


Venezuela is a country on the northern coast of South America, consisting of continental landmass and many islands and islets in the Caribbean Sea. It has a territorial extension of 16,445 km (353,841 sq mi), and its population was estimated at 29 million in 2022. The capital and largest urban agglomeration is the city of Caracas.
The continental territory is bordered on the north by the Caribbean Sea and the Atlantic Ocean, on the west by Colombia, Brazil on the south, Trinidad and Tobago to the north-east and on the east by Guyana. The Venezuelan government maintains a claim against Guyana to Guayana Esequiba. Venezuela is a federal presidential republic consisting of 23 states, the Capital District and federal dependencies covering Venezuela’s offshore islands. Venezuela is among the most urbanized countries in Latin America; he vast majority of Venezuelans live in the cities of the north and in the capital.
Venezuela has a national universal health care system. The current government has created a program to expand access to health care known as Misión Barrio Adentro, although its efficiency and work conditions have been criticized. It has been reported that many Misión Barrio Adentro clinics have been closed, and (as of December 2014) it is estimated that 80% of Barrio Adentro establishments in Venezuela are abandoned.
Infant mortality in Venezuela was 19 deaths per 1,000 births for 2014 which was lower than the South American average. Child malnutrition (defined as stunting or wasting in children under the age of five) was 17%. Delta Amacuro and Amazonas had the nation’s highest rates. According to the United Nations, 32% of Venezuelans lacked adequate sanitation, primarily those living in rural areas. Diseases ranging from diphtheria, plague, malaria, typhoid fever, yellow fever, cholera, hepatitis A, hepatitis B, and hepatitis D were present in the country. Obesity was prevalent in approximately 30% of the adult population in Venezuela.
Source:https://en.wikipedia.org/wiki/Venezuela
GLOBAL PRETERM BIRTH RATES – Venezuela
Estimated # of preterm births: 9.73 per 100 live births
(USA 9.56-Global Average: 10.6)
Source- WHO 2014- https://ptb.srhr.org/

COMMUNITY

| We appreciate March of Dimes and the excellent and progressive work the March of Dimes performs locally and globally. The positive effects resulting from the March of Dimes intent and action, shared so generously with global Maternal and Child healthcare communities, and the continuous and positive impact the March of Dimes provides to educate and inspire individuals and organizations worldwide while generating increased support, education, and empowerment for women, children and families is simply…immeasurable and beautifully present. I share with heart-felt respect and gratitude the email we received (below) with our Neonatal Womb Warrior/Preterm Birth community. Please enjoy the email and consider clicking on the link that follows in order to share your voice towards inspiring supportive action for the health and well-being of Moms, Children, and Families everywhere. Add your voice today to the thousands of advocates calling for improved outcomes for moms, babies and families across the nation. March of Dimes Email to Kathy: Dear Kathy, Today, the Centers for Disease Control (CDC) and Prevention National Center for Health Statistics released the annual Maternal Mortality Rates in the United States Report and the data are alarming. Since 2018, the maternal mortality rate increased nearly 89%. The maternal mortality rate for 2021 was 32.9 deaths per 100,000 live births compared to a rate of 23.8 in 2020. This is a 38% increase which is more than 2x the increase observed between 2019 and 2020. While rates of maternal mortality significantly increased between 2020 and 2021 for all race and Hispanic origin groups, the data show that significant racial and ethnic disparities in maternal mortality persist. Maternal mortality rates for Black and Hispanic women significantly increased. In 2021, Black women were more than 2.5 times more likely to die than White and Hispanic women. Since 2018, the maternal mortality rate increased nearly 89%. The maternal mortality rate for 2021 was 32.9 deaths per 100,000 live births compared to a rate of 23.8 in 2020. This is a 38% increase which is more than 2x the increase observed between 2019 and 2020. While rates of maternal mortality significantly increased between 2020 and 2021 for all race and Hispanic origin groups, the data show that significant racial and ethnic disparities in maternal mortality persist. Maternal mortality rates for Black and Hispanic women significantly increased. In 2021, Black women were more than 2.5 times more likely to die than White and Hispanic women. Kathy, our nation is facing a maternal and infant health crisis. The U.S. remains among the worst developed nations for childbirth. The report released today only emphasizes that and is critical in raising awareness of the most pressing maternal and infant health issues families experience. From helping to provide access to quality and equitable health care across the country to mobilizing our community to create lasting change for moms and babies through research and advocacy, March of Dimes is working to ensure all families can get the best possible start. Thank you for everything you do to fight for the health of all moms and babies. Sincerely, Dr. Elizabeth Cherot Chief Medical & Health Officer March of Dimes P.S. Kathy, we’re calling for #BlanketChange to improve the health of all moms and babies. Families in the U.S. need #BlanketChange. Help us achieve equity, access, and prevention for all moms and babies. Every family deserves to be healthy and receive the best possible start, regardless of income, race, gender or geography. But for too many in the United States, that isn’t the case. The U.S. is among the most dangerous developed nations for childbirth, and preterm birth–one of the leading causes of infant death–is at a 15-year high. The U.S. earned a D+ grade for preterm birth with the preterm birth rate increasing to 10.5%– the worst rate March of Dimes has ever reported. Maternal mortality has increased by 89% since 2018. While maternal mortality rates significantly increased for all races, clear and substantial racial and ethnic disparities continue to persist across key maternal health measures. Black women are 2.6 times more likely to die than White women and 2.5 times more likely to die than Hispanic women. The maternal and infant health crisis is worsening. March of Dimes is calling for #BlanketChange to improve the health of all moms and babies. Our agenda includes three key pillars: Equity: Eliminating racial and ethnic health disparities by focusing on prevention, treatment and social determinants of health to improve birth outcomes. Access: Improving unequal access to health care which contributes to the maternal and infant health crisis. Prevention: Expanding research and data collection on maternal mortality and morbidity to address preventable health conditions. Join us and tell your legislators we need #BlanketChange NOW. Add your voice to the thousands of advocates calling for improved outcomes for moms, babies and families across the nation. Add your voice today to the thousands of advocates calling for improved outcomes for moms, babies and families across the nation. |

At NICU Discharge, Considering Social Determinants of Health
A successful transition to home requires addressing a family’s environmental, financial, literacy, transportation, and social challenges.

Stefanie LaManna September 10, 2022
- Emma was born three months prematurely, with a variety of medical complications. After a long neonatal intensive care unit (NICU) stay, she is finally ready to go home—to a rural town more than an hour from the hospital.
- Emma will need follow-up with multiple medical specialists, as well as physical therapy and speech-language treatment. She also needs her parents to manage her feeding tube, as she is unable to eat fully by mouth. Emma’s mother, Denise, quit her cashier job to care for her; her father, Tim, works long hours as a mechanic. Denise faces long hours caring for Emma alone, which feels overwhelming. The family is enrolled in Medicaid and the Special Supplemental Nutrition Program (WIC) in their state.
Nearly 50% of extremely preterm infants (those born at less than 28 weeks gestational age) who require prolonged NICU stays are re-hospitalized within the first two years of life (see sources). These medically complex infants need care from a variety of specialists to reduce the risk of re-hospitalization.
This interprofessional team is aware of the family’s socioeconomic and logistical barriers that may increase Emma’s risk—and they know how to incorporate these factors into discharge planning to ensure the family is prepared and well-supported for home.
Social determinants of health
A family’s socioeconomic status is one of the social determinants of health (SDOH)—the conditions in the family’s environment that affect a wide range of health, functioning, and quality-of-life outcomes and risks. Per the U.S. Department of Health and Human Services, SDOH can be grouped into five domains: economic stability; education access and quality; health care access and quality; neighborhood and built environment; and social and community context.
SDOH affect people’s health and quality of life and may also lead to disparities and inequities in access to food, education, and health care (see last issue’s Leader article “Why Social Determinants of Health Matter So Much to Care.”
Emma and her family face barriers in each domain that may affect the transition to home.
Economic stability
Economic stability can influence a family’s ability to obtain specialty feeding supplies for their infant after NICU discharge, such as hypoallergenic formulas or specialty bottle systems. Even if one parent is steadily employed, frequent follow-up appointments and unanticipated medical expenses can strain family finances. Or perhaps a family member can no longer work because the family lacks access to medical daycare.
- Denise is concerned that they cannot afford the bottle and nipple system that Emma has been using. The speech-language pathologist gives her extra nipples and bottles, as well as a gift card from the hospital’s charitable foundation to purchase extra supplies. The neonatologist and social worker collaborate to ensure that Emma’s specialty formula is available in her town and the physician writes a prescription for the formula so it will be covered by their medical assistance.
Education access and quality
A family’s access to education can affect their health literacy—the ability to understand basic health information needed to make appropriate health decisions. For example, almost half of adults who did not graduate from high school have low health literacy (see sources). People with low health literacy may have difficulty reading medication labels and dosages and formula-mixing instructions, or may find it challenging to report specifics such as their infant’s medications and feeding regimen to specialists and other medical staff.
- Denise and Tim have learned to feed Emma using a feeding tube. Tim often gets frustrated figuring out how much formula to feed Emma and how to program the pump. The dietitian and NICU nurse collaborate to provide easy-to-follow, written instructions Tim can keep and easily access on his phone.
Health care access and quality
Infants born extremely preterm or critically ill may require immediate transfer to a facility capable of handling their unique needs—which may be far from home or across state lines. After discharge, they usually have a variety of follow-up specialist appointments. Lack of transportation or inadequate insurance coverage may result in transferring care to specialists closer to home, though families may face long wait lists or delays in care.
It will be challenging for Denise and Tim to attend weekly appointments at the hospital, so the team transfers some of Emma’s care closer to her home—to a local pediatrician they provide with a comprehensive transition plan. The SLP connects Emma’s parents with a colleague who can provide feeding and swallowing treatment in their town, and refers the family to the state’s early intervention program so they can receive services in their home. The neonatologist schedules initial follow-ups with medical specialists on the same day so the family has only one trip to the hospital.
Neighborhood and built environment
Location, race, ethnicity, and socioeconomic status can affect environmental exposures, and poor communities are disproportionately affected by environmental conditions such as polluted air and water (see sources). A family living in a community with pollution may not have access to clean water to mix with formula or to wash feeding supplies, such as breast pump parts or bottles.
- The dietitian and NICU nurse discuss formula-mixing instructions with Emma’s parents. They explain the importance of using sterile water (purchased from the store or boiled tap water) to decrease risk of infection. The social worker helps Denise apply for the supplemental nutrition assistance program (SNAP) to help pay for sterile water.
Social and community context
Parents of extremely preterm infants report higher levels of anxiety, depression, and parenting stress than parents of infants born at term, and a lengthy NICU stay can result in isolation from family and friends (see sources). Loved ones may not understand the implications of preterm birth and required medical supports on an infant’s development, or they may put well-intentioned pressure on an infant’s family to hasten discharge from the hospital, which may make for uncomfortable interactions.
- Denise and Tim have no local family. Denise’s best friend has been supportive, but the friend’s son was born full-term, and Denise feels like she doesn’t understand the NICU experience. The patient advocate connects Denise with a virtual support group for NICU parents, in the hospital and after discharge. The social worker collaborates with their insurance company to secure nursing care for Emma so Denise has assistance while Tim is at work.
Discharge from the NICU is a significant milestone for an infant and family—but it can be a complex process with hurdles that make going home seem overwhelming. Considering a family’s unique SDOH during discharge planning can reduce health inequities and disparities, support a smooth transition to home, and ensure families have access to the resources to help them thrive.
Source:https://leader.pubs.asha.org/do/10.1044/leader.OTP.27092022.ipp-nicu-slp.38/full/

