 years, 12 years, 17 years, and 23 years of age. The 215 originally enrolled infants represent a wide range of gestational ages, birth weights, and illness severity, and includes both preterm and full-term participants.
In response to an Institute of Medicine recommendation for long-term outcome studies for premature infants into young adulthood, we are currently conducting the tenth wave of the study, with participants aged 30-35 years old.
We are fortunate to have retained 96% of the participant sample between ages 17 and 23 years, and 85% since birth. To our knowledge, this is the only U.S. based study to follow preterm and full-term participants from birth into age 30.
Source: https://www.rhodestudy.com/

INNOVATIONS

‘Smart pacifier’ in development with help from WSU Vancouver researchers:2701:45
Clinical trials are still to come, but the academic group hopes the small medical device eventually replaces blood draws, and a lot of wires and electrodes.
Author: kgw.com Published: 5:43 PM PDT June 11, 2022 Updated: 5:43 PM PDT June 11, 2022


Comparison of the effect of two methods of sucking on pacifier and mother’s finger on oral feeding behavior in preterm infants: a randomized clinical trial
Fatemeh Shaki, Parvin Aziznejadroshan, Zahra Akbarian Rad,
Mohammad Chehrazi & Afsaneh Arzani
BMC Pediatrics volume 22, Article number: 292 (2022)

Abstract
Background
Oral feeding problems will cause long-term hospitalization of the infant and increase the cost of hospitalization. This study aimed to compare the effect of two methods of sucking on pacifier and mother’s finger on oral feeding behavior in preterm infants.
Methods
This single-blind randomized controlled clinical trial was performed in the neonatal intensive care unit of Babol Rouhani Hospital, Iran. 150 preterm infants with the gestational age of 31 to 33 weeks were selected and were divided into three groups of 50 samples using randomized block method, including non-nutritive sucking on mother’s finger (A), pacifier (B) and control (C). Infants in groups A and B were stimulated with mother’s finger or pacifier three times a day for five minutes before gavage, for ten days exactly. For data collection, demographic characteristics questionnaire and preterm infant breastfeeding behavior scale were used.
Results
The mean score of breastfeeding behavior in preterm infants in the three groups of A,B,C was 12.34 ± 3.37, 11.00 ± 3.55, 10.40 ± 4.29 respectively, which had a significant difference between the three groups (p = 0.03). The mean rooting score between three groups of A, B, and C was 1.76 ± 0.47, 1.64 ± 0.48, and 1.40 ± 0.90 (p < 0.001) respectively. Also, the mean sucking score in groups of A, B and C was 2.52 ± 0.76, 2.28 ± 0.64 and 2.02 ± 0.74 respectively, which had a significant difference (p = 0.003), but other scales had no significant difference between the three groups (P > 0.05). The mean time to achieve independent oral feeding between the three groups of A, B, C was 22.12 ± 8.15, 22.54 ± 7.54 and 25.86 ± 7.93 days respectively (p = 0.03), and duration of hospitalization was 25.98 ± 6.78, 27.28 ± 6.20, and 29.36 ± 5.97 days (p = 0.02), which had a significant difference. But there was no significant difference between the two groups of A and B in terms of rooting, sucking, the total score of breastfeeding behavior and time of achieving independent oral feeding (P > 0.05).
Conclusion
Considering the positive effect of these two methods, especially non-nutritive sucking on mother’s finger, on increasing oral feeding behaviors, it is recommended to implement these low-cost methods for preterm infants admitted to neonatal intensive care unit.
Source:https://bmcpediatr.biomedcentral.com/articles/10.1186/s12887-022-03352-9

EFCNI involved in new study on blood transfusions in preterm babies

POSTED ON 11 MAY 2022
Most preterm babies admitted to a Neonatal Intensive Care Unit (NICU) receive blood transfusions. Some neonates, however, receive blood transfusions even though these transfusions may not be necessary, cause side effects or even harm. Therefore, the International Neonatal tranSfusion PoInt pREvalence study (INSPIRE) aims to describe the current state and indications for blood transfusions among preterm babies in Europe.
Although most preterm babies receive blood transfusions in the NICU, there are no international guidelines that have been incorporated into clinical practice, and there is significant variation in blood transfusion practice within Europe. Additionally, high-quality data on neonatal transfusion practice in Europe is lacking. The INSPIRE-study will describe current neonatal transfusion practices within Europe. These results will help to improve practice, develop future clinical studies, and inform guideline writing. Additionally, the results may help to reduce unnecessary transfusions through increased awareness of the proper use of transfusions in this vulnerable patient group.
In collaboration with the Neonatal Transfusion Network (NTN), EFCNI coordinates an international parental advisory board (PAB). The PAB is chaired by EFCNI and meets on a regular basis throughout the duration of the project. Furthermore, EFCNI gives advice and provides input on topics related to ethics and patient information throughout the project.
Ongoing updates on the project can also be found on our project page.

Current Status and Future Directions of Neuromonitoring With Emerging Technologies in Neonatal Care

Gabriel Fernando Todeschi Variane1,2,3*, João Paulo Vasques Camargo2,4, Daniela Pereira Rodrigues2,5, Maurício Magalhães1,2,6 and Marcelo Jenné Mimica7,8
Neonatology has experienced a significant reduction in mortality rates of the preterm population and critically ill infants over the last few decades. Now, the emphasis is directed toward improving long-term neurodevelopmental outcomes and quality of life. Brain-focused care has emerged as a necessity. The creation of neonatal neurocritical care units, or Neuro-NICUs, provides strategies to reduce brain injury using standardized clinical protocols, methodologies, and provider education and training. Bedside neuromonitoring has dramatically improved our ability to provide assessment of newborns at high risk. Non-invasive tools, such as continuous electroencephalography (cEEG), amplitude-integrated electroencephalography (aEEG), and near-infrared spectroscopy (NIRS), allow screening for seizures and continuous evaluation of brain function and cerebral oxygenation at the bedside. Extended and combined uses of these techniques, also described as multimodal monitoring, may allow practitioners to better understand the physiology of critically ill neonates. Furthermore, the rapid growth of technology in the Neuro-NICU, along with the increasing use of telemedicine and artificial intelligence with improved data mining techniques and machine learning (ML), has the potential to vastly improve decision-making processes and positively impact outcomes. This article will cover the current applications of neuromonitoring in the Neuro-NICU, recent advances, potential pitfalls, and future perspectives in this field.
Full Article: https://www.frontiersin.org/articles/10.3389/fped.2021.755144/full

