


Ireland is an island in the North Atlantic. It is separated from Great Britain to its east by the North Channel, the Irish Sea, and St George’s Channel. Ireland is the second-largest island of the British Isles, the third-largest in Europe, and the twentieth-largest on Earth.
Geopolitically, Ireland is divided between the Republic of Ireland (officially named Ireland), which covers five-sixths of the island, and Northern Ireland, which is part of the United Kingdom. In 2011, the population of Ireland was about 6.6 million, ranking it the second-most populous island in Europe after Great Britain. As of 2016, 4.8 million lived in the Republic of Ireland, and 1.8 million in Northern Ireland.
Health care in Ireland is delivered through public and private healthcare. The public health care system is governed by the Health Act 2004, which established a new body to be responsible for providing health and personal social services to everyone living in Ireland – the Health Service Executive. The new national health service came into being officially on 1 January 2005; however the new structures are currently in the process of being established as the reform programme continues. In addition to the public-sector, there is also a large private healthcare market.
Source:https://en.wikipedia.org/wiki/Ireland
PRETERM BIRTH RATES – Ireland
Rank: 170 –Rate: 6.4 Estimated # of preterm births per 100 live births
(USA – 12 %, Global Average: 11.1%)

COMMUNITY
We applaud the collaborative work INHA shares with our global preterm birth community. Numerous resources of significant value are provided through the INHA website. An important example we are sharing below targets the journey of loss of a preemie infant/infants.

The INHA is Ireland’s first collaborative platform and network to represent the interests of preterm infants, ill infants in the Neonatal Intensive Care Units (NICU) and their families. It comprises of families affected by a preterm birth, multi-disciplinary healthcare experts, educators, researchers, political decision makers and industry partners who share the common goal of reducing the incidence of preterm birth in Ireland, supporting families with infants in the NICU and improving the long-term health of preterm infants by ensuring the optimum prevention, treatment, care and support.
Our vision is to support and empower families affected by prematurity by advocating increased awareness, improved pre-conceptual, ante-natal and post natal education, equitable and standardized neonatal care and improved long-term care for both the premature baby and the family.
Resources for Bereaved Parents
If your baby has died, this is a devastating loss for you and your family. We are working hard to develop bereavement supports and resources for families whose baby has died some of which are outlined below.
We have produced a suite of information booklets on baby loss. Two of these booklets aim to offer support and guidance to you as bereaved parents who have experienced loss of your baby (babies). You can download them below:
- When your baby has died: a guide to coping with grief and loss
- Loss in a multiple pregnancy: a guide for parents to coping with grief and loss
We have also developed two booklets which contain a collection of 20 short stories written by bereaved parents about life after loss of their baby or babies.
- Download “A memoir of life after loss in a singleton pregnancy”
- Download “A memoir of life after loss in a multiple pregnancy”
In addition, we have developed a guide for bereaved parents, which offers guidance about parenting your surviving twin or triplet (s).
Recommended books
Books for children about loss of a baby brother or sister
- Where are you Lydie? by Emma Poore
- ‘The Story Of…’ personalised books
- We Were Gonna Have a Baby, But We Had an Angel Instead by Pat Schwiebert
- Someone Came Before You by Pat Schwiebert
- Perfectly Imperfect Family by Amie Lands
- Something happened by Cathy Blanford
- These Precious Little People by Frankie Brunker
- Always My Twin by Valerie Samuels
- I’ll Always Be a Preemie Twin by Nicki Cooper
- Two Little Monkeys by Kimberly Jackson
Source:https://www.inha.ie/resources-bereaved-parents/