Estoy Vivo Feat Chino y Nacho


UNICEF supports the growth and development of babies born prematurely or underweight

28 June 2022
To contribute to the decrease in neonatal and infant morbidity and mortality and to promote breastfeeding, UNICEF supports the Kangaroo Method and its three fundamental pillars: kangaroo position, breastfeeding and outpatient follow-up
Children that are born before the 37 weeks or underweight face a risk such as mild alterations in their cognitive functions, delayed psychomotor development, vision loss, deafness, and even autism.
To mitigate these risks, UNICEF supports the early care of premature infants, and their families, through skin-to-skin contact from the moment of birth and according to the degree of prematurity or affectation, such practice is known as Kangaroo Mother Care Method. Thus, UNICEF, alongside health authorities, and multidisciplinary and family medical teams, work so every child enjoys their right to the highest possible level of health and quality services for the treatment of diseases, as it is established by the Convention on the Rights of the Child.
In the lactation center, mothers are assisted by a team of doctors, promoters, and nurses who guide and teach them the proper techniques for successful breastfeeding and how to preserve their breast milk. “Several promoters assist mothers from the moment they arrive at the emergency room. These new spaces reduce work for us since we now count on a mechanical device that helps women to prevent mastitis, hardening of their breasts, and those who have difficulty breastfeeding their baby. In this location, we set up the device (manual breast pump) and she feels relieved”, Indicates Elba Melchor, who is a promoter of humanized birth in the hospital.
In the outpatient consult, we offer medical assistance to monitor the growth and development of children until they are two years old, and to continue educating family members on the care of their children. Likewise, medical advice on breastfeeding and complementary feeding, and immunizations, among other key aspects for the health of these children is provided to the mothers. This consult is of vital importance since it allows timely diagnosis and treatment of some pathologies that occur in these children, such as metabolic or gastrointestinal disorders, sensorineural disorders such as cerebral paralysis, blindness, deafness; language problems, among others.
This care design allows the inclusion of both parents, as well as the whole family together with a group of professionals from different disciplines such as doctors, nurses, physiotherapists, speech therapists, and social workers, among others, all integrated into an environment aimed at the care and stimulation of these children.
In this consult, parents are reinforced with the importance of early attachment, through the kangaroo mother care method, and this way they are actively involved in the development of their baby.
Suarnny is 7 months old. She was born at 35 weeks weighing 2.4 kilograms and then gradually lost weight. Today she has an expected development thanks to the accompaniment of the multidisciplinary team that has been with her watching over her development and growth process.
“The first days were tough, she had to be in an incubator for a month. In the hospital they encouraged me, they explained to me how to breastfeed her at the clinic and that I should talk to her and stimulate her. Little by little I was getting ahead, my girl was gradually gaining weight. I bring her monthly to her consultation”, indicates her mom Neyra.
Through their nutrition programme, in coordination with the health authorities and thanks to the contribution of international donors, UNICEF contributes to the reduction of infant mortality by improving the care of children born prematurely and underweight.

HEALTHCARE PARTNERS
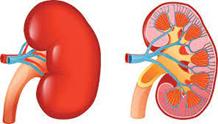
Clinical Pearl: Understanding the Impact of Neonatal Acute Kidney Injury

Kellie Barsotti, MD; Melanie Wielicka, MD PhD
In recent years, we have significantly advanced our understanding of acute kidney injury (AKI) within the neonatal population. At birth, only about 4% of cardiac output reaches the kidneys; this is reflected in infants’ low glomerular filtration rate, especially those born prematurely. Any additional stressors such as hypoxia, hemodynamic instability, or infection, all of which we frequently encounter in preemies, have the potential to impact renal perfusion further and induce AKI. The incidence of AKI in infants born before 29 weeks gestation has been reported to be as high as 43%. Thus, significant efforts have been made to define neonatal AKI better and identify the risk factors and the related short and long-term outcomes.
Over the past ten years, the neonatal modified Kidney Disease: Improving Global Outcomes (KDIGO) criteria have become the gold standard definition for neonatal AKI. It determines the severity of AKI based on the magnitude of the rise in serum creatinine from prior values and the decrease in urine output and may be used in patients <120 days of age. This definition, as many other ones used in pediatrics, was adapted mainly from an adult patient-driven one. For instance, it fails to account for the physiologic changes in neonatal creatinine, which initially reflects maternal creatinine. If maternal serum creatinine is low, it would be expected that in an extremely premature infant, their creatinine would increase over the first several days of life, which would not necessarily be representative of AKI.
Additionally, serum creatinine (SCr) is a marker of renal function, not injury. The initial insult must cause a significant decline in renal function in order to result in an increase in SCr, which can sometimes take several days. This issue leads to a delay in SCr increase in relation to the timing of the injury. Furthermore, the KDIGO criteria fail to account for the neonate’s chronological and post-menstrual age. Despite its flaws, this definition has provided a certain degree of standardization and has allowed us to describe neonatal AKI’s epidemiology and outcomes better.
The Assessment of Worldwide Acute Kidney Epidemiology in Neonates (AWAKEN) study included 24 centers and collected data from almost one thousand neonates admitted to neonatal intensive care units. It has demonstrated that the risk of AKI increases significantly with decreasing gestational age and that neonates with AKI have higher odds of death and prolonged hospitalization. It has also expanded upon the neonatal-modified KDIGO definition to address neonatal physiology and redefine absolute serum creatinine thresholds based on gestational age. Using mortality as a meaningful clinical outcome, they tested the hypothesis that ideal cutoffs for serum creatinine levels within the first week of life will differ by gestational age. Their data shows that absolute and percent serum creatinine cutoffs are higher in those neonates born at less than 29 weeks gestation, suggesting that the neonatal modified KDIGO definition does not adequately account for physiologic differences seen within the first week of life and also between neonates of different gestational ages. This project marks an important milestone in AKI research in that previously, we relied on retrospective, single-center studies and lacked meaningful data on AKI incidence and risk factors in patients categorized by gestational age and time point in their hospital course.
Last year, Aziz et al.’s smaller, single-center study provided supportive evidence for AKI being inversely proportional to both gestational age and birth weight and for an association between AKI and increased mortality in extremely low-birth-weight neonates. Interestingly, they suggested that while mortality is strongly associated with neonatal AKI, it does not directly result from it, and its amelioration does not reduce the risk of death in this population. In response to these findings, Askenazi et al. discussed in a commentary piece why this is less likely to be true. The authors note that there is a possibility of bias within the statistical approach of the initial study with the use of Shapley Additive Explanations Analysis (a structural model that shows the relative association of each measured variable with a given outcome) to determine the association between each variable and their relationship to mortality. Another reason this paper cites is the limitations of using the neonatal-modified KDIGO criteria in this patient population, especially in the first several days of life, some of which we have already discussed. Because of the potential for this miscalculation bias, many studies do not include serum creatinine from the first 48 hours of life, unlike Aziz et al. Since serum creatinine often does not increase for up to 48 hours following a renal insult, it becomes challenging to assess AKI›s relationship with mortality in this population when elevation in serum creatinine has been proven to lag behind the injury. As there seems to be a widespread consensus that serum creatinine is a suboptimal marker for monitoring neonatal renal function, identifying novel biomarkers that would allow for earlier identification and better classification of AKI continues to generate interest. Some of the ones that have been suggested thus far include urine neutrophil gelatinase-associated lipocalin, cystatin-c, and kidney injury molecule-1, although further work is needed before we will be able to use them in our clinical practice .
Source:http://neonatologytoday.net/newsletters/nt-feb23.pdf

Venezuelan medical professionals step in to fill healthcare gaps in Peru
Among the 1.5 million Venezuelan refugees and migrants in Peru are doctors and nurses who want nothing more than the chance to serve.