Accuracy and Completeness of Intermediate-Level Nursery Descriptions on Hospital Websites
David C. Goodman, MD, MS1,2,3,4; Timothy J. Price, MS1; David Braun, MD5,6
JAMA Netw Open. 2022;5(6):e2215596. doi:10.1001/jamanetworkopen.2022.15596
Key Points
Question How completely and accurately do hospital websites describe their level II special care (ie, intermediate care) nurseries?
Findings In this cross-sectional study of hospital nurseries (including 1.99 million live births and 268 level II units) in 10 large US states that regulate nursery levels of care, state-designated intermediate (ie, level II) units were inaccurately or incompletely described in 39% and 25% of the hospital websites, respectively. There was substantial and statistically significant variation in rates of incompleteness and inaccuracy across states.
Meaning These results suggest that hospital websites, often the only source of publicly available information describing a hospital’s neonatal unit, do not provide reliable information for prospective parents, referring physicians, and the public to assess the capacity to care for ill newborns.
Abstract
Importance Birth at hospitals with an appropriate level of neonatal intensive care units is associated with better neonatal outcomes. The primary sources for information about hospital neonatal unit levels for prospective parents, referring physicians, and the public are hospital websites, but the accuracy of neonatal unit capacity is unclear.
Objective To determine if hospital websites accurately report the capabilities of intermediate (ie, level II) units, which are intended for care of newborns with low to moderate illness levels or the stabilization of newborns prior to transfer.
Design, Setting, and Participants This cross-sectional study compared descriptions of level II unit capabilities on hospital web pages in 10 large states with their respective state-level designation. Analyzed units were located in the 10 states with the highest number of live births in 2019 (excluding states with no level II regulations) and had active websites as of May 2021.
Main Outcomes and Measures Hospital websites were assessed for whether there was any mention of the unit, the description of the unit was provided, the unit was identified as a level III or both levels II and III, the terms “neonatal intensive care unit” or “NICU” were used without indicating limits in care available or newborn acuity, or the unit was claimed to provide the most advanced level of care.
Results A total 28 states had no regulation of nursery unit levels; in the 10 large, regulated states, web descriptions of level II units were incomplete for 39.2% of hospitals (95% CI, 33.3%-45.3%) and inaccurate for 24.6% (95% CI, 19.6%-30.2%). Within incomplete descriptions, 2.6% (95% CI, 1.1%-5.3%) of hospitals did not mention an advanced care unit and 22.0% (95% CI, 17.2%-27.5%) identified a level II unit without providing further description. Within inaccurate descriptions, 25.4% (95% CI, 20.3%-31.0%) of hospitals described the unit as a “neonatal intensive care unit” or “NICU” without any qualification and 9.3% (95% CI, 6.3%-13.5%) claimed that the unit provided the most advanced neonatal care or care to the sickest newborns; 3.0% of hospitals (95% CI, 1.3%-6.0%) stated that their unit was level III and 1.5% (95% CI, 0.4%-3.8%) as level II and III. Across states there was substantial variation in rates of incompleteness and inaccuracy.
Conclusions and Relevance Incomplete and inaccurate hospital web descriptions of intermediate newborn care units are common. These deficits can mislead parents, clinicians, and the public about the appropriateness of a hospital for sick newborns, which raises important ethical questions.
Source:https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2793015