Prof John Murphy: ‘The modern intensive care unit is a quiet place.’ Photograph: Dara Mac Dónaill
‘A lot of people don’t know neonatology exists – until they get a small baby who is sick’
Over the decades, Prof John Murphy has seen many advances in the care of newborns
Tue, Oct 26, 2021 – Sheila Wayman
On the pavement outside the front door of the National Maternity Hospital on Holles Street, a neonatal nurse and neonatal doctor are preparing to clamber into a waiting ambulance that is adapted for the transport of critically ill newborn babies.
As consultant neonatologist Prof John Murphy walks by, he stops to have a quick word about what has been a busy week for this transport team, which can be mobilised within 20 minutes of a call. The three Dublin maternity hospitals take turns to supply specialist staff for the National Neonatal Transport Programme and this is the NMH’s week on, with the crew about to depart for Cork, having been to Sligo the day before.
It’s now a 24/7 transport service, in no small part thanks to Murphy who, as clinical lead for the National Clinical Programme for Paediatrics and Neonatology, oversaw its expansion from a 9am-5pm operation. This speedy, specialised transfer of infants to the Republic’s four tertiary neonatal intensive care units (NICUs) – three in Dublin, one in Cork – is one of many innovations in the care of newborns over recent decades that have all played a part in the saving of thousands of fragile lives.
Back in 1970, for every 1,000 live births in Ireland, 13 babies would die within the first month. By 2019, that rate had dropped to two per 1,000 live births.
“For every 1,000 births, an additional 11 babies now go home alive,” says Murphy, whose 35 years as a neonatologist in the NMH and Temple Street hospital have spanned many advances in the care of newborns. For instance, he can still remember, in 1992, giving the first dose of surfactant, which “looks like skim milk” and helps babies with immature lungs to breathe.
“I couldn’t believe it. A baby that was very blue and unwell suddenly going very pink; the change was so dramatic. That was a key, life-saving event, one of the keys that unlocked the door to survival of small babies. You could put a tube into their windpipe and give it to them and that made their lungs very flexible and that had a huge impact on mortality.”
Tiny babies of just 23 weeks’ gestation now have a fighting chance of life, while the survival rate for those who reach 26 weeks before birth is close on 80 per cent.
Murphy was “surprised and flattered” to be this year’s recipient of the Kathleen Lynn Medal, awarded by the Royal College of Physicians of Ireland (RCPI) for “exceptional service on behalf of children.” Nevertheless, in this interview to mark the occasion, he is quick to deflect any reflection of personal achievement and instead welcomes it as “very good recognition of neonatology, which is not necessarily the most widely known speciality. I think a lot of people don’t know it exists – until they get a small baby who is sick,” he says, sitting in a boardroom at the top of NMH offices on Mount Street.
Neonatology is a speciality in medical and nursing care that only began to emerge in the 1960s. Other professionals, including dietitians, pharmacists, psychologists and clinical engineers who maintain NICUs’ complex equipment, now have vital roles in the field too.
Covering the care of all babies from birth until one month of age, he describes neonatology as “the ‘human turnstile’ through which everyone passes,” as we adapt to life outside the womb. About 10 per cent of babies require admission to a special care baby unit, although the time spent there may range from hours to several months.
The death of baby Patrick Bouvier Kennedy in August 1963, just three months before his father, US president John F Kennedy, was assassinated, kickstarted huge investment into research around prematurity. Jacqueline Kennedy, who missed her husband’s trip to Ireland earlier that summer due to the pregnancy, had to have a Caesarean section to deliver their infant son 5½ weeks early. Suffering from respiratory distress syndrome, he lived only 39 hours, despite access to the best medical care the US could offer at the time.
Today, he would be a very routine case in any neonatal unit. Although 7 per cent of babies born in Ireland are premature, defined as less than 37 weeks’ gestation, “only about 1-2 per cent of those are really immature and going to cause all the problems”, says Murphy. Initially, neonatology was all about saving lives but its focus has broadened to trying to minimise lifelong effects of a baby’s early departure from its mothership. The brain is the new frontier in the constant quest for improved neonatal care.
“Once you meet a level of survival and your specialty matures, you begin to look at the quality of survival, that is what you are really after.”
Low birthweight, sometimes no more than half a standard bag of sugar, is not the principal problem in itself. Rather, it is the immaturity of their organs. Also, their skin is thin, resulting in a “lobster red” appearance and making them liable to rapid loss of heat and water, as well as open to infections.
Murphy, described as “a true prince of neonatology and paediatrics in Ireland” in the award citation delivered by Royal College of Surgeons in Ireland -Bahrain vice-president and fellow paediatrician Prof Alf Nicholson, traces his choice of career back to childhood. At home in Cork city he used to watch Dr Finlay’s Casebook, a 1960s TV series about a doctor working in the fictional Scottish town of Tannochbrae. “I saw him one day going into a house and seeing a child who was sick and making a diagnosis of meningitis. Then doing a lumbar puncture and the child got better; I thought, ‘I’m going to do that’.” He successfully applied to study medicine at University College Cork.
During medical training, the sight of a baby with apnoea breathing irregularly, made a big impression on him. There was no treatment for it at the time and it made him think if only there was something that could be done. That was before the administration of caffeine was discovered to be really effective for treating this condition, by improving the contracting of the diaphragm.
After several years of further training in the UK, Murphy was the first consultant neonatologist appointed in Wales, before returning to Ireland in 1986 to become one of three at the NMH. Since then, big changes he has worked through include the handling of sensory issues in neonatal care. “There was a time when people were probably less aware of pain in babies. My rule of thumb is that if I find something painful, the baby is jolly well going to find it painful too.”
Loud noises can be very upsetting for these babies who cannot yet filter stimuli. “The modern intensive care unit is a quiet place. No hoovers are allowed in, the floor must be brushed; phones are put on a light system so less noisy.
“Then we have these quiet hours where all the lights go out in the unit and everybody speaks in a whisper and activity goes right down so the babies can rest.” Things that have to be done for a baby, such as taking a blood sample, a swab, changing a nappy, are planned, to reduce the number of disturbances.
“It’s all an attempt to replicate what goes on in the womb, which is really protective, but also to recognise that over-stimulation of these babies may have consequences on their development.”
Another simple intervention has been the placement of preterm babies in a plastic bag immediately after birth to keep them warm before transfer to an incubator. They can lose up to 1 degree Celsius a minute and when once, he recalls, theatre and corridor windows were hastily closed in an effort to alleviate heat loss, this “phenomenal technique” now does a very effective job.
He’s also seen the introduction of nitric oxide gas for the treatment of respiratory distress syndrome and improvements in minimising brain injuries in preterms through the giving of steroids to mothers at risk of premature delivery.
Tracking how these babies fare after they are discharged is vital. At the NMH, the neonatal department’s clinical development psychologist Marie Slevin sees all premature babies back at two years of age for what is known as the Bayley assessment, looking at cognitive skills and speech and language development.
Prof John Murphy is this year’s recipient of the Kathleen Lynn Medal, awarded by the Royal College of Physicians of Ireland for ‘exceptional service on behalf of children.’
“It is very helpful to be constantly getting the feedback,” says Murphy, who sees upcoming World Prematurity Day on November 17th as a way to mark the impact prematurity has on society. “There are very few families, either parents or grandparents, uncles or aunts, who won’t have come across, or had, a baby that was preterm.”
Incidence of prematurity has gone up, mainly because multiple births are a big factor and the rate of twinning has increased significantly, due to more widespread use of assisted reproduction. The Economic and Social Research Institute reported a twinning rate of 18.8 per 1,000 maternities for 2016, an increase of 22.1 per cent over the previous decade.
At the NMH on November 17th, as at other maternity hospitals, some “preemies” and their parents are invited in to celebrate what is achieved within the walls of their NICU. But these are not the only cohort of former patients that Murphy is always delighted to see come bouncing back.
There are also full-term babies for whom the treatment of therapeutic hypothermia (TH), introduced in Ireland in 2009, has proven to be “one of the most amazing changes” in the prevention of disability resulting from oxygen deprivation during birth. Such babies are at high risk of cerebral palsy.
With TH, a cooling jacket is used to lower a baby’s body temperature to 33.5 degrees Celsius, about four degrees lower than normal, within six hours of birth and until it’s 72 hours old. Nobody yet knows precisely how it works, he explains, “but if we learn more about that, we may be able to use some pharmacological methods as well as this physical method of cooling. It seems to act by slowing down, or cooling, the brain activity – and that way the brain cells get a chance to recover.”
About 70 babies are cooled in Ireland every year, giving good results in the term of outcomes. For every case, antenatal, labour and neonatal data is collected and analysed to help increase knowledge in maternity hospitals about oxygen deprivation and see if and where it might have been preventable.
“It has been very rewarding to me to see children who obviously have got a problem at birth and then they have been cooled – and then see them running into you at a clinic, when I would have seen the opposite. As the cooling has gone on, it’s got better and the equipment has got better. And we have got better at managing it.”
Murphy acknowledges the “dichotomy” in keeping preterm babies warm to save life and then cooling some full-term babies to do likewise. “A lot of medicine is counter-intuitive – it doesn’t work out the way you think it’s going to work out,” he says.
Hundreds of trainee paediatricians have benefited from his experience and inspiring passion for the care of the youngest possible members of our population. The training programme set up by the RCPI’s faculty of paediatrics, established in 1992, is, he asserts, “second to none”. About 40 doctors come into it annually after completing their intern year and do an initial two years. They can progress to higher specialist training, which takes another five years.
“They come out at the end of that with their certificate of full training, which is recognised very well internationally. All our young consultants who have been appointed in recent years have all come through our training system, which is very flattering in a way that all these bright young doctors have chosen to stay in Ireland.”
He believes the clinical nature of paediatrics appeals to student doctors. “You have to work out what’s wrong with the child from observation. It’s not as much about tests, as it is with an adult; tests are painful and difficult to do, so you have to go a lot on your clinical skills.”
As for himself, it’s the opportunity to be working with long-term survivors of medical care that he relishes. With a sick, premature baby, there is the satisfaction of setting them up for a lifetime of maybe 80 or 90 years.
He has always found writing up individual cases very stimulating. His father, who used to do a lot of writing advised him that “writing gives an existence to what you do, gives us some meaning.” In his “spare” time, Murphy has, since 1989, edited the Irish Medical Journal, now published only online, and plays golf. He’s married to a doctor and two of their three adult children have followed in their footsteps, while the third is a solicitor.
It’s said that the age of viability for preterm babies is lowered by a week for about every decade of improved neonatal care. Last December, the RCPI recommended 23 weeks’ gestation as the threshold for viability, the previous bar of 24 weeks having been set in 2006. “Anecdotally, we were beginning to resuscitate 23 weeks’ gestation babies so we decided we would lower the limit in recognition of that.”
How much lower does Murphy think it can go? “We haven’t had survivors of 22 weeks, we don’t see that,” he says, while acknowledging that they do in Japan. He reckons it would need another fairly significant innovation before the threshold drops again.
Active management of extremely premature babies is ethically complex and when a baby is born at 23 weeks, important conversations have to be held with the parents about the merits and demerits of intensive care. “You may institute intensive care and then a few days into the intensive care sequence, you find the baby has a major complication, say a brain bleed, and then you reconsider.” There are frank discussions when complications arise, in some “very challenging human scenarios.” Maybe a couple has been through three or four rounds of IVF before achieving a pregnancy that has resulted in an extremely premature delivery.
Constant interaction with colleagues and a sense of camaraderie is what he finds “destressing” in the job. “With our team, the junior hospital doctors are teaching every morning and we all go for tea. You’re meeting every day and discussing things every morning, that takes the stress out of situations because you discuss and unburden your concerns and get the best opinions on how to do X, Y and Z. The hospital has that tradition of being a good place to work.”
Will he ever retire?
“I will eventually,” he smiles.
But he’s certainly showing no sign of it yet.

Westlife perform Starlight in the Ballroom ✨ BBC Strictly 2021
Oct 17, 2021 BBC Strictly Come Dancing

PREEMIE FAMILY PARTNERS
#3 James Boardman: Growing up following premature birth
July 24, 2018
Professor James Boardman, Professor of Neonatal Medicine at the University of Edinburgh, describes his work on the brain development of premature babies, as part of Their world Edinburgh Birth cohort (http://www.tebc.ed.ac.uk/). This presentation was part of a public engagement event called ‘Celebrating your contribution to Scottish Cohort Studies’, which took place in The Assembly Hall on the Mound, on 10th June 2018.