By Jenny Barchfield in Lima, Peru | 15 February 2023
There were times, during the darkest days of the pandemic, when the Venezuelan nurse started vaccinating at 7am and finished, many hundreds of patients later, only at midnight.
“We didn’t get tired,” Edixioney recalled. “What we wanted was for people to be able to get vaccinated so that they wouldn’t have to go home, unvaccinated, after having wasted their time in line.”
For 39-year-old Edixioney, who left Venezuela to seek life-saving heart surgery for her daughter and spent her first months in Peru working in a restaurant, the chance to serve in her chosen profession feels like nothing short of a miracle.
“Our thing is vaccinating,” said Edixioney, adding that she and the other Venezuelan nurses she works with at the Los Libertadores public health clinic in Lima’s San Martín de Porres neighbourhood will be eternally grateful for “the opportunity to earn a living doing what we love.”
Peru is home to the second-largest population of Venezuelan refugees and migrants in the region, playing host to nearly 1.5 million of the total 7.1 million Venezuelan nationals who have left their country in recent years amid the ongoing social and economic crisis there. Many of them are educated professionals, including nurses, physical therapists, and physicians who, despite having skills that are highly sought after in their adopted country, have sometimes faced administrative hurdles that have make it difficult for them to practice in their adopted country.
That was initially the case for Néstor Márquez, a 53-year-old physician who settled in Lima in 2018. When he first arrived, Néstor was in no position to revalidate his medical licenses – a long and expensive process that can take upwards of a year and a half. His first priority was to save up enough money to be able to bring his wife and three young children to Peru.
To do so, he traded the scrubs that had been his daily uniform during his decades-long medical career in Venezuela for a pair of comfortable shoes.
“I worked selling books at sidewalk stands…. I was a travelling book salesman,” said Néstor, a smile just visible from behind his surgical mask. “It helped me so much. With what I made selling books, I was able to bring my family.”
Now, thanks, in part, to an agreement between UNHCR, the UN Refugee Agency, and Peru’s Health Ministry, Néstor is working in physical therapy – the specialty he trained for back in Venezuela – at a new public clinic in North Lima. Under the deal, UNHCR funds the salary of the staff, nearly all of whom are Venezuelan nationals, for an initial three months while they are onboarded.
Since it opened last year, residents from across the Peruvian capital have been flocking to the Los Olivos de Pro Rehabilitation Centre, seeking relief for ailments such as back pain, nerve damage, and long-lasting respiratory problems resulting from COVID-19. The team has also seen a surge in parents seeking speech therapy for young children who, kept inside during the pandemic at crucial stages in their development, are having a hard time communicating.
Ironically, Néstor says that it was the coronavirus pandemic that helped Venezuelan health professionals in Peru, like him, get back to work.
In 2020, Peru’s healthcare workers were among the hardest hit by the coronavirus, which further depleted an already overburdened workforce. The pandemic created a dire need for qualified and experienced medical professionals, which prompted Peruvian authorities to fast-track medical licenses for qualified staff hailing from other countries who were already living in Peru. It was then that Néstor applied for and was granted the right to practice in Peru.
“For me, it’s like a dream come true to be here, in this place where there is so much need,” he said, gesturing toward the waiting area, where a little boy in a wheelchair and leg braces was awaiting his appointment. “Working here in this clinic allows me to carry out what I’ve spent my whole life thinking about and doing, surrounded by a group of extraordinary Venezuelan professionals.”
Asked whether any of the patients have balked at being cared for by the clinic’s near all-Venezuelan staff, Néstor said that, on the contrary “they are happy and grateful.”
Yesenia Ramos Sandóval, the mother of the little boy in the wheelchair, 7-year-old Jeremy, echoed that sentiment.
“We’re just so happy to be able to get Jeremy the therapy he needs,” said Yesenia, a 30-year-old native of the Peruvian capital, with a broad smile.

Moms’ and babies’ medical data predicts prematurity complications, Stanford Medicine-led study shows
Stanford Medicine scientists and their colleagues have shown they can tap mothers’ and babies’ medical records to better predict newborn health risks.

February 15, 2023 – By Erin Digitale
By sifting through electronic health records of moms and babies using a machine-learning algorithm, scientists can predict how at-risk newborns will fare in their first two months of life. The new method allows physicians to classify, at or before birth, which infants are likely to develop complications of prematurity.
A study describing the method, developed at the Stanford School of Medicine, was published online Feb. 15 in Science Translational Medicine.
“This is a new way of thinking about preterm birth, placing the focus on individual health factors of the newborns rather than looking only at how early they are born,” said senior study author Nima Aghaeepour, PhD, an associate professor of anesthesiology, perioperative and pain medicine and of pediatrics. The study’s lead authors are postdoctoral scholar Davide De Francesco, PhD, and Jonathan Reiss, MD, an instructor in pediatrics.
Traditionally defined as birth occurring at least three weeks early, premature birth is linked to complications in babies’ lungs, brains, vision, hearing and digestive system. Although earlier births generally carry higher risks, the timing of birth predicts only approximately how a specific infant will fare. Some infants who are born quite early develop no complications, while others born at the same stage of pregnancy become very ill or die.
“Preterm birth is the single largest cause of death in children under age 5 worldwide, and we haven’t had good solutions,” Aghaeepour said. “By focusing our research on predicting the health of these babies, we can optimize their care.”
Many complications of prematurity take days or weeks after birth to emerge, causing substantial damage to newborns’ health in the meantime. Knowing which infants are at risk could enable preventive measures.
“We look mainly at the baby to make treatment decisions in neonatology, but we are finding that we can get valuable information from the maternal health record, really homing in on how individual babies’ trajectories have been shaped by exposure to their specific maternal environment,” said study coauthor David Stevenson, MD, a neonatologist at Lucile Packard Children’s Hospital Stanford, professor of pediatrics and director of the March of Dimes Prematurity Research Center at the Stanford School of Medicine.
“This is a move toward precision medicine for babies,” he added.
The researchers linked electronic medical records for mothers at Stanford Health Care and for their babies at Stanford Medicine Children’s Health, covering 32,354 live births that occurred between 2014 and 2020. The mothers’ medical records included information from the pregnancy and, for those who had been patients at Stanford Medicine prior to pregnancy, health data from before they became pregnant. The infants’ records started with information recorded at birth, including weight; blood tests; and Apgar score, which is assessed in the delivery room one and five minutes after birth. The Apgar score incorporates factors such as the infant’s pulse, breathing and muscle tone.
Using a machine learning algorithm called a long short-term memory neural network, the researchers built a mathematical model from the medical records and tested whether it could predict 24 possible health outcomes for infants up to two months after birth.
“There is a computational challenge in using electronic health records because they are longitudinal and contain a large amount of data from each patient,” Aghaeepour said. “A long short-term memory neural network operates similarly to a person reading a book. When we’re reading, we don’t remember every word, but we remember the key concepts, read the next part, add more key concepts and carry that forward. The algorithm doesn’t memorize the entire electronic health record of every patient, but it can remember key concepts and carry those forward to the point where we make a prediction.”
At the time of birth, the machine learning model provided strong predictions for which infants would develop various conditions including bronchopulmonary dysplasia, a type of chronic lung disease; retinopathy of prematurity, a problem with the retina that can cause vision loss or blindness; anemia of prematurity; and necrotizing enterocolitis, a severe gastrointestinal complication often not diagnosed until weeks after birth, by which time interventions are complex and associated with poor outcomes.
The model also gave strong predictions a week before birth for multiple outcomes including mortality and retinopathy of prematurity, which can cause vision loss or blindness, as well as moderately strong predictions for 11 other conditions.
“I was surprised by how much predictive power we have before the baby is even born, and right at birth,” Aghaeepour said. “I did not expect to see that. I had thought accuracy would come several days after birth, once we had collected data from the baby.”
Some complications were not reliably predicted by the model, such as which infants would develop candidiasis, or yeast infections; polycythemia, a high concentration of red cells in the blood; or meconium aspiration syndrome, in which the infant inhales meconium, a sticky substance expelled from the fetal bowel, during birth.
The researchers validated that the strength of the predictions did not change over the years (comparing births from 2014 to 2018 with those from 2019 to 2020); they also validated some of the findings using an independent group of 12,258 mother-baby pairs from UC San Francisco.
The model’s predictions at birth provided more accurate information than currently used risk assessment tools such as Apgar scores and the National Institute of Child Health and Human Development risk score. These scores consider only the condition of the baby at birth and do not incorporate any information from the mother’s medical history, the researchers noted. However, additional studies in more diverse populations are needed before this machine-learning tool is ready to replace existing risk calculators at the bedside, the researchers said.
Mother’s health matters
The model revealed unexpected connections between certain health or social conditions in mothers and the health of their infants, according to the researchers.
For instance, mothers with anemia — a common pregnancy complication — were more likely to have newborns with anemia. These infants were also more likely to develop the bowel complication necrotizing enterocolitis, the study found.
“We need to explore what linkages explain these relationships at a biological level, as these might offer clues to how certain conditions occur,” Stevenson said. “That will allow us to intervene better to help those kids.”
The new algorithm was also able to link specific types of socioeconomic disadvantage in mothers with certain prematurity complications in their babies.
“If a mother was homeless, we found that the health impact on the baby would be different from the impact of incarceration, whereas under traditional paradigms both of these socioeconomic factors might be thought to have similar effects on prematurity risk,” Aghaeepour said.
Predictions from the model could help neonatologists better identify which patients will benefit from existing protocols to prevent birth complications, Stevenson said. For example, newborns who experience lack of oxygen during birth can now receive cooling protocols in early life, which lower their body temperature for a few days to prevent brain injury. Predictive scores may help identify additional infants who could be helped by cooling, he said.
The work needs to be replicated in larger, more diverse patient populations and folded together with other Stanford Medicine research that characterizes pregnancies according to thousands of biomarkers that change during gestation, the scientists said.
Source:https://med.stanford.edu/news/all-news/2023/02/prematurity-complications.html