PREEMIE FAMILY PARTNERS

Turns out not where but who you’re with that really matters

Terrie Eleanor Inder Pediatric Research volume 88, pages533–534 (2020)
An understanding of the impact of the environment, including the new enhanced single-family room (SFR) structure, on outcomes in the preterm infant is critical. The study by van Veenendaal et al. in this edition of Pediatric Research expands on others’ work by analyzing a level II neonatal facility SFR setting and concludes that the SFR environment was associated with lower rates of late onset sepsis, mediated by the lower use of intravenous and central venous catheters. The authors hypothesized that the presence of parents, who know their infants well, may have resulted in less antibiotic treatment for symptoms and signs that were interpreted by less familiar medical caregivers as concerning for late onset sepsis. It is important to note that the definition of “sepsis” included any culture positive infant, independent of treatment, and infants treated for ≥7 days with antibiotics after clinical signs of concern for sepsis with negative cultures.
This study compared two epochs from 2012−2014 and 2017−2018 with 1046 infants who were predominantly level II late preterm infants (<37 weeks’ gestation and hospital stay ≥3 days) with average gestational age of 34−35 weeks. During this time of change to SFR environment, Family Integrated Care (FICare) was also introduced with parents being present to provide most of the care for their infants. Their SFR included a full parent bed for the parent to live and sleep in the room with their infant. The major mediator of the reduction in late onset sepsis, from 9.3% in the open bay to 5.3% in the SFR, was an approximately 50% reduction in vascular lines (peripheral and central) and use of parenteral nutrition. Although the reasons for the reduction in line use remain unclear, the authors hypothesized that the presence of the parents resulted in joint decision making and avoidance of painful procedures—both leading to reduced lines and parenteral nutrition. The authors also report a trend toward higher exclusive breastfeeding at discharge and a shorter length of stay.
Although infection rates in the neonatal intensive care unit have been consistently falling over the last two decades, this study informs us that in a less intensively sick population of infants, the SFR environment may reduce the risk of late onset sepsis. Importantly, they define that the association is mediated by invasive vascular access, which may be avoided with parental engagement. This study did not evaluate early breast milk supply in the new SFR setting, but others have noted in a similarly designed study a significant increase in the availability of human milk in the SFR environment being a key driver of SFR-associated improved neurodevelopmental outcomes.
In contrast to the current study, a study from a typical larger neonatal intensive care unit setting in Texas, USA, found an increased rate of sepsis documented following their renovation to SFR environment in 2015. They analyzed 9995 encounters in their 90-bed unit, with a trend toward increased sepsis rates in the SFR in the moderately preterm infant (OR 1.33, 95% CI 0.7−3.3) that reached significance in the term/post-term infant (OR 1.79, 95% CI 1.2−3.3). It was noted that the trend was reversed toward lower infection rates in the preterm infants <32 weeks. Their definition of sepsis was based on medical records alone and not as carefully curated as the current study.
Single-family room environments have been noted to have numerous advantages, including enhancing parent−infant closeness and engagement in infant care and improved parental psychological wellbeing with reductions in maternal depression and parental stress in both parents. In these studies, based in Scandinavia, parents in the SFR were present 21 h/day compared with 7 h/day previously in the open bay unit. The SFR environment has also been associated with improved neurodevelopmental outcomes following discharge, with an approximate 3-point advantage in cognitive and language scores on Bayley III at 18−24 months. However, in our own neonatal intensive care unit setting in St. Louis, we documented a negative impact of SFR with lower language scores (−8.3 (95% CI −2.4 to 14.2), p = 0.006) and a strong trend toward worsening motor scores at 24 months follow-up. We attributed this to the sensory isolation within the SFR environment if the parental presence and engagement was low. A subsequent study in the same unit in St. Louis by Dr. Pineda’s team demonstrated that the average presence of parents was higher in the SFR environment at 3.6 h/day compared to 2.4 h/day in the open bay environment. Notably, mothers reported more NICU stress in the SFR environment.
A recent meta-analysis of 13 study populations (n = 4793) concluded that there was no clear difference between room environments in cognitive neurodevelopment on the Bayley Scales of Infant and Toddler Development-III at 18–24 months (680 infants analyzed; mean difference 1.04 [95% CI −3.45 to 5.52], p = 0·65; I2 = 42%). However, the authors did note a lower incidence of sepsis (4165 infants analyzed; 108,035 days in hospital [hospitalization days]; risk ratio 0.63 [95% CI 0.50−0.78], p < 0·0001; I2 = 0%) and higher rates of exclusive breastfeeding at discharge (484 infants analyzed; 1.31 [1.07−1.61], p = 0.01; I2 = 0%) in SFRs than in open bay units. No other differences in neonatal outcomes were noted. This meta-analysis combined Scandinavian, Australian, and USA studies.
Differences in these studies point to a clear explanation—it is “not where but who you’re with that really matters” (the lyrics from “The Best of What’s Around” by the Dave Mathews Band). In the studies documenting benefit from the SFR environment, parental presence is almost universal and routinely >12 h in duration with shared decision making. The current study adds to this literature by documenting that such parental engagement may assist in both prevention of invasive vascular devices, that are associated with increased sepsis, and more informed interpretation of their infant’s clinical signs to better define the risk of sepsis. In the current study, it is not possible to untangle the effects of the SFR from the FICare model, with both promoting the presence and engagement of the family in care decisions. It appears that it is this critical combination that renders the benefits seen in this and other studies of the SFR, predominantly reported from Scandinavia.
In contrast, the studies documenting the adverse effects from the SFR environment, typically studies in the settings of large urban NICUs within the USA, parental presence averaged <4 h/day. Although this was increased compared to the open bay environment, it appeared associated with greater NICU stress in the mothers with both greater adult and infant isolation. Thus, without a structured program of parental support and engagement with their infant and shared decision making, this modest increase in parental presence may not offset the deficit in human language exposure which appears critical during the third trimester for language development.
In conclusion, although much effort has been focused on the room type, it appears more pertinent to ask what is happening in any space in which an infant is being cared for in the neonatal intensive care unit. This appears just as relevant for shorter lengths of stay, as shown by the current study. It is worthy of note that it is common for medical rounds or records to lack any systematic documentation or summary review of the nature of the parent’s presence or engagement, other than to discuss in a socially cursory manner. The SFR encourages greater presence of the parents to be “living” with their infant, enabling a family-centered model of care, with the combination in many studies resulting in reduced sepsis, enhanced human milk production, improved parental mental health and attachment and improved infant neurodevelopmental outcomes. To achieve the presence of parents for >12 h, and ideally 24 h/day, in the setting of the USA will require firm advocacy from the neonatal community as a fundamentally important facet of care. It is no longer “nice to have” but a “necessary element of care” for optimal outcomes. The provision of paid parental leave during the time of an infant’s neonatal intensive care course for both parents should be federally mandated as medically necessary, and we must fight for our infants’ right to their parent’s presence. The SFR environment greatly assists parents and staff with such a model of family-centered care but it is only a facilitator of the true key—the parents.
Source:https://www.nature.com/articles/s41390-020-1040-1

Preemies at greater risk for mortality in adulthood
By Svein Inge Meland – Published 23.03.2021