Pregnant Women Urged to Get COVID-19 Vaccine
Michelle Winokur, DrPH, and the AfPA Governmental Affairs Team, Alliance for Patient Access (AfPA)

Public health officials are urging pregnant and breastfeeding moms to get the COVID-19 vaccine – and soon. A federal health advisory from the Centers for Disease Control and Prevention follows the release of new data showing a 70% increased risk of death from COVID-19 during pregnancy. Unvaccinated pregnant women also have a higher risk of early delivery or stillbirth.
Pregnancy and Vaccine Safety
As part of their campaign to encourage pregnant women to get inoculated, Federal health officials are highlighting the safety and efficacy of the vaccine. As the health advisory notes, the vaccine does not increase the risk of miscarriage or birth defects or affect fertility. The COVID-19 vaccine is recommended for pregnant women, recently pregnant, breastfeeding, or trying to get pregnant. Professional medical organizations have endorsed these recommendations, including the American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine. COVID-19 Among Pregnant Women Despite the benefits to mothers and their unborn babies, only 31% of pregnant women are vaccinated against COVID-19. Being unvaccinated leaves expectant moms vulnerable to contracting COVID-19, while pregnancy makes them more likely to experience severe symptoms and require intensive-level care.
As part of their campaign to encourage pregnant women to get inoculated, Federal health officials are highlighting the safety and efficacy of the vaccine. As the health advisory notes, the vaccine does not increase the risk of miscarriage or birth defects or affect fertility. The COVID-19 vaccine is recommended for pregnant women, recently pregnant, breastfeeding, or trying to get pregnant. Professional medical organizations have endorsed these recommendations, including the American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine.
COVID-19 Among Pregnant Women
Despite the benefits to mothers and their unborn babies, only 31% of pregnant women are vaccinated against COVID-19. Being unvaccinated leaves expectant moms vulnerable to contracting COVID-19, while pregnancy makes them more likely to experience severe symptoms and require intensive-level care.
Thus far, approximately 97% of pregnant women hospitalized with COVID-19 were unvaccinated. Moreover, in August, 22 pregnant women died of COVID-19, making it the single highest month for COVID-related pregnancy deaths since the pandemic began. In contrast, getting vaccinated protects both expectant moms and her baby. Getting vaccinated is the single most effective way to prevent serious illnesses, death, and adverse pregnancy outcomes from the coronavirus.
A Precaution Not to be Overlooked
Women who are planning to get pregnant take many steps to prepare. Likewise, expectant moms pay extra attention to their health and safety for the sake of their babies. Getting vaccinated against COVID-19 is one precaution they should not overlook. The sooner, the better, say the experts.
References: https://emergency.cdc.gov/han/2021/han00453.asphttp://neonatologytoday.net/newsletters/nt-nov21.pdf

Pregnancy and infancy loss – Grandparents grief
Nov 9, 2020 Pascale Vermont
Pascale Vermont, PhD – Grief counselor Author of Surviving the Unimaginable -Grandparents’ grief after a baby loss Most grandparents feel devastated and very lonely when their son or daughter loses a baby during pregnancy or infancy. In this video I share some suggestions other grandparents have found to be very helpful.

INNOVATIONS

What Happened With Preterm Birth During the Pandemic?
Some mothers — and their babies — may have fared better than others
by Amanda D’Ambrosio, Enterprise & Investigative Writer, MedPage Today – April 8, 2021
While pregnant women have been warned about their potential for more severe COVID-19 illness, a few early reports have suggested one positive finding for this population — that pandemic lockdown restrictions may have coincided with a decrease in preterm births.
Early studies have observed a decline in preterm birth rates during the lockdowns, highlighting a potential “silver lining” of the pandemic. But while these findings are encouraging, experts say there is still not enough data to know whether the reduction in preterm births was widespread, or what factors may have caused this outcome to drop in the first place.
“The jury is out, in terms of what’s the overall impact [of the pandemic] on preterm birth,” said Rahul Gupta, MD, MPH, chief medical and health officer at March of Dimes. While early data may provide some insight into lifestyle changes such as working from home and remote access to healthcare, Gupta said more information is needed before drawing conclusions about preterm birth reductions — and which populations were most affected.
Globally, preterm birth is the leading cause of death in children under 5 years old, according to the WHO. In the U.S., the preterm birth rate has been on a consistent upward trajectory, with 2019 being the fifth straight year in a row that the rate increased. Between 2018 and 2019, the preterm birth rate rose by 2%, according to the CDC.
Clinicians from Denmark and Ireland first began to notice a decline in preterm births last spring — specifically, those that were earliest and most critical. A preprint study from Denmark, which included more than 31,000 infants born between 2015 and 2020, showed around a 90% decrease in extremely preterm births (those born before 32 weeks’ gestation) during the lockdown period. In Ireland, another study published in BMJ Global Health observed a 73% reduction in extremely low birthweight deliveries, from January to April of last year.
Other studies have found that rates decrease for specific populations. A recent systematic review and meta-analysis in The Lancet Global Health found that while the overall preterm birth rate was not significantly different before and during the pandemic, the rate in high-income countries declined by 9%. Spontaneous preterm births in high-income countries saw an even greater reduction, falling by almost 20%.
“Interestingly, there are happy numbers mainly from high-income countries,” said the study’s lead author, Asma Khalil, MD, of St. George’s University Hospitals NHS Foundation Trust in London.
Some reports from the U.S. also reflected a decline, albeit a smaller one. Last April, Stephen Patrick, MD, MPH, of Vanderbilt University, wrote on Twitter that he noticed a lower number of infants in the neonatal intensive care unit (NICU) at his institution.
Last month, Patrick and colleagues published a study in JAMA Pediatrics showing the relationship between preterm birth and stay-at-home orders in Tennessee. Patrick’s team found that the risk of preterm birth fell nearly 15% during the lockdown period, after controlling for maternal age, race, education level, hypertension, and diabetes.
Naima Joseph, MD, MPH, a maternal-fetal medicine fellow at Emory University School of Medicine, said it could be that the decline is related to the environmental and lifestyle changes that occurred during the early months of the pandemic.
Alison Gemmill, PhD, of Johns Hopkins University, said that a number of changes during lockdown may have been associated with drops in the preterm birth rate. When most cars were off the roads, there may have been a decline in the number of preterm births associated with air pollution. Additionally, as pregnant people shifted to remote work and found themselves at home and off their feet, Gemmill said there may have been a decline in physical stress.
Another hypothesis, Gemmill added, is that the decrease in preterm births may have occurred simultaneously with an increase in stillbirths. Some reports have shown an increase in stillbirths during the pandemic (including Khalil’s analysis), but U.S. data has yet to confirm this increase.
Gemmill and colleagues published a study last week (which has not yet been peer-reviewed) showing that the preterm birth rate in the U.S. was one of several birth outcomes that was lower than expected in March and April of last year. But the group also observed that the rate dipped significantly again in November and December — coinciding with the months when infection rates climbed.
“Something is definitely going on,” Gemmill said in an interview. She added that the rates her group observed are crude, and do not describe how different demographic groups in the U.S. were affected. However, she said her research is “detecting a really important signal that doesn’t occur in birth outcomes research.”
Not all U.S. data confirm this pattern. A JAMA study of nearly 9,000 infants at the University of Pennsylvania showed that mothers in 2020 were at the same risk of preterm birth than they had been in years prior.
Gupta, of March of Dimes, stated that the U.S. is not a homogenous society, and preterm birth rates will look different across different populations. Black parents, for example, have a 50% higher chance of having a premature infant than white or Hispanic parents. And while preterm births may have coincided with remote work, that would not apply for the essential workers who continued their employment throughout lockdowns.
Regarding preterm birth outcomes during the pandemic, Gupta said that once scientists break down data by demographics, social determinants of health, and medical comorbidities, he expects there will be a “variety of outcomes.” There is no real-time, national birth surveillance data in the U.S. — so it will take time to understand these outcomes fully.
As far as the theories about which factors may have impacted preterm birth, Joseph said that “mostly, these data have led to more hypothesis generation than anything else more conclusive.”
Gupta agreed, adding that there is more research to be done about both the impacts of COVID-19 infection, as well as the indirect effects of the pandemic.
“I think we really have to better understand what factors during COVID — including lockdowns, unemployment, social interactions, mental health, adherence to medications, job loss — all played a role,” he said. “I think we should not take any of these one factors for granted.”
Source: https://www.medpagetoday.com/special-reports/exclusives/92000