An exodus of primary care doctors has officials re-imagining healthcare in South County
By Bill Seymour Special to the Independent Feb 17, 2023
Dr. Sal Abbruzzese recently opened his internal medicine practice in South Kingstown, where he works with his wife, Sarah. Abbruzzese, who was the president of South County Hospital medical staff until he resigned in December, is the first doctor to open a solo practice in the area in several years and says Southern Rhode Island’s lack of primary care doctors is a problem that is only going to get worse. “It’s like watching a train crash,” he said this week.

Stephanie Nowell of Charlestown got very sick on January 6 with various symptoms, visited a walk-in clinic and received antibiotics that didn’t work for her.
She returned to the walk-in once more and was given additional antibiotics that helped. Her primary care doctor had left the practice to which Nowell belonged and she was having difficulty finding a new doctor.
“If I had a primary care doctor I could have consulted with, I think I could have gotten better faster,” she said.
It is tough to get an appointment with an internal medicine doctor in South County today. Waiting times could be long and a walk-in medical treatment center, pharmacy clinic or hospital emergency room — when it’s not really needed — may be the only place to go.
The difficulty of finding a primary care physician stems from an exodus of them from the practice of medicine. Many doctors point to a variety of reasons for leaving and less interest in young medical students wanting to pursue general medicine.
Among the reasons are too much stress, onerous requirements by medical systems seeking to cut costs, insurance companies wanting detailed records to qualify for payment, low pay and overall changes in the practice of internal medicine that make it less fulfilling as a career.
In their place are an increase of mid-level medical professionals — often called advanced practice providers — like nurse practitioners and physician assistants.
Now these professionals are getting their day in the sun with a rise in demand for their needed skills that also come with less cost in billing to insurance companies and less training for patients.
In several interviews with physicians about the shortage of primary care doctors, all are pointing to more demands in their jobs that take away from patient care as frustrations and stress build. Most would only speak anonymously because of fear of repercussions from hospital systems.
“It’s like watching a train crash. I know what’s coming and it’s going to be a worse crash,” said Dr. Sal Abbruzzese, former president of the South County Hospital medical staff who departed in December to open up a practice in Wakefield. It is the first time in many years that a doctor has opened a solo practice in the area, he said.
“I have people calling me, leaving wine on my doorstep with a note asking to be taken on, referrals from many other doctors who just can’t take on any more patients. It’s incredible, I’ve never seen such a thing,” said Abbruzzese who started work as a doctor more than 20 years ago.
Other doctors in the area interviewed echoed similar statements about the administrative headaches now forcing them to leave practice or open up “concierge” services where a patient pays a multi-thousand-dollar fee — sometimes upwards of $3,000 or more.
The high out-of-pocket cost brings for the few that can afford this convenience round-the-clock access and the kind of personal attention often missing now from many busy practices focusing on patient volume or through-put.
“Yes, I would say that people could soon be up the creek without a paddle if this continues,” said Dr. Gloria Sun, another physician who shelved her general practice career because of excessive demands and is now in a job at the University of Rhode Island student health services.
However, leaving was not easy, she said.
“It was very difficult for me. I feel like I’ve given up,” she added in a voice that slowly and softly let out the words. Her youthful brimming enthusiasm and idealism have faded to later-in-life resignation to dealing with the current medical industrial complex.
A spokesman for South County Health pointed to the mid-level professionals stepping in as an inevitability in the industry as more doctors leave both on the local and national scenes.
“In a primary care setting, advanced practice providers will fill an increasingly important role as the physician workforce ages into retirement and fewer new physicians choose to establish practices in Rhode Island,” explained Matt Moeller, SCH spokesman.
These mid-level APPs are licensed nurse practitioners, physician assistants, advanced practice registered nurses and others. To help ease the transition of doctor-only visits for patients, health systems are lumping the term “advanced practice provider” to mean both the doctor and the mid-levels together in a “team” approach.
Gone from reference often these days is your “personal physician” or your “primary care physician” known colloquially as your “PCP.”
Fewer Internists
Local doctors, who did not want their names used, said that the practice of medicine in profit-centered medical systems has beaten down many general medicine doctors.
They feel beleaguered by too much medical records paperwork, low pay, and hard-driving measures putting performance — the volume of patients seen — over patient care to make up for reduced insurance payments.
Alarm bells were sounded in the state more than two years ago, according to state Department of Public Health officials, as evidence mounted that thousands of doctors could potentially leave primary care practice by 2030.
The shortage of primary care doctors is also a national problem, too. Many want out because retirement looks far better than dealing with defeating requirements for endless after-hours of filling out patients’ detailed electronic medical records (EMR), they say.
Sun was one of them.
“I was spending up to three hours every night on paperwork. It’s just so all-consuming, even for a short and simple visit. EMR is what is killing medicine,” she said about records needing to be filled out in exacting detail so that insurance companies don’t lowball reimbursements already low on a profit scale for operations of medical practices and hospitals, say health care business managers.
Abbruzzese, 50, who last month opened his private practice, said that health systems are “running doctors out of town. They are not providing us with the tools we need. They want more and more and give less and less.”
For example, he referenced that various tests are available only on certain days, needed scans cannot be done on weekends, picc lines are inserted only on particular days and “even the cafeteria staff wasn’t around on weekends.”
Making matters worse, he and others added, is that the COVID pandemic has pushed doctors to the brink of sacrificing their own health and many died across the country in that service. It brought about a new reality of their limitations in today’s world of medicine.
“When we older doctors went into practice, we were told by our older doctors that this is a lifestyle — not a job — and this is your life now. Your job is to take care of your patients. That is slipping away from many of my colleagues’ abilities to do,” he said.
For instance, 57-year-old Sun’s colleagues and patients call her a devoted doctor. One patient who had cancer and lost her husband after an accident in which he was paralyzed from the neck down found a trusted medical advisor and friend in Sun.
“I just love her. Please tell her to take me. I can’t find anyone in the area,” the former patient said. It’s a sentiment that plies on Sun and other doctors interviewed who also have changed their medical career paths.
Sun, like many doctors her age, entered medicine to help people overcome or cope with diseases and be compassionate as much as possible in times of real need.
For those in medical school today that mission in primary care is an unappealing career. It’s akin to a caged mouse on a wheel being electronically stimulated to go faster and faster, some medical students have said.
Burnout comes quickly. This upcoming generation of doctors values the work-life balance, so the cage is out of the question for many, say young doctors preferring specialties that have a less hectic pace.
Who’s left to help?
More and more health systems are putting a stronger focus on mid-level advanced practice providers to step in as South County Health is doing. Thundermist Health Center reported it started with mid-levels before the primary care doctor shortage became the current topic of public and media attention.
In federally reported training standards, the National Institute of Health said physicians, physician assistants (PAs), nurse practitioners (NPs) and advanced practice registered nurses (APRNs) have vastly different requirements for admission to graduate programs, clinical exposure, and postgraduate training.
The National Institute of Health reported that nurse practitioners on average have about 500 clinical contact hours in training compared to 2,000 for a physician’s assistant and 5,000 or more for a doctor. Neither the NP nor the PA has a residency requirement in training as does the medical doctor, NIH said.
For specialty areas, the PA or NP also has no further training, but the doctor has three- and four-year programs with 13,500 to 18,000 clinical hours.
According to the Bureau of Labor Statistics Occupational Outlook, growth projections for advanced practice providers are much faster than the average for other professions.
The projected growth for advanced practice registered nurses over the ten-year period 2019-2029 is 45%. Over the same period, physician assistant jobs are projected to grow by 31%.
Thundermist has had a nurse practitioner fellowship for over five years for training in community health and integrates them into its healthcare teams, said Amanda Barney, spokeswoman for Thundermist, which has offices in Wakefield.
She said that at Thundermist there is roughly a 50-50 split in the number of doctors compared to other primary care specialists and APPs.
Moeller of South County Health did not give a ratio, but said that in 2022 SCH hired six new primary care providers, defined as either APPs or doctors. Barney did not have any immediate figures on her organization’s hiring numbers last year.
With retirements and turnover, he said, “we are net positive two primary care providers during that same time.” Nonetheless, there remains a need for local primary care services.
“South County Health estimates there is demand for 6-12 additional primary care providers in Washington County,” he added.
“We are in the final stages of rolling out a formal program for on-boarding and mentoring nurse practitioners early in their career that have an interest in primary care,” Moeller said.
Like Thundermist, SCH’s primary care nurse practitioners and other APPs work in teams that include physicians, pharmacists, nurses and possibly social workers as needed. As with Thundermist, SCH also refers patients to specialists when needed.
More and increased training is underway as the need for them becomes more apparent.
“The mentorship program that South County Health is developing focuses on pairing new nurse practitioners with senior-level providers who have extensive experience navigating the healthcare landscape,” said Ian Clark, SCH vice president.
“It’s our hope this partnership will facilitate orienting those who are new to practice in Rhode Island to the intangibles, like working with our electronic health record, networking with other medical staff, and building a durable practice for long-term sustainability in the community,” he said.
“This program, we are confident, will allow us to increase the number of primary care nurse practitioners in our area and better meet the needs of the community,” Moeller added.
While APPs across the country are in many different medical services — oncology, orthopedics, surgery and neonatal — their use in primary care is also a boon for insurance and managed-care companies who may pay fees lower than they might for a medical doctor.
The State of Rhode Island licenses some advanced practice providers, like nurse practitioners, to also practice autonomously.
Increase Use of APPs
Last July a new survey of more than 60 organizations representing over 3,000 APPs nationwide found that three-fourths of diverse health systems have a strategy in place to increase the use of their APPs.
One of the largest studies focusing specifically on these roles, the 2022 Advanced Practice Provider Strategy & Oversight Survey provided key data points to help hospitals and medical groups.
These focus on better use of APPs while also spotlighting key areas for leaders to be aware of when pursuing an APP strategy, said the research firm the Coker Group.
This national healthcare advisory firm based in Alpharetta, Ga., found that organizations who said they are increasing APP involvement were responding to several market drivers, including the need to improve access to care including a shortage in primary care doctors, adapt to organizational growth, and improve the efficiency and quality of care.
These needs have been magnified nationally across healthcare following the COVID-19 pandemic and a growing labor shortage, it said.
“Our goal in creating this survey was to fill some of the gaps in data-driven information available and to better understand industry best practices,” said Matt Jensen, senior manager at the Coker Group.
“When organizations utilize APPs in the right way, they’re able to expand patient access, increase quality and drive performance. Across healthcare, however, hiring experienced APPs is extremely difficult, and the survey reflects that by showing just how many organizations are investing the time and resources required to onboard and train new APPs.”
It also pointed to challenges ahead, especially with resistant medical doctors who have concerns about APP training that is not as in-depth as full-scale medical school, internship, residency and fellowship that all bring over a decade of learning.
Roughly 67% of those polled said they allow their physicians to choose if they work with APPs for coverage of certain responsibilities. But about half of those physicians are hesitant to work with others, citing a heavy time commitment and a lack of incentive.
The experience of an APP also makes a difference in physicians’ use, with respondents indicating they spend more than 2.5 times the amount of time supervising APPs with less than two years of experience.
When asked about the barriers physicians have in a willingness to oversee APPs, the majority cited the time commitment and a lack of monetary incentive. While 46% of those overseeing APPs receive a fixed stipend for their supervision, 36% said there was no additional compensation.
Several local doctors did not want their names used when discussing the greater use of APPs. They acknowledged, however, that these advanced provider practitioners serve a vital role in handling minor issues.
“They are useful to support the practice and handle sinus infections, urinary tract infections and colds, but they need to know their limits,” one doctor said.
“You need to give new ones a lot of time — that you don’t have — to train them and this comes on top of all the other things, and a larger volume of patients that health systems want you to see. There aren’t the resources to help them,” a South Kingstown doctor added.
Abbruzzese was blunter.
“You get what you pay for, you get what you are trained in and it’s going to be a problem,” he said noting that doctors go through at least eight years of post-university training while for APPs it’s it far fewer.
“We’ll see what happens,” he said, while healthcare systems say they are putting bets on additional training and mentoring will add to the value of these professionals.
Source:https://www.independentri.com/news/article_e2a57180-ad84-11ed-ab0c-5b3ac57c8917.html