*** It’s important to remember that most people who are born prematurely do well, and that treatment and follow-up are constantly improving, says Professor Kari Risnes at NTNU.
The risk of dying from heart disease, chronic lung disease or diabetes in adulthood is twice as high for preemies —premature infants — as for the general population. Even those who were born just two to three weeks before term have a slightly increased risk.
A new study of mortality among young adults who were premature infants includes 6.3 million adults under the age of 50 in Norway, Sweden, Finland and Denmark. Among this group, 5.4 per cent were preemies, or born before term, according to Professor Kari Risnes at NTNU’s Department of Clinical and Molecular Medicine and St. Olavs Hospital.
Researchers used the national birth registers and compared them with the cause of death registers that all Scandinavian countries have.
“We already know that preemies have increased mortality in childhood and early adulthood. Now we’ve confirmed the risk of death from chronic diseases such as heart disease, lung disease and diabetes before the age of 50,” says Risnes.
Normal cancer and stroke risk
The study shows that the risk of preemies dying before the age of 50 is 40 per cent higher than for the population as a whole. Researchers found that the risk of dying for individuals born before full gestation and who have chronic heart disease, lung disease or diabetes is twice that of the population as a whole. However, this group has no increased risk of death from cancer and stroke.
“We were surprised to see that the risk of death was higher even in people who were born as late as weeks 37 and 38, only a few weeks before full gestation. Although the extra risk was only about 10 per cent, this group makes up about 15 per cent of all births, and we have to try to map the causal relationships here,” says the paediatrician.
Findings should be factored in
Risnes believes that the results from the study should be factored in when doctors assess the patient’s risk of disease and their preventive advice for the patient.
“Our idea is that we should increase awareness in both the general population and among doctors so that the risk can be reduced. We need to recognize that prematurity is a factor to take into account when assessing risk, just like we do with a family history of heart disease, obesity or smoking,” says Risnes.
“It’s important to be aware of additional factors that increase the risk of cardiovascular disease and diabetes, like high blood pressure, obesity, inactivity and high blood sugar, plus the high levels of all these additional factors that we see more of in premature births,” she says.
Early prevention important
“These diseases are often preventable. Good treatment is important and can often be longterm to maintain a good quality of life and avoid illness and death. We should be identifying lifestyle changes from an early age that reduce the risks, like more physical activity and avoiding obesity and smoking,” says Risnes.
One question still to be answered is whether more premature than full-term infants develop these chronic diseases, or if they are just generally less well equipped to survive the diseases.
“We need to try to address this question in the next round of research. It may be that the diseases crop up earlier in premature babies. We don’t have data on this yet,” Risnes says.
In the 1960s and 1970s, only 20 to 30 per cent of the most premature infants reached 15 years of age. Today, their survival rate is over 90 per cent. This means that the strong ones, the survivors, were preemies in Risne’s study of adults.
“With better neonatal medicine, the proportion of the population born prematurely is growing,” says Risne. She believes it will be important to follow this population closely in terms of risk. In the study, individuals born prematurely around 1980 had a slightly higher risk of cardiovascular disease than those born around 1970.
Not genetics or environment
The study doesn’t indicate that the social status of the mother or conditions of upbringing explain the increased risk of mortality. The researchers compared siblings to find out if the excess mortality was due to genetics or socioeconomic conditions.
“We found that risk of death for these diseases was higher for people born prematurely — preemies — than for their full-term siblings. We concluded that the increased risk can’t be fully explained by genes, which siblings have in common, or by socio-economic conditions and living conditions in childhood,” says Risnes.
Most common diseases
Dying in the first 50 years of life is rare. For 30-year-olds, the risk of dying is one in 1 000 per year, for 50-year-olds the risk rises to two in 1 000. Chronic diseases make up a minor percentage of these deaths. The researchers in the EU study chose to look at cancer, heart disease, stroke, chronic lung disease and diabetes because these are the most common chronic diseases that can be fatal.
In the past, it has been difficult to access other nations’ health databases. Risnes is very happy that such access was possible for this study. Robust results are easier to attain with such a large volume of health data. The findings of the study are consistent between countries.

Recognising a Grandparent’s Journey

FRIDAY, MAY 22, 2020
When a family travels the difficult journey of welcoming a premature or sick baby into the world, it isn’t just the parents or carers who are impacted.
The whole family feels the reality and shares in the emotions of the experience. None more so than grandparents. Grandparents are often an invisible casualty when a birth does not go to plan and ends in an emergency delivery and admission to the NICU. Grandparents are part of a common phenomenon where there’s a double concern for both the newborn grandchild, and their adult child who is managing this stressful event physically, mentally, and emotionally.
While Grandparents are the most common support system for new parents, the hospital restrictions and fragile health of an NICU baby can create an imbalance of involvement and un-involvement, which is often difficult to avoid. Hence, grandparents may require great flexibility to help in other ways.
One common way to help is in the home, attending to the needs of the siblings, and supporting the family’s routine which is a huge and much-needed help. During this time grandparents provide new parents the opportunity to be with their baby and to also be part of the healthcare team. In a way, they become the scaffolding for parents to be in this very important position for the best outcome for their grandchild.
It’s important to also acknowledge the challenges for grandparents of babies in the hospital during COVID-19 who would have no involvement in the NICU and for some, possibly meeting this new baby for the first-time months later, once discharged. The restrictions that are put into place are there to protect the fragile health of the baby as well as protecting this particular age group from entering a building where patients are being treated for the COVID-19 virus. All of those feelings of fear, worry, and uncertainty are shared by the new parents and extended family, however grandparents are unique and medical staff should understand and welcome them in their supportive presence. They are the unsung heroes of this life-changing event.
We are looking for stories from a grandparents perspective, sharing your experience of having a grandchild in NICU or SCN and watching your own child navigate the challenges of such a journey. If you would like to share your story click HERE.
Source:https://www.miraclebabies.org.au/content/recognising-a-grandparents-journey/gjj5f6

She Had a Preemie — and Then She Started to Ask Important Questions
By Randi Hutter Epstein & Sarah DiGregorio – Jan. 28, 2020