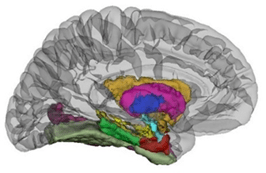
INFANT Led European Network to Advance Development of Algorithms that Detect Brain Injuries in Infants
By Alan Drumm|October 27th, 2021
Working alongside a team of scientists, clinicians and technical experts from 14 different European countries, Dr John O’Toole aims to build capacity and strengthen cooperation among international research groups, with the goal of developing algorithms that will minimise the risk of babies developing catastrophic life-long neonatal brain injuries.
Insufficient oxygen around the time of birth can cause brain injury. For babies born prematurely, the heart and lungs may struggle to adapt to the new environment which can lead to brain injury too. Brain monitoring of a tiny infant in an intensive care unit is challenging.
It can be difficult and slow to interpret the complex brain-wave patterns. AI systems are a perfect fit to this problem, as they can be designed to automatically recognise signs of brain injury.
Funded by the European Cooperation in Science and Technology, the researchers involved in the AI-4-NICU project plan to build on existing cot-side technologies, such as devices that measure brain waves, by including AI algorithms to detect markers of brain injury.
This, Dr O’Toole anticipates, will lead to the development of decision-support tools that will help clinicians in neonatal intensive care units to quickly identify potential brain injuries that can result in death, cerebral palsy, or delayed development.
Reading and interpreting the brain-wave signals is a notoriously difficult task which requires highly specialised expertise. AI systems can be designed to mimic the human expert, by shifting through enormous amounts of data to automatically find signs of brain injury.
These AI systems, unlike the human expert, can then run around the clock for all at-risk infants to provide a continuous assessment of brain health.
To develop the device, Dr O’Toole and his team will first develop the tools necessary to acquire, pool, share, and manage neuro-physiological data sets.
They will then create a framework to develop, test, and compare algorithms that they hope will act as decision-support tools in neonatal intensive care units.

In prematurity, twins can have developmental advantages over singletons
November 2, 2021 Marian Freedman, Jon Matthew Farber, MD

A recent study indicates that when born prematurely, twins may have some gains over singleton babies.
A milestone-related assessment of early psychomotor development of preterm (PT) twins compared with PT singletons found that twins born between 32 and 33 weeks’ gestational age (GA) have an early neuro- development advantage over their singleton peers. Italian investigators conducted developmental assessments in 73 PT twins and 207 PT singletons throughout the first 18 months of life. Assessments, using standardized tests and parental observation, included primary gross motor milestones, beginning of babbling, early visual fixation, and being able to follow a moving object. Investigators divided participants into 3 groups according to GA: 17 born at less than 31 weeks (group 1), 30 born between 32 and 33 weeks (group 2), and 26 born between 34 and 36 weeks (group 3). Twins in group 1 not only spoke their first single word significantly earlier than singletons in the group did but also demonstrated persistent superior language skill achievement at long-term follow-up together with better oculomanual abilities. Compared with singletons, group 2 twins also spoke their first single words at a younger age and achieved standing, walking, and pointing earlier. No significant differences emerged between group 3 twins and singletons except that twins demonstrated worse personal and social skills than singletons at long-term follow-up. Overall, investigators concluded that the differences in twins compared with singletons in the 3 groups were independently related to their gemellarity (“twinness”).
Thoughts from Dr. Farber
This is an interesting finding. An earlier study showed that firstborn twins above 28 weeks’ gestation were less likely to have respiratory distress syndrome than singletons. I wonder whether better lungs account for some of the difference. Unfortunately, many of the children, twins or not, had developmental delays at 25 to 36 months of corrected age.

Child Development: How to Improve Educational Outcomes of Children Born Preterm
Education and Training Foundation

Posted on January 4th, 2021 – In a guest blog, Dr Joanna Goodman, an independent education consultant and expert panel member for developing T Levels, writes why the new Education and Childcare T Level must signpost to evidence-based educational resources for children born prematurely.
In the UK, in an average sized classroom, two to three children are likely to have been born preterm (before 37 weeks of pregnancy). Whilst the numbers of children born preterm are rising, there has been very little training available to education professionals – teachers, educational psychologists, nursery nurses or teaching assistants– with regard to the potential learning difficulties that these children can encounter in early years settings or schools.
It is, therefore, particularly important that the new ‘gold standard’ T Level qualification in Education and Childcare signposts to the evidence-based educational resources for children born prematurely: PRISM resources. These free resources, aimed at education professionals, not only raise the awareness of the impact of prematurity on learning, but also highlight a range of strategies that can be used to improve the educational experiences of these children, ultimately leading to improving their life chances.
As part of the panel of experts who worked on developing the curriculum for the Education and Childcare T Level, I am now keen to raise awareness and understanding of the potential needs of these children – to bridge the gap between healthcare and education. Additionally, learning from my experience developing NICE guidelines for the follow-up of children born preterm and subsequently making a contribution to the development of PRISM resources, I feel that I am well placed to raise awareness among education professionals of the potential risk factors and learning needs of this cohort. Moreover, it is critical that any new quality training for education professionals – for example the T Level Professional Development (TLPD) offer – should include evidence-based information that is relevant to particular workplaces. This is particularly imperative when information applies to 8% of the school population, and when education professionals have received very little training in this area to date.
Research asserts that:
…education professionals receive very little training about the impact of preterm birth on children’s development and learning and have poor knowledge of how to support preterm-born children in the classroom. In a recent national survey, only 16% of teachers had received any training about preterm birth and over 90% expressed the need for training. As teachers have primary responsibility for supporting the learning and development of preterm born children in the long term, this represents a significant public health concern. (Johnson, S. et al., 2019).
To address this gap in knowledge and training, it is crucial that any new training or qualification for professionals working with children in education or early years settings, includes high quality evidence-based resources on how to improve the outcomes of children born preterm.
For those undertaking training within the TLPD offer, the Education and Childcare courses will signpost practitioners to the PRISM resources, which serve to raise awareness and understanding of the different learning techniques when teaching preterm children.
Furthermore, as “preterm birth places children at an increased risk for a range of developmental problems and disorders later in life” and “this disadvantage persists throughout the lifespan with fewer preterm-born adults having completed high school and undertaken higher education” (Johnson, S. et al., 2019), this issue is not only of concern to professionals working in primary school or early years settings. Clearly, awareness of prematurity and potential learning difficulties is applicable to all educational settings, so appropriate teaching and learning strategies can be used for improved outcomes.
As an experienced educator and an expert on learning, I cannot emphasise enough how fundamental it is for all staff working with children to have the right level of knowledge with regard to child development, including the impact of birth problems on subsequent cognitive, sensory or physical development. Free access PRISM e-resources provide valuable information for adults working with children on risk factors for child development and expected milestones. Despite significant improvements in neonatal care, to date there is no evidence of improved long-term outcomes for these young people. The experts highlight that:
The continued increase in preterm birth rates for extremely preterm babies [born <27 weeks gestation] means that there are increasing numbers of preterm survivors entering societies year on year. This results in greater demands being placed on education systems and their professionals to identify difficulties and provide support for these children in the long term.(Johnson, S. et al., 2019).
According to evidence, these particular areas may require additional support:
- difficulties with mathematics
- inattention
- working memory difficulties
- slow processing speed
- poor hand-eye co-ordination
- social and emotional problems
- sensory impairments
- poor fine and gross motor skills.
However, as these children’s development is different to children born full term, it is important to understand that preterm children have different developmental mechanisms behind their difficulties than term-born children. For example, inattention can be linked to poor working memory or visual impairment, rather than attention-deficit-hyperactivity disorder, as known in term-born children. It is also worth noting that the attainment of these children is often lower by comparison with peers and some may never attain at the same level as their peers born at term.
For these reasons, and to minimise external interventions, it is important for any professionals working with children to engage with these interactive free e-learning resources, which are the only kind of resources available worldwide. An early evaluation of these resources indicates they have “substantially improved teachers’ knowledge of preterm birth and their confidence in supporting preterm children in the classroom.” (Johnson, S. et al., 2019). This is why the access to these resources provides another important dimension to the study of child development as part of T Level training in Education and Childcare, through the TLPD offer.