PREEMIE FAMILY PARTNERS

Courtesy Shakina Rajendram
Canadian siblings born four months early set record as the world’s most premature twins

By Paula Newton, CNN – March 9, 2023
CNN —
For expectant parents Shakina Rajendram and Kevin Nadarajah, the doctor’s words were both definitive and devastating: Their twins were not “viable.”
“Even in that moment, as I was hearing those words come out of the doctor’s mouth, I could still feel the babies very much alive within me. And so for me, I just wasn’t able to comprehend how babies who felt very much alive within me could not be viable,” Rajendram recalled.
Still, she knew that there was no way she would be able to carry to term. She had begun bleeding, and the doctor said she would give birth soon. The parents-to-be were told that they would be able to hold their babies but that they would not be resuscitated, as they were too premature.
Rajendram, 35, and Nadarajah, 37, had married and settled in Ajax, Ontario, about 35 miles east of Toronto, to start a family. They had conceived once before, but the pregnancy was ectopic – outside the uterus – and ended after a few months.
As crushing as the doctor’s news was, Nadarajah said, they both refused to believe their babies would not make it. And so they scoured the Internet, finding information that both alarmed and encouraged them. The babies were at just 21 weeks and five days gestation; to have a chance, they would need to stay in the womb a day and a half longer, and Rajendram would have to go to a specialized hospital that could treat “micropreemies.”
The earlier a baby is born, the higher the risk of death or serious disability, the US Centers for Disease Control and Prevention says. Babies born preterm, before 37 weeks gestation, can have breathing issues, digestive problems and brain bleeds. Development challenges and delays can also last a lifetime.
The problems can be especially severe for micropreemies, those born before 26 weeks gestation who weigh less than 26 ounces.
Research has found that infants born at 22 weeks who get active medical treatment have survival rates of 25% to 50%, according to a 2019 study.
Rajendram and Nadarajah requested a transfer to Mount Sinai Hospital in Toronto, one of a limited number of medical centers in North America that provides resuscitation and active care at 22 weeks gestation.
Then, they say, they “prayed hard,” with Rajendram determined to keep the babies inside her just a few hours longer.
Just one hour after midnight on March 4, 2022, at 22 weeks gestation, Adiah Laelynn Nadarajah was born weighing under 12 ounces. Her brother, Adrial Luka Nadarajah, joined her 23 minutes later, weighing not quite 15 ounces.
According to Guinness World Records, the pair are both the most premature and lightest twins ever born. The previous record holders for premature twins were the Ewoldt twins, born in Iowa at the gestational age of 22 weeks, 1 day.
It is a record these parents say they want broken as soon as possible so more babies are given the opportunity to survive.
“They were perfect in every sense to us,” Rajendram said. “They were born smaller than the palm of our hands. People still don’t believe us when we tell them.”
‘They’re definitely miracles’
The babies were born at just the right time to be eligible to receive proactive care, resuscitation, nutrition and vital organ support, according to Mount Sinai Hospital. Even an hour earlier, the care team may not have been able to intervene medically.
“We just didn’t really understand why that strict cut off at 22, but we know that the hospital had their reasons. They were in uncharted territory, and I know that they had to possibly create some parameters around what they could do,” Rajendram said.
“They’re definitely miracles,” Nadarajah said as he described seeing the twins in the neonatal intensive care unit for the first time and trying to come to terms with what they would go through in their fight to survive.
“I had challenging feelings, conflicting feelings, seeing how tiny they were on one hand, feeling the joy of seeing two babies on the second hand. I was thinking, ‘how much pain they are in?’ It was so conflicting. They were so tiny,” he said.
These risks and setbacks are common in the lives of micropreemies.
Dr. Prakesh Shah, the pediatrician-in-chief at Mount Sinai Hospital, said he was straightforward with the couple about the challenges ahead for their twins.
He warned of a struggle just to keep Adiah and Adrial breathing, let alone feed them.
The babies weighed little more than a can of soda, with their organs visible through translucent skin. The needle used to give them nutrition was less than 2 millimeters in diameter, about the size of a thin knitting needle.
“At some stage, many of us would have felt that, ‘is this the right thing to do for these babies?’ These babies were in significant pain, distress, and their skin was peeling off. Even removing surgical tape would mean that their skin would peel off,” Shah told CNN.
But what their parents saw gave them hope.
“We could see through their skin. We could see their hearts beating,” Rajendram said.
They had to weigh all the risks of going forward and agreeing to more and more medical intervention. There could be months or even years of painful, difficult treatment ahead, along with the long-term risks of things like muscle development problems, cerebral palsy, language delays, cognitive delays, blindness and deafness.
Rajendram and Nadarajah did not dare hope for another miracle, but they say they knew their babies were fighters, and they resolved to give them a chance at life.
“The strength that Kevin and I had as parents, we had to believe that our babies had that same strength, that they have that same resilience. And so yes, they would have to go through pain, and they’re going to continue going through difficult moments, even through their adult life, not only as premature babies. But we believed that they would have a stronger resolve, a resilience that would enable them to get through those painful moments in the NICU,” Rajendram said.
There were painful setbacks over nearly half a year of treatment in the hospital, especially in the first few weeks.
“There were several instances in the early days where we were asked about withdrawing care, that’s just a fact, and so those were the moments where we just rallied in prayer, and we saw a turnaround,” Nadarajah said.
Adiah spent 161 days in the hospital and went home on August 11, six days before her brother, Adrial, joined her there.
Adrial’s road has been a bit more difficult. He has been hospitalized three more times with various infections, sometimes spending weeks in the hospital.
Both siblings continue with specialist checkups and various types of therapy several times a month.
But the new parents are finally more at ease, celebrating their babies’ homecoming and learning all they can about their personalities.
The twins are now meeting many of the milestones of babies for their “corrected age,” where they would be if they were born at full-term.
“The one thing that really surprised me, when both of them were ready to go home, both of them went home without oxygen, no feeding tube, nothing, they just went home. They were feeding on their own and maintaining their oxygen,” Shah said.
Adiah is now very social and has long conversations with everyone she meets. Their parents describe Adrial as wise for his years, curious and intelligent, with a love of music.
“We feel it’s very important to highlight that contrary to what was expected of them, our babies are happy, healthy, active babies who are breathing and feeding on their own, rolling over, babbling all the time, growing well, playing, and enjoying life as babies,” Rajendram said.
These parents hope their story will inspire other families and health professionals to reassess the issue of viability before 22 weeks gestation, even when confronted with sobering survival rates and risks of long-term disability.
“Even five years ago, we would not have gone for it, if it was not for the better help we can now provide,” Shah said, adding that medical teams are using life-sustaining technology in a better way than in previous years. “It’s allowing us to sustain these babies, helping keep oxygen in their bodies, the role of carbon dioxide, without causing lung injury.”
Adiah and Adrial’s parents say they’re not expecting perfect children with perfect health but are striving to provide the best possible life for them.
“This journey has empowered us to advocate for the lives of other preterm infants like Adiah and Adrial, who would not be alive today if the boundaries of viability had not been challenged by their health care team,” Rajendram said.
Source:https://www.cnn.com/2023/03/09/health/earliest-premature-babies-canada/index.html