EARLY: An Intimate History of Premature Birth and What It Teaches Us About Being Human
Sarah DiGregorio was 28 weeks pregnant when she found out that her baby had stopped growing. Two days later, her daughter, Mira, was delivered via an emergency cesarean section. She weighed 1 pound 13 ounces.
“My body had been trying to kill her,” DiGregorio writes.
“Early” opens like a medical thriller. Newborn Mira is whisked away to a neonatal intensive care unit while her parents are bombarded with statistics, terrified about her future. It closes with Mira, a robust toddler, diving into a pit of foam blocks. This isn’t a spoiler — but the heart of DiGregorio’s illuminating book isn’t just about her family’s journey; it’s an expansive examination of the history and ethics of neonatology.
For most of human history, babies born months too soon were left to die. They were considered less than full-fledged beings, not quite living and therefore not worth saving. Plus, there wasn’t much to be done.
The field of neonatology took off in the second half of the 20th century when a few pediatricians, often against the advice of colleagues, dared to save newborns.
In 1961, Dr. Mildred Stahlman, a Vanderbilt University pediatrician, fitted a premature baby into a miniature iron lung machine. These machines, originally for polio patients, used negative pressure to pull open weak chest muscles to draw air into the lungs. The baby survived. Stahlman then created one of the first neonatal units and trained a cadre of disciples.
By the 1970s, negative pressure machines were replaced with positive pressure ones that worked by inflating the lungs. It was a tricky technique that required threading the tiniest of tubes through the trachea and into the lungs. Dr. Maria Delivoria-Papadopoulos, then a pediatrician at Toronto’s Hospital for Sick Children, was one of the first to try. Seventeen attempts were unsuccessful. Then she saved one baby girl. Her tenacity paved the way for half a million people born prematurely living today.
And yet, DiGregorio reminds us, every advance — every attempt at every advance — brings with it new dilemmas. Such innovations may save a child’s life but can leave them with significant disabilities. A doctor cannot predict how a particular premature baby will fare. Complicating the matter, who’s to say what kind of life is worth fighting for and how much treatment is too much?
In “Early,” we read about neonatologists, bioethicists and parents grappling with the toughest decisions. We meet pediatric palliative care specialists and parents who forgo further treatment and embrace their babies as they die. DiGregorio covers other factors that influence prematurity, such as poverty and racism.
DiGregorio, a food editor and writer, is such a beautiful storyteller, I found myself underlining passages, turning corners of pages and keeping track of the page numbers at the back of the book until I had a hodgepodge of numbers scribbled on top of each other.
She imagines her nonfunctioning placenta as “a beat-up old car, chugging along, belching smoke”; after her emergency C-section, she writes, her body “felt like an empty house that had been vacated in a rush, leaving dirty dishes in the sink.” And later, DiGregorio refers to a 1-year-old as “that sweet spot between baby and toddler.”
By the epilogue, when the narrative returns to DiGregorio’s personal story, readers will appreciate how medicine lurches forward with leaps and mishaps along with the inevitably tense discussions about which path to take and when. All doctors wrestle with these issues, yet they seem particularly poignant when we are dealing with tiny babies. That’s because, as DiGregorio puts it, the field of neonatology has “changed the way we understand what it means to be alive, what it means to be human, and what constitutes a life worth living.”
Randi Hutter Epstein is the writer in residence at the Yale School of Medicine and author of “Aroused: The History of Hormones and How They Control Just About Everything.”
EARLY
An Intimate History of Premature Birth and What It Teaches Us About Being Human
By Sarah DiGregorio
A version of this article appears in print on Feb. 9, 2020, Page 17 of the Sunday Book Review with the headline: Born Too Soon.
Source:https://www.nytimes.com/2020/01/28/books/review/early-sarah-digregorio.html

NEW FATHER TO CELEBRATE FIRST FATHER”S DAY IN HOSPITAL WITH PREEMIE BORN AT 25 WEEKS
Laura Crimaldi – The Boston Globe
Brian and Kristen Sardini didn’t expect to become parents in time to mark Mother’s Day and Father’s Day this year. Their first baby was due on July 4.
But little Aila had different plans.
The baby girl was born March 26 during her mother’s 25th week of pregnancy. She weighed just over a pound.
On Sunday, the family will mark Brian Sardini’s first Father’s Day with Aila in the Newborn Intensive Care Unit, or NICU, at Brigham and Women’s Hospital.
“It’s the best Father’s Day gift in the world,” he said Saturday. “I’ve always wanted to be a dad and wouldn’t change anything because Aila’s perfect.”
During her three months in the unit, Aila has made tremendous strides, her parents said. The ventilator and continuous positive airway pressure or CPAP machine that Aila once used for breathing are history. A crib has replaced the isolette where she once spent most of her time. She’s tried out breastfeeding and started wearing clothes from the Preemie Store, which sells “micro” sizes for babies who weigh between 1 and 3 pounds.
On Friday night, Aila tipped the scales at just over 4 pounds. She has a collection of colorful, hand-knitted octopuses, which are used in hospitals to comfort premature babies.
What’s more, her parents have already read her the first four books in the “Harry Potter” series and are now halfway through reading her the fifth book, “Harry Potter and the Order of the Phoenix.”
“We started reading her ‘Harry Potter’ when she was, I think, 3 days old,” said Kristen.
Dr. Elisa Abdulhayoglu, the NICU’s medical director, said she was in the room when Aila was born and watched Brian meet his daughter.
“He bent down, looked at his beautiful little girl, and he said, ‘Yup. I’m a daddy’s girl for sure,’” she said. “It was an absolutely beautiful, beautiful moment.”
Good thing beautiful moments don’t require planning. Four days before Aila was born, Kristen said she had an uneventful appointment with her obstetrician. On the following day, the couple, both 27, planned to go to work and turn in a down payment for their new home in Medway.
But that day, they also went to an ultrasound appointment, and got some troubling news. Kristen had pre-eclampsia and needed to be admitted to the hospital for monitoring. Her routine checkup from the day before was suddenly ancient history.
“I had a totally normal OB appointment. My blood pressure was like 112 over 79. Completely normal. No red flags. Nothing wrong,” she said. “Within 24 hours, I was being sent to the Brigham. That’s how quickly this stuff can happen. And it’s really crazy.”
Kristen credits her husband with getting her through the Cesarean section birth.
“He just really helped me stay calm, and just like he said, focus on the task at hand and just take one thing at a time, and not let myself get lost in in mumbo jumbo of everything,” she said.
Before the birth, the couple said they were warned that their daughter wasn’t likely to cry or move when she was born and they wouldn’t have a chance to cut her umbilical cord.
Once again, Aila had something else in mind. She entered the world kicking, waving, and “crying at the top of her lungs,” her parents said. Brian also got to cut the umbilical cord.
“People say that when you see your child for the first time, it’s just an instant, instant bond and your whole life kind of changes,” Brian said. “As cliché as it sounds, it really is what happens.”
At a gestational age of 25 weeks, Abdulhayoglu said Aila is considered young by preterm standards. The majority of preterm babies born in the United States have reached a gestational age of at least 32 weeks, she said. The Brigham’s NICU cares for preterm babies as young as 22 weeks gestation, though, according to Abdulhayoglu.
In the long-term, she said outcomes are “excellent” for babies born at 25 weeks gestation.
“Parents are the true champions for these tiny, preterm babies, and her parents are amazing,” Abdulhayoglu said. “They’re there every day.”
The couple said they don’t know when Aila will be ready to leave the hospital, but they hope to take her home next month.
On Sunday, the couple said they plan to spend most of the day at the hospital with Aila, reading and snuggling. They heaped praise on the nurses, doctors, social workers, and other Brigham employees who have assisted them during Aila’s hospitalization.
Aila shares a room overlooking a courtyard with six other babies and decorated by her nurses with photographs of her and prints of her feet positioned to look like butterfly wings.
On Mother’s Day, Kristen said her daughter’s nurses gave her a mug that read, “Mom,” with Aila’s handprint in the spot for the letter O.
Kristen said she wants her husband to enjoy his first Father’s Day with their daughter.
“I hope that he just has the best day possible,” she said. “He has 100 percent earned it.”