HEALTH CARE PARTNERS

The U.S. needs more nurses, but nursing schools don’t have enough slots
October 25, 20215:00 AM ET YUKI NOGUCHI HEALTH INC
Struggle is nothing new to Foxx Whitford.
He grew up desperately poor in Fairfield, Calif., losing a beloved brother to epilepsy and getting evicted from his home as a child. As a teenager, he joined the Marines to help put himself through college and he completed a harrowing tour in Afghanistan. All of that hardship, he says, prepared him for one of his biggest life challenges: getting into and through nursing school during a pandemic.
“Every time things get hard, I always think about all those losses and hard times,” says Whitford, a nursing student at California State University, East Bay.
And everything about his nurse training has been hard. Whitford, a C-average student in high school, says he spent sleepless nights in community college, studying and teaching himself to learn. After nearly failing an anatomy course, he eventually made the dean’s list and won student-athlete awards. Still, when he tried to transfer to a four-year bachelor of science in nursing program, he lost out. There were some 800 others applying for 64 slots.
He waited a year to reapply and finally got in. Then the pandemic hit — making it even more difficult to get the clinical experience he needs to graduate.
Across the country, hospitals desperate for nurses — especially in acute care —are trying to address intense burnout among health care workers and accelerated nurse retirements by hiring new graduates. They’re offering jobs to students even before they graduate, and in many cases offering bonuses and loan repayment as financial incentives. And the interest is there; enrollments and applications in baccalaureate and advanced nursing degree programs increased last year. Leaders in nursing say the trends — which predate the pandemic — are the same for certificate programs in licensed practical nursing, licensed vocational nursing and certified nursing assistants programs.
Yet — paradoxically — becoming a nurse has become more difficult, narrowing the pipeline for new nurses coming through the system.
A lack of instructors is part of the problem
One of the biggest bottlenecks in the system is long-standing: There are not enough people who teach nursing. Educators in the field are required to have advanced degrees yet typically earn about half that of a nurse working the floor of a hospital.
Health workers know what good care is. Pandemic burnout is getting in the way
The pandemic worsened those financial strains, forcing many educators to look for more lucrative work, says Sharon Goldfarb, who has advanced degrees in nursing care, has worked as an RN and family nurse practitioner and teaches nursing at several schools near San Francisco. Her spouse lost his job during the pandemic and that is one of the most common reasons educators are leaving, she says. She surveyed 91 community colleges in California and found nursing faculty declined 30% since the pandemic began.
“To lose an additional 30% has been devastating,” she says. “There is not a school I know of that isn’t desperately looking for nursing faculty.”
That desperation is compounded by an aging demographic. With so many in their late 50s and 60s, the country’s nursing faculty is continuing to decline, to about two-thirds what it was in 2015.
Taken together, those factors are severely limiting the number of students that schools can accept, and in some cases it disrupts classes themselves.
“Some schools went on hiatus; some schools reduced their enrollment, so they took even fewer students; some schools … scrambled so much, they actually have to extend semesters,” Goldfarb says.
The pandemic curtailed training programs
In addition, since the beginning of the pandemic, nursing students have had a harder time getting the clinical or hands-on training required to graduate, because hospitals curtailed their training programs to control the risk of infection.
“Faculties and schools have found ways to innovate, to educate students by the use of the internet, distance learning, and simulation labs,” says Peter Buerhaus, a professor and health economist at Montana State University’s College of Nursing who studies the nursing workforce. Those innovations have helped mitigate the impact of the pandemic on education, he says, but schools aren’t like factories that can ramp up their production.
The nursing shortage, he says, was more acute in the 1990s, when hospitals drastically cut back on staff to cut costs. But with the retirement of baby boomers, the influx of new nurses needs to keep up.
Last year, enrollment in baccalaureate and higher-level nursing degree programs increased, but colleges and universities (not including community college nursing programs) still turned away more than 80,000 qualified applicants due to shortages of faculty, clinical sites and other resources, according to the American Association of Colleges of Nursing.
How one applicant persevered
Whitford, the nursing student aiming to become an RN, is getting even more specialized training as an ER nurse. He says many people ask him how he has persevered through the gantlet of nursing school. “Everything I have, I’ve always had to work extremely hard for,” he tells them.
At age 10, shortly after his brother — whom he describes as his “best friend” and idol — died of epilepsy, Whitford started working at a bowling alley to supplement his father’s truck-driving income. “We had to struggle a lot when I was growing up, in terms of getting food on the table.”
His early childhood tested him, he says, and ultimately deepened his resolve.
“Pursuing nursing,” he says, “was my ticket to doing everything that I wanted.” And that meant getting out of poverty and into meaningful work he loved.
His childhood experiences also made him feel comfortable in chaos. So when the pandemic hit, Whitford became even more eager to join the front lines: “I like being in tents outside in [expletive] conditions — terrible stuff that people don’t want to do,” he says. “I’m not always the strongest in those conditions, but I like working through them, so that way I can learn how to be strong in those situations. Because I feel like, a lot of times when things go wrong, people would look to me for answers.”
For many others, though, the path to nursing is too steep.
Financial strain often gets in the way
Over the past 15 years, Nathan Ballenger, 46, has tried three separate times to enroll in nursing school. He’s harbored lifelong dreams of a career in medicine, which the Colorado native considers heroic work. During the pandemic, he even got certified as an emergency medical technician, hoping that would give him a foot in the door and an advantage over his fellow nursing school applicants.
But the cost and difficulties of a nursing degree program and training — and the pay cut he would have had to take compared to what he earns his current salesman’s job — meant he simply couldn’t afford to go in that direction.
“It’s hard for me to say that I see a path toward that,” he says, “regardless of the fact that I hold it in my mind and in my heart as something that I sure wish I could have done in this lifetime.”
Hospitals recognize the need to lower some of the barriers to becoming a nurse, while maintaining high standards of education, training and patient care.
Hospitals are not only offering full scholarships and loan repayment to recruit registered nurses these days, many are also offering to put new graduates through intensive training to acquire special skills, says Robin Begley, CEO of the American Organization for Nursing Leadership and chief nursing officer and senior vice president of workforce for the American Hospital Association. Many hospitals are also partnering with nursing schools to do what they can to widen the pipeline by allowing hospital nurses to take time off to teach, for example.
“We really have to put a real emphasis on the pipeline and making sure that everybody who wants to become a nurse has the opportunity to be able to secure a position in a nursing program,” Begley says.

Losing Touch
Perspective -Ken Wu, M.B., B.S.