A NICU Baby Gives Hope to a Waiting Family
How a NICU team joined forces with social workers and an adoption agency to introduce a baby to her new family on Mother’s Day:
In April 2021, the sickest newborn in the neonatal intensive care unit (NICU) at Atrium Health Levine Children’s Hospital was born awaiting a family. She didn’t have a revolving door of visitors itching at the chance to hold her or anyone to make medical decisions for her. Her doctors didn’t know if the baby would survive her first week.
Just two months later, that baby girl – Evelyn – was healthy, happy and at home with a new family. The NICU team joined forces with an adoption agency, a caring birth mom, and an adoptive family to help this baby heal in the hospital and to create a happily-ever-after for her beyond it.
This is a story about one of the happiest moms celebrating Mother’s Day this year, Laura Cobb, and the team who connected her to her daughter, Evelyn.
A Heartbreaking First Week
With no family available to make decisions for the sick newborn, the NICU doctors cared for baby Evelyn like they would any other, and charted the medical course for her based on the standard of care and best practices.
“We think about each baby in terms of, ‘If this was my child, what would I want this team to do?’” says Jessica Clarke-Pounder, M.D., a neonatologist at Levine Children’s Hospital. “We treat each baby how we would want our family members treated, with the same gravity to decision making that we would have with our own children.”
Evelyn faced multiple life-threatening challenges during her first few days. For one, she was born with an infection and was delivered by emergency C-section due to fetal distress which led to required resuscitation by the NICU team in the delivery room. She was placed on therapeutic hypothermia protocol after delivery due to concern for brain injury. The baby also had meconium aspiration, in which feces enters the lungs. Then, Evelyn developed pulmonary hypertension. Then, kidney failure. Evelyn’s body was essentially shutting down, and she required a heart/lung bypass machine – called ECMO, or extracorporeal membrane oxygenation – to keep her alive. Evelyn was so fragile that the pediatric surgical team performed the surgery to place her on the ECMO pump inside the NICU.
“Levine Children’s Hospital is the only center in this area that offers ECMO. If she was born anywhere else, she would’ve had to be transferred,” says Dr. Clarke-Pounder. “The pump saved her life.”
The NICU team offered the little girl more than decision making. The NICU team offered her love. Doctors and nurses, full of all faith backgrounds, prayed over this little girl to heal. They cuddled the baby every chance they could.
By the end of that first week, Evelyn stabilized and was healthy enough to come off the ECMO machine. Her birth mom chose to pursue adoption, and social workers and an adoption agency helped her find a forever family for her baby.
The Worst Day Becomes the Best Day
Mother’s Day used to be Laura Cobb’s most dreaded day of the year.
For seven years, Laura and her husband James tried to have a baby. They learned they couldn’t have biological children, and the adoption process was slow. Mother’s Day weekends were so painful that the couple turned off their phones and went on off-grid getaways to be alone. The Friday before Mother’s Day of 2021, however, Laura’s phone rang as she drove home from work. She decided to answer one last call before turning it off.
It was the adoption agency, who told Laura about a very sick baby in the NICU who needed a family. The baby was stable, but she could face developmental hurdles and possibly brain damage. The agency told Laura that she and her husband should talk and pray about it.
“My husband and I were like, ‘No, we’ve prayed enough! This is what we’ve been praying for! This is our daughter!’” Laura says, smiling and wiping tears at the memory. “We are her parents, that is it. And so, we met her the very next day.”
On the day before Mother’s Day, they met the 10-day-old baby. Evelyn wore the cutest pink outfit to meet her new parents. Laura later learned the outfit was a personal gift from someone who loved Evelyn, too: Dr. Clarke-Pounder.
“There are there lots of families that, for one reason or another, can’t be in the NICU. Families can feel a lot of guilt over that, but there are moms and dads who have limited time off from work, or babies who get transferred here from far away,” Dr. Clarke-Pounder says. “Every baby who’s there, especially ones who don’t have families, we really take care of them as if they’re our family.”
A Big Team Supports a Little Baby
Laura and James joined an already large group of people who were part of Team Evelyn. There were NICU doctors, nurse practitioners, pediatric surgeons, respiratory therapists, ECMO therapists, gastrointestinal specialists, speech therapists, social workers, and an adoption agency.
People across many disciplines collaborated to create a seamless care plan to support this little girl.
While James needed to return to work, Laura came to the NICU daily to hold Evelyn, to sing to her, and to work with the therapists as they taught the little girl to take a bottle.
“At first, I didn’t want to leave Evelyn because I didn’t want her to feel alone, but she wasn’t alone. She was so loved by the nurses and doctors, who were amazing. They were her family before we were,” Laura says. “And I felt taken care of by them just as much.”
About a month later, Evelyn learned how to take a bottle and she became strong enough to go home with the Cobbs. Before the family left the hospital together, the NICU team helped them make follow-up appointments with specialists and a pediatrician to help them transition to the next stage of their daughter’s care.
A Healthy Little Girl, a Grateful New Mom
Evelyn just celebrated her first birthday. She returns for developmental appointments at a neonatal follow up office, which works with her pediatrician to make sure she’s developing appropriately. All signs point to a healthy little girl, developing on schedule.
Laura says that the past year has shown her a capacity to love beyond what she’s ever known: for Evelyn, for Evelyn’s birth mother who continues to be a loving presence in her daughter’s life and for the NICU doctors and nurses.
Now, Laura’s preparing to celebrate her second happy Mother’s Day.
“Because Mother’s Day weekend is the weekend we met Evelyn, it’s our family weekend,” Laura says. “It’s not about me. It’s about Evelyn, and it’s about honoring her birth mom. I’ve never met someone as strong and courageous and faith-filled as her birth mom – she’s amazing.”
The Cobbs remain in touch with Dr. Clarke-Pounder, sending her photos and updates of the baby she guided through those first few scary weeks.
“It was really special to me to see Evelyn progress from being the sickest baby in the NICU to becoming a baby who went home with a loving family,” Dr. Clarke-Pounder says. “It is really special when families are so impacted that they choose to stay in contact with us, and it’s really nice to see that our hard work has paid off.”
Laura kept the pink outfit that Dr. Clarke-Pounder gave Evelyn on the day the family met.
“One day I’m going to show Evelyn this outfit,” Laura says. “And I’m going to tell her, ‘This was from your doctor – she loved you before I even met you.’”
Source:https://atriumhealth.org/dailydose/2022/04/28/a-nicu-baby-gives-hope-to-a-waiting-family