HEALTH CARE PARTNERS
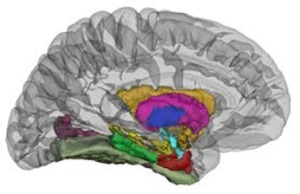
MRI Detects Atypical Brain Development in Premature Babies By News Release – School of Medicine in Boston

Subtle differences in brain structure can be detected by quantitative MRI (qMRI) in premature babies who later develop abnormalities such as autism or cerebral palsy. The study, published in Radiology, demonstrates the potential for qMRI, which obtains numerical measurements, to help improve outcomes for the growing numbers of people born preterm.
Advances in neonatal care have boosted survival rates for children born extremely preterm, defined as fewer than 28 weeks of gestation. With so many preterm infants surviving, there is interest in understanding the effects of preterm birth on brain development. Research has shown that extremely preterm babies face higher risks of brain abnormalities.
“So much of the maturation of brain occurs during the third trimester when the fetus is in the womb’s nourishing environment,” said study co-author Thomas M. O’Shea, MD, from the University of North Carolina in Chapel Hill. “These preterm babies don’t experience that, so it seems likely that there are alterations in the brain maturation during that interval.”
Dr. O’Shea and colleagues at 14 academic medical centers in the US launched a study 20 years ago to better understand the effects of preterm birth. The study, known as the Extremely Low Gestational Age Newborn-Environmental Influences on Child Health Outcomes (ELGAN-ECHO), evolved over the years to include experts in medical imaging like medical physicist Hernán Jara, PhD, professor of radiology at Boston University School of Medicine in Boston.
For the new study, Dr. Jara, Dr. O’Shea, and other ELGAN-ECHO researchers used qMRI. The noninvasive technique generates rich information on the brain without radiation. The researchers used it to assess the brains of adolescents who had been born extremely preterm.
“Quantitative MRI in a large dataset allows you to identify small differences between populations that may reflect microstructural tissue abnormalities not visually observable from imaging,” Dr. Jara said.
The researchers collected data from MRI scanners at 12 different centers on females and males, ages 14 to 16 years. They compared the qMRI results between atypically versus neurotypically developing adolescents. They also compared females versus males. The comparison included common MRI parameters, or measurements, like brain volume. It looked at less commonly used parameters too. One such example was proton density, a measurement related to the amount of water in the brain’s gray and white matter.
“What we aimed to do with qMRI was establish a biological marker that could help us discern these preterm children who had a diagnosis of disorder from those who didn’t,” said study lead author Ryan McNaughton, MS, a PhD student in mechanical engineering at Boston University.
There was no control group of people born after the typical nine months of gestation. Instead, the researchers used the neurotypically developed children for comparison.
Of the 368 adolescents in the study, 252 developed neurotypically while 116 had atypical development. The atypically developing participants had differences in brain structure visible on qMRI. For instance, there were subtle differences in white matter related to proton density that corresponded with less free water.
“This might be the tip of the iceberg since the amount of free water is highly regulated in the brain,” Dr. Jara said. “The fact that this difference was observed more in females than males may also be related to the known comparative resilience of females as demonstrated in findings from earlier ELGAN-ECHO and other studies.”
The researchers collected umbilical cord and blood samples at the beginning of the study. They plan to use them to look for correlations between qMRI findings and the presence of toxic elements like cadmium, arsenic, and other metals. The power of qMRI will allow them to study both the quantity and quality of myelin, the protective covering of nerves that is important in cognitive development. They also want to bring in psychiatrists and psychologists to relate qMRI findings to intelligence, social cognition and other outcomes.
“This project shows how researchers with different expertise can work together to use qMRI as a predictor of psychiatric and neurocognitive outcome,” McNaughton said.
“The teamwork required to get where we are now is pretty astounding,” Dr. O’Shea added. “I’m really grateful for the families, the nursing coordinators, and everyone else who made this possible.”
Dr. Philip Sunshine, founding father of Neonatology, is turning 90!
Jun 12, 2020
Our beloved Dr. Philip Sunshine, one of the founding fathers of Neonatology, is turning 90 years young! His only birthday wish? To help save more babies.
Fascinated? Learn more about Dr. Sunshine here: https://www.youtube.com/watch?v=h4ZjVfN3u0g