We called it the “cold light.” It looked like a small blue button with a power cord attached to the end of it. At its center was a single round eye that emitted a light, crimson in color and piercing in power. In the neonatal intensive care unit (NICU), we used the cold light to find our patients’ veins, but in the baby in front of us, we found nothing.
My attending physician switched off the cold light. I looked at my patient, pondering this tiny embodiment of life writhing inside an incubator. She had been born at 24 weeks of gestation, weighing just over one pound. She was so small that I could see all of her in a single gaze. Her body was smaller than my hand, her hand smaller than my finger. I had looked after her for 3 weeks, but I’d never seen her face — it was always obscured by equipment that was helping her breathe. Yet her vigor far exceeded her size; she had already survived two different infections and now needed a blood transfusion. To give her the transfusion, we needed access to her veins.
We switched the light on again and placed it under one of her arms for another look. The anemic limb transformed into a translucent pearl surrounded by a red halo. Inside the pearl were black lines, some of which were veins. We moved the light up and down the limb, tracking each black line to see if it might be a vein long and straight enough to accommodate an intravenous cannula.
For a moment, I looked at my own arm, its veins bulging from the heat of the incubator. Fortunate to have veins that can easily be seen and felt, I often use my own limbs as an anatomy reference when inserting an intravenous line. I sometimes feel guilty for relying on this guide, especially when I notice a parent’s envious gaze at my arm as I make my nth attempt to find a vein in their child. “I am sorry this is difficult. I hated needles as a child,” I always say, adding, “I still hate getting my flu vaccine every year.”
Although in the NICU most procedures are not done under the watchful eye of worried parents, I still felt the guilt and shared the parents’ pain. My patient’s limbs were dotted with puncture marks and bruises. Practically, I used them as a record of previous attempts and a road map for potential entry points. Viscerally, I could not help but feel the twitch of a limb withdrawing from pain every time a needle went through the baby’s skin. “I’m sorry, baby,” I murmured. But who I was talking to — the still-nameless baby, who lacked the awareness to accept apologies? The parents, absent in body but present in mind?
Or was I really apologizing to myself for physicians’ facile recourse to medical necessity as justification for inflicting physical pain? From the moment this baby was born, we had intubated her, fed her using an orogastric tube, and repeatedly inserted intravenous lines to give her medications. Although I knew these invasions of her organs were necessary in order to replace the lifeline from which she’d been prematurely separated, their importance did not diminish their noxiousness. In my mind, I could still see the imprint of a laryngoscope blade in the baby’s neck as she was intubated and feel the silent gags of a voiceless newborn as the orogastric tube passed through her mouth. The knowledge that these procedures were lifesaving dampened but did not eliminate my empathetic discomfort.
After every blood test I’d had as a child, I’d run into the arms of my parents. But here in the NICU, there were no comforting hugs, no whispers of “It’s OK, it’s all over,” no rewards of lollipops or bravery stickers. When we finished inserting the cannula, I cleaned the area, checked the insertion site for bleeding and leaks, and closed the doors of the incubator. The sterility was as necessary as it was jarring. I glanced back as I walked away and saw one tiny arm outstretched, while the other was weighed down by the cannula. Although we’d obtained the access we needed, the baby seemed to be reaching out for the parental touch she missed.
But the only people she could touch worked in the NICU, living and thriving in an intimidating environment defined by a hawkish hygiene policy, the complex fragility of the newborns, and the minutiae of the care we provided. When new parents first enter the NICU, I can always see the subdued heartache reflected in their crestfallen faces. For them, the NICU is a place of hope, of patience, but also of submission. For the first weeks or months of their child’s life, it is up to the NICU team to feed and diaper their baby. Procedures are carried out, investigations done, and treatments started with emergency consent only, in the absence of parents. The complexities of neonatal medicine, the difficulties of neonatal procedures, and the absurdities of minute size all overwhelm parents who are newly flooded with the emotions of parenthood and protection. The parents’ role is reduced to receiving daily updates from a team that has usurped their position as the protectors and nurturers of their baby. Every time I see parents looking at their baby in an incubator, I imagine them struggling to reconcile the joyful anticipation of pregnancy with the frustrating reality of a baby whose skin they cannot touch, whose cries they cannot hear, but whose pain they always feel.
I am conscious that in providing surrogate incubators for babies who were born too soon, we in the NICU place painful restrictions on the most basic of human relationships, the one between parents and their child. Although the team always tries to involve parents in as much of the care and decisions as possible, part of the NICU experience requires parents and baby to lose touch with one another. The touch that is lost by parents is gained by physicians, and we know that our touch can hurt as well as heal.
Taking on some of parents’ responsibilities also means adopting their instinctive burdens. Though I fully grasp the medical necessity of our interventions, I sometimes find carrying them out and justifying them as difficult as parental bystanders find caring for their newborn from afar, especially when it involves so much discomfort for someone so small. Not only am I the one doing the procedures, I am also the one who can and must touch, viscerally connected and thus feeling the immediate effects of causing pain.
As I prepare to insert an intravenous cannula in my next patient, his mother stands up and leaves. “I can’t watch,” she says. “It’s just too much.” Sometimes I wish the parents could stay, or the baby could understand me when I apologize before inflicting more suffering in the name of healing. I stay, the baby’s foot in one hand, cannula in the other, bracing myself for the reflexive kick as the needle pierces the skin.
Source:https://www.nejm.org/doi/full/10.1056/NEJMp2033590

Implementation and Outcomes of a Telehealth Neonatology Program in a Single Healthcare System
Front. Pediatr., 23 April 2021 | https://doi.org/10.3389/fped.2021.648536Lory J. Maddox, Jordan Albritton, Janice Morse, Gwen Latendresse, Paula Meek and Stephen Minton
Background: Intermountain Healthcare, an early adopter and champion for newborn video-assisted resuscitation (VAR), identified a reduction in facility-level transfers and an estimated savings of $1. 2 million in potentially avoided transfers in a 2018 study. This study was conducted to increase understanding of VAR at the individual, newborn level.
Study Aim: To compare transfers to a newborn intensive care unit (NICU), length of stay (LOS), and days of life on oxygen between newborns managed by neonatal VAR and those receiving standard care (SC).
Methods: This retrospective, nonequivalent group study includes infants born in an Intermountain hospital between 2013 and 2017, 34 weeks gestation or greater, and requiring oxygen support in the first 15 minutes of life. Data came from billing and clinical records from Intermountain’s enterprise data warehouse and chart reviews. We used logistic regression to estimate neonatal VAR’s impact on transfers. Negative binomial regression estimated the impact on LOS and days of life on supplemental oxygen.
Results: The VAR intervention was used in 46.2 percent of post-implementation cases and is associated with (1) a 12 percentage points reduction in the transfer rate, p = 0.02, (2) a reduction in spoke hospital (SH) LOS of 8.33 h (p < 0.01) for all transfers; (3) a reduction in SH LOS of 2.21 h (p < 0.01) for newborns transferred within 24 h; (4) a reduction in SH LOS of 17.85 h (p = 0.06) among non-transferred newborns; (5) a reduction in days of life on supplemental oxygen of 1.4 days (p = 0.08) among all transferred newborns, and (6) a reduction in days of life on supplemental oxygen of 0.41 days (p = 0.04) among non-transferred newborns.
Conclusion: This study provides evidence that neonatal VAR improves care quality and increases local hospitals’ capabilities to keep patients close to home. There is an ongoing demand for support to rural and community hospitals for urgent newborn resuscitations, and complex, mandatory NICU transfers. Efforts may be necessary to encourage neonatal VAR since the intervention was only used in 46.2 percent of this study’s potential cases. Additional work is needed to understand the short- and long-term impacts of Neonatal VAR on health outcomes.
Full Article: https://www.frontiersin.org/articles/10.3389/fped.2021.648536/full

WHY HEALTH-CARE WORKERS ARE QUITTING IN DROVES
About one in five health-care workers has left their job since the pandemic started. This is their story—and the story of those left behind.