A NICU Baby Gives Hope to a Waiting Family – YOUTUBE

INNOVATIONS

Norwegian paediatric residents surveyed on whether they would want life support for their own extremely preterm infant
Janicke Syltern, Trond Markestad 18 January 2023

Advances in perinatal and neonatal medicine have made it possible for preterm infants to survive at earlier ages. However, survival rates vary substantially between high-income countries and perinatal centres, suggesting that attitudes on providing life support differs. Survival rates for live-born infants vary, particularly at 22–23 weeks of gestation, but differences extend to 27 weeks when stillbirths are included. This suggests that proactive, life-saving prenatal care vary across a wider range of gestational ages. Differences may be due to variations in legislation or values, national or local consensuses by involved health professionals and how parents are included in decision making. Although there are multiple prognostic factors, the vulnerability of extremely preterm infants increases profoundly with decreasing gestational age in terms of survival, neonatal morbidity, burden of treatment and subsequent physical and mental health. Some European guidelines on resuscitating premature newborns have been developed by just perinatologists and neonatologists and they particularly vary on how active interventions should be at 22–25 weeks.
In Norway, guidelines based on the 1998 national consensus state that life support is standard care from 25 weeks. Infants born at 23–24 weeks should be individually assessed by neonatologists and consider the parents’ opinions. Life support at 22 weeks should be regarded as experimental. In practice, the so-called grey zone of 23–24 weeks has been narrowed down to 23 weeks, based on 2009–2014 data. This showed that 97% of infants born at 24 weeks were transferred to a neonatal intensive care unit, as were 74% born at 23 weeks and 19% born at 22 weeks. We have no data on how parents were involved in the decision-making process.
This study explored whether Norwegian paediatric residents would want life support to be provided if their own hypothetical preterm infant was born at 22–26 week of gestation. Short questionnaires, which were distributed after one-week compulsory national training courses in neonatology, were completed anonymously by 80/96 (83%) of participants, on paper in 2017 and 2019 and as an online Mentimeter survey (Mentimeter AB) in 2020. Most participants were in their thirties, with a median paediatric residency of 36 (range 3–84) months. The majority (94%) would not have wanted life support at 22 weeks, 73% at 23 weeks, 36% at 24 weeks and 8% at 25 weeks. One wanted life support before 24 weeks, 14% at 24 weeks, 59% at 25 weeks and 79% at 26 weeks. A particularly large percentage (50%) were unsure at 24 weeks (Table 1).
TABLE 1. How 80 Norwegian paediatric residents responded to whether they would want their hypothetical child to receive life support at 22–26 weeks of gestational age.
| Yes | Not sure | No | |
| 22 weeks, n (%) | 1 (1) | 4 (5) | 75 (94) |
| 23 weeks, n (%) | 0 (0) | 22 (28) | 58 (73) |
| 24 weeks, n (%) | 11 (14) | 40 (50) | 29 (36) |
| 25 weeks, n (%) | 47 (59) | 27 (34) | 6 (8) |
| 26 weeks, n (%) | 63 (79) | 12 (15) | 5 (6) |
The residents’ opinions were even more restrictive than the 1998 guidelines and deviated markedly from current Norwegian practice. This could challenge the golden rule of treating others as we would want to be treated. Although we cannot assume that others share our preferences, it seems unethical to impose what we would not want ourselves on them, without providing real choice. Most importantly, this hypothetical question may not predict what would happen in real life. However, the residents were at a common age for parenthood, knew the risks and burdens of treatment and had already had time to reflect on the issue during their clinical training and the newly completed course. In contrast, parents are generally unprepared and at the mercy of neonatal intensive care practices and how physicians provide information and frame alternatives.
Our findings agreed with other studies on whether informed healthcare personnel would want life support for their own infant. One found that only 54% of Norwegian paediatricians would want this at 24 weeks and another reported that 23/24 Australian neonatal nurses would not want this before 25 weeks. It seems unlikely that discrepancies between the attitudes of healthcare personnel and neonatal intensive care practices reflect different moral values of healthcare personnel and potential parents. It points towards different experiences and the burden and urgency when healthcare personnel and parents make difficult decisions. Although some parents of premature babies accept disabilities more than healthcare personnel, parents also worry about the short-term and long-term suffering of their baby and family and want to be involved in decision making.
Improved survival rates may encourage neonatologists to resuscitate ever more immature infants, but their decisions need to reflect society’s moral norms. We believe that national guidelines on challenging ethical medical dilemmas like this should not just be left to involved healthcare personnel. Relevant stakeholders should include professionals with experience from long-term follow-up, educators, ethicists, lawmakers and public representatives. Parents should be involved if decisions about providing life support fall within an agreed grey zone, where the child’s best interests are not clear. We believe that guidelines based on broad social support will increase social awareness about the ethical dilemmas of periviability and promote transparency. These are prerequisites for parents to become competent decision-making partners. We need to speak about values as well as medical facts and statistics. In our experience, parents need a trusting and open atmosphere to voice their doubts. Many of the paediatric residents we surveyed would have preferred a palliative approach for their own vulnerable infant and knowing this may encourage open dialogues about complex decisions at the margin of viability.
Source:https://onlinelibrary.wiley.com/doi/full/10.1111/apa.16631

Strengthening neonatal and obstetric healthcare in the war-affected regions of Ukraine

9 Mar 2023 by Milena Chodoła and Dorota Zadroga
At the end of February, the Polish Medical Mission completed the first six months of the one-year project titled “Strengthening neonatal and obstetric healthcare in the war-affected regions of Ukraine”. Activities are being implemented in 10 neonatology hospitals in Ukraine, located in the cities of Kyiv, Dnipro, Chernihiv, Kharkiv, Chernivtsi, Zaporizhzhia, Poltava and Lviv. Cooperation with Ukrainian neonatologists in supporting this branch of medicine is a continuation of one of the leading projects of the Polish Medical Mission’s portfolio worldwide. The Polish association is carrying out similar activities in Colombia, Venezuela and Tanzania. The organization became involved in activities to help Ukraine’s healthcare system after the conflict began, providing specialized assistance to hospitals across the country.
In the first quarter of the project, starting September 1st 2022, a needs assessment on medical training for Neonatology and Neonatal Intensive Care Units (NICUs) was conducted in 10 hospitals. Based on it, a training plan (including the approach, methodology, scheme and work plan of trainers) was prepared, taking into account the current needs of each hospital. The process of purchasing specialized equipment has also begun — an advanced and high-quality neonatal resuscitation station, as well as a neonatal patient monitor (for measuring and analyzing vital signs) and a neonatal infusion pump were on the list for each institution. In accordance with the schedule, a complete plan of activities for the next second quarter of the project was developed by the end of November. Cooperation agreements with hospitals were signed and a project team of 27 staff members was recruited in Ukraine, including medical training coordinators, medical trainers, patient rights training coordinators, patient rights educators and administrative representatives of hospitals.
As part of the support for pregnant and postpartum patients, a series of onsite sessions raising awareness of patients’ rights, pregnancy and newborn care, will be held up monthly at each of the hospitals included in the project. Of the planned 80 trainings, 10 have already taken place, one at each facility. A total of 102 patients have taken part in them. There have also been two complementary online sessions (out of a planned 8) raising awareness about patients’ rights, pregnancy and newborn care for women who are patients or whose newborns are patients. A total of 42 female patients attended.
The second quarter was devoted to equipping hospitals and launching medical and patient rights trainings for health workers and awareness-raising sessions for patients. In each of the 10 hospitals, also stationary training sessions were being held for medical personnel in the use of neonatal resuscitation stations and neonatal patient monitors.
In December 2022, stationary medical training for staff of the neonatology and obstetrics departments began, ending in early February 2023. The project held one 4-day medical training in each of the 10 hospitals. A total of 346 doctors from Ukraine participated in all 10 medical trainings (the project’s indicators planned for a minimum of 100 doctors from 10 hospitals to participate in in-person medical trainings, more than tripling the expected result).
Prior to attending the in-person medical trainings for health workers in 10 hospitals, trainees filled out an anonymous knowledge test, which was repeated upon its completion. By compiling the results from the test before the training, as well as after the training, it was verified to what extent the trainees raised their level of knowledge. Approximately 95% of the participating doctors increased their level of knowledge in the topics that were covered in the training. They also filled out an anonymous questionnaire surveying their level of satisfaction with the training. Some 93% of the doctors gave the maximum score for the training, or 5 points; the remaining 7% of doctors rated the training on a scale of 4 to 4.9 points.
In the second half of January 2023, two online events were also organized on the Ukrainian medical platform Medvoice, streaming from January 17-19, while recordings of them are now available online. One, titled “Becoming a mom during wartime: important things to know”, is prepared for patients across Ukraine. The webinar has been replayed 780 times so far (February 28, 2023). The second is aimed at medical professionals, also across Ukraine, and was titled “Doctor-patient communication: foreign practices and Ukrainian realities”. So far, 1,607 doctors from Ukraine have registered, of which 995 doctors took the online course, passed the test and received a certificate. The events were held under the auspices of the National Health Service of Ukraine. In addition, the online course for doctors has been registered with the Ministry of Health of Ukraine, so doctors who participated and passed the online test received a certificate and official credits from the Ministry, which doctors collect to confirm the continuous development of their professional qualifications.
On February 16, 2023 the second online training on patient rights was held for the medical staff of the 10 neonatology hospitals participating in the project (a total of 8 such online trainings conducted at regular intervals are planned). A total of 50 doctors from 10 hospitals have already participated in these trainings. The purpose of the meetings run on the Zoom platform is to raise awareness among medical professionals about patient rights, legal liability of hospitals and doctors, communication with patients, and counteracting professional burnout and taking care of doctors’ well-being. It also demonstrates good practices used by Polish and EU doctors in the field of patient rights. Small groups allow participants to exchange insights and experiences, and to a greater extent assimilate the knowledge from the training.
Total numbers:
- 10 NICUs in project
- 995 trained medical staff representatives in online course on patient rights on Medvoice
- 346 trained medical staff representatives in stationary medical training
- 50 trained medical staff representatives in online trainings on patient rights
- 780 patients in webinar on Medvoice
- 144 patients in online and stationary awareness-raising sessions