Policy Strategies for Addressing Current Threats to the U.S. Nursing Workforce
List of authors. Deena Kelly Costa, Ph.D., R.N., and Christopher R. Friese, Ph.D., R.N.
The Covid-19 pandemic has made it clear that without enough registered nurses, physicians, respiratory therapists, pharmacists, and other clinicians, the U.S. health care system cannot function. Weaknesses in health care staffing are of particular concern when it comes to the workforce of registered nurses, which could well see a mass exodus as the Covid-19 pandemic eases in the United States and the economy recovers. In a 2021 national survey conducted by the American Association of Critical-Care Nurses, 66% of respondents reported having considered leaving the profession, a percentage that is much higher than previously reported rates. Unsafe work environments — which predated the pandemic — are a key contributor to intentions to leave. Clinicians, health system executives, and policymakers have issued calls to address this crisis, but there has been little in the way of tangible federal or state policy action to prevent workforce losses or to build capacity.
Although it may comfort hospital executives to imagine a post-Covid future in which nurses are again willing to accept positions at local pay scales, such a scenario is unlikely to come about anytime soon. Historically, nurses have reduced their working hours or left the workforce during economic growth periods and returned during recessions, when family incomes fall.1 Nurses may again choose reduced employment as Covid-19 pressures ease and economic conditions improve. Moreover, nurses reported pervasive unsafe working conditions before the pandemic, and during Covid, they have cited a range of stressors and traumatic experiences, including furloughs, a lack of adequate protective equipment, increased violence, excessive workloads, and reduced support services. Pressures on the nursing workforce may therefore only worsen as Covid-19 subsides.
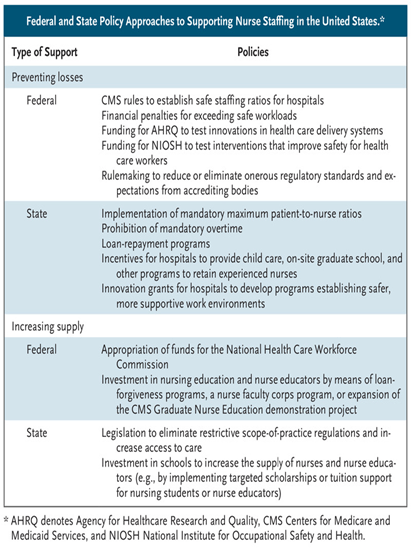
Federal and State Policy Approaches to Supporting Nurse Staffing in the United States.
State and federal policy solutions could prevent workforce losses and increase the supply of nurses (see table). Although there are challenges and opportunities for the nursing workforce throughout health care settings, hospitals are a particularly important area of focus.
Preventing the loss of current nurses is an essential component of shoring up the hospital nursing workforce. We contend that there isn’t a shortage of nurses, but a shortage of hospitals that provide nurses with safe work environments and adequate pay and benefits. At the federal level, the Centers for Medicare and Medicaid Services (CMS) could publish regulations, similar to recently announced policies governing skilled nursing facilities, that specify standards (including maximum patient-to-nurse ratios) for ensuring safe nursing care — and could establish financial penalties for hospitals that violate these regulations. Data supporting increased nurse staffing have been available for decades.2
Another federal strategy centers on investing in reimagined, safer health care systems. Congress could appropriate funds to the Agency for Healthcare Research and Quality to support investigator-initiated grants focused on developing new, scalable care-delivery models that are designed to improve outcomes for patients and clinicians. The National Institute for Occupational Safety and Health could expand testing of protective equipment and strategies for improving health care workers’ well-being. Data are needed on care-delivery models that keep patients safe and on approaches for promoting joy and safety in clinical work.
Regulatory bodies, including CMS and CMS-approved accreditors, such as the Joint Commission, could scale back regulations and standards that add to nursing workloads. Although some regulations were temporarily eased during the pandemic, new rulemaking could eliminate especially burdensome provisions that aren’t essential to patient safety. For example, clinical-documentation burden is a frequently cited source of job dissatisfaction and burnout. Documentation requirements, which are interpreted in various ways by different hospitals, could be minimized to reduce burnout and attrition.
States have more flexibility than the federal government when it comes to enacting legislative and regulatory changes to improve work environments and prevent losses in the nursing workforce. In the absence of federal action in this area, state legislation promoting safer nurse-staffing practices — such as laws establishing mandatory patient-to-nurse ratios — is an evidence-based intervention to support patient safety and reduce the likelihood of nurse departures. Studies have reported improved nurse staffing, improved job satisfaction among nurses, and improved patient outcomes in California after the state enacted legislation prohibiting mandatory overtime for nurses and establishing maximum patient-to-nurse ratios.3 Many U.S. hospitals continue to require nurses to work overtime hours, however, and few have mandated staffing ratios. Legislatures in some states have introduced bipartisan bills similar to California’s law that would restrict mandated overtime and implement maximum staffing ratios. When considered at a national scale, mandated staffing ratios face implementation hurdles, since coordination would be required to distribute the nursing workforce equitably throughout the country. But such policies would most likely prevent workforce losses and boost the number of entrants into the profession.
Policies could also support career development among nurses. Studies have documented the negative effects of Covid-19 on the careers of women in particular. Approximately 90% of U.S. nurses are women, and many of them have faced pressures related to family care during the pandemic, amid school and child-care facility closures. To ease nurses’ household burdens, states could offer loan-repayment programs and offset nursing school tuition debt. They could also provide grants or tax benefits to hospitals offering on-site child care, after-school care, or comprehensive dependent-care programs. Finally, states could offer innovation grants to hospitals to develop safer, more supportive workplaces or fund new initiatives to support on-site graduate-school and professional-development programs designed to retain experienced nurses.
Preventing workforce losses is important, but so is increasing the supply of nurses. The United States lacks access to real-time workforce data and expert guidance for evaluating those data and for advising policymakers on workforce shortages. The National Health Care Workforce Commission was authorized as part of the Affordable Care Act, but Congress never funded it. Appropriating funds for this commission would strengthen the country’s ability to respond to the current threat to nurse staffing and prepare for future ones.
A key factor constraining the supply of nurses derives from structural barriers within nursing education. Being hired as a nursing school faculty member requires having an advanced degree, but expert nurses rarely accept faculty positions because salaries are higher for practice roles. Faculty shortages, among other factors, limit nursing school enrollments; over the past decade, schools turned away between 47,000 and 68,000 qualified applicants annually.4 Federal policies could loosen the nursing bottleneck. For example, policymakers could increase financial incentives to recruit nurse educators, expand nursing school loan-forgiveness programs, fund grants for hospitals and nursing schools to share expert nurses as clinician-educators, and develop a nurse faculty corps program to raise salaries in regions with shortages of nurses. Creative financial incentives, such as tuition-remission programs or programs that provide loans at low interest rates, could encourage prospective students to choose nursing careers. Pipeline programs and partnerships among high schools, technical schools, and universities could permit emergency medical technicians, certified nursing assistants, and armed forces corpsmen or medics to apply clinical work hours toward nursing degrees and qualify for targeted scholarships supported by state or federal funds. Expansion of the CMS Graduate Nurse Education demonstration project could substantially increase the number of qualified nurse practitioners, who could also serve as clinical nursing faculty.
State legislation that eliminates onerous scope-of-practice regulations for advanced practice providers would enable nurse practitioners, including midwives, to practice independently and could increase access to health care. In Michigan, Senate Bill 680 would implement these reforms, thereby allowing nurse practitioners to prescribe tests, medications, and services. This bill could increase the state’s supply of clinicians and potentially attract nurses planning to pursue advanced degrees.
Threats to the nursing workforce aren’t new, and neither are proposals to address them.5 Although policies aimed at individual components of this problem could be helpful, a comprehensive package of federal, state, and local efforts would probably be the most effective approach for averting health care system dysfunction and adverse outcomes. We believe federal and state policies should both prevent the loss of current nurses and increase the supply of nurses. Without timely investments in the nursing workforce, the United States may have enough hospital beds for seriously ill patients, but not enough nurses to deliver essential, safe care.
Source:https://www.nejm.org/doi/full/10.1056/NEJMp2202662