By Ed Yong NOVEMBER 16, 2021
The moment that broke Cassie Alexander came nine months into the pandemic. As an intensive-care-unit nurse of 14 years, Alexander had seen plenty of “Hellraiser stuff,” she told me. But when COVID-19 hit her Bay Area hospital, she witnessed “death on a scale I had never seen before.”
Last December, at the height of the winter surge, she cared for a patient who had caught the coronavirus after being pressured into a Thanksgiving dinner. Their lungs were so ruined that only a hand-pumped ventilation bag could supply enough oxygen. Alexander squeezed the bag every two seconds for 40 minutes straight to give the family time to say goodbye. Her hands cramped and blistered as the family screamed and prayed. When one of them said that a miracle might happen, Alexander found herself thinking, I am the miracle. I’m the only person keeping your loved one alive. (Cassie Alexander is a pseudonym that she has used when writing a book about these experiences. I agreed to use that pseudonym here.)
The senselessness of the death, and her guilt over her own resentment, messed her up. Weeks later, when the same family called to ask if the staff had really done everything they could, “it was like being punched in the gut,” she told me. She had given everything—to that patient, and to the stream of others who had died in the same room. She felt like a stranger to herself, a commodity to her hospital, and an outsider to her own relatives, who downplayed the pandemic despite everything she told them. In April, she texted her friends: “Nothing like feeling strongly suicidal at a job where you’re supposed to be keeping people alive.” Shortly after, she was diagnosed with post-traumatic stress disorder, and she left her job.
Since COVID-19 first pummeled the U.S., Americans have been told to flatten the curve lest hospitals be overwhelmed. But hospitals have been overwhelmed. The nation has avoided the most apocalyptic scenarios, such as ventilators running out by the thousands, but it’s still sleepwalked into repeated surges that have overrun the capacity of many hospitals, killed more than 762,000 people, and traumatized countless health-care workers. “It’s like it takes a piece of you every time you walk in,” says Ashley Harlow, a Virginia-based nurse practitioner who left her ICU after watching her grandmother Nellie die there in December. She and others have gotten through the surges on adrenaline and camaraderie, only to realize, once the ICUs are empty, that so too are they.
Some health-care workers have lost their jobs during the pandemic, while others have been forced to leave because they’ve contracted long COVID and can no longer work. But many choose to leave, including “people whom I thought would nurse patients until the day they died,” Amanda Bettencourt, the president-elect of the American Association of Critical-Care Nurses, told me. The U.S. Bureau of Labor Statistics estimates that the health-care sector has lost nearly half a million workers since February 2020. Morning Consult, a survey research company, says that 18 percent of health-care workers have quit since the pandemic began, while 12 percent have been laid off.
Stories about these departures have been trickling out, but they might portend a bigger exodus. Morning Consult, in the same survey, found that 31 percent of the remaining health-care workers have considered leaving their employer, while the American Association of Critical-Care Nurses found that 66 percent of acute and critical-care nurses have thought about quitting nursing entirely.
“We’ve never seen numbers like that before,” Bettencourt told me. Normally, she said, only 20 percent would even consider leaving their institution, let alone the entire profession. Esther Choo, an emergency physician at Oregon Health and Science University, told me that she now cringes when a colleague approaches her at the end of a shift, because she fears that they’ll quietly announce their resignation too. Vineet Arora, who is dean for medical education at University of Chicago Medicine, says that “in meetings with other health-care leaders, when we go around the room, everyone says, ‘We’re struggling to retain our workforce.’ Nobody says, ‘We’re fine.’”
When national COVID hospitalizations fell in September and October, it was possible to hope that the health-care system had already endured the worst of the pandemic. But that decline is now starting to plateau, and in 17 states hospitalizations are rising. And even if the country dodges another surge over the winter, the health-care system is hemorrhaging from the untreated wounds of the past two years. “In my experience, physicians are some of the most resilient people out there,” Sheetal Rao, a primary-care physician who left her job last October, told me. “When this group of people starts leaving en masse, something is very wrong.”
Health-care workers, under any circumstances, live in the thick of death, stress, and trauma. “You go in knowing those are the things you’ll see,” Cassandra Werry, an ICU nurse currently working in Idaho, told me. “Not everyone pulls through, but at the end of the day, the point is to get people better. You strive for those wins.” COVID-19 has upset that balance, confronting even experienced people with the worst conditions they have ever faced and turning difficult jobs into unbearable ones.
In the spring of 2020, “I’d walk past an ice truck of dead bodies, and pictures on the wall of cleaning staff and nurses who’d died, into a room with more dead bodies,” Lindsay Fox, a former emergency-medicine doctor from Newark, New Jersey, told me. At the same time, Artec Durham, an ICU nurse from Flagstaff, Arizona, was watching his hospital fill with patients from the Navajo Nation. “Nearly every one of them died, and there was nothing we could do,” he said. “We ran out of body bags.”
Most drugs for COVID-19 are either useless, incrementally beneficial, or—as with the new, promising antivirals—mostly effective in the disease’s early stages. And because people who are hospitalized with COVID-19 tend to be much sicker than average patients, they are also very hard to save—especially when hospitals overflow. Many health-care workers imagined that such traumas were behind them once the vaccines arrived. But plateauing vaccination rates, premature lifts on masking, and the ascendant Delta variant undid those hopes. This summer, many hospitals clogged up again. As patients waited to be admitted into ICUs, they filled emergency rooms, and then waiting rooms and hallways. That unrealized promise of “some sort of normalcy has made the feelings of exhaustion and frustration worse,” Bettencourt told me.
Health-care workers want to help their patients, and their inability to do so properly is hollowing them out. “Especially now, with Delta, not many people get better and go home,” Werry told me. People have asked her if she would have gone to nursing school had she known the circumstances she would encounter, and for her, “it’s a resounding no,” she said. (Werry quit her job in an Arizona hospital last December and plans on leaving medicine once she pays off her student debts.)
COVID patients are also becoming harder to deal with. Most now are unvaccinated, and while some didn’t have a choice in the matter, those who did are often belligerent and vocal. Even after they’re hospitalized, some resist basic medical procedures like proning or oxygenation, thinking themselves to be fighters, only to become delirious, anxious, and impulsive when their lungs struggle for oxygen. Others have assaulted nurses, thrown trash around their rooms, and yelled for hydroxychloroquine or ivermectin, neither of which has any proven benefit for COVID-19. Once, Americans clapped for health-care heroes; now “we’re at war with a virus and its hosts are at war with us,” Werry told me.
Beyond making workdays wretched, these experiences are inflicting deep psychological scars. “We want to be rooting for our patients,” Durham told me, “but anyone I know who’s working in COVID has zero compassion remaining, especially for people who chose not to get the vaccine.” That’s why he has opted to do travel-nursing stints, which are time-limited and more lucrative than staff jobs: “It just isn’t worth it to do the job for less than the most I can get paid,” he said. He’s still providing care, but he finds himself emotionally detached, and unsettled by his own numbness. For a health-care worker, being shaken by a patient’s death comes with the job. Finding yourself unmoved is almost worse.
Many have told me that they’re bone-weary, depressed, irritable, and (unusually for them) unable to hide any of that. Nurses excel at “feeling their feelings in a supply closet or bathroom, and then putting their game face back on and jumping into the ring,” Werry said. But she and others are now constantly on the verge of tears, or prone to snapping at colleagues and patients. Some call this burnout, but Gerard Brogan, the director of nursing practice at National Nurses United, dislikes the term because “it implies a lack of character,” he told me. He prefers moral distress—the anguish of being unable to take the course of action that you know is right.
Health-care workers aren’t quitting because they can’t handle their jobs. They’re quitting because they can’t handle being unable to do their jobs. Even before COVID-19, many of them struggled to bridge the gap between the noble ideals of their profession and the realities of its business. The pandemic simply pushed them past the limits of that compromise.
The United States uses the rod of Asclepius—a snake entwined around a staff—as a symbol of medicine. But the pandemic suggests that the more fitting symbol might be the Ouroboros, a snake devouring its own tail.
Several health-care workers told me that, amid the most grueling working conditions of their careers, their hospitals cut salaries, reduced benefits, and canceled raises; forced staff to work more shifts with longer hours; offered trite wellness tips, such as keeping gratitude journals, while denying paid time off or reduced hours; failed to provide adequate personal protective equipment; and downplayed the severity of their experiences.
The American Hospital Association, which represents hospital administrators, turned down my interview request; instead, it sent me links to a letter that criticized anticompetitive pricing from travel-nursing agencies and to a report showing that staff shortages have cost hospitals $24 billion over the course of the pandemic. But from the perspective of health-care workers, those financial problems look at least partly self-inflicted: Many workers left because they were poorly treated or compensated, forcing hospitals to hire travel nurses at greater cost. Those nurses then stoke resentment among full-time staff who are paid substantially less but are often asked to care for the sickest patients. And in some farcical situations, “hospitals hired their own staff back as travel nurses and paid them higher rates,” Bettencourt said.
Whatever the intentions behind these decisions, they were the final straw for the many health-care workers who told me that they left medicine less because of COVID-19 itself and more because of how their institutions acted. “I’ve been a nurse 45 years and I’ve never seen this level of disaffection between clinicians and their employers,” Brogan told me. The same is true across almost every sector of the U.S. Record-breaking numbers of Americans left their jobs this April—and then again in July and August. This “Great Resignation,” as my colleague Derek Thompson wrote, “is really an expression of optimism that says, We can do better.”
The culture of medicine makes it hard for health-care workers to realize that. Most enter medicine “as a calling,” Vineet Arora told me, which can push them to sacrifice ever more of their time, energy, and self. But that attitude, combined with taboos around complaining or seeking mental-health help, can make them vulnerable to exploitation, blurring the line between service and servitude. Between 35 and 54 percent of American nurses and physicians were already feeling burned out before the pandemic. During it, many have taken stock of their difficult working conditions and inadequate pay and decided that, instead of being resigned, they will simply resign.
Molly Phelps, an emergency doctor of 18 years, considered herself a lifer. Her medical career had cost her time with her family, wrecked her circadian rhythms, and taxed her mental health, but it offered so much meaning that “I was willing to stay and be miserable,” she told me. But after the horrific winter surge, Phelps was shocked that her hospital’s administrators “never acknowledged what we went through,” while many of her patients “seemed to forget their humanity.” Medicine’s personal cost seemed greater than ever, but the fulfillment that had previously tempered it was missing. On July 21, during an uneventful evening spent scrolling through news of the Delta surge, Phelps had a sudden epiphany. “Oh my God, I think I’m done,” she realized. “And I think it’s okay to walk away and be happy.”
America’s medical exodus is especially tragic because of how little it might have taken to stop it. Phelps told me that if her workplace “had thrown a little more of a bone, that would have been enough to keep me miserable for 13 more years.” Some health systems are starting to offer retention bonuses, long-overdue raises, or hazard pay. And the next generation of health-care workers doesn’t seem to be deterred. Applications to medical and nursing schools have risen during the pandemic. “That workforce is apparently seeing the best of us, and maybe their vision and energy is what we need to make us whole again,” Esther Choo told me.
But today’s students will take years to graduate, and the onus is on the current establishment to reshape an environment that won’t immediately break them, Choo said. “We need to say, ‘We got this wrong, and despite that, you’re willing to invest your lives in this career? What an incredible gift. We can’t look at that and change nothing.’”
The health-care workers who have stayed in their jobs now face a “crushing downward spiral,” Choo told me. Each resignation saddles the remaining staff with more work, increasing the odds that they too might quit. They don’t resent their former colleagues, but some feel that medicine’s social contract, wherein health-care workers show up for one another through tragedy, is fraying. Before the pandemic, “I knew exactly who I would be working with in every single role,” Choo said.
“There was a lot of unspoken communication, and my shifts were so smooth.” But with so many people having left, the momentum that comes from trust and familiarity is gone.
Expertise is also hemorrhaging. Many older nurses and doctors have retired early—people who “know that one thing that happened 10 years ago that saved someone’s life in a clutch situation,” Cassie Alexander said. And because of their missing experience, “things are being missed,” Artec Durham added. “The care feels frantic and sloppy even though we’re not overrun with COVID right now.” Future patients may also suffer because the next generation of health-care workers won’t inherit the knowledge and wisdom of their predecessors. “I foresee at least three or four years post-COVID where health-care outcomes are dismal,” Cassandra Werry told me. That problem might be especially stark for rural hospitals, which are struggling more with staff shortages and unvaccinated populations.
This decline in the quality of health care will likely occur as demand increases. Even in the unlikely event that no further COVID-19 infections occur, the past months have left millions with long COVID and other severe, chronic problems. “I’m seeing a lot of younger people with end-stage cardiac or neurological disease—people in their 30s and 40s who look like they’re in their 60s and 70s,” Vineet Arora told me. “I don’t think people understand the disability wave that’s coming.”
Hospitals are also being flooded by people who don’t have COVID but who delayed care for other conditions and are now in terrible shape. “People are coming in with liver failure, renal failure, and heart attacks they sat on for weeks,” Durham told me. “Even if you take COVID out of the equation, the place is a mess with sick patients.” This pattern has persisted throughout the pandemic, trapping health-care workers in a continuous, nearly two-year-long peak of either COVID or catch-up care. “It doesn’t feel great between surges,” Choo told me. “Something always replaces COVID.”
Throughout the pandemic, commentators have looked to COVID-hospitalization numbers as an indicator of the health-care system’s state. But those numbers say nothing about the dwindling workforce, the mounting exhaustion of those left behind, the expertise now missing from hospitals, or the waves of post-COVID or non-COVID patients. Focusing on COVID numbers belies how much harder getting good medical care for anything is now—and how long that trend could potentially continue. Several health-care workers told me that they are now more concerned about their own loved ones being admitted to the hospital. “I’m worried about the future of medicine,” Sheetal Rao said. “And I think we all should be.”
A life outside medicine can be hard for people who have built their identities within it. For some, it’s like returning from war and mingling with civilians who don’t understand what you went through. “I met up with some friends who are really bright people but who said, ‘Wait, the winter was traumatizing?’” Molly Phelps told me. She thinks that “health-care workers are either preparing for work, at work, or recovering from work,” which leaves little time for talking about their experiences. And those who do talk can hit a brick wall of pandemic denial.
Cassie Alexander also struggled with the fact that she was struggling. “I built my whole identity around being the toughest person I knew, and it was shattering to admit that I was broken and needed help,” she said. She returned to work last week, partly for financial reasons and partly to prove to herself that she can still do it. Others have peeled off to less intense medical roles. And some have no plans to return at all—but feel guilty about abandoning their colleagues and patients. “People going into medicine want to be of service in moments of crisis, so it was hard to watch [further surges] and feel like I was on the sidelines,” Lindsay Fox told me.
Some former health-care workers have found new purpose in tackling health problems at a different scale. Sheetal Rao has helped launch an environmental nonprofit that plants trees in Chicago, especially in poorer neighborhoods that lack them. “In primary care, we focus on prevention, but that’s also about advocating for cleaner air so I’m not just sending my patients home with an inhaler,” she told me.
Dona Kim Murphey, a former physician who now has long COVID, started a political action committee to get doctors into office as part of a plan to reform medicine. “I was growing increasingly concerned about how inhumane our profession is,” she told me. “There’s no culture of physicians organizing and fighting for their rights, but that’s something we should think about to leverage the outrage and frustration that people have.” For the same reason, Nerissa Black, a nurse in Valencia, California, is staying in medicine. She was so disillusioned by her hospital’s handling of the pandemic that she almost left nursing entirely. But she changed her mind to continue being part of the National Nurses United union and advocating for better working conditions. For example, California is the only state that caps the ratio of patients to nurses, and she wants to see similar limits nationwide. “I feel more resolute,” she told me.
Phelps, meanwhile, found the last thing she expected—a sense of peace. She used to scoff when she heard people say that you’re more than your job. “I thought, That may be true for all you nonmedical laypeople, but I am a doctor and it’s who I am,” she told me. And yet, she has experienced no identity crisis. After her last shift this September, she was on a random weekend trip with her children when, in the middle of a pumpkin patch, she started sobbing. “I realized that I was happy, and I hadn’t experienced that in almost two years,” she told me. “I’m not sure I can ever see myself going into an ER again.”