Improvement of Maternal Morbidity and Mortality: Maternal Level of Care, Maternal Transport, and Regionalization
Mary Fang, BS M.D. Candidate
In my mind’s eye, I painted a picture of her experience flying here. She lay down to get her routine ultrasound done and watch the grayscale frames of the twins headknocking inside her uterus, eager to share some polaroids of her growing babes with her husband that evening, suddenly gazing back to the screen, which showed red and blue lines over her cervix she did not remember seeing or being told about previously. She was not going to go home that evening; she was going to the hospital via airlift from an island to the mainland major hospital. Mrs. Smith was tearful and expressed difficulty understanding why doctors recommended she stay in-patient in a hospital far from home for the remainder of her pregnancy, which she had just learned would end four weeks earlier than initially planned. She felt no change compared to before that ultrasound visit, where type I vasa previa and absent end diastolic flow of growth-restricted twin A were newly diagnosed. With the constellation of mo-di twins, vasa previa, and AEDF (absent end-diastolic flow), the possibility of her needing to be transported urgently or emergently was significant. However, with her now at a high-level care center, the transport would be up the elevator, not in an ambulance or aircraft, when life or death could be a matter of milliliters of fetal blood within minutes.
Perinatal care, comprised of the maternal-fetal/neonatal triad, has improved throughout the decades. However, the improvement is predominantly based on improved neonatal outcomes. Implementing risk-appropriate neonatal care in the 1970s has significantly reduced neonatal and infant morbidity and mortality, especially among very low birthweight infants that receive appropriate care in at least a level III NICU. However, the other side of the perinatal triad, the maternal side, continues to face rises in maternal mortality and morbidity in the U.S., especially among women of color. The longstanding neonatal model of levels of care has more recently inspired similar maternal levels of care models, whereby each level has a minimum ability related to staffing and resources. Appropriate level of maternal care spans the antenatal, perinatal, and postpartum periods. Efforts for assigning levels of maternal care at the national level are at their early stages, with mandatory versus voluntary efforts by the state. Efforts were piloted in 14 hospitals in 3 states in 2017. In Texas, the first iteration of maternity designation was codified in 2018, and all facilities in Texas were designated a level by September 2021 by the Department of State Health Services. Level 1 centers provide basic care to low to moderate-risk pregnant patients and detect, stabilize, and initiate management until the patient is transferred. Level 2 facilities provide specialty care, and level 3 facilities provide subspecialty care and are equipped to manage complex maternal and obstetric complications. Level 4 facilities are regional perinatal health care centers that are equipped to manage the most complex conditions and critically ill pregnant patients. There are challenges with adoption and acceptance in other states due to concern primarily for lower level hospitals and the process of applying, preparing prior to site review, the site review, and post-site report.
Despite the aforementioned concerns, regionalization through identifying high-level facilities and maternal transport is necessary to improve outcomes based on assigned risk. Maternal transport is one of the keystones for improving mortality or major morbidity through transferring care from a low-acuity to a high-acuity facility. These improved outcomes relate to preventing near-miss events, adverse outcomes that may have occurred in the absence of transport. However, maternal transport accessibility is not equal or equitable due to differences in time and distance from the nearest high-acuity center, inefficient identification of the nearest center, and/or lack of clear hospital protocols to appropriately transfer patients who require it. Improving equitable access to transfer to appropriate levels of care, especially highlighted in rural facilities, demands hospital-level quality improvement initiatives, including identifying patients who need transport and clear plans on the method of transport and distance. Reasons for maternal transfer fall into maternal and/or fetal/neonatal indications. While the most common reason is the lack of availability of appropriate-level neonatal care, maternal medical or surgical conditions or emergency care at a facility without obstetric services also require transfer. Improved maternal regionalization is another effort to facilitate the transfer of care via defining relationships between different level facilities and labeling the capabilities of a facility. Some instances may necessitate the identification of multiple higher-level facilities, depending on the facility’s capacity to accept new transfers. Mode-of-transport (i.e., ambulance versus airlift) is also an important consideration, reliant on distance, urgency, and availability of the transport means.
Fragmentation of perinatal care also contributes to increased morbidity and mortality. This discordance is multi-fold, with some facilities with appropriate high-level care for the maternal side but not the neonatal side, or vice versa, and hospitals without MFMs or neonatologists within a 10-mile radius. This incongruity between appropriate maternal and neonatal care availability significantly affects outcomes for high-risk pregnancies. Studies have demonstrated improved outcomes for maternal transfer for neonatal indications prenatally versus postnatally. Improved regionalization can help increase the number of high-risk births occurring at the appropriate-level facility, avoiding separation of the mother and newborn after birth. This is achieved by better defining the scope of maternal and neonatal care concurrently to plan for delivery at a center that provides appropriate care for both the mother and the newborn.
Risk stratification and planning for delivery for high-risk pregnancies in advance require longitudinal care by a multidisciplinary team, including a maternal-fetal medicine specialist. Adequate prenatal care aids in the delivery plan by identifying and monitoring high-risk conditions. Unfortunately, there also exist disparities in the adequacy of prenatal care and, subsequently, differences in access to management by MFM. Co-morbidities that are unidentified or not adequately managed during pregnancy, including interval ultrasounds and antenatal testing, increase morbidity and mortality. In such cases, without access to routine prenatal care, presentations to care are often only to the emergency room, which might not be able to take care of the obstetric emergency, especially if it was undiagnosed beforehand due to lack of longitudinal obstetric care. An undiagnosed obstetric condition presenting for the first time in an emergent setting without appropriate resources and personnel can further delay transfer due to the stabilization requirement before transfer. Perinatal health includes consideration of the maternal and fetal/neonatal perspectives. Conditions associated with maternal morbidity and mortality can directly impact fetal/neonatal outcomes and thus warrant high-level care antenatally with an MFM to make decisions about antenatal surveillance and include other specialists during the pregnancy.
Accurate risk stratification depends on identifying and controlling co-morbidities identified antenatally and informs management during the antenatal, perinatal, and postnatal/postpartum period, including assigning the appropriate level of care. As high-risk maternal patients are often associated with high-risk fetal/neonatal counterparts, planning care at a facility with level-appropriate care for both the mother and newborn improves outcomes. Maternal transport and regionalization, in addition to risk stratification, improve maternal morbidity and mortality with care at a facility equipped with resources and personnel to adequately and promptly respond appropriately. Lack of access to prenatal or MFM care and, thus, inappropriate diagnosis and management of maternal and/or fetal conditions underlie disparities in outcomes despite these improvements. Fortunately, identifying the barriers and inequities in accessing appropriate levels of care is ongoing, leading to the development of quality, evidence-based tools to lessen these gaps.


The connecting power of shared laughter | Karen Eddington | TEDxIdahoFalls
Shared laughter reverses the belief that we are alone. The most dangerous emotion we face is mental isolation. How would your life be different IF you felt connected? We can solve the struggle of when you are surrounded by people yet still feel alone. Karen Eddington is the author of Understanding Self-Worth and she uses her experience in stand-up comedy and improv to teach laughter as a form of self-care. This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at http://ted.com/tedx



In times of stress and vulnerability practicing humor can be instrumental in helping us move through life’s challenges. Humor can help us connect with ourselves and others on a more intimate level. Being met with some challenges in my personal life recently, it’s the simple moments with close friends that have helped me see the humor within certain circumstances I am navigating. Finding ways to laugh about ourselves, the things we tend to take at times too seriously, and engaging with humor in our seemingly mundane moments can help us find the positive momentum we need to keep moving forward in a positive direction.
Finding comfort in bringing laughter to those we hold close and appreciating the funny moments we share with ourselves and others is food for our souls. Who are some of the people and things in your life that bring you laughter? How does humor empower your relationship with yourself and others, and enhance your life journey?
I believe by choosing joy, laughter, and engaging in some light-hearted fun through humor we can learn to embrace our grace. With April Fools around the corner my hope is that together we can bring a little more light into our world through the laughter we spark in each other.


Surfing in Venezuela