Skin injuries to babies in neonatal care could be avoided with new splint, trial shows
by Victoria University of Wellington – MAY 26, 2022
A new device to prevent skin injuries to babies in neonatal intensive care units has been successfully trialed in a study led by Dr. Deborah Harris, a neonatal nurse practitioner at Te Herenga Waka—Victoria University of Wellington.
Most babies admitted to hospital need an intravenous drip to deliver fluids and medications, says Dr. Harris. This drip is secured to the baby’s skin using adhesive tape.
“Removing the adhesive tape is painful and can cause skin injuries and scarring. Skin damage also increases the risk of the baby getting an infection and being in hospital longer. We designed a device called a Pēpi Splint that can be used to secure the drip without the need to apply adhesive tape to the baby’s skin,” Dr. Harris says.
A trial of the Pēpi Splint on 38 babies at Wellington Hospital’s neonatal intensive care unit showed it was effective and avoided the skin damage caused by adhesives.
“The Pēpi Splint held the drips secure for 34 of the 38 babies in our trial. In four cases, the splint became loose either because it hadn’t been secured properly or was dislodged when the baby was removed from the cot for breastfeeding.”
Dr. Harris says the results provide support for a larger randomized controlled trial.
“Skin injuries are common in neonatal units and the damage caused to a baby’s skin by adhesive tape can be considerable. Removing the tape has the potential to strip 70% to 90% of a baby’s epidermis. We hope the Pēpi Splint will help reduce these injuries to newborns.”
The splint is made from medical-grade silicon gel and contains an aluminum mesh, allowing it to be molded to the baby’s limb. Adhesive tape is used on the Pēpi Splint itself to secure it to the drip, but tape is not applied to the baby’s skin.
During the trial, modifications were made to the splint to make it easier to use. “After these changes, clinicians involved in the trial reported the splint was easy to apply,” Dr. Harris says.
Most parents supported the device’s use: 52 of 58 (90%) said they would participate in the study again if they had another eligible baby.
The Pēpi Splint, developed in collaboration with a design engineer, can be washed and sterilized for reuse.
Source:https://medicalxpress.com/news/2022-05-skin-injuries-babies-neonatal-splint.html




PREEMIE RISING STAR!!!
Golden Buzzer: Avery Dixon’s Emotional Audition Moves Terry Crews to Tears | AGT 2022
May 31, 2022 – #AGT #AmericasGotTalent #Auditions

Grab your tissues; Avery Dixon’s emotional audition might make you cry. Terry Crews was moved to tears when he heard Avery’s sensational saxophone skills and harrowing story about being bullied.
Kat’s Korner

Fellow Warriors and Preemie Parents,
As per the NTNU St. Olay Hospital’s Study, “ the risk of dying before the age of 50 is 40 percent higher for preemies than for the population as a whole. Researchers found that the risk of dying for individuals born before full gestation and who have chronic heart disease, lung disease, or diabetes is twice that of the population as a whole.” These findings provide valuable information in regard to the morbidity risk of preemie infant survivors and highlight the need for further research.
Increased diagnosis and early detection of disease conditions that preemie survivors are more prone to experience are critical as our rate of survival is improving and more of us are thriving well into adulthood. While research efforts to improve outcomes, reduce mortality and enhance care for neonates have drastically improved over the past 50 years, few studies have investigated long-term outcomes, health disparities, and the impact of the life-long physical and psychological impact of being premature among the adult population. We need to establish specialist education/credentialing that support workforce opportunities to partake in diagnostics, treatment, research and development aimed at addressing adult care for preemie infant survivors.
As a community that makes up 11-12% of the global population, we can connect and engage with each other as preemie survivors, promote collaboration between all members of our community, and actively advocate for change in the clinical management of preemie infant survivors to include long-term and specialized care.
If you or someone you know is interested in learning more about ways to connect with our adult preemie community a great resource is the Adult Preemie Advocacy Network, sharing safe space communication platforms for preemie survivors and opportunities to participate in research activities, and partake in advocacy activities to support our resilient community. Check out this great resource below-
Source:https://adultpreemies.com/

Surfing Under the Northern Lights w/ Mick Fanning | Chasing the Shot: Norway Ep 1
Mar 20, 2017