Hi Friends! Welcome back to my channel! I’ve missed you guys so much! November is Prematurity Awareness Month so all month long we will be reading books by Preemie Authors, Parents, Siblings, and Healthcare workers who work with Preemies!


As we transition from a month-long celebration of Premature Awareness in November, I encourage our community to continue the momentum of raising advocacy for our global healthcare/medical community.
It is troubling that our pre-term birth/Neonatal Womb Warrior community is losing some of its most essential members and that a severely reduced access to trained providers lies ahead. There is a critical shortage globally of access to healthcare providers who are more challenged now than ever to keep all of our hearts beating.
In the specialty of neonatology clinicians are essential to saving lives and to guiding/empowering parents/caregivers and families in some of their most life-changing and challenging life chapters.
Throughout the past almost 5 years within this blog we have shared articles calling attention to the critical global Healthcare Workforce shortages. Recently, the loss of many members of our vital global healthcare/medical community has been and is becoming better understood, more clearly documented, and shared to some extent with the Public at large. It is a quickly evolving and sometimes complex situation that demands intelligent and expedited attention in order to mitigate the damaged caused so far. Solutions for developing and rebuilding/expanding the healthcare/medical workforce require the collaborative efforts of actual healthcare/medical provider-directed solutions and a clear patient population needs assessment generated by the patient population itself.
The loss of clinicians has a staggering impact on the overall functionality and progress of positive health outcomes in every community. Just as we are all touched by preterm birth and preterm birth loss, we are all directly and indirectly impacted by the loss of our clinical workforce at large.
I encourage us all to do what we can to promote awareness and support for our local and global medical/healthcare community at this time. We all need safe, equitable, timely and sustainable access to preterm birth care, maternal care, general medical and surgical healthcare and ancillary services. We require more than pharmaceuticals thrown our way; we need trained providers to provide us with optimal care that is curative when possible and personalized to meet our unique individual needs.
With great appreciation and love for our preterm birth/Neonatal Womb Warrior Community, we Thank You.
Kat, Kathy, and Gannon (our beloved cat).

These Are The Burly Souls Who Brave Ireland’s Biggest Waves
Nov 7, 2020Red Bull Surfing
The start of the 2020–21 big wave season has been nothing if not historic. Especially in Ireland, where Conor Maguire nabbed what many are calling the biggest wave ever surfed at Ireland’s premiere – and most terrifying – wave, Mullaghmore. Here’s a look back at filmmaker Mikey Corker’s award-winning 2018 docu-series Made In Ireland, which traces surfing’s roots in what was once considered the unlikeliest of surf destinations.

